
Quality of Life, Sarcopenia and Nutritional Status in Patients with Esophagogastric Tumors before and after Neoadjuvant Therapy

 , , ,
, , ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design and Study Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
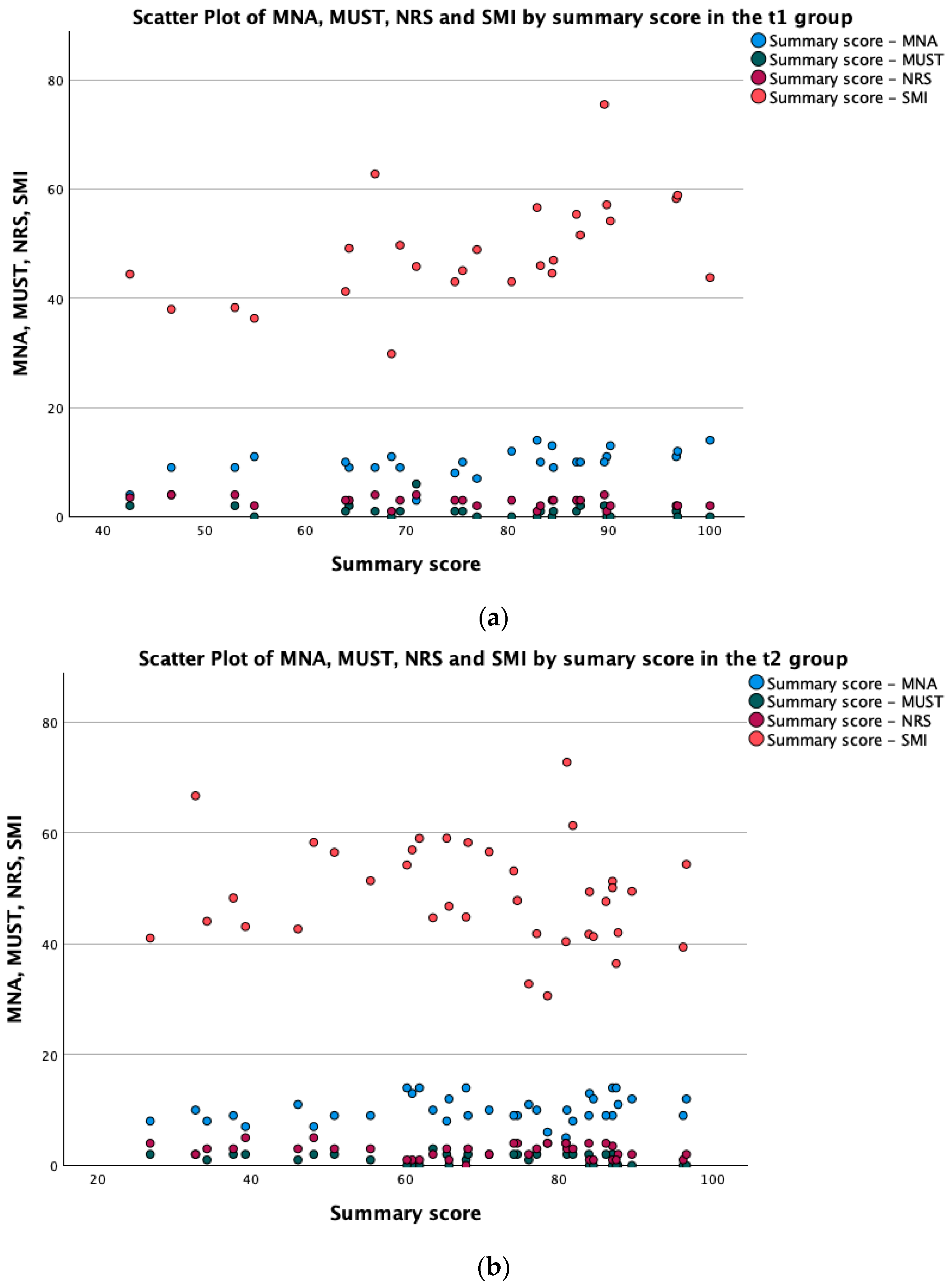
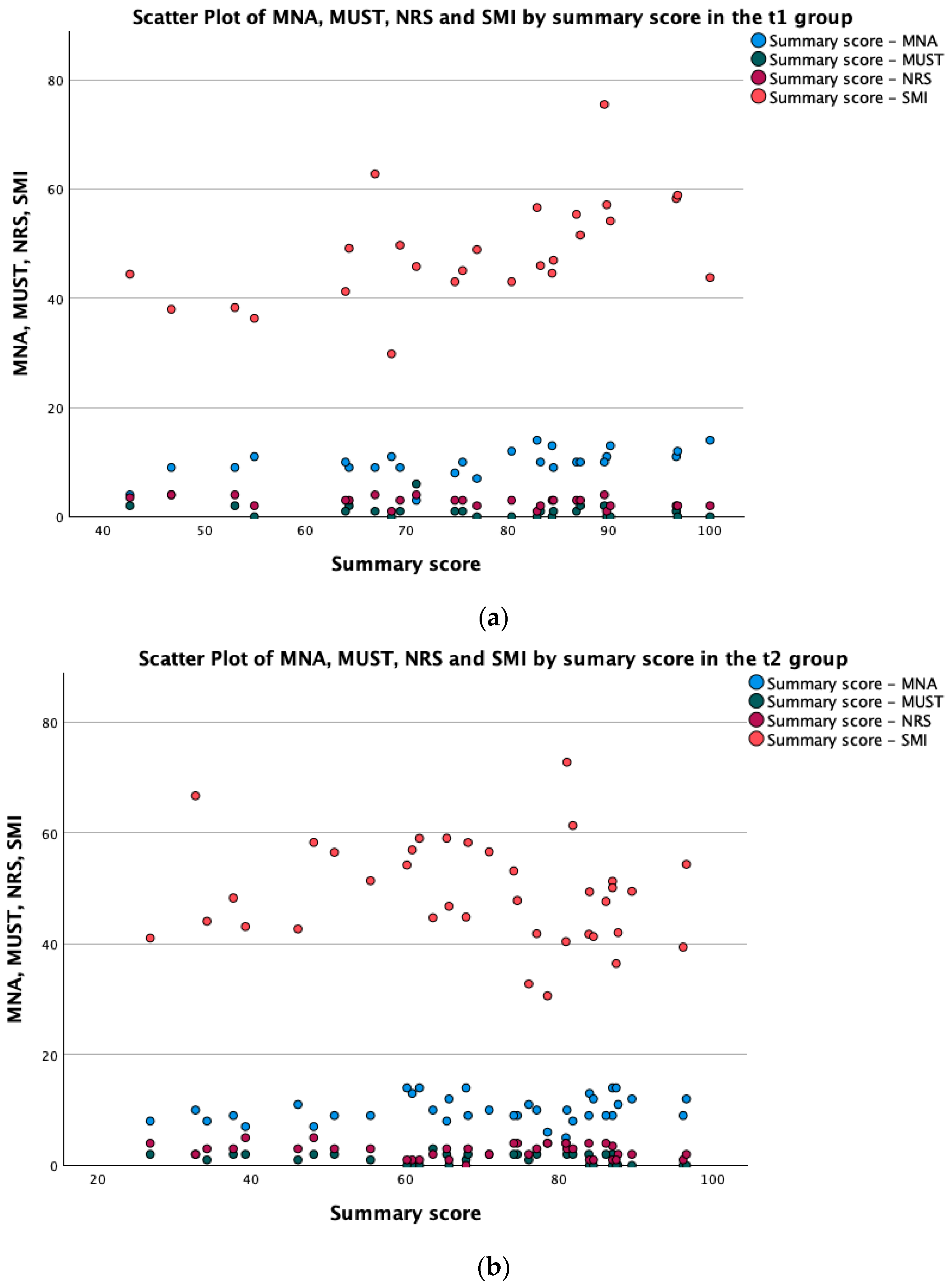
3.1. Nutritional Scores
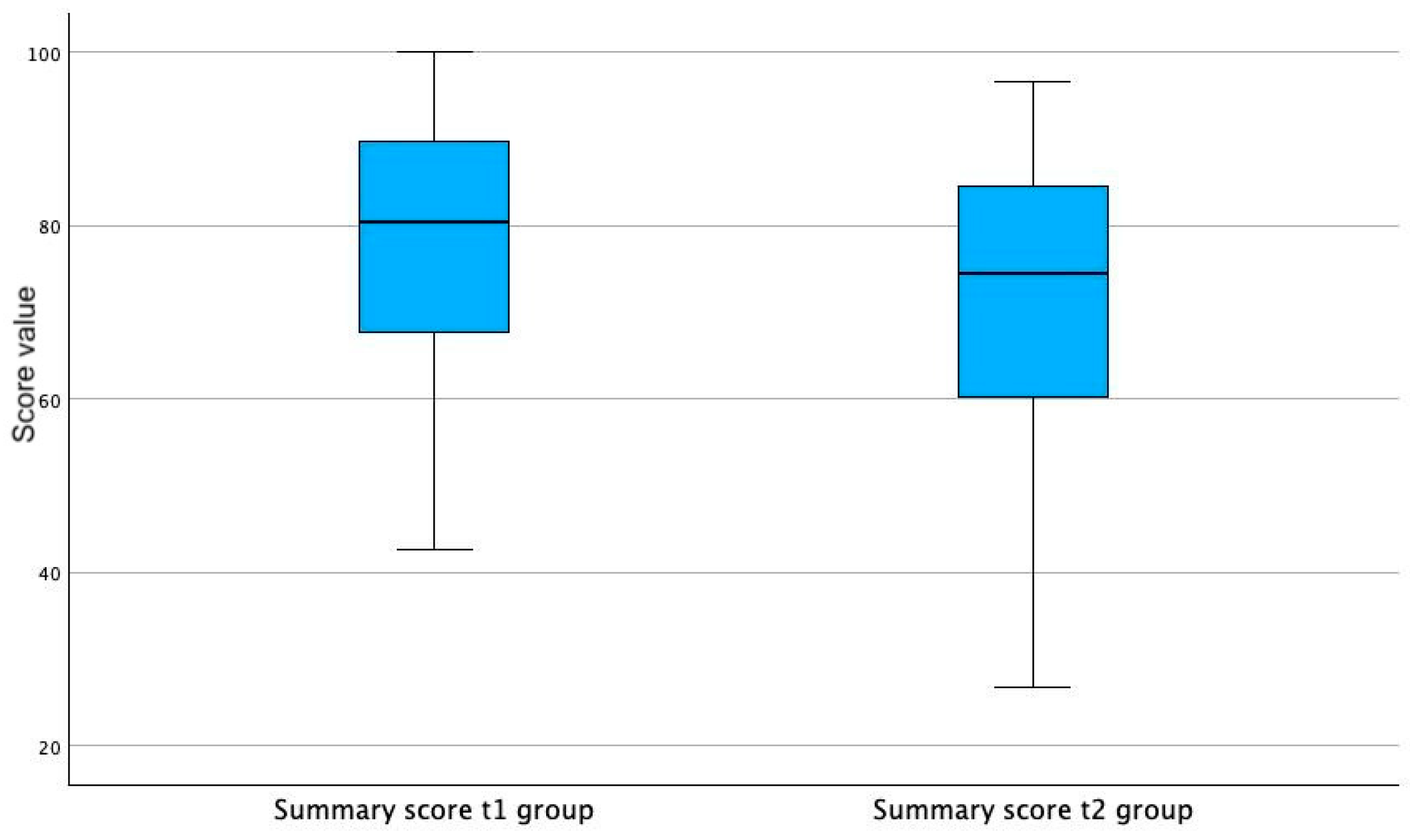
3.2. HRQoL Summary Score
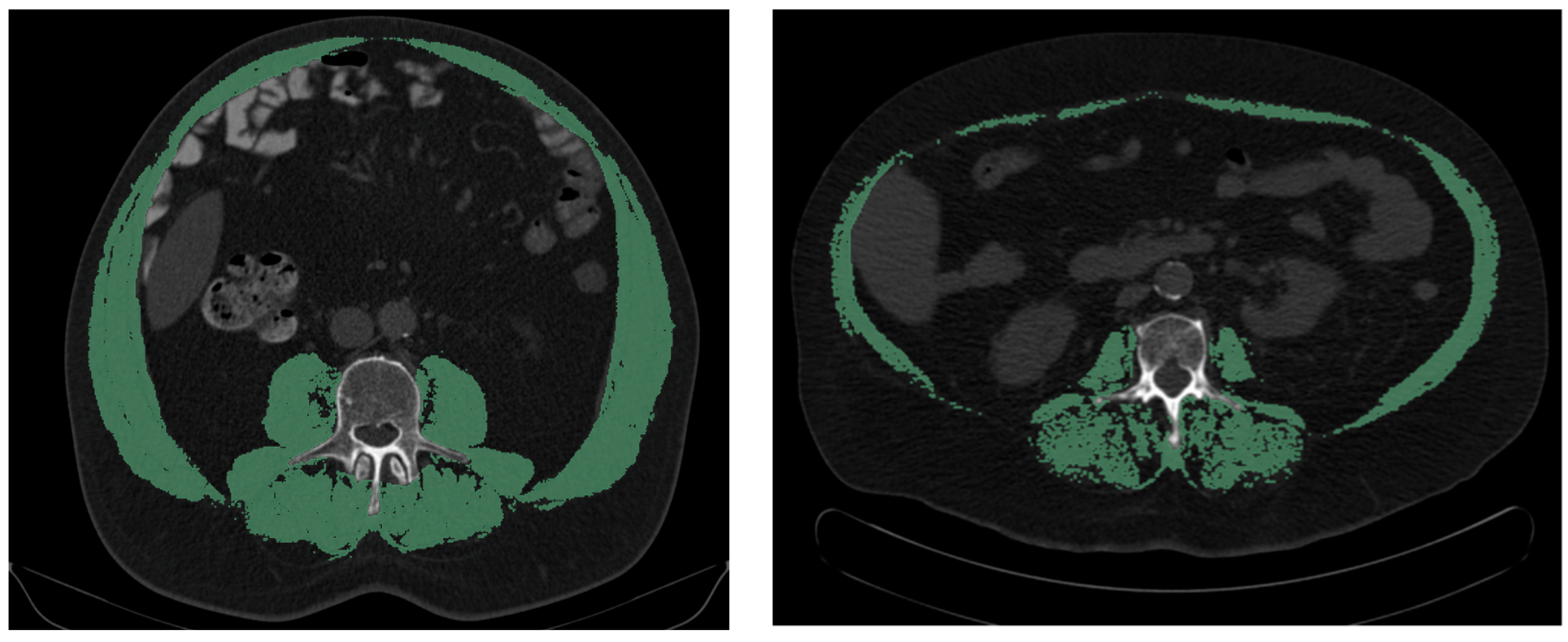
