

Using Targeted Transcriptome and Machine Learning of Pre- and Post-Transplant Bone Marrow Samples to Predict Acute Graft-versus-Host Disease and Overall Survival after Allogeneic Stem Cell Transplantation

 , , , , , ,
, , , , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Diagnosis of aGvHD
2.3. Sample Collection
2.4. RNA Extraction and Next Generation Sequencing (NGS)
2.5. Machine Learning Algorithm for Predicting aGvHD
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics
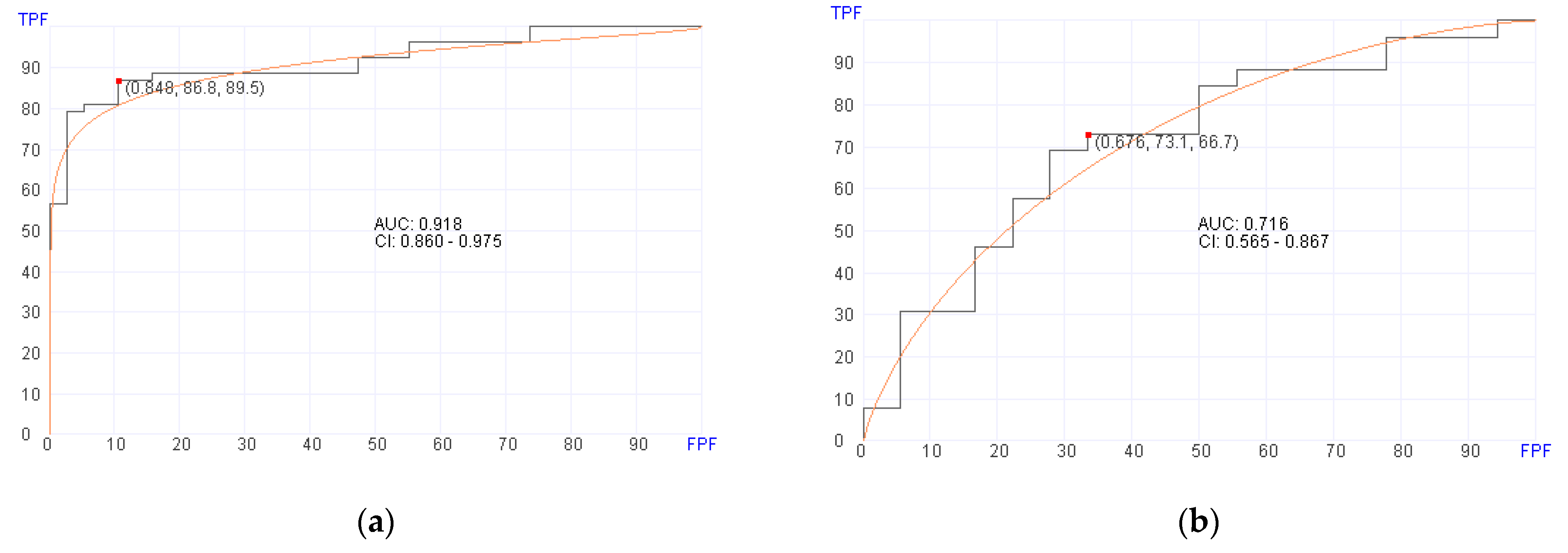
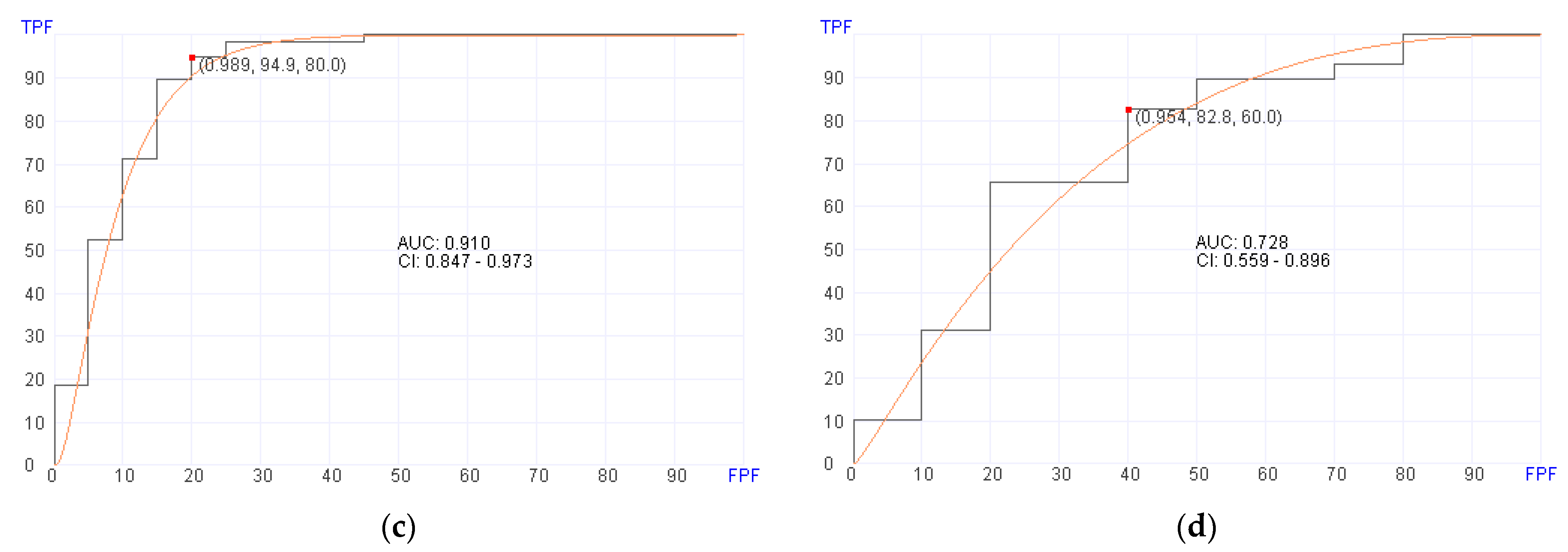
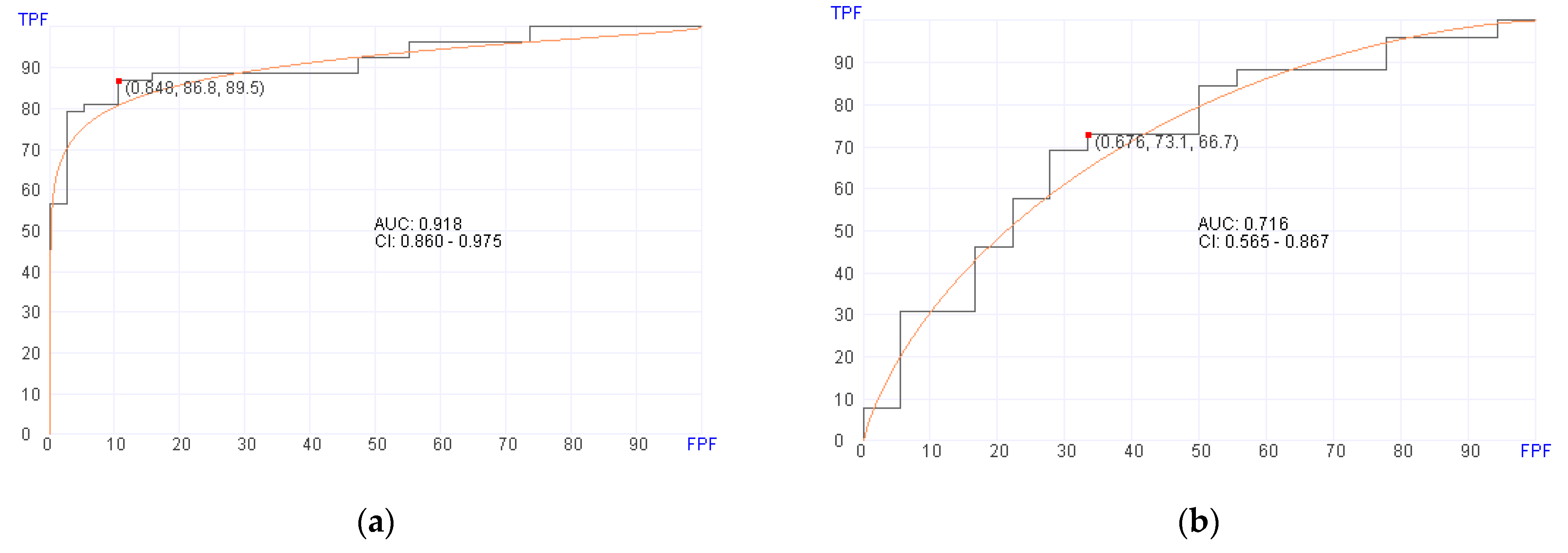
3.2. Prediction of aGvHD Using Post-Transplant Samples
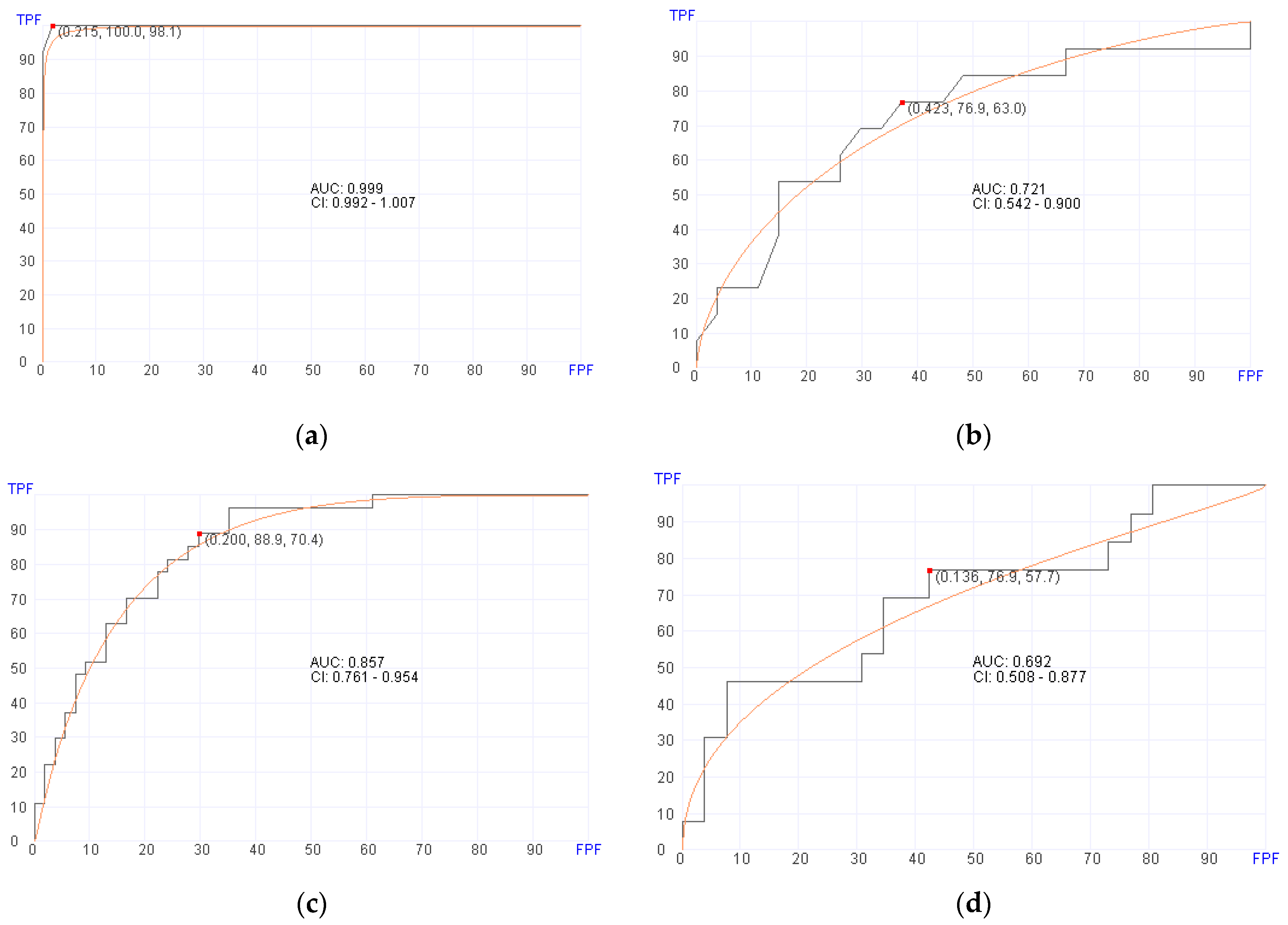
3.3. Prediction of aGvHD Using Pre-Transplant Samples
3.4. Prediction of Overall Survival (OS) Using Post-Transplant Samples
3.5. Prediction of Overall Survival (OS) Using Pre-Transplant Samples
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ramdial, J.L.; Mehta, R.S.; Saliba, R.M.; Alousi, A.M.; Bashir, Q.; Hosing, C.; Kebriaei, P.; Olson, A.L.; Oran, B.; Qazilbash, M.H.; et al. Acute graft-versus-host-disease is the foremost cause of late nonrelapse mortality. Bone Marrow Transplant. 2021, 56, 2005–2012. [Google Scholar] [CrossRef] [PubMed]
- Hartwell, M.J.; Ozbek, U.; Holler, E.; Renteria, A.S.; Major-Monfried, H.; Reddy, P.; Aziz, M.; Hogan, W.J.; Ayuk, F.; Efebera, Y.A.; et al. An early-biomarker algorithm predicts lethal graft-versus-host disease and survival. JCI Insight 2017, 2, e89798, Erratum in JCI Insight 2018, 3, e124015. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.W.; Reddy, P. Current and emerging strategies for the prevention of graft-versus-host disease. Nat. Rev. Clin. Oncol. 2014, 11, 536–547. [Google Scholar] [CrossRef] [PubMed]
