
Autoimmune Atrophic Gastritis: A Clinical Review

 , , , and
, , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Epidemiology
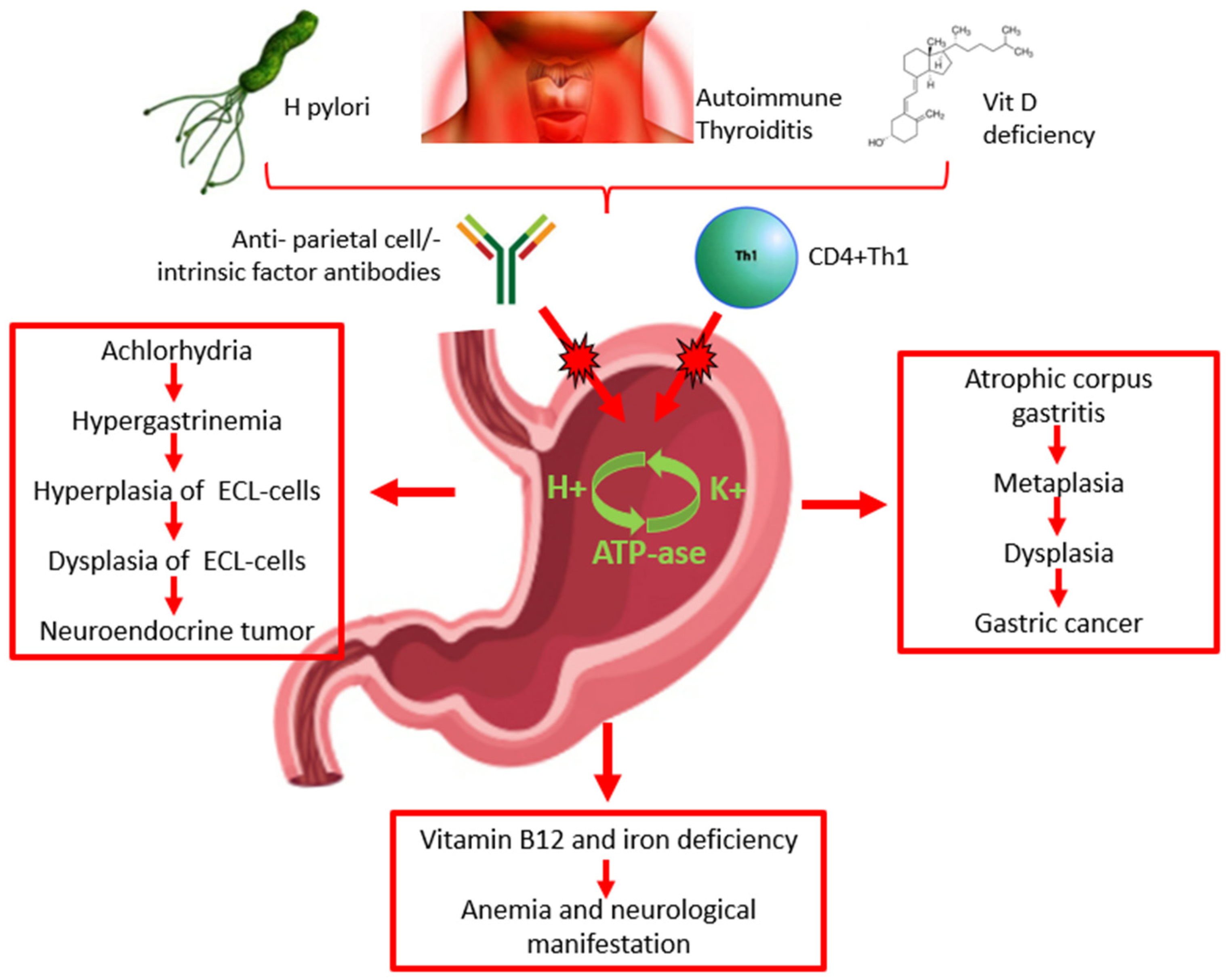
3. Etiopathogenesis
4. Diagnosis
5. Clinical Manifestations
6. Risk of Malignancy
7. Management
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kamada, T.; Maruyama, Y.; Monobe, Y.; Haruma, K. Endoscopic features and clinical importance of autoimmune gastritis. Dig. Endosc. 2022, 34, 700–713. [Google Scholar] [CrossRef] [PubMed]
- Hall, S.N.; Appelman, H.D. Autoimmune Gastritis. Arch. Pathol. Lab. Med. 2019, 143, 1327–1331. [Google Scholar] [CrossRef]
- Torbenson, M.; Abraham, S.C.; Boitnott, J.; Yardley, J.H.; Wu, T.T. Autoimmune gastritis: Distinct histological and immunohistochemical findings before complete loss of oxyntic glands. Mod. Pathol. 2002, 15, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Conti, L.; Annibale, B.; Corleto, V.D. Current Perspectives in Atrophic Gastritis. Curr. Gastroenterol. Rep. 2020, 22, 38. [Google Scholar] [CrossRef] [PubMed]
- Rustgi, S.D.; Bijlani, P.; Shah, S.C. Autoimmune gastritis, with or without pernicious anemia: Epidemiology, risk factors, and clinical management. Therap. Adv. Gastroenterol. 2021, 14. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, T.; Yoshida, S.; Watanabe, H.; Toyoshima, A.; Kataoka, Y.; Takahashi, Y.; Kanazawa, T.; Ebinuma, H.; Suzuki, H.; Koike, K.; et al. Clue of Diagnosis for Autoimmune Gastritis. Digestion 2021, 102, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Dilaghi, E.; Cingolani, S.; Pivetta, G.; Dottori, L.; Esposito, G.; Marzinotto, I.; Lampasona, V.; Buzzetti, R.; Annibale, B. Gender-sex differences in autoimmune atrophic gastritis. Transl. Res. 2022, 248, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Minalyan, A.; Benhammou, J.N.; Artashesyan, A.; Lewis, M.S.; Pisegna, J.R. Autoimmune atrophic gastritis: Current perspectives. Clin. Exp. Gastroenterol. 2017, 10, 19–27. [Google Scholar] [CrossRef] [PubMed]
- De Block, C.E.; De Leeuw, I.H.; Van Gaal, L.F. Autoimmune gastritis in type 1 diabetes: A clinically oriented review. J. Clin. Endocrinol. Metab. 2008, 93, 363–371. [Google Scholar] [CrossRef]
- Fallahi, P.; Ferrari, S.M.; Ruffilli, I.; Elia, G.; Biricotti, M.; Vita, R.; Benvenga, S.; Antonelli, A. The association of other autoimmune diseases in patients with autoimmune thyroiditis: Review of the literature and report of a large series of patients. Autoimmun. Rev. 2016, 15, 1125–1128. [Google Scholar] [CrossRef] [PubMed]
- Kalkan, Ç.; Soykan, I. Polyautoimmunity in autoimmune gastritis. Eur. J. Intern. Med. 2016, 31, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Betterle, C.; Dal Pra, C.; Mantero, F.; Zanchetta, R. Autoimmune adrenal insufficiency and autoimmune polyendocrine syndromes: Autoantibodies, autoantigens, and their applicability in diagnosis and disease prediction. Endocr. Rev. 2002, 23, 327–364. [Google Scholar] [CrossRef] [PubMed]
- Toh, B.H. Diagnosis and classification of autoimmune gastritis. Autoimmun. Rev. 2014, 13, 459–462. [Google Scholar] [CrossRef]
