

Mezigdomide—A Novel Cereblon E3 Ligase Modulator under Investigation in Relapsed/Refractory Multiple Myeloma


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
Current Treatment of Relapsed/Refractory MM (RRMM)
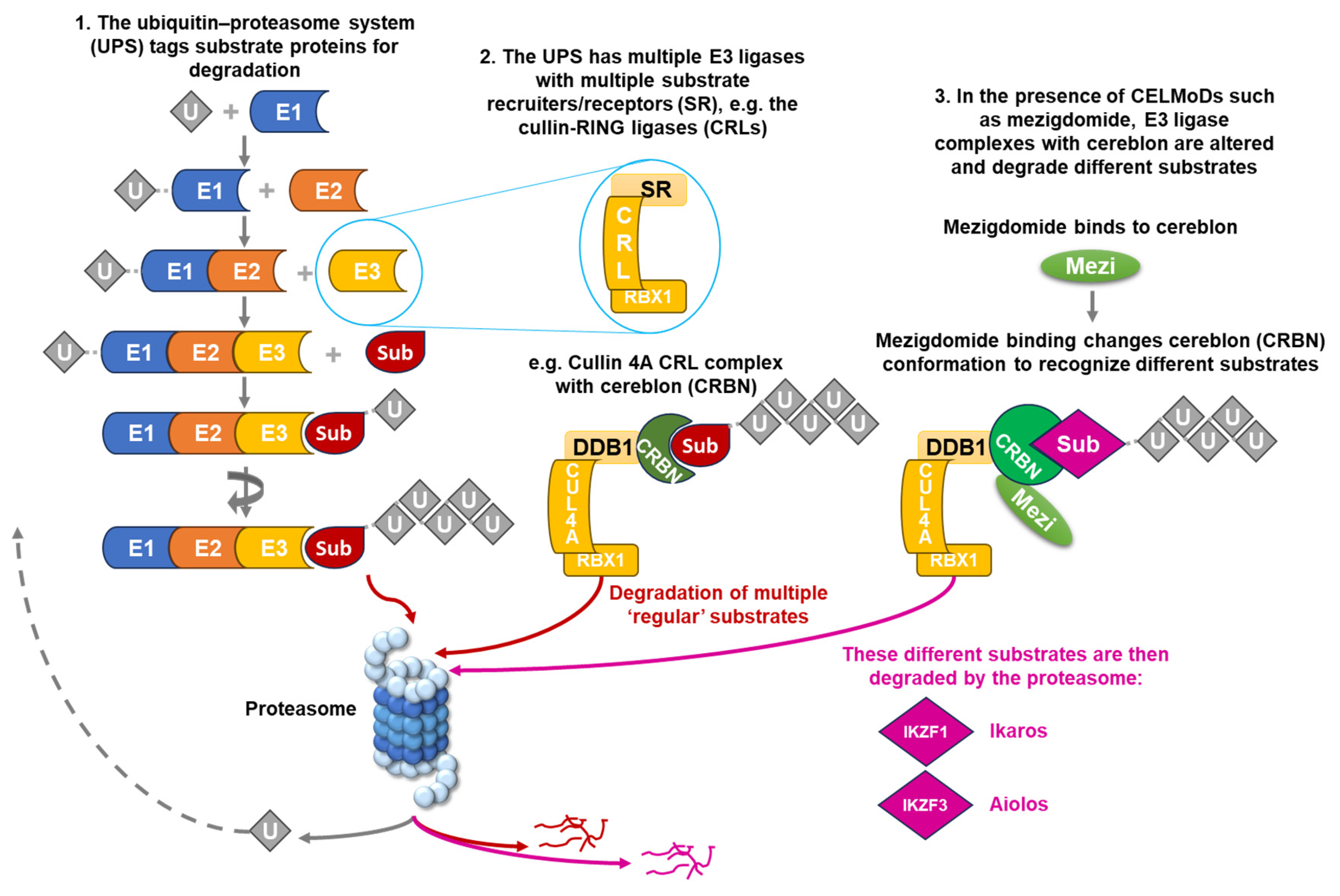
2. Targeting the UPS in the Treatment of MM
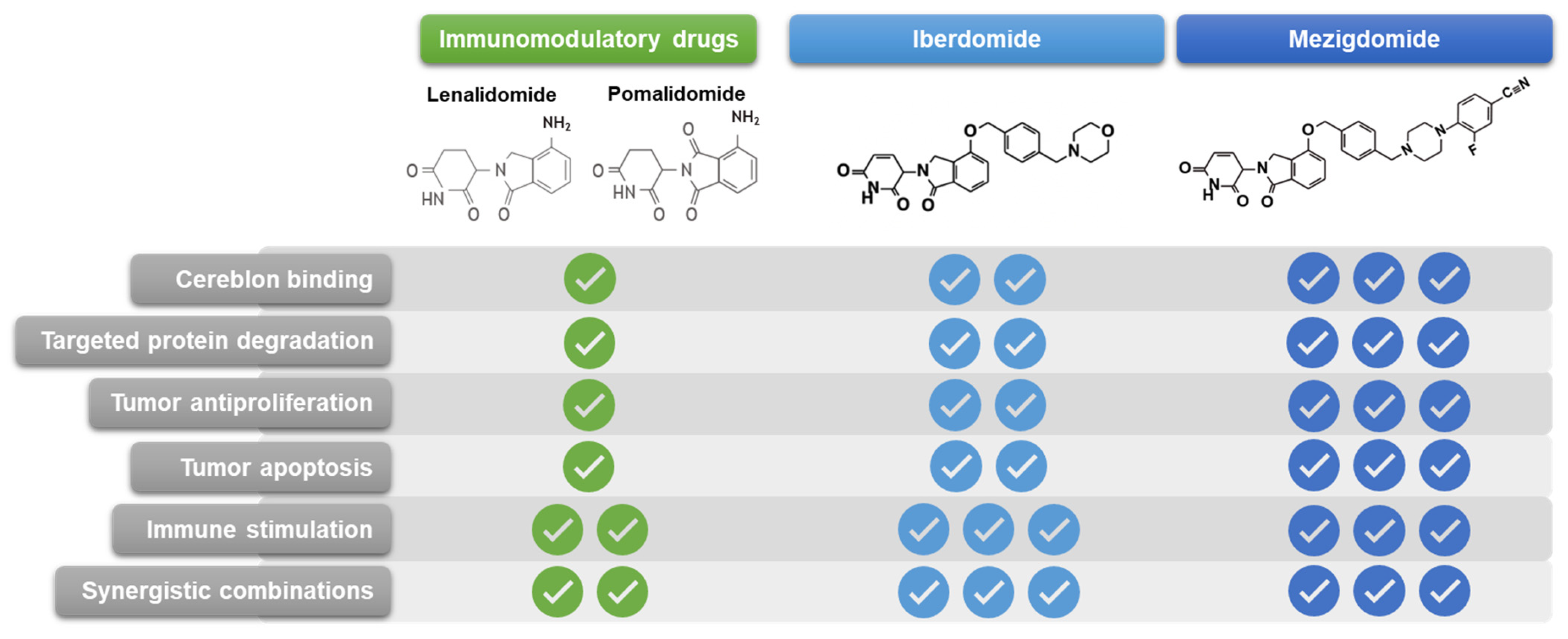
CELMoDs
3. Preclinical Rationale for Activity of Mezigdomide in RRMM
4. Clinical Data from Studies of Mezigdomide in RRMM
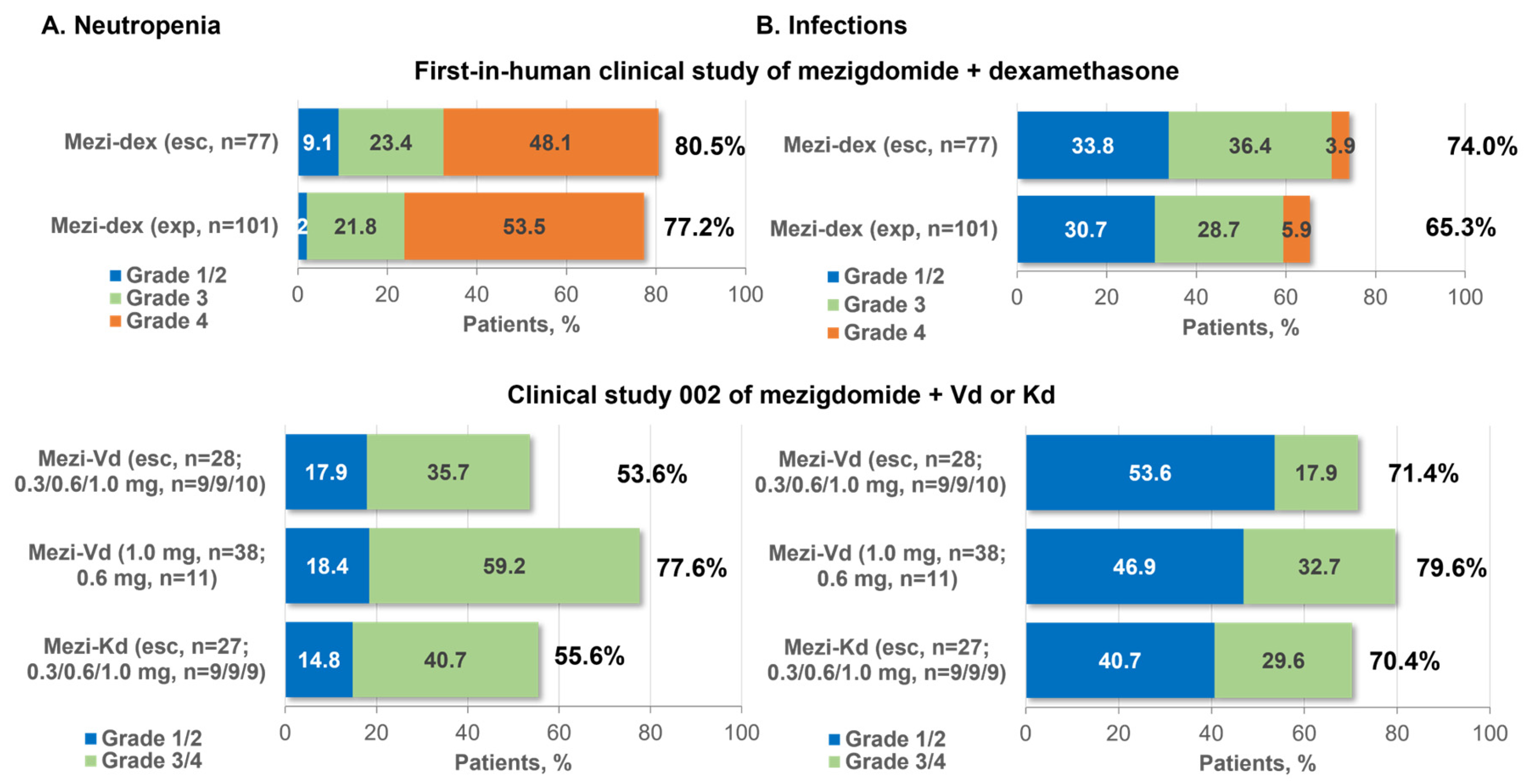
4.1. Clinical Safety Profile of Mezigdomide
4.2. Clinical Pharmacokinetics and Pharmacodynamics of Mezigdomide
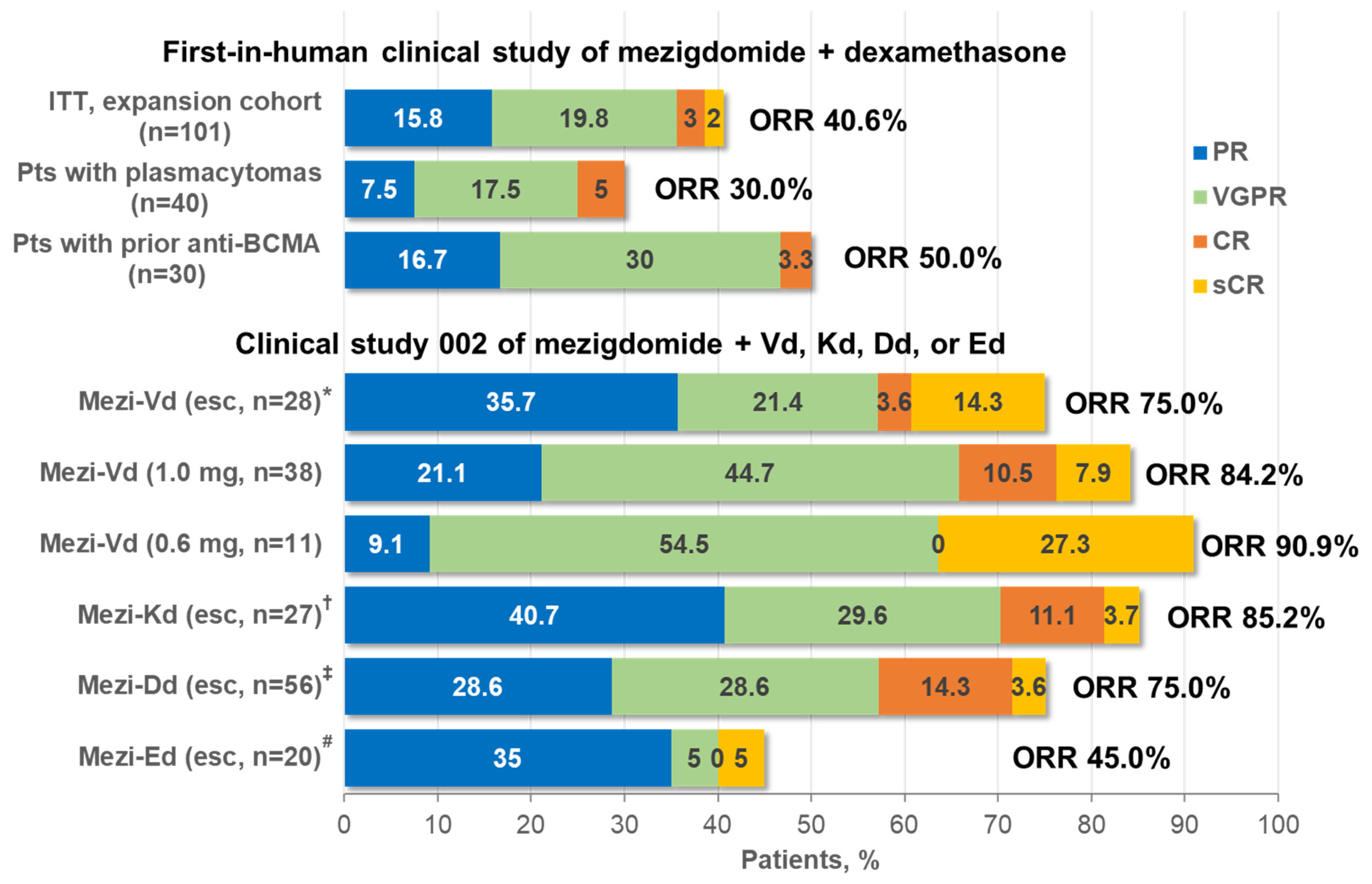
4.3. Clinical Efficacy of Mezigdomide
5. Discussion and Future Perspectives