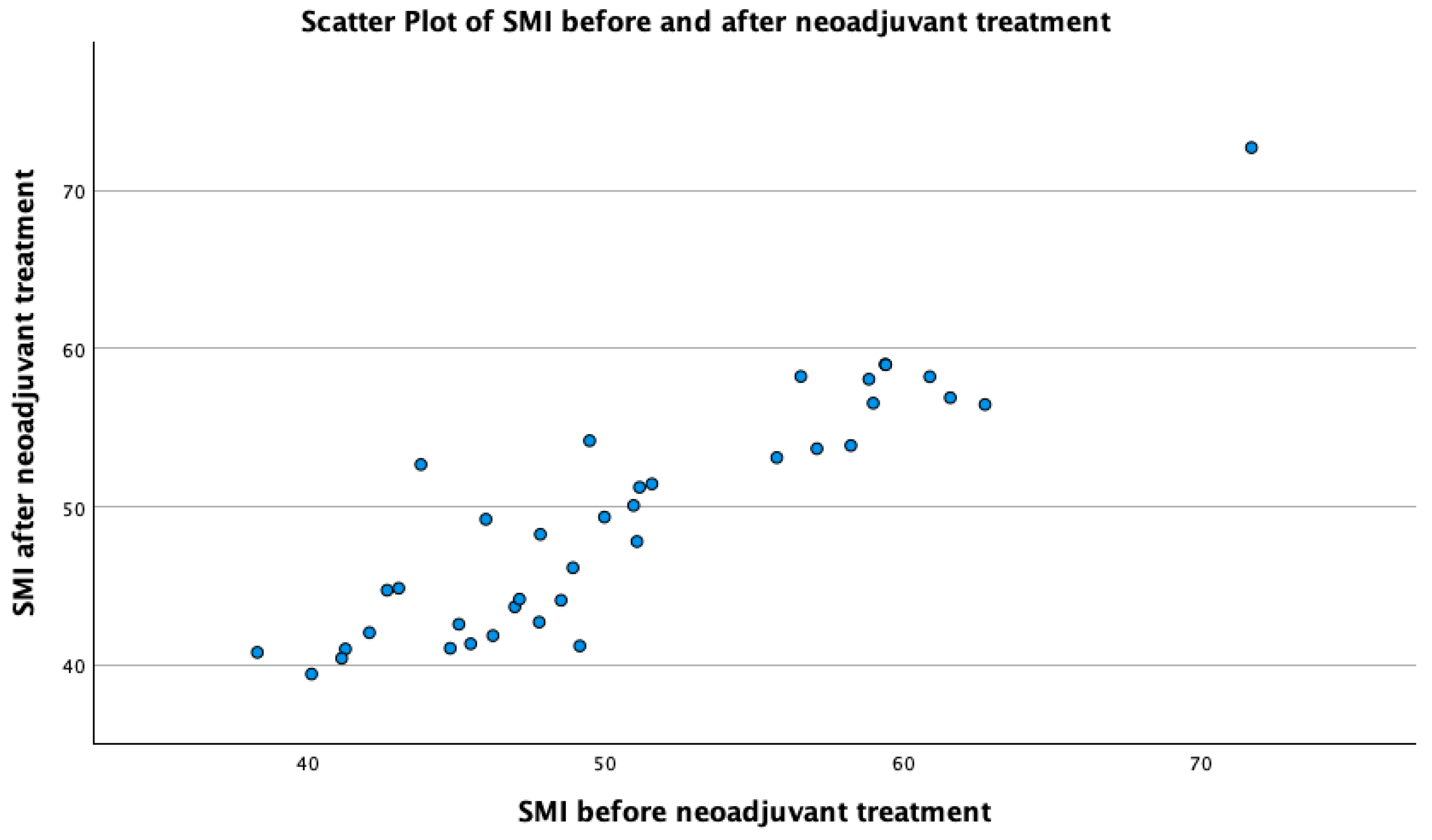
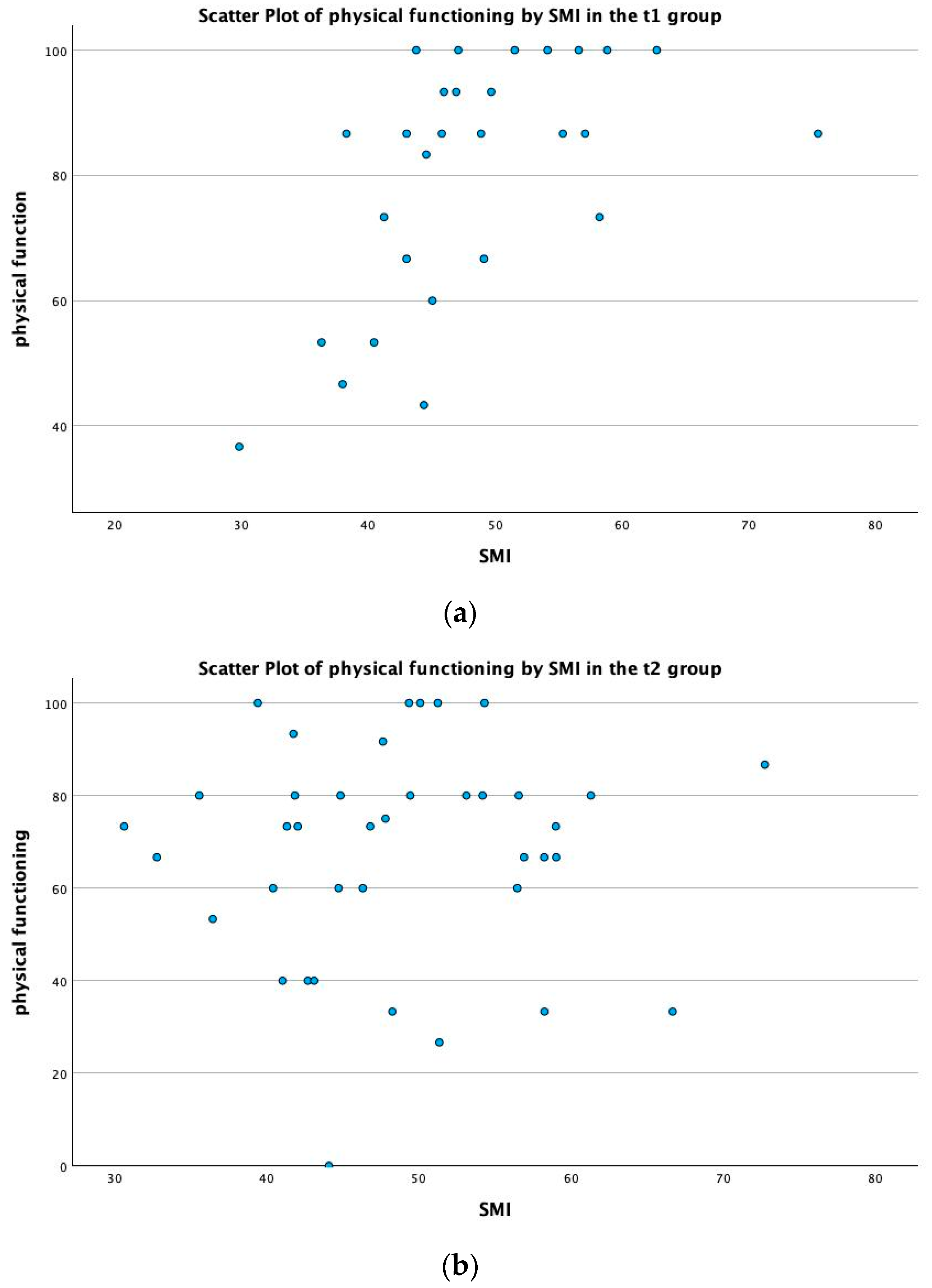
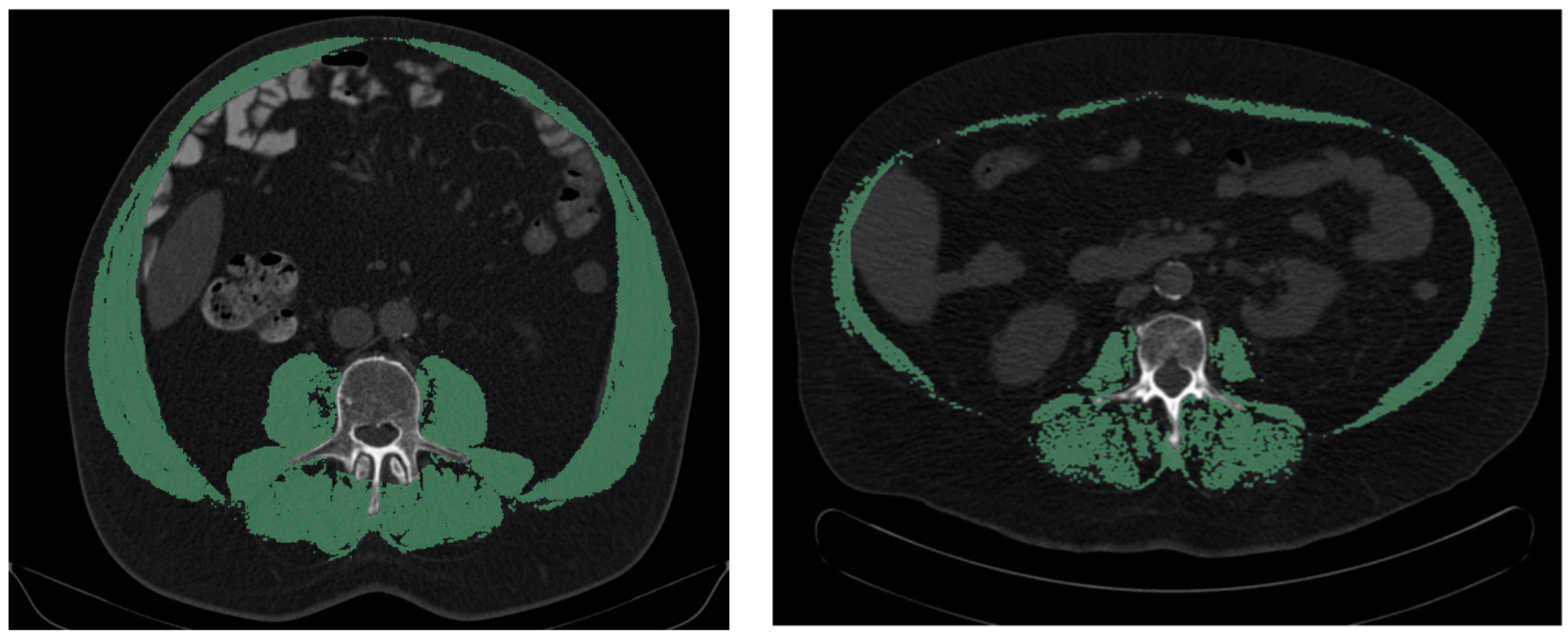
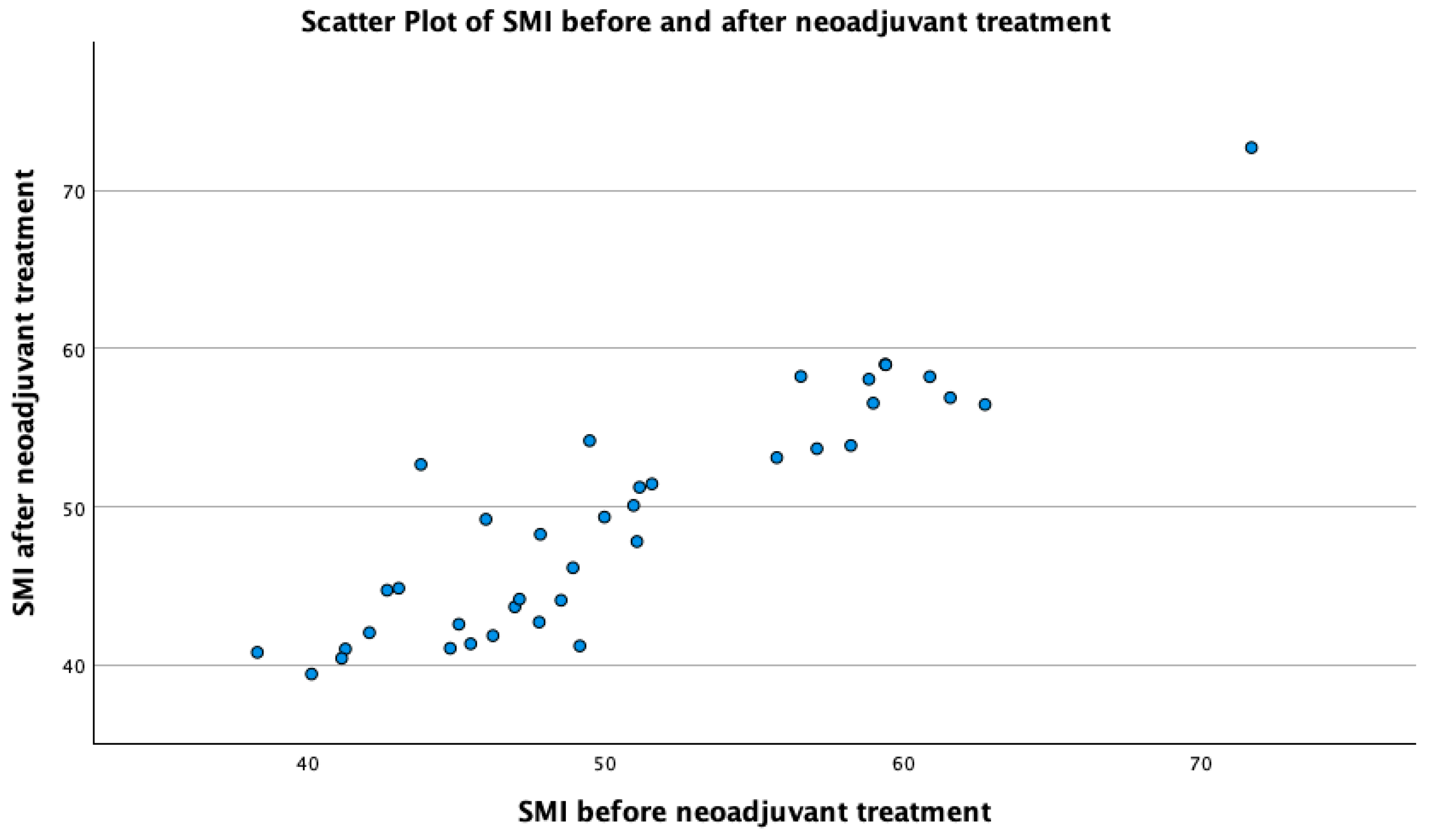
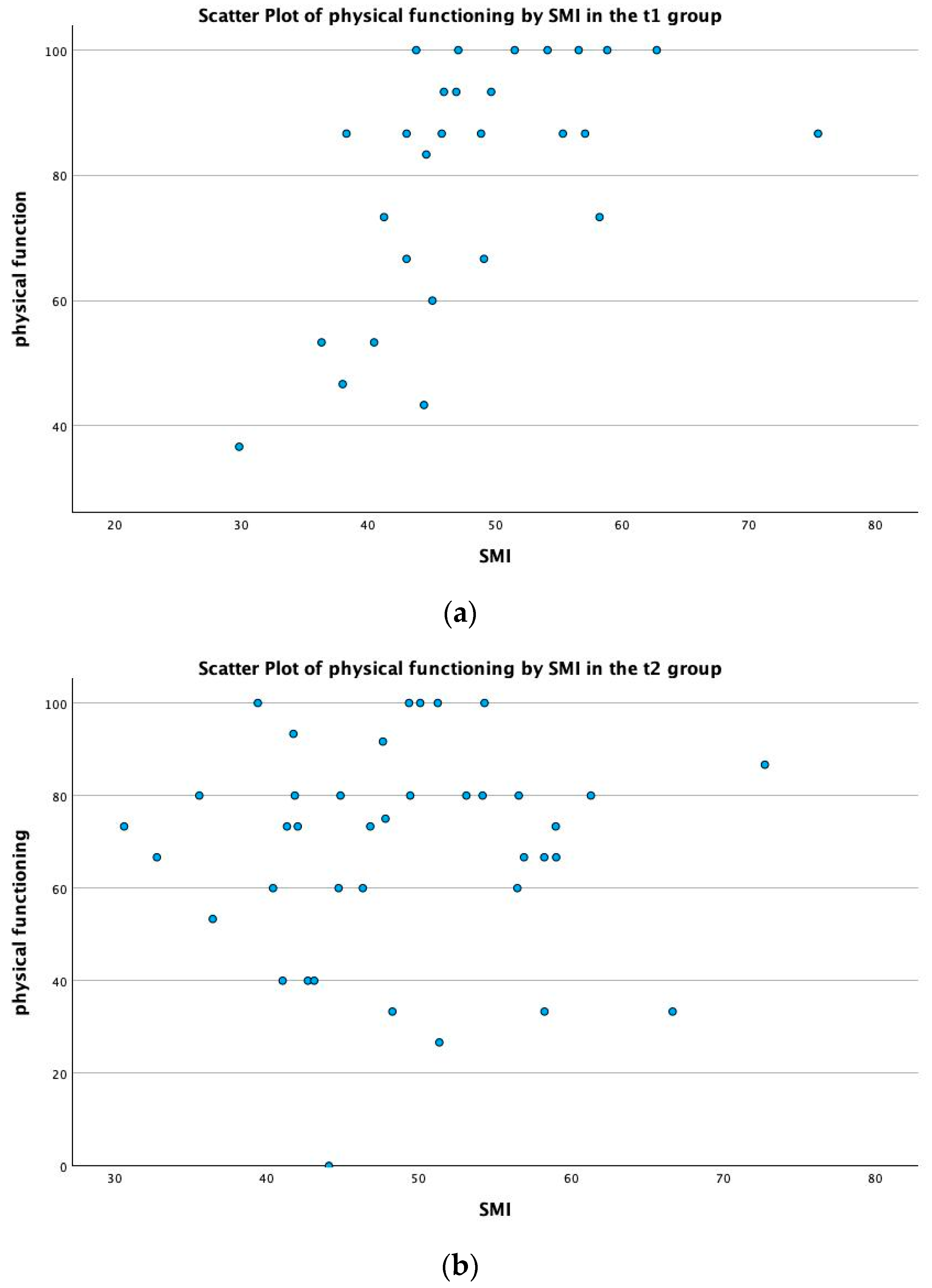
3.3. Skeletal Muscle Index
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Cancer Research Fund International. Worldwide Cancer Data. Available online: https://www.wcrf.org/cancer-trends/worldwide-cancer-data/ (accessed on 27 February 2023).