- Rusak, E.; Chobot, A.; Krzywicka, A.; Wenzlau, J. Anti-parietal cell antibodies—Diagnostic significance. Adv. Med. Sci. 2016, 61, 175–179. [Google Scholar] [CrossRef] [PubMed]
- D’Aurizio, F.; Villalta, D.; Metus, P.; Doretto, P.; Tozzoli, R. Is vitamin D a player or not in the pathophysiology of autoimmune thyroid diseases? Autoimmun. Rev. 2015, 14, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Iwamuro, M.; Tanaka, T.; Otsuka, M. Update in Molecular Aspects and Diagnosis of Autoimmune Gastritis. Curr. Issues Mol. Biol. 2023, 45, 5263–5275. [Google Scholar] [CrossRef] [PubMed]
- Ihara, T.; Ihara, N.; Kushima, R. Autoimmune Gastritis with a Long-term Course of Type B Gastritis: A Report of Two Cases. Intern. Med. 2023, 62, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Ohana, M.; Okazaki, K.; Oshima, C.; Kawasaki, K.; Fukui, T.; Tamaki, H.; Matsuura, M.; Asada, M.; Nishi, T.; Uchida, K.; et al. Inhibitory effects of Helicobacter pylori infection on murine autoimmune gastritis. Gut 2003, 52, 1102–1110. [Google Scholar] [CrossRef]
- Ihara, T.; Ihara, N.; Kushima, R.; Haruma, K. Rapid Progression of Autoimmune Gastritis after Helicobacter pylori Eradication Therapy. Intern. Med. 2023, 62, 1603–1609. [Google Scholar] [CrossRef] [PubMed]
- Miceli, E.; Lenti, M.V.; Gentile, A.; Gambini, G.; Petrucci, C.; Pitotti, L.; Mengoli, C.; Di Stefano, M.; Vanoli, A.; Luinetti, O.; et al. Long-term natural history of autoimmune gastritis: Results from a prospective, monocentric series. Am. J. Gastroenterol. 2024. [Google Scholar] [CrossRef]
- Guo, X.; Schreurs, M.W.J.; Marijnissen, F.E.; Mommersteeg, M.C.; Nieuwenburg, S.A.V.; Doukas, M.; Erler, N.S.; Capelle, L.G.; Bruno, M.J.; Peppelenbosch, M.P.; et al. Increased Prevalence of Autoimmune Gastritis in Patients with a Gastric Precancerous Lesion. J. Clin. Med. 2023, 12, 6152. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Chakole, S.; Agrawal, S.; Shetty, N.; Prasad, R.; Lohakare, T.; Wanjari, M.; Yelne, S. A Comprehensive Review of Upper Gastrointestinal Symptom Management in Autoimmune Gastritis: Current Insights and Future Directions. Cureus 2023, 15, e43418. [Google Scholar] [CrossRef] [PubMed]
- Conti, L.; Annibale, B.; Lahner, E. Autoimmune Gastritis and Gastric Microbiota. Microorganisms 2020, 8, 1827. [Google Scholar] [CrossRef] [PubMed]
- Miceli, E.; Di Stefano, M.; Lenti, M.V.; Pitotti, L.; Corazza, G.R.; Di Sabatino, A.; the Autoimmune Gastritis Working Group. Pregnancy-related complications in autoimmune atrophic gastritis: A monocentric experience. Dig. Liver Dis. 2023, 55, 146–148. [Google Scholar] [CrossRef] [PubMed]
- Rugge, M.; Bricca, L.; Guzzinati, S.; Sacchi, D.; Pizzi, M.; Savarino, E.; Farinati, F.; Zorzi, M.; Fassan, M.; Dei Tos, A.P.; et al. Autoimmune gastritis: Long-term natural history in naive Helicobacter pylori-negative patients. Gut 2023, 72, 30–38. [Google Scholar] [CrossRef]