- Rimando, J.; McCurdy, S.R.; Luznik, L. How I prevent GVHD in high-risk patients: Posttransplant cyclophosphamide and beyond. Blood 2023, 141, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Ghimire, S.; Weber, D.; Mavin, E.; Wang, X.N.; Dickinson, A.M.; Holler, E. Pathophysiology of GvHD and other HSCT-related major complications. Front. Immunol. 2017, 8, 79. [Google Scholar] [CrossRef] [PubMed]
- Srinagesh, H.K.; Levine, J.E.; Ferrara, J.L.M. Biomarkers in acute graft-versus-host disease: New insights. Ther. Adv. Hematol. 2019, 10, 2040620719891358. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.S.; Huang, X.J. Seeking biomarkers for acute graft-versus-host disease: Where we are and where we are heading? Biomark. Res. 2019, 7, 17. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.C.; Ferrara, J.L.; Levine, J.E. Advances in predicting acute GVHD. Br. J. Haematol. 2013, 160, 288–302. [Google Scholar] [CrossRef] [PubMed]
- Jagasia, M.; Arora, M.; Flowers, M.E.; Chao, N.J.; McCarthy, P.L.; Cutler, C.S.; Urbano-Ispizua, A.; Pavletic, S.Z.; Haagenson, M.D.; Zhang, M.-J.; et al. Risk Factors for acute GVHD and survival after hematopoietic cell transplantation. Blood 2012, 119, 296–307. [Google Scholar] [CrossRef]
- Paczesny, S. Discovery and validation of graft-versus-host disease biomarkers. Blood 2013, 121, 585–594. [Google Scholar] [CrossRef]
- Srinagesh, H.K.; Ozbek, U.; Kapoor, U.; Ayuk, F.; Aziz, M.; Ben-David, K.; Choe, H.K.; DeFilipp, Z.; Etra, A.; Grupp, S.A.; et al. The MAGIC algorithm probability is a validated response biomarker of treatment of acute graft-versus-host disease. Blood Adv. 2019, 3, 4034–4042. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Chappell, G.T.; Mazzoli, A.; Tewari, M.; Choi, S.W.; Wiens, J. Predicting acute graft-versus-host disease using machine learning and longitudinal vital sign data from electronic health records. JCO Clin. Cancer Inform. 2020, 4, 128–135. [Google Scholar] [CrossRef]