- Zentrum für Krebsregisterdaten. Available online: www.krebsdaten.de/abfrage (accessed on 27 February 2023).
- Robert Koch-Institut. Krebs in Deutschland für 2017/2018. 2021. Available online: https://edoc.rki.de/bitstream/handle/176904/9042/krebs_in_deutschland_2021.pdf%3bjsessionid%3d3B7086E853920E599859A5232A68DFA9.pdf (accessed on 27 February 2023).
- Arnold, M.R.M.; Lam, F.; Bray, F.; Ervik, M. Soerjomataram I ICBP SURVMARK-2 Online Tool: International Cancer Survival Benchmarking. Lyon, France: International Agency for Research on Cancer. 2019. Available online: http://gco.iarc.fr/survival/survmark (accessed on 31 January 2022).
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 177–180. [Google Scholar] [CrossRef]
- Rolland, Y.; Abellan van Kann, G.; Gillette-Guyonnet, S.; Vellas, B. Cachexia versus sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 15–21. [Google Scholar] [CrossRef] [PubMed]
- EORTC. Quality of Life. Available online: https://qol.eortc.org/quality-of-life/ (accessed on 13 March 2024).
- Rogers, S.N.; Waylen, A.E.; Thomas, S.; Penfold, C.; Pring, M.; Waterboer, T.; Pawlita, M.; Hurley, K.; Ness, A.R. Quality of life, cognitive, physical and emotional function at diagnosis predicts head and neck cancer survival: Analysis of cases from the Head and Neck 5000 study. Eur. Arch. Otorhinolaryngol. 2020, 277, 1515–1523. [Google Scholar] [CrossRef] [PubMed]
- Golzy, M.; Rosen, G.H.; Kruse, R.L.; Hooshmand, K.; Mehr, D.R.; Murray, K.S. Holistic Assessment of Quality of Life Predicts Survival in Older Patients with Bladder Cancer. Urology 2023, 174, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Westhofen, T.; Eismann, L.; Buchner, A.; Schlenker, B.; Giessen-Jung, C.; Becker, A.; Stief, C.G.; Kretschmer, A. Baseline Health-related Quality of Life Predicts Bladder Cancer-specific Survival Following Radical Cystectomy. Eur. Urol. Focus 2022, 8, 1659–1665. [Google Scholar] [CrossRef] [PubMed]
- Roncolato, F.T.; Gibbs, E.; Lee, C.K.; Asher, R.; Davies, L.C.; Gebski, V.J.; Friedlander, M.; Hilpert, F.; Wenzel, L.; Stockler, M.R.; et al. Quality of life predicts overall survival in women with platinum-resistant ovarian cancer: An AURELIA substudy. Ann. Oncol. 2017, 28, 1849–1855. [Google Scholar] [CrossRef] [PubMed]
- Pompili, C.; McLennan Battleday, F.; Chia, W.L.; Chaudhuri, N.; Kefaloyannis, E.; Milton, R.; Papagiannopoulos, K.; Tcherveniakov, P.; Brunelli, A. Poor preoperative quality of life predicts prolonged hospital stay after VATS lobectomy for lung cancer. Eur. J. Cardiothorac. Surg. 2021, 59, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Landgrebe, M.; Tobberup, R.; Carus, A.; Rasmussen, H.H. GLIM diagnosed malnutrition predicts clinical outcomes and quality of life in patients with non-small cell lung cancer. Clin. Nutr. 2023, 42, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Chen, A.; Xie, F.; Li, X.; Hu, G.; Lin, G. Low prognostic nutrition index predicts poorer quality of life in late-stage lung cancer. Ann. Palliat. Med. 2020, 9, 3976–3984. [Google Scholar] [CrossRef]
- Mito, M.; Sakata, J.; Hirose, Y.; Abe, S.; Saito, S.; Miura, Y.; Ishikawa, H.; Miura, K.; Takizawa, K.; Ichikawa, H.; et al. Preoperative controlling nutritional status score predicts systemic disease recurrence in patients with resectable biliary tract cancer. Eur. J. Surg. Oncol. 2023, 49, 399–409. [Google Scholar] [CrossRef]
- Shoji, F.; Haratake, N.; Akamine, T.; Takamori, S.; Katsura, M.; Takada, K.; Toyokawa, G.; Okamoto, T.; Maehara, Y. The Preoperative Controlling Nutritional Status Score Predicts Survival After Curative Surgery in Patients with Pathological Stage I Non-small Cell Lung Cancer. Anticancer Res. 2017, 37, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Wolf, J.H.; Ahuja, V.; D’Adamo, C.R.; Coleman, J.; Katlic, M.; Blumberg, D. Preoperative Nutritional Status Predicts Major Morbidity After Primary Rectal Cancer Resection. J. Surg. Res. 2020, 255, 325–331. [Google Scholar] [CrossRef]
- Mascarella, M.A.; Ferdus, J.; Vendra, V.; Sridharan, S.; Sultanem, K.; Tsien, C.; Shenouda, G.; Bouganim, N.; Esfahani, K.; Richardson, K.; et al. Sarcopenia predicts short-term treatment-related toxicity in patients undergoing curative-intent therapy for head and neck cancer: A systematic review and meta-analysis. Head Neck 2024. [Google Scholar] [CrossRef]
- Li, Z.Z.; Yan, X.L.; Jiang, H.J.; Ke, H.W.; Chen, Z.T.; Chen, D.H.; Xu, J.Y.; Liu, X.C.; Shen, X.; Huang, D.D. Sarcopenia predicts postoperative complications and survival in colorectal cancer patients with GLIM-defined malnutrition: Analysis from a prospective cohort study. Eur. J. Surg. Oncol. 2024, 50, 107295. [Google Scholar] [CrossRef] [PubMed]
- Troschel, F.M.; Jin, Q.; Eichhorn, F.; Muley, T.; Best, T.D.; Leppelmann, K.S.; Yang, C.J.; Troschel, A.S.; Winter, H.; Heussel, C.P.; et al. Sarcopenia on preoperative chest computed tomography predicts cancer-specific and all-cause mortality following pneumonectomy for lung cancer: A multicenter analysis. Cancer Med. 2021, 10, 6677–6686. [Google Scholar] [CrossRef] [PubMed]
- Trejo-Avila, M.; Bozada-Gutierrez, K.; Valenzuela-Salazar, C.; Herrera-Esquivel, J.; Moreno-Portillo, M. Sarcopenia predicts worse postoperative outcomes and decreased survival rates in patients with colorectal cancer: A systematic review and meta-analysis. Int. J. Color. Dis. 2021, 36, 1077–1096. [Google Scholar] [CrossRef] [PubMed]
- Mayr, R.; Fritsche, H.M.; Zeman, F.; Reiffen, M.; Siebertz, L.; Niessen, C.; Pycha, A.; van Rhijn, B.W.G.; Burger, M.; Gierth, M. Sarcopenia predicts 90-day mortality and postoperative complications after radical cystectomy for bladder cancer. World J. Urol. 2018, 36, 1201–1207. [Google Scholar] [CrossRef]
- Antoun, S.; Morel, H.; Souquet, P.J.; Surmont, V.; Planchard, D.; Bonnetain, F.; Foucher, P.; Egenod, T.; Krakowski, I.; Gaudin, H.; et al. Staging of nutrition disorders in non-small-cell lung cancer patients: Utility of skeletal muscle mass assessment. J. Cachexia Sarcopenia Muscle 2019, 10, 782–793. [Google Scholar] [CrossRef]
- Nipp, R.D.; Fuchs, G.; El-Jawahri, A.; Mario, J.; Troschel, F.M.; Greer, J.A.; Gallagher, E.R.; Jackson, V.A.; Kambadakone, A.; Hong, T.S.; et al. Sarcopenia Is Associated with Quality of Life and Depression in Patients with Advanced Cancer. Oncologist 2018, 23, 97–104. [Google Scholar] [CrossRef]
- Fuchs, H.; Holscher, A.H.; Leers, J.; Bludau, M.; Brinkmann, S.; Schroder, W.; Alakus, H.; Monig, S.; Gutschow, C.A. Long-term quality of life after surgery for adenocarcinoma of the esophagogastric junction: Extended gastrectomy or transthoracic esophagectomy? Gastric Cancer 2016, 19, 312–317. [Google Scholar] [CrossRef]