- Dilaghi, E.; Dottori, L.; Pivetta, G.; Dalla Bella, M.; Esposito, G.; Ligato, I.; Pilozzi, E.; Annibale, B.; Lahner, E. Incidence and Predictors of Gastric Neoplastic Lesions in Corpus-Restricted Atrophic Gastritis: A Single-Center Cohort Study. Am. J. Gastroenterol. 2023, 118, 2157–2165. [Google Scholar] [CrossRef] [PubMed]
- Centanni, M.; Marignani, M.; Gargano, L.; Corleto, V.D.; Casini, A.; Delle Fave, G.; Andreoli, M.; Annibale, B. Atrophic body gastritis in patients with autoimmune thyroid disease: An underdiagnosed association. Arch. Intern. Med. 1999, 159, 1726–1730. [Google Scholar] [CrossRef] [PubMed]
- Winter, S.; Rehm, A.; Wichner, K.; Scheel, T.; Batra, A.; Siegmund, B.; Berek, C.; Lipp, M.; Höpken, U.E. Manifestation of spontaneous and early autoimmune gastritis in CCR7-deficient mice. Am. J. Pathol. 2011, 179, 754–765. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Xiao, X.; An, H.; Wang, J.; Ma, Y.; Qian, Y.H. Inhibition of CCR7 promotes NF-κB-dependent apoptosis and suppresses epithelial-mesenchymal transition in non-small cell lung cancer. Oncol. Rep. 2017, 37, 2913–2919. [Google Scholar] [CrossRef] [PubMed]
- Krike, P.; Appel, M.S.; Shums, Z.; Polaka, I.; Kojalo, I.; Rudzite, D.; Tolmanis, I.; Kirsners, A.; Bogdanova, I.; Aleksandravica, I.; et al. Autoimmune gastritis serological biomarkers in gastric cancer patients. Eur. J. Cancer Prev. 2024, 33, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Lenti, M.V.; Miceli, E.; Vanoli, A.; Klersy, C.; Corazza, G.R.; Di Sabatino, A. Time course and risk factors of evolution from potential to overt autoimmune gastritis. Dig. Liver Dis. 2022, 54, 642–644. [Google Scholar] [CrossRef] [PubMed]
- Lenti, M.V.; Vanoli, A.; Miceli, E.; Arpa, G.; Di Stefano, M.; Soriano, S.; Capuano, F.; Gentile, A.; Aronico, N.; Coppola, L.; et al. Increase of Deep Intraepithelial Lymphocytes in the Oxyntic Mucosa of Patients With Potential and Overt Autoimmune Gastritis. Front. Immunol. 2022, 13, 866167. [Google Scholar] [CrossRef]
- Huang, Y.K.; Yu, J.C.; Kang, W.M.; Ma, Z.Q.; Ye, X.; Tian, S.B.; Yan, C. Significance of Serum Pepsinogens as a Biomarker for Gastric Cancer and Atrophic Gastritis Screening: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0142080. [Google Scholar] [CrossRef] [PubMed]
- Terao, S.; Suzuki, S.; Yaita, H.; Kurahara, K.; Shunto, J.; Furuta, T.; Maruyama, Y.; Ito, M.; Kamada, T.; Aoki, R.; et al. Multicenter study of autoimmune gastritis in Japan: Clinical and endoscopic characteristics. Dig. Endosc. 2020, 32, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Zagari, R.M.; Rabitti, S.; Greenwood, D.C.; Eusebi, L.H.; Vestito, A.; Bazzoli, F. Systematic review with meta-analysis: Diagnostic performance of the combination of pepsinogen, gastrin-17 and anti-Helicobacter pylori antibodies serum assays for the diagnosis of atrophic gastritis. Aliment. Pharmacol. Ther. 2017, 46, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Nehme, F.; Rowe, K.; Palko, W.; Tofteland, N.; Salyers, W. Autoimmune metaplastic atrophic gastritis and association with neuroendocrine tumors of the stomach. Clin. J. Gastroenterol. 2020, 13, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Anagnostopoulos, G.K.; Ragunath, K.; Shonde, A.; Hawkey, C.J.; Yao, K. Diagnosis of autoimmune gastritis by high resolution magnification endoscopy. World J. Gastroenterol. 2006, 12, 4586–4587. [Google Scholar] [CrossRef]