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anderson, K.C. The 39th David A. Karnofsky Lecture: Bench-to-Bedside Translation of Targeted Therapies in Multiple Myeloma. J. Clin. Oncol. 2012, 30, 445–452. [Google Scholar] [CrossRef]
- Joseph, N.S.; Kaufman, J.L.; Dhodapkar, M.V.; Hofmeister, C.C.; Almaula, D.K.; Heffner, L.T.; Gupta, V.A.; Boise, L.H.; Lonial, S.; Nooka, A.K. Long-Term Follow-up Results of Lenalidomide, Bortezomib, and Dexamethasone Induction Therapy and Risk-Adapted Maintenance Approach in Newly Diagnosed Multiple Myeloma. J. Clin. Oncol. 2020, 38, 1928–1937. [Google Scholar] [CrossRef]
- Fonseca, R.; Facon, T.; Hashim, M.; Nair, S.; He, J.; Ammann, E.; Lam, A.; Wildgust, M.; Kumar, S. Impact of Treatment Sequencing on Overall Survival in Patients with Transplant-Ineligible Newly Diagnosed Myeloma. Oncologist 2023, 28, e263–e269. [Google Scholar] [CrossRef]
- Raje, N.; Mateos, M.V.; Iida, S.; Reece, D. Clinical Evidence for Immune-Based Strategies in Early-Line Multiple Myeloma: Current Challenges in Decision-Making for Subsequent Therapy. Blood Cancer J. 2023, 13, 41. [Google Scholar] [CrossRef]
- Benda, M.A.; Ulmer, H.; Weger, R.; Reimann, P.; Lang, T.; Pichler, P.; Winder, T.; Hartmann, B.; Strassl, I.; Krauth, M.T.; et al. Attrition Rates in Multiple Myeloma Treatment under Real World Conditions-an Analysis from the Austrian Myeloma Registry (Amr). Cancers 2023, 15, 962. [Google Scholar] [CrossRef]
- McCurdy, A.; Mian, H.; LeBlanc, R.; Jimenez-Zepeda, V.H.; Su, J.; Masih-Khan, E.; Visram, A.; Louzada, M.; Song, K.; White, D.; et al. Redefining Attrition in Multiple Myeloma (Mm): A Canadian Myeloma Research Group (Cmrg) Analysis. Blood Cancer J. 2023, 13, 111. [Google Scholar] [CrossRef] [PubMed]
- Callander, N.S.; Baljevic, M.; Adekola, K.; Anderson, L.D.; Campagnaro, E.; Castillo, J.J.; Costello, C.; Devarakonda, S.; Elsedawy, N.; Faiman, M.; et al. Nccn Guidelines(R) Insights: Multiple Myeloma, Version 3.2022. J. Natl. Compr. Cancer Netw. 2022, 20, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer Statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- NIH National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Myeloma. 2023. Available online: https://seer.cancer.gov/statfacts/html/mulmy.html (accessed on 16 February 2024).