- Reel, P.S.; Reel, S.; Pearson, E.; Trucco, E.; Jefferson, E. Using machine learning approaches for multi-omics data analysis: A review. Biotechnol. Adv. 2021, 49, 107739. [Google Scholar] [CrossRef]
- Sen, S.K.; Green, E.D.; Hutter, C.M.; Craven, M.; Ideker, T.; Di Francesco, V. Opportunities for basic, clinical, and bioethics research at the intersection of machine learning and genomics. Cell Genom. 2024, 4, 100466. [Google Scholar] [CrossRef] [PubMed]
- Khandelwal, P.; Lounder, D.T.; Bartlett, A.; Haberman, Y.; Jegga, A.G.; Ghandikota, S.; Koo, J.; Luebbering, N.; Leino, D.; Abdullah, S.; et al. Transcriptome analysis in acute gastrointestinal graft-versus-host disease reveals a unique signature in children and shared biology with pediatric inflammatory bowel disease. Haematologica 2023, 108, 1803–1816. [Google Scholar] [CrossRef] [PubMed]
- Zouali, H.; Lemasson, J.; Calugareanu, A.; Battail, C.; Michonneau, D.; le Buanec, H.; Grolleau, C.; Cassius, C.; Robin, M.; Merandet, M.M.; et al. RNA sequencing of chronic GVHD skin lesions defines shared and unique inflammatory pathways characterizing lichen planus and morphea. Blood Adv. 2022, 6, 2805–2811. [Google Scholar] [CrossRef] [PubMed]
- Bacigalupo, A.; Ballen, K.; Rizzo, D.; Giralt, S.; Lazarus, H.; Ho, V.; Apperley, J.; Slavin, S.; Pasquini, M.; Sandmaier, B.M.; et al. Defining the intensity of conditioning regimens: Working definitions. Biol. Blood Marrow Transplant. 2009, 15, 1628–1633. [Google Scholar] [CrossRef] [PubMed]
- Przepiorka, D.; Weisdorf, D.; Martin, P.; Klingemann, H.G.; Beatty, P.; Hows, J.; Thomas, E.D. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995, 15, 825–828. [Google Scholar] [PubMed]
- Harris, A.C.; Young, R.; Devine, S.; Hogan, W.J.; Ayuk, F.; Bunworasate, U.; Chanswangphuwana, C.; Efebera, Y.A.; Holler, E.; Litzow, M.; et al. International, multicenter standardization of acute graft-versus-host disease clinical data collection: A report from the Mount Sinai Acute GVHD International Consortium. Biol. Blood Marrow Transplant. 2016, 22, 4–10. [Google Scholar] [CrossRef]