- Talagala, I.A.; Arambepola, C. Changes in quality of life following initial treatment of oesophageal carcinoma: A cohort study from Sri Lanka. BMC Cancer 2018, 18, 1184. [Google Scholar] [CrossRef]
- Sunde, B.; Lindblad, M.; Malmstrom, M.; Hedberg, J.; Lagergren, P.; Nilsson, M. Health-related quality of life one year after the diagnosis of oesophageal cancer: A population-based study from the Swedish National Registry for Oesophageal and Gastric Cancer. BMC Cancer 2021, 21, 1277. [Google Scholar] [CrossRef]
- Husson, O.; de Rooij, B.H.; Kieffer, J.; Oerlemans, S.; Mols, F.; Aaronson, N.K.; van der Graaf, W.T.A.; van de Poll-Franse, L.V. The EORTC QLQ-C30 Summary Score as Prognostic Factor for Survival of Patients with Cancer in the “Real-World”: Results from the Population-Based PROFILES Registry. Oncologist 2020, 25, e722–e732. [Google Scholar] [CrossRef]
- Van Kleef, J.J.; Dijksterhuis, W.P.M.; van den Boorn, H.G.; Prins, M.; Verhoeven, R.H.A.; Gisbertz, S.S.; Slingerland, M.; Mohammad, N.H.; Creemers, G.J.; Neelis, K.J.; et al. Prognostic value of patient-reported quality of life for survival in oesophagogastric cancer: Analysis from the population-based POCOP study. Gastric Cancer 2021, 24, 1203–1212. [Google Scholar] [CrossRef]
- Husson, O.; Mols, F.; Ezendam, N.P.; Schep, G.; van de Poll-Franse, L.V. Health-related quality of life is associated with physical activity levels among colorectal cancer survivors: A longitudinal, 3-year study of the PROFILES registry. J. Cancer Surviv. 2015, 9, 472–480. [Google Scholar] [CrossRef]
- Kawamura, T.; Makuuchi, R.; Tokunaga, M.; Tanizawa, Y.; Bando, E.; Yasui, H.; Aoyama, T.; Inano, T.; Terashima, M. Long-Term Outcomes of Gastric Cancer Patients with Preoperative Sarcopenia. Ann. Surg. Oncol. 2018, 25, 1625–1632. [Google Scholar] [CrossRef]
- Huang, D.D.; Cai, H.Y.; Chen, X.Y.; Dong, W.X.; Wangchuk, D.; Yan, J.Y.; Chen, X.L.; Dong, Q.T. Value of Sarcopenia defined by the new EWGSOP2 consensus for the prediction of Postoperative Complications and Long-term Survival after Radical Gastrectomy for Gastric Cancer: A comparison with four common nutritional screening tools. J. Cancer 2020, 11, 5852–5860. [Google Scholar] [CrossRef]
- Hacker, U.T.; Hasenclever, D.; Linder, N.; Stocker, G.; Chung, H.C.; Kang, Y.K.; Moehler, M.; Busse, H.; Lordick, F. Prognostic role of body composition parameters in gastric/gastroesophageal junction cancer patients from the EXPAND trial. J. Cachexia Sarcopenia Muscle 2020, 11, 135–144. [Google Scholar] [CrossRef]
- Huang, D.D.; Chen, X.X.; Chen, X.Y.; Wang, S.L.; Shen, X.; Chen, X.L.; Yu, Z.; Zhuang, C.L. Sarcopenia predicts 1-year mortality in elderly patients undergoing curative gastrectomy for gastric cancer: A prospective study. J. Cancer Res. Clin. Oncol. 2016, 142, 2347–2356. [Google Scholar] [CrossRef] [PubMed]
- Borggreve, A.S.; den Boer, R.B.; van Boxel, G.I.; de Jong, P.A.; Veldhuis, W.B.; Steenhagen, E.; van Hillegersberg, R.; Ruurda, J.P. The Predictive Value of Low Muscle Mass as Measured on CT Scans for Postoperative Complications and Mortality in Gastric Cancer Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 199. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Han, S.H.; Kim, H.I. Detection of sarcopenic obesity and prediction of long-term survival in patients with gastric cancer using preoperative computed tomography and machine learning. J. Surg. Oncol. 2021, 124, 1347–1355. [Google Scholar] [CrossRef]
- Jogiat, U.M.; Baracos, V.; Turner, S.R.; Eurich, D.; Filafilo, H.; Rouhi, A.; Bedard, A.; Bedard, E.L.R. Changes in Sarcopenia Status Predict Survival among Patients with Resectable Esophageal Cancer. Ann. Surg. Oncol. 2023, 30, 7412–7421. [Google Scholar] [CrossRef]
- Srpcic, M.; Jordan, T.; Popuri, K.; Sok, M. Sarcopenia and myosteatosis at presentation adversely affect survival after esophagectomy for esophageal cancer. Radiol. Oncol. 2020, 54, 237–246. [Google Scholar] [CrossRef]
- Fukuda, Y.; Yamamoto, K.; Hirao, M.; Nishikawa, K.; Nagatsuma, Y.; Nakayama, T.; Tanikawa, S.; Maeda, S.; Uemura, M.; Miyake, M.; et al. Sarcopenia is associated with severe postoperative complications in elderly gastric cancer patients undergoing gastrectomy. Gastric Cancer 2016, 19, 986–993. [Google Scholar] [CrossRef]
- Fujihata, S.; Ogawa, R.; Nakaya, S.; Hayakawa, S.; Okubo, T.; Sagawa, H.; Tanaka, T.; Takahashi, H.; Matsuo, Y.; Takiguchi, S. The impact of skeletal muscle wasting during neoadjuvant chemotherapy on postoperative anastomotic leakage in patients with esophageal cancer. Esophagus 2020, 18, 258–266. [Google Scholar] [CrossRef]
- Figueroa-Giralt, M.; Araya, F.; Torrealba, A.; Weisz, J.; Lanzarini, E.; Musleh, M.; Molina, J.C.; Korn, O.; Braghetto, I.; Csendes, A. Tomographic Sarcopenia Predicts Anastomotic Leaks and Long-Term Survival in Gastric Cancer Patients Operated with Curative Intent. Arq. Bras. Cir. Dig. 2023, 36, e1723. [Google Scholar] [CrossRef]
- Matsui, R.; Inaki, N.; Tsuji, T.; Momosaki, R.; Fukunaga, T. Impact of Preoperative Handgrip Strength on Postoperative Outcome after Radical Gastrectomy for Gastric Cancer Patients. J. Clin. Med. 2022, 11, 7129. [Google Scholar] [CrossRef]
- Donlon, N.E.; Moran, B.; Kamilli, A.; Davern, M.; Sheppard, A.; King, S.; Donohoe, C.L.; Lowery, M.; Cunningham, M.; Ravi, N.; et al. CROSS Versus FLOT Regimens in Esophageal and Esophagogastric Junction Adenocarcinoma: A Propensity-Matched Comparison. Ann. Surg. 2022, 276, 792–798. [Google Scholar] [CrossRef]
- Tribolet, P.; Kaegi-Braun, N.; Gressies, C.; Baumgartner, A.; Wagner, K.H.; Stanga, Z.; Schuetz, P. Handgrip Strength Values Depend on Tumor Entity and Predict 180-Day Mortality in Malnourished Cancer Patients. Nutrients 2022, 14, 2173. [Google Scholar] [CrossRef]
- Barbosa, M.V.; Dos Santos, M.P.; Leite, J.A.; Rodrigues, V.D.; de Pinho, N.B.; Martucci, R.B. Association between functional aspects and health-related quality of life in patients with colorectal cancer: Can handgrip strength be the measure of choice in clinical practice? Support. Care Cancer 2023, 31, 144. [Google Scholar] [CrossRef]
- Kizilirmak, A.S.; Karadibak, D.; Gultekin, S.C.; Ozsoy, I.; Yavuzsen, H.T.; Yavuzsen, T.; Oztop, I. Predictors of the 6-min walk test in patients with ovarian cancer. Support. Care Cancer 2023, 31, 248. [Google Scholar] [CrossRef]