- Pimentel-Nunes, P.; Libânio, D.; Marcos-Pinto, R.; Areia, M.; Leja, M.; Esposito, G.; Garrido, M.; Kikuste, I.; Megraud, F.; Matysiak-Budnik, T.; et al. Management of epithelial precancerous conditions and lesions in the stomach (MAPS II): European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter and Microbiota Study Group (EHMSG), European Society of Pathology (ESP), and Sociedade Portuguesa de Endoscopia Digestiva (SPED) guideline update 2019. Endoscopy 2019, 51, 365–388. [Google Scholar]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Correa, P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am. J. Surg. Pathol. 1996, 20, 1161–1181. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Conti, L.; Cicone, F.; Capriello, S.; Cazzato, M.; Centanni, M.; Annibale, B.; Virili, C. Thyro-entero-gastric autoimmunity: Pathophysiology and implications for patient management. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101373. [Google Scholar] [CrossRef] [PubMed]
- Carabotti, M.; Lahner, E.; Esposito, G.; Sacchi, M.C.; Severi, C.; Annibale, B. Upper gastrointestinal symptoms in autoimmune gastritis: A cross-sectional study. Medicine 2017, 96, e5784. [Google Scholar] [CrossRef] [PubMed]
- Iwai, W.; Abe, Y.; Iijima, K.; Koike, T.; Uno, K.; Asano, N.; Imatani, A.; Shimosegawa, T. Gastric hypochlorhydria is associated with an exacerbation of dyspeptic symptoms in female patients. J. Gastroenterol. 2013, 48, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Kalkan, C.; Soykan, I.; Soydal, C.; Ozkan, E.; Kalkan, E. Assessment of Gastric Emptying in Patients with Autoimmune Gastritis. Dig. Dis. Sci. 2016, 61, 1597–1602. [Google Scholar] [CrossRef] [PubMed]
- Carabotti, M.; Esposito, G.; Lahner, E.; Pilozzi, E.; Conti, L.; Ranazzi, G.; Severi, C.; Bellini, M.; Annibale, B. Gastroesophageal reflux symptoms and microscopic esophagitis in a cohort of consecutive patients affected by atrophic body gastritis: A pilot study. Scand. J. Gastroenterol. 2019, 54, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Tenca, A.; Massironi, S.; Pugliese, D.; Consonni, D.; Mauro, A.; Cavalcoli, F.; Franchina, M.; Spampatti, M.; Conte, D.; Penagini, R. Gastro-esophageal reflux and antisecretory drugs use among patients with chronic autoimmune atrophic gastritis: A study with pH-impedance monitoring. Neurogastroenterol. Motil. 2016, 28, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Candelario, N.; Klein, C. Megaloblastic anemia due to severe vitamin B(12) deficiency. Cleve. Clin. J. Med. 2022, 89, 8–9. [Google Scholar] [CrossRef] [PubMed]
- Toh, B.H. Pathophysiology and laboratory diagnosis of pernicious anemia. Immunol. Res. 2017, 65, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Zittoun, J. Biermer’s disease. Rev. Prat 2001, 51, 1542–1546. [Google Scholar] [PubMed]