- Richardson, P.G.; San Miguel, J.F.; Moreau, P.; Hajek, R.; Dimopoulos, M.A.; Laubach, J.P.; Palumbo, A.; Luptakova, K.; Romanus, D.; Skacel, T.; et al. Interpreting Clinical Trial Data in Multiple Myeloma: Translating Findings to the Real-World Setting. Blood Cancer J. 2018, 8, 109. [Google Scholar] [CrossRef]
- Gandolfi, S.; Vekstein, C.; Laubach, J.P.; O’Brien, A.; Masone, K.; Munshi, N.C.; Anderson, K.C.; Richardson, P.G. The Evolving Role of Transplantation in Multiple Myeloma: The Need for a Heterogeneous Approach to a Heterogeneous Disease. Clin. Adv. Hematol. Oncol. 2018, 16, 564–574. [Google Scholar] [PubMed]
- Dimopoulos, M.A.; Moreau, P.; Terpos, E.; Mateos, M.V.; Zweegman, S.; Cook, G.; Delforge, M.; Hajek, R.; Schjesvold, F.; Cavo, M.; et al. Multiple Myeloma: Eha-Esmo Clinical Practice Guidelines for Diagnosis, Treatment and Follow-up. Ann. Oncol. 2021, 32, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.V. Multiple Myeloma: 2022 Update on Diagnosis, Risk Stratification, and Management. Am. J. Hematol. 2022, 97, 1086–1107. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.K.; Unawane, R.; Wang, S.; Ahn, J.; Aleman, A.; Siegel, D.S.; Vesole, D.H.; Parmar, H.; Phull, P.; Biran, N. I-Open: Inferior Outcomes of Penta-Refractory Compared to Penta-Exposed Multiple Myeloma Patients. Blood Cancer J. 2022, 12, 138. [Google Scholar] [CrossRef] [PubMed]
- Stalker, M.E.; Mark, T.M. Clinical Management of Triple-Class Refractory Multiple Myeloma: A Review of Current Strategies and Emerging Therapies. Curr. Oncol. 2022, 29, 4464–4477. [Google Scholar] [CrossRef] [PubMed]
- Mo, C.C.; Yee, A.J.; Midha, S.; Hartley-Brown, M.A.; Nadeem, O.; O’Donnell, E.K.; Bianchi, G.; Sperling, A.S.; Laubach, J.P.; Richardson, P.G. Selinexor: Targeting a Novel Pathway in Multiple Myeloma. EJHaem 2023, 4, 792–810. [Google Scholar] [CrossRef]
- Nadeem, O.; Mateos, M.V.; Efebera, Y.A.; Paner, A.; Larocca, A.; Rodriguez-Otero, P.; Leleu, X.; Richardson, P.G. Melphalan Flufenamide for Relapsed/Refractory Multiple Myeloma. Drugs Today 2022, 58, 407–423. [Google Scholar] [CrossRef]
- Parikh, R.H.; Lonial, S. Chimeric Antigen Receptor T-Cell Therapy in Multiple Myeloma: A Comprehensive Review of Current Data and Implications for Clinical Practice. CA Cancer J. Clin. 2023, 73, 275–285. [Google Scholar] [CrossRef]
- Cipkar, C.; Chen, C.; Trudel, S. Antibodies and Bispecifics for Multiple Myeloma: Effective Effector Therapy. Hematol. Am. Soc. Hematol. Educ. Program. 2022, 2022, 163–172. [Google Scholar] [CrossRef]
- Cho, S.F.; Yeh, T.J.; Anderson, K.C.; Tai, Y.T. Bispecific Antibodies in Multiple Myeloma Treatment: A Journey in Progress. Front. Oncol. 2022, 12, 1032775. [Google Scholar] [CrossRef]
- Munshi, N.C.; Anderson, L.D., Jr.; Shah, N.; Madduri, D.; Berdeja, J.; Lonial, S.; Raje, N.; Lin, Y.; Siegel, D.; Oriol, A.; et al. Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. N. Engl. J. Med. 2021, 384, 705–716. [Google Scholar] [CrossRef]