- Kanehisa, M.; Goto, S. KEGG: Kyoto encyclopedia of genes and genomes. Nucleic Acids Res. 2000, 28, 27–30. [Google Scholar] [CrossRef]
- Kanehisa, M. Toward understanding the origin and evolution of cellular organisms. Protein Sci. 2019, 28, 1947–1951. [Google Scholar] [CrossRef] [PubMed]
- Kanehisa, M.; Furumichi, M.; Sato, Y.; Kawashima, M.; Ishiguro-Watanabe, M. KEGG for taxonomy-based analysis of pathways and genomes. Nucleic Acids Res. 2023, 51, D587–D592. [Google Scholar] [CrossRef]
- Zhang, H.; Qureshi, M.A.; Wahid, M.; Charifa, A.; Ehsan, A.; Ip, A.; De Dios, I.; Ma, W.; Sharma, I.; McCloskey, J.; et al. Differential diagnosis of hematologic and solid tumors using targeted transcriptome and artificial intelligence. Am. J. Pathol. 2023, 193, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Albitar, M.; Zhang, H.; Pecora, A.; Waintraub, S.; Graham, D.; Hellmann, M.; McNamara, D.; Charifa, A.; De Dios, I.; Ma, W.; et al. Homologous recombination abnormalities associated with BRCA1/2 mutations as predicted by machine learning of targeted next-generation sequencing data. Breast Cancer 2023, 17, 11782234231198979. [Google Scholar] [CrossRef] [PubMed]
- Jagasia, M.; Perales, M.A.; Schroeder, M.A.; Ali, H.; Shah, N.N.; Chen, Y.-B.; Fazal, S.; Dawkins, F.W.; Arbushites, M.C.; Tian, C.; et al. Ruxolitinib for the treatment of steroid-refractory acute GVHD (REACH1): A multicenter, open-label phase 2 trial. Blood 2020, 135, 1739–1749. [Google Scholar] [CrossRef] [PubMed]
- Zeiser, R.; Polverelli, N.; Ram, R.; Hashmi, S.K.; Chakraverty, R.; Middeke, J.M.; Musso, M.; Giebel, S.; Uzay, A.; Langmuir, P.; et al. Ruxolitinib for glucocorticoid-refractory chronic graft-versus-host disease. N. Engl. J. Med. 2021, 385, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Cooper, M.L.; Alahmari, B.; Ritchey, J.; Collins, L.; Holt, M.; DiPersio, J.F. Pharmacologic blockade of JAK1/JAK2 reduces GvHD and preserves the graft-versus-leukemia effect. PLoS ONE 2014, 9, e109799. [Google Scholar] [CrossRef]