- Naghashi, S.; Somi, M.H.; Nikniaz, Z. Pretreatment nutritional status is associated with quality of life in patients with gastric cancer: A cross-sectional study from Iran. Support. Care Cancer 2022, 30, 3313–3319. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Qiu, G.Q.; Bao, W.A.; Zhang, D.H. The prognostic role of nutrition risk score (NRS) in patients with metastatic or recurrent esophageal squamous cell carcinoma (ESCC). Oncotarget 2017, 8, 77465–77473. [Google Scholar] [CrossRef]
- Toyota, K.; Mori, M.; Hirahara, S.; Yoshioka, S.; Kubota, H.; Yano, R.; Kobayashi, H.; Hashimoto, Y.; Sakashita, Y.; Yokoyama, Y.; et al. Nutritional Status Indicators Affecting the Tolerability of Postoperative Chemotherapy After Total Gastrectomy in Patients With Gastric Cancer. J. Gastric Cancer 2022, 22, 56–66. [Google Scholar] [CrossRef]
- Suzuki, S.; Kanaji, S.; Yamamoto, M.; Oshikiri, T.; Nakamura, T.; Kakeji, Y. Controlling Nutritional Status (CONUT) Score Predicts Outcomes of Curative Resection for Gastric Cancer in the Elderly. World J. Surg. 2019, 43, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.S.; Zhao, Y.; Ma, F.Y.; Xuan, L.; Wu, S.K. Nutritional status predicts clinical outcomes in patients with gastric cancer undergoing radical gastrectomy. Zhonghua Yi Xue Za Zhi 2021, 101, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Qian, Y.; Liu, H.; Pan, J.; Yu, W.; Lv, J.; Yan, J.; Gao, J.; Wang, X.; Ge, X.; Zhou, W. Preoperative Controlling Nutritional Status (CONUT) score predicts short-term outcomes of patients with gastric cancer after laparoscopy-assisted radical gastrectomy. World J. Surg. Oncol. 2021, 19, 25. [Google Scholar] [CrossRef] [PubMed]
- Pirlich, M.; Schutz, T.; Norman, K.; Gastell, S.; Lubke, H.J.; Bischoff, S.C.; Bolder, U.; Frieling, T.; Guldenzoph, H.; Hahn, K.; et al. The German hospital malnutrition study. Clin. Nutr. 2006, 25, 563–572. [Google Scholar] [CrossRef]
- Cai, Y.; Chen, S.; Chen, X.; Chen, W.; Wang, P.; Zhu, G.; Jin, J. Association of Sarcopenia and Low Nutritional Status with Unplanned Hospital Readmission after Radical Gastrectomy in Patients with Gastric Cancer: A Case-Control Study. J. Healthc. Eng. 2022, 2022, 7246848. [Google Scholar] [CrossRef]
- Oberhoff, G.; Schooren, L.; Vondran, F.; Kroh, A.; Koch, A.; Bednarsch, J.; Neumann, U.P.; Schmitz, S.M.; Alizai, P.H. Impairment of Nutritional Status and Quality of Life Following Minimal-Invasive Esophagectomy-A Prospective Cohort Analysis. Cancers 2024, 16, 266. [Google Scholar] [CrossRef]
- Calomino, N.; Malerba, M.; Tanzini, G. Total gastrectomy and quality of life. Minerva Chir. 1998, 53, 135–140. [Google Scholar]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.; de Haes, J.C.J.M.; et al. The European Organisation for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Lagergren, P.; Fayers, P.; Conroy, T.; Stein, H.J.; Sezer, O.; Hardwick, R.; Hammerlid, E.; Bottomley, A.; Van Cutsem, E.; Blazeby, J.M. Clinical and Psychometric Validation of a Questionnaire Module, the EORTC QLQ-OG25, to Assess Health-Related Quality of Life in Patients with Cancer of the Oesophagus, the Oesophago-Gastric Junction and the Stomach. Eur. J. Cancer 2007, 43, 2066–2073. [Google Scholar] [CrossRef]
- Guigoz, Y. The Mini-Nutritional Assessment (MNA®) Review of the Literature—What does it tell us? J. Nutr. Health Aging 2006, 10, 466–487. [Google Scholar]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M. ESPEN guidelines for nutrition screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- EORTC. Scoring of the QLQ-C30 Summary Score. Available online: https://qol.eortc.org/app/uploads/sites/2/2018/02/scoring_of_the_qlq-c30_summary_score.pdf (accessed on 26 February 2023).
- Zhang, F.M.; Song, C.H.; Guo, Z.Q.; Yu, Z.; Weng, M.; Zhou, F.X.; Liu, M.; Cong, M.H.; Li, T.; Li, Z.N.; et al. Sarcopenia prevalence in patients with cancer and association with adverse prognosis: A nationwide survey on common cancers. Nutrition 2023, 114, 112107. [Google Scholar] [CrossRef]
- Liu, Y.Y.; Ruan, G.T.; Ge, Y.Z.; Li, Q.Q.; Zhang, Q.; Zhang, X.; Tang, M.; Song, M.M.; Zhang, X.W.; Li, X.R.; et al. Systemic inflammation with sarcopenia predicts survival in patients with gastric cancer. J. Cancer Res. Clin. Oncol. 2023, 149, 1249–1259. [Google Scholar] [CrossRef]
- Han, Y.; Wu, J.; Ji, R.; Tan, H.; Tian, S.; Yin, J.; Xu, J.; Chen, X.; Liu, W.; Cui, H. Preoperative sarcopenia combined with prognostic nutritional index predicts long-term prognosis of radical gastrectomy with advanced gastric cancer: A comprehensive analysis of two-center study. BMC Cancer 2023, 23, 751. [Google Scholar] [CrossRef] [PubMed]
- Tweed, T.T.T.; van der Veen, A.; Tummers, S.; van Dijk, D.P.J.; Luyer, M.D.P.; Ruurda, J.P.; van Hillegersberg, R.; Stoot, J.; LOGICA Study Group; Tegels, J.J.W.; et al. Body Composition Is a Predictor for Postoperative Complications After Gastrectomy for Gastric Cancer: A Prospective Side Study of the LOGICA Trial. J. Gastrointest. Surg. 2022, 26, 1373–1387. [Google Scholar] [CrossRef] [PubMed]
- Jogiat, U.M.; Sasewich, H.; Turner, S.R.; Baracos, V.; Eurich, D.T.; Filafilo, H.; Bedard, E.L.R. Sarcopenia Determined by Skeletal Muscle Index Predicts Overall Survival, Disease-free Survival, and Postoperative Complications in Resectable Esophageal Cancer: A Systematic Review and Meta-analysis. Ann. Surg. 2022, 276, e311–e318. [Google Scholar] [CrossRef] [PubMed]
- Zou, H.B.; Yan, X.L.; Dong, W.X.; Yu, D.Y.; Zhang, F.M.; Zhou, L.P.; Shen, Z.L.; Cai, G.J.; Zhuang, C.L.; Yu, Z. Sarcopenia is a predictive factor of poor quality of life and prognosis in patients after radical gastrectomy. Eur. J. Surg. Oncol. 2021, 47, 1976–1984. [Google Scholar] [CrossRef]
- Sato, K.; Kamiya, K.; Hamazaki, N.; Nozaki, K.; Ichikawa, T.; Uchida, S.; Ueno, K.; Yamashita, M.; Noda, T.; Ogura, K.; et al. Association of sarcopenia defined by different skeletal muscle mass measurements with prognosis and quality of life in older patients with heart failure. J. Cardiol. 2023. [Google Scholar] [CrossRef]
- Celoto, B.R.B.; Marin, F.A.; Spexoto, M.C.B. Assessment of the components of sarcopenia and quality of life perceived of individuals on hemodialysis. Rev. Bras. Enferm. 2023, 76, e20220677. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Yang, J.; Yu, H.; Bo, Z.; Chen, K.; Wang, D.; Xie, Y.; Wang, Y.; Chen, G. Effect of Sarcopenia on Survival and Health-Related Quality of Life in Patients with Hepatocellular Carcinoma after Hepatectomy. Cancers 2022, 14, 6144. [Google Scholar] [CrossRef] [PubMed]