- Rodriguez-Otero, P.; Ailawadhi, S.; Arnulf, B.; Patel, K.; Cavo, M.; Nooka, A.K.; Manier, S.; Callander, N.; Costa, L.J.; Vij, R.; et al. Ide-Cel or Standard Regimens in Relapsed and Refractory Multiple Myeloma. N. Engl. J. Med. 2023, 388, 1002–1014. [Google Scholar] [CrossRef]
- Berdeja, J.G.; Madduri, D.; Usmani, S.Z.; Jakubowiak, A.; Agha, M.; Cohen, A.D.; Stewart, A.K.; Hari, P.; Htut, M.; Lesokhin, A.; et al. Ciltacabtagene Autoleucel, a B-Cell Maturation Antigen-Directed Chimeric Antigen Receptor T-Cell Therapy in Patients with Relapsed or Refractory Multiple Myeloma (Cartitude-1): A Phase 1b/2 Open-Label Study. Lancet 2021, 398, 314–324. [Google Scholar] [CrossRef] [PubMed]
- San-Miguel, J.; Dhakal, B.; Yong, K.; Spencer, A.; Anguille, S.; Mateos, M.V.; Fernandez de Larrea, C.; Martinez-Lopez, J.; Moreau, P.; Touzeau, C.; et al. Cilta-Cel or Standard Care in Lenalidomide-Refractory Multiple Myeloma. N. Engl. J. Med. 2023, 389, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Moreau, P.; Garfall, A.L.; van de Donk, N.; Nahi, H.; San-Miguel, J.F.; Oriol, A.; Nooka, A.K.; Martin, T.; Rosinol, L.; Chari, A.; et al. Teclistamab in Relapsed or Refractory Multiple Myeloma. N. Engl. J. Med. 2022, 387, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Chari, A.; Minnema, M.C.; Berdeja, J.G.; Oriol, A.; van de Donk, N.; Rodriguez-Otero, P.; Askari, E.; Mateos, M.V.; Costa, L.J.; Caers, J.; et al. Talquetamab, a T-Cell-Redirecting Gprc5d Bispecific Antibody for Multiple Myeloma. N. Engl. J. Med. 2022, 387, 2232–2244. [Google Scholar] [CrossRef] [PubMed]
- Lesokhin, A.M.; Tomasson, M.H.; Arnulf, B.; Bahlis, N.J.; Miles Prince, H.; Niesvizky, R.; Rodriotaguez-Otero, P.; Martinez-Lopez, J.; Koehne, G.; Touzeau, C.; et al. Elranatamab in Relapsed or Refractory Multiple Myeloma: Phase 2 Magnetismm-3 Trial Results. Nat. Med. 2023, 29, 2259–2267. [Google Scholar] [CrossRef] [PubMed]
- Lonial, S.; Lee, H.C.; Badros, A.; Trudel, S.; Nooka, A.K.; Chari, A.; Abdallah, A.O.; Callander, N.; Sborov, D.; Suvannasankha, A.; et al. Longer Term Outcomes with Single-Agent Belantamab Mafodotin in Patients with Relapsed or Refractory Multiple Myeloma: 13-Month Follow-up from the Pivotal Dreamm-2 Study. Cancer 2021, 127, 4198–4212. [Google Scholar] [CrossRef] [PubMed]
- Snowden, J.A.; Greenfield, D.M.; Bird, J.M.; Boland, E.; Bowcock, S.; Fisher, A.; Low, E.; Morris, M.; Yong, K.; Pratt, G.; et al. Guidelines for Screening and Management of Late and Long-Term Consequences of Myeloma and Its Treatment. Br. J. Haematol. 2017, 176, 888–907. [Google Scholar] [CrossRef]
- Terpos, E.; Mikhael, J.; Hajek, R.; Chari, A.; Zweegman, S.; Lee, H.C.; Mateos, M.V.; Larocca, A.; Ramasamy, K.; Kaiser, M.; et al. Management of Patients with Multiple Myeloma Beyond the Clinical-Trial Setting: Understanding the Balance between Efficacy, Safety and Tolerability, and Quality of Life. Blood Cancer J. 2021, 11, 40. [Google Scholar] [CrossRef]