- Dubovsky, J.A.; Flynn, R.; Du, J.; Harrington, B.K.; Zhong, Y.; Kaffenberger, B.; Yang, C.; Towns, W.H.; Lehman, A.; Johnson, A.J.; et al. Ibrutinib treatment ameliorates murine chronic graft-versus-host disease. J. Clin. Investig. 2014, 124, 4867–4876. [Google Scholar] [CrossRef] [PubMed]
- Schutt, S.D.; Fu, J.; Nguyen, H.; Bastian, D.; Heinrichs, J.; Wu, Y.; Liu, C.; McDonald, D.G.; Pidala, J.; Yu, X.-Z. Inhibition of BTK and ITK with ibrutinib is effective in the prevention of chronic graft-versus-host disease in mice. PLoS ONE 2015, 10, e0137641. [Google Scholar] [CrossRef]
- Waller, E.K.; Miklos, D.; Cutler, C.; Arora, M.; Jagasia, M.H.; Pusic, I.; Flowers, M.E.; Logan, A.C.; Nakamura, R.; Chang, S.; et al. Ibrutinib for chronic graft-versus-host disease after failure of prior therapy: 1-year update of a phase 1b/2 study. Biol. Blood Marrow Transplant. 2019, 25, 2002–2007. [Google Scholar] [CrossRef]
- Cutler, C.; Lee, S.J.; Arai, S.; Rotta, M.; Zoghi, B.; Lazaryan, A.; Ramakrishnan, A.; DeFilipp, Z.; Salhotra, A.; Chai-Ho, W.; et al. Belumosudil for chronic graft-versus-host disease after 2 or more prior lines of therapy: The ROCKstar Study. Blood 2021, 138, 2278–2289, Erratum in Blood 2022, 139, 1772. [Google Scholar] [CrossRef] [PubMed]
- Martini, D.J.; Chen, Y.B.; DeFilipp, Z. Recent FDA approvals in the treatment of graft-versus-host disease. Oncologist 2022, 27, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Pitea, M.; Canale, F.A.; Porto, G.; Verduci, C.; Utano, G.; Policastro, G.; Alati, C.; Santoro, L.; Imbalzano, L.; Martino, M. The Role of MicroRNA in Graft-Versus-Host-Disease: A Review. Genes 2023, 14, 1796. [Google Scholar] [CrossRef] [PubMed]