- Moore, C.A.; Adil, A. Macrocytic Anemia; StatPearls: Treasure Island, FL, USA, 2024. [Google Scholar]
- Shipton, M.J.; Thachil, J. Vitamin B12 deficiency—A 21st century perspective. Clin. Med. 2015, 15, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Cellini, M.; Santaguida, M.G.; Stramazzo, I.; Capriello, S.; Brusca, N.; Antonelli, A.; Fallahi, P.; Gargano, L.; Centanni, M.; Virili, C. Recurrent Pregnancy Loss in Women with Hashimoto’s Thyroiditis with Concurrent Non-Endocrine Autoimmune Disorders. Thyroid 2020, 30, 457–462. [Google Scholar] [CrossRef]
- Mahmud, N.; Stashek, K.; Katona, B.W.; Tondon, R.; Shroff, S.G.; Roses, R.; Furth, E.E.; Metz, D.C. The incidence of neoplasia in patients with autoimmune metaplastic atrophic gastritis: A renewed call for surveillance. Ann. Gastroenterol. 2019, 32, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Schubert, M.L. Physiologic, pathophysiologic, and pharmacologic regulation of gastric acid secretion. Curr. Opin. Gastroenterol. 2017, 33, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Imamura, H.; Kaizaki, Y.; Koizumi, W.; Ishido, K.; Kurahara, K.; Suzuki, H.; Fujisaki, J.; Hirakawa, K.; Hosokawa, O.; et al. Management and clinical outcomes of type I gastric carcinoid patients: Retrospective, multicenter study in Japan. Dig. Endosc. 2014, 26, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.C.; Piazuelo, M.B.; Kuipers, E.J.; Li, D. AGA Clinical Practice Update on the Diagnosis and Management of Atrophic Gastritis: Expert Review. Gastroenterology 2021, 161, 1325–1332.e1327. [Google Scholar] [CrossRef] [PubMed]
- Eusebi, L.H.; Telese, A.; Marasco, G.; Bazzoli, F.; Zagari, R.M. Gastric cancer prevention strategies: A global perspective. J. Gastroenterol. Hepatol. 2020, 35, 1495–1502. [Google Scholar] [CrossRef] [PubMed]
- Landgren, A.M.; Landgren, O.; Gridley, G.; Dores, G.M.; Linet, M.S.; Morton, L.M. Autoimmune disease and subsequent risk of developing alimentary tract cancers among 4.5 million US male veterans. Cancer 2011, 117, 1163–1171. [Google Scholar] [CrossRef] [PubMed]
- Correa, P.; Piazuelo, M.B. The gastric precancerous cascade. J. Dig. Dis. 2012, 13, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Rugge, M.; Savarino, E.; Sbaraglia, M.; Bricca, L.; Malfertheiner, P. Gastritis: The clinico-pathological spectrum. Dig. Liver Dis. 2021, 53, 1237–1246. [Google Scholar] [CrossRef] [PubMed]
- Parsons, B.N.; Ijaz, U.Z.; D’Amore, R.; Burkitt, M.D.; Eccles, R.; Lenzi, L.; Duckworth, C.A.; Moore, A.R.; Tiszlavicz, L.; Varro, A.; et al. Comparison of the human gastric microbiota in hypochlorhydric states arising as a result of Helicobacter pylori-induced atrophic gastritis, autoimmune atrophic gastritis and proton pump inhibitor use. PLoS Pathog. 2017, 13, e1006653. [Google Scholar] [CrossRef] [PubMed]