- Seok, M.; Kim, W.; Kim, J. Machine Learning for Sarcopenia Prediction in the Elderly Using Socioeconomic, Infrastructure, and Quality-of-Life Data. Healthcare 2023, 11, 2881. [Google Scholar] [CrossRef] [PubMed]
- Palmela, C.; Velho, S.; Agostinho, L.; Branco, F.; Santos, M.; Santos, M.P.; Oliveira, M.H.; Strecht, J.; Maio, R.; Cravo, M.; et al. Body Composition as a Prognostic Factor of Neoadjuvant Chemotherapy Toxicity and Outcome in Patients with Locally Advanced Gastric Cancer. J. Gastric Cancer 2017, 17, 74–87. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.H.; Brammer, K.; Randhawa, N.; Welch, N.T.; Parsons, S.L.; James, E.J.; Catton, J.A. Sarcopenia is associated with toxicity in patients undergoing neo-adjuvant chemotherapy for oesophago-gastric cancer. Eur. J. Surg. Oncol. 2015, 41, 333–338. [Google Scholar] [CrossRef]
- Dalamaga, M. Interplay of adipokines and myokines in cancer pathophysiology: Emerging therapeutic implications. World J. Exp. Med. 2013, 3, 26–33. [Google Scholar] [CrossRef]
- Chou, Y.J.; Liou, Y.T.; Lai, S.R.; Tien, Y.W.; Kuo, H.J.; Yang, H.Y.; Shun, S.C. Role of preoperative malnutrition and symptom severity in anorexia-cachexia-related quality of life in patients with operable pancreatic cancer. Eur. J. Oncol. Nurs. 2023, 66, 102352. [Google Scholar] [CrossRef]
- Velasco, R.N., Jr.; Catedral, L.I.G.; Chua, A.V., Jr.; Hernandez, A.R.B.; King, R.E.C.; Leones, L.M.B.; Mondragon, K.A.M.; Ting, F.I.L.; Callueng, J.M.C.; Tampo, M.M.T.; et al. The Impact of Malnutrition on the Quality of Life of Colorectal Cancer Patients in a Tertiary Hospital. Nutr. Cancer 2022, 74, 2937–2945. [Google Scholar] [CrossRef]
- Gharagozlian, S.; Mala, T.; Brekke, H.K.; Kolbjornsen, L.C.; Ullerud, A.A.; Johnson, E. Nutritional status, sarcopenia, gastrointestinal symptoms and quality of life after gastrectomy for cancer—A cross-sectional pilot study. Clin. Nutr. ESPEN 2020, 37, 195–201. [Google Scholar] [CrossRef]
- Maia, F.C.P.; Silva, T.A.; Generoso, S.V.; Correia, M. Malnutrition is associated with poor health-related quality of life in surgical patients with gastrointestinal cancer. Nutrition 2020, 75–76, 110769. [Google Scholar] [CrossRef]
- Chen, F.F.; Zhang, F.Y.; Zhou, X.Y.; Shen, X.; Yu, Z.; Zhuang, C.L. Role of frailty and nutritional status in predicting complications following total gastrectomy with D2 lymphadenectomy in patients with gastric cancer: A prospective study. Langenbecks Arch. Surg. 2016, 401, 813–822. [Google Scholar] [CrossRef]
- Kurita, D.; Oguma, J.; Ishiyama, K.; Hirano, Y.; Kanamori, J.; Daiko, H. Handgrip Strength Predicts Postoperative Pneumonia After Thoracoscopic-Laparoscopic Esophagectomy for Patients with Esophageal Cancer. Ann. Surg. Oncol. 2020, 27, 3173–3181. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.Y.; Li, B.; Ma, B.W.; Zhang, X.Z.; Chen, W.Z.; Lu, L.S.; Shen, X.; Zhuang, C.L.; Yu, Z. Sarcopenia is an effective prognostic indicator of postoperative outcomes in laparoscopic-assisted gastrectomy. Eur. J. Surg. Oncol. 2019, 45, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Van Putten, M.; Husson, O.; Mols, F.; Luyer, M.D.P.; van de Poll-Franse, L.V.; Ezendam, N.P.M. Correlates of physical activity among colorectal cancer survivors: Results from the longitudinal population-based profiles registry. Support. Care Cancer 2016, 24, 573–583. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N (%) | Median (IQR) | Min | Max | ||
|---|---|---|---|---|---|
| Age | 65.0 (19.0) | 28.0 | 82.0 | ||
| Height in cm | 175.0 (10.0) | 147.0 | 194.0 | ||
| Weight in kg | 80.0 (18.4) | 38.0 | 141.0 | ||
| Tumor localization | EG junction | 41 (51.2) | |||
| esophageal | 19 (23.8) | ||||
| gastric | 20 (25.0) | ||||
| Sex | female | 14 (17.5) | |||
| male | 66 (82.5) | ||||
| ASA | ASA ≤ 2 | 22 (27.5) | |||
| ASA ≥ 3 | 58 (72.5) | ||||
| Weight loss in % | 6.6 (13.8) | 0.0 | 47.1 |
| N (%) | Median (IQR) | Min | Max | ||
|---|---|---|---|---|---|
| Physical performance (measured in number of floors patients were able to climb) | ≤1 | 6 (17.1) | |||
| 2–3 | 9 (25.7) | ||||
| >3 | 20 (57.1) | ||||
| SMI in cm2/m2 | 48.14 (13) | 29.8 | 75.5 | ||
| MNA | 0–7 | 4 (12.1) | |||
| 8–11 | 18 (54.6) | ||||
| 12–14 | 11 (33.3) | ||||
| Missing | 2 | ||||
| MUST | 0 | 15 (44.1) | |||
| 1 | 10 (29.4) | ||||
| ≥2 | 9 (26.5) | ||||
| Missing | 1 | ||||
| NRS | <3 | 15 (45.5) | |||
| ≥3 | 18 (54.5) | ||||
| Missing | 2 | ||||
| QL2 | 58.3 (25.0) | 25.0 | 100.0 | ||
| PF2 | 86.7 (33.3) | 33.3 | 100.0 | ||
| Sum | 80.4 (23.0) | 42.6 | 100.0 |
| N (%) | Median (IQR) | Min | Max | ||
|---|---|---|---|---|---|
| Physical performance (measured in number of floors patients were able to climb) | ≤1 | 11 (26.2) | |||
| 2–3 | 9 (21.4) | ||||
| >3 | 22 (52.4) | ||||
| Missing | 3 | ||||
| SMI in cm2/m2 | 47.7 (12.0) | 30.6 | 72.7 | ||
| MNA | 0–7 | 6 (14.3) | |||
| 8–11 | 24 (57.1) | ||||
| 12–14 | 12 (28.6) | ||||
| Missing | 3 | ||||
| MUST | 0 | 13 (31.0) | |||
| 1 | 5 (11.9) | ||||
| ≥2 | 24 (57.1) | ||||
| Missing | 3 | ||||
| NRS | <3 | 18 (43.9) | |||
| ≥3 | 23 (56.1) | ||||
| Missing | 4 | ||||
| QL2 | 50.0 (33.3) | 16.7 | 100.0 | ||
| PF2 | 73.3 (29.2) | 0.0 | 100.0 | ||
| Sum | 74.6 (27.0) | 26.8 | 97.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schooren, L.; Oberhoff, G.H.; Koch, A.; Kroh, A.; Ulmer, T.F.; Vondran, F.; Bednarsch, J.; Neumann, U.P.; Schmitz, S.M.; Alizai, P.H. Quality of Life, Sarcopenia and Nutritional Status in Patients with Esophagogastric Tumors before and after Neoadjuvant Therapy. Cancers 2024, 16, 1232. https://doi.org/10.3390/cancers16061232
Schooren L, Oberhoff GH, Koch A, Kroh A, Ulmer TF, Vondran F, Bednarsch J, Neumann UP, Schmitz SM, Alizai PH. Quality of Life, Sarcopenia and Nutritional Status in Patients with Esophagogastric Tumors before and after Neoadjuvant Therapy. Cancers. 2024; 16(6):1232. https://doi.org/10.3390/cancers16061232
Chicago/Turabian StyleSchooren, Lena, Grace H. Oberhoff, Alexander Koch, Andreas Kroh, Tom F. Ulmer, Florian Vondran, Jan Bednarsch, Ulf P. Neumann, Sophia M. Schmitz, and Patrick H. Alizai. 2024. "Quality of Life, Sarcopenia and Nutritional Status in Patients with Esophagogastric Tumors before and after Neoadjuvant Therapy" Cancers 16, no. 6: 1232. https://doi.org/10.3390/cancers16061232
APA StyleSchooren, L., Oberhoff, G. H., Koch, A., Kroh, A., Ulmer, T. F., Vondran, F., Bednarsch, J., Neumann, U. P., Schmitz, S. M., & Alizai, P. H. (2024). Quality of Life, Sarcopenia and Nutritional Status in Patients with Esophagogastric Tumors before and after Neoadjuvant Therapy. Cancers, 16(6), 1232. https://doi.org/10.3390/cancers16061232