- Shono, Y.; van den Brink, M. Gut microbiota injury in allogeneic haematopoietic stem cell transplantation. Nat. Rev. Cancer 2018, 18, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, A.; Ebadi, M.; Rehman, T.U.; Elhusseini, H.; Kazadi, D.; Halaweish, H.; Khan, M.H.; Hoeschen, A.; Cao, Q.; Luo, X.; et al. Potential of fecal microbiota transplantation to prevent acute GVHD: Analysis from a phase II trial. Clin. Cancer Res. 2023, 29, 4920–4929. [Google Scholar] [CrossRef]
- McCurdy, S.R.; Radojcic, V.; Tsai, H.L.; Vulic, A.; Thompson, E.; Ivcevic, S.; Kanakry, C.G.; Powell, J.D.; Lohman, B.K.; Adom, D.; et al. Signatures of GVHD and relapse after posttransplant cyclophosphamide revealed by immune profiling and machine learning. Blood 2022, 139, 608–623. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients N = 167 n (%) | Pre-Transplant Patients N = 132 n (%) | Post-Transplant Patients N = 119 n (%) |
|---|---|---|---|
| Recipient age, median years (range) | 63.0 (20.8–79.0) | 64.0 (20.8–79.0) | 63.7 (20.8–79.0) |
| Recipient sex | |||
| Male | 89 (53) | 71 (54) | 62 (52) |
| Indication for allo-HSCT | |||
| ALL | 20 (12) | 15 (11) | 15 (13) |
| AML | 57 (34) | 40 (30) | 47 (39) |
| CML | 3 (2) | 2 (2) | 3 (3) |
| MDS | 44 (26) | 37 (28) | 31 (26) |
| Myelofibrosis/CMML | 32 (19) | 27 (20) | 19 (16) |
| SAA | 4 (2) | 4 (3) | 1 (1) |
| NHL | 7 (4) | 7 (5) | 3 (3) |
| Graft source | |||
| Bone marrow | 130 (78) | 30 (23) | 23 (19) |
| Peripheral blood | 37 (22) | 102 (77) | 96 (81) |
| HLA compatibility | |||
| Unrelated donor HLA match | 84 (50) | 64 (48) | 65 (55) |
| Unrelated donor HLA mismatch | 17 (10) | 13 (10) | 13 (11) |
| HLA matched related donor | 14 (8) | 11 (8) | 9 (8) |
| Related donor, haploidentical | 52 (31) | 44 (33) | 32 (27) |
| Donor age, median years (range) | 28.3 (14.0–63.7) | 28.1 (17.6–63.7) | 28.0 (14.0–59.0) |