- Petersen, C.P.; Weis, V.G.; Nam, K.T.; Sousa, J.F.; Fingleton, B.; Goldenring, J.R. Macrophages promote progression of spasmolytic polypeptide-expressing metaplasia after acute loss of parietal cells. Gastroenterology 2014, 146, 1727–1738.e1728. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.; Choi, E.; Petersen, C.P.; Roland, J.T.; Federico, A.; Ippolito, R.; D’Armiento, F.P.; Nardone, G.; Nagano, O.; Saya, H.; et al. Distinct metaplastic and inflammatory phenotypes in autoimmune and adenocarcinoma-associated chronic atrophic gastritis. United Eur. Gastroenterol. J. 2017, 5, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Goldenring, J. No H. pylori, no adenocarcinoma for patients with autoimmune gastritis. Gut 2023, 72, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Haruma, K.; Ito, M. Review article: Clinical significance of mucosal-protective agents: Acid, inflammation, carcinogenesis and rebamipide. Aliment. Pharmacol. Ther. 2003, 18 (Suppl. S1), 153–159. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M. Gastrointestinal hormones and regulation of gastric emptying. Curr. Opin. Endocrinol. Diabetes Obes. 2019, 26, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.J.; Wu, E. The role of gut microbiota in immune homeostasis and autoimmunity. Gut Microbes 2012, 3, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Annibale, B. Pernicious anemia: New insights from a gastroenterological point of view. World J. Gastroenterol. 2009, 15, 5121–5128. [Google Scholar] [CrossRef] [PubMed]
- ASGE Standards of Practice Committee; Evans, J.A.; Chandrasekhara, V.; Chathadi, K.V.; Decker, G.A.; Early, D.S.; Fisher, D.A.; Foley, K.; Hwang, J.H.; Jue, T.L.; et al. The role of endoscopy in the management of premalignant and malignant conditions of the stomach. Gastrointest. Endosc. 2015, 82, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bisschops, R.; Areia, M.; Coron, E.; Dobru, D.; Kaskas, B.; Kuvaev, R.; Pech, O.; Ragunath, K.; Weusten, B.; Familiari, P.; et al. Performance measures for upper gastrointestinal endoscopy: A European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative. Endoscopy 2016, 48, 843–864. [Google Scholar] [CrossRef] [PubMed]
- Venerito, M.; Link, A.; Rokkas, T.; Malfertheiner, P. Gastric cancer—Clinical and epidemiological aspects. Helicobacter 2016, 21 (Suppl. 1), 39–44. [Google Scholar] [CrossRef] [PubMed]
- Deprez, P.H.; Moons, L.M.G.; O’Toole, D.; Gincul, R.; Seicean, A.; Pimentel-Nunes, P.; Fernández-Esparrach, G.; Polkowski, M.; Vieth, M.; Borbath, I.; et al. Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2022, 54, 412–429. [Google Scholar] [CrossRef] [PubMed]
- Boyce, M.; Moore, A.R.; Sagatun, L.; Parsons, B.N.; Varro, A.; Campbell, F.; Fossmark, R.; Waldum, H.L.; Pritchard, D.M. Netazepide, a gastrin/cholecystokinin-2 receptor antagonist, can eradicate gastric neuroendocrine tumours in patients with autoimmune chronic atrophic gastritis. Br. J. Clin. Pharmacol. 2017, 83, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Fossmark, R.; Sordal, O.; Jianu, C.S.; Qvigstad, G.; Nordrum, I.S.; Boyce, M.; Waldum, H.L. Treatment of gastric carcinoids type 1 with the gastrin receptor antagonist netazepide (YF476) results in regression of tumours and normalisation of serum chromogranin A. Aliment. Pharmacol. Ther. 2012, 36, 1067–1075. [Google Scholar] [CrossRef] [PubMed]