| Donor age < 35 years | 120 (72) | 98 (74) | 89 (75) |
| Donor sex | |||
| Male | 109 (65) | 82 (62) | 77 (65) |
| Conditioning regimen | |||
| Myeloablative | 43 (26) | 30 (23) | 33 (28) |
| Non-myeloablative | 47 (28) | 41 (31) | 31 (26) |
| Reduced intensity | 77 (46) | 61 (46) | 55 (46) |
| aGvHD prophylaxis regimen | |||
| PtCy | 73 (44) | 62 (47) | 49 (41) |
| TacMTX | 75 (45) | 55 (42) | 58 (49) |
| RapaCspMMF | 19 (11) | 15 (11) | 12 (10) |
| Addition of abatacept | 21 (13) | 18 (14) | 16 (13) |
| Addition of anti-thymocyte globulin | 38 (23) | 26 (20) | 31 (26) |
| Diagnosed with aGvHD | |||
| Stage 1–4 | 109 (65) | 87 (66) | 80 (67) |
| Stage 3–4 | 7 (4) | 6 (5) | 1 (1) |
| Site of aGvHD | |||
| Gastrointestinal | 65 (39) | 51 (71) | 49 (40) |
| Lower | 17 (10) | 12 (30) | 10 (8) |
| Upper | 48 (29) | 39 (41) | 39 (32) |
| Liver | 5 (3) | 4 (3) | 4 (3) |
| Skin | 63 (38) | 54 (41) | 51 (43) |
| 92 Genes Predicting GvHD | |||
|---|---|---|---|
| 1–23 | 24–46 | 47–69 | 70–92 |
| DUSP2 | CDKN1A | NEURL1 | SUZ12 |
| CD22 | TFRC (CD71) | TNFRSF17 (BCMA) | TRIM33 |
| FLNA | DLL3 | BCL7A | CDK9 |
| PAX8 | SSBP2 | YTHDF2 | FLYWCH1 |
| ARHGEF12 | TRAF3 | KIF5B | HIST1H2BC |
| AKAP9 | PSIP1 | IRS1 | MAPK1 |
| DLL4 | 43717SEPT9 | DGKZ | RAC2 |
| AIP | SPTBN1 | CENPU | TCF7L2 |
| CDC14B | HIST1H2AC | STIL | USP42 |
| FOXO3 | TFDP1 | XKR3 | FGFR1OP |
| EGR4 | TRAF5 | CCT6B | MTCP1 |
| MUTYH | BACH2 | CD28 | PTPRO |
| SS18L1 | TNFRSF10D | OLIG1 | SH3D19 |
| PRKCG | SLC45A3 | CCND2 | CTDSP2 |
| HOOK3 | NACA | GID4 | ID3 |
| TCEA1 | ASPH | STYK1 | SMAP1 |
| UBE2C | ZBTB16 | ATF3 | STL |
| FIGF | EPHA2 | FGF9 | TAL1 |
| TOP1 | APOD | ZNF703 | DNMT3A |
| DTX1 | KAT2B | AKAP12 | IKBKE |
| TNF | ETV5 | PTCRA | IKZF3 |
| CCNE1 | FGF13 | SMAD6 | AKT3 |
| BAIAP2L1 | FLT3LG | DNAJB1 | HSPA4 |
| Genes Predicting Survival | |
|---|---|
| 1–10 | 11–20 |
| ATIC | TGFBI |
| PLAG1 | BRSK1 |
| CD36 | KIT (CD117) |
| HSP90AB1 | MSH6 |
| DNMT1 | HIST1H1D |
| WDR1 | HEY1 |
| CDC14A | FOXO1 |
| MALT1 | PRKCA |
| SP3 | CCNB1IP1 |
| MAP3K14 | FANCC |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rowley, S.D.; Gunning, T.S.; Pelliccia, M.; Della Pia, A.; Lee, A.; Behrmann, J.; Bangolo, A.; Jandir, P.; Zhang, H.; Kaur, S.; et al. Using Targeted Transcriptome and Machine Learning of Pre- and Post-Transplant Bone Marrow Samples to Predict Acute Graft-versus-Host Disease and Overall Survival after Allogeneic Stem Cell Transplantation. Cancers 2024, 16, 1357. https://doi.org/10.3390/cancers16071357
Rowley SD, Gunning TS, Pelliccia M, Della Pia A, Lee A, Behrmann J, Bangolo A, Jandir P, Zhang H, Kaur S, et al. Using Targeted Transcriptome and Machine Learning of Pre- and Post-Transplant Bone Marrow Samples to Predict Acute Graft-versus-Host Disease and Overall Survival after Allogeneic Stem Cell Transplantation. Cancers. 2024; 16(7):1357. https://doi.org/10.3390/cancers16071357
Chicago/Turabian StyleRowley, Scott D., Thomas S. Gunning, Michael Pelliccia, Alexandra Della Pia, Albert Lee, James Behrmann, Ayrton Bangolo, Parul Jandir, Hong Zhang, Sukhdeep Kaur, and et al. 2024. "Using Targeted Transcriptome and Machine Learning of Pre- and Post-Transplant Bone Marrow Samples to Predict Acute Graft-versus-Host Disease and Overall Survival after Allogeneic Stem Cell Transplantation" Cancers 16, no. 7: 1357. https://doi.org/10.3390/cancers16071357
APA StyleRowley, S. D., Gunning, T. S., Pelliccia, M., Della Pia, A., Lee, A., Behrmann, J., Bangolo, A., Jandir, P., Zhang, H., Kaur, S., Suh, H. C., Donato, M., Albitar, M., & Ip, A. (2024). Using Targeted Transcriptome and Machine Learning of Pre- and Post-Transplant Bone Marrow Samples to Predict Acute Graft-versus-Host Disease and Overall Survival after Allogeneic Stem Cell Transplantation. Cancers, 16(7), 1357. https://doi.org/10.3390/cancers16071357