- Massironi, S.; Zilli, A.; Fanetti, I.; Ciafardini, C.; Conte, D.; Peracchi, M. Intermittent treatment of recurrent type-1 gastric carcinoids with somatostatin analogues in patients with chronic autoimmune atrophic gastritis. Dig. Liver Dis. 2015, 47, 978–983. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| References | Finding |
|---|---|
| Iwamuro M, Curr Issues Mol Biol 2023 [16] | Helicobacter pylori may play a role in the induction/exacerbation of AAG. |
| Miceli E, Am J Gastroenterol 2023 [20] | The annual rate of progression of 10.9% from “potential” to “overt” AAG would suggest that anti-parietal cell antibodies are a true marker of “potential” AAG in patients without corpus atrophy. |
| Guo X, J Clin Med 2023 [21] | Anti-parietal cell antibodies, serum gastrin, PGI/PGII ratio, and vitamin B12 can be useful to identify patients with AAG among those with precancerous conditions, i.e., atrophic gastritis and intestinal metaplasia. |
| Singh S, Cureus 2023 [22] | Patients with AAG are often asymptomatic, but they can refer dyspeptic or reflux symptoms. |
| Conti L, Microorganisms 2020 [23] | Hypochloridria results in alteration of composition of gastric microbiota and patients with AAG have higher microbial diversity. |
| Miceli E, Dig Liv Dis 2023 [24] | Atrophic autoimmune gastritis can be linked to infertility, recurrent miscarriage, congenital abnormalities, and several obstetric complications. |
| Rugge M, GUT 2023 [25] | In patients with AAG, the cumulative incidence of type 1 neuroendocrine tumors (NETs) is 4.7% at 2 years of follow-up. |
| Dilaghi E, Am J Gastroenterol 2023 [26] | The incidence rate of gastric cancer/high grade dysplasia is 0.5% per person/year; risk factors for gastric cancer are age >60 years, intestinal metaplasia with absence of pseudopyloric metaplasia, pernicious anemia. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castellana, C.; Eusebi, L.H.; Dajti, E.; Iascone, V.; Vestito, A.; Fusaroli, P.; Fuccio, L.; D’Errico, A.; Zagari, R.M. Autoimmune Atrophic Gastritis: A Clinical Review. Cancers 2024, 16, 1310. https://doi.org/10.3390/cancers16071310
Castellana C, Eusebi LH, Dajti E, Iascone V, Vestito A, Fusaroli P, Fuccio L, D’Errico A, Zagari RM. Autoimmune Atrophic Gastritis: A Clinical Review. Cancers. 2024; 16(7):1310. https://doi.org/10.3390/cancers16071310
Chicago/Turabian StyleCastellana, Chiara, Leonardo Henry Eusebi, Elton Dajti, Veronica Iascone, Amanda Vestito, Pietro Fusaroli, Lorenzo Fuccio, Antonietta D’Errico, and Rocco Maurizio Zagari. 2024. "Autoimmune Atrophic Gastritis: A Clinical Review" Cancers 16, no. 7: 1310. https://doi.org/10.3390/cancers16071310
APA StyleCastellana, C., Eusebi, L. H., Dajti, E., Iascone, V., Vestito, A., Fusaroli, P., Fuccio, L., D’Errico, A., & Zagari, R. M. (2024). Autoimmune Atrophic Gastritis: A Clinical Review. Cancers, 16(7), 1310. https://doi.org/10.3390/cancers16071310