- Kourelis, T.; Bansal, R.; Patel, K.K.; Berdeja, J.G.; Raje, N.S.; Alsina, M.; Cohen, A.D.; Siegel, D.S.D.; Mailankody, S.; Htut, M.; et al. Ethical Challenges with Car T Slot Allocation with Idecabtagene Vicleucel Manufacturing Access. J. Clin. Oncol. 2022, 40, e20021. [Google Scholar] [CrossRef]
- Richardson, P.G.; Trudel, S.; Popat, R.; Mateos, M.V.; Vangsted, A.J.; Ramasamy, K.; Martinez-Lopez, J.; Quach, H.; Orlowski, R.Z.; Arnao, M.; et al. Mezigdomide Plus Dexamethasone in Relapsed and Refractory Multiple Myeloma. N. Engl. J. Med. 2023, 389, 1009–1022. [Google Scholar] [CrossRef]
- LaPlante, G.; Zhang, W. Targeting the Ubiquitin-Proteasome System for Cancer Therapeutics by Small-Molecule Inhibitors. Cancers 2021, 13, 3079. [Google Scholar] [CrossRef]
- Lub, S.; Maes, K.; Menu, E.; De Bruyne, E.; Vanderkerken, K.; Van Valckenborgh, E. Novel Strategies to Target the Ubiquitin Proteasome System in Multiple Myeloma. Oncotarget 2016, 7, 6521–6537. [Google Scholar] [CrossRef] [PubMed]
- Dou, Q.P.; Zonder, J.A. Overview of Proteasome Inhibitor-Based Anti-Cancer Therapies: Perspective on Bortezomib and Second Generation Proteasome Inhibitors Versus Future Generation Inhibitors of Ubiquitin-Proteasome System. Curr. Cancer Drug Targets 2014, 14, 517–536. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, S.; Laubach, J.P.; Hideshima, T.; Chauhan, D.; Anderson, K.C.; Richardson, P.G. The Proteasome and Proteasome Inhibitors in Multiple Myeloma. Cancer Metastasis Rev. 2017, 36, 561–584. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.G.; Mateos, M.V.; Vangsted, A.J.; Ramasamy, K.; Abildgaard, N.; Ho, P.J.; Quach, H.; Bahlis, N.J. The Role of E3 Ubiquitin Ligase in Multiple Myeloma: Potential for Cereblon E3 Ligase Modulators in the Treatment of Relapsed/Refractory Disease. Expert. Rev. Proteom. 2022, 19, 235–246. [Google Scholar] [CrossRef] [PubMed]
- Singhal, S.; Mehta, J.; Desikan, R.; Ayers, D.; Roberson, P.; Eddlemon, P.; Munshi, N.; Anaissie, E.; Wilson, C.; Dhodapkar, M.; et al. Antitumor Activity of Thalidomide in Refractory Multiple Myeloma. N. Engl. J. Med. 1999, 341, 1565–1571. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.V.; Hayman, S.R.; Lacy, M.Q.; Dispenzieri, A.; Geyer, S.M.; Kabat, B.; Zeldenrust, S.R.; Kumar, S.; Greipp, P.R.; Fonseca, R.; et al. Combination Therapy with Lenalidomide Plus Dexamethasone (Rev/Dex) for Newly Diagnosed Myeloma. Blood 2005, 106, 4050–4053. [Google Scholar] [CrossRef] [PubMed]
- Miguel, J.S.; Weisel, K.; Moreau, P.; Lacy, M.; Song, K.; Delforge, M.; Karlin, L.; Goldschmidt, H.; Banos, A.; Oriol, A.; et al. Pomalidomide Plus Low-Dose Dexamethasone Versus High-Dose Dexamethasone Alone for Patients with Relapsed and Refractory Multiple Myeloma (Mm-003): A Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2013, 14, 1055–1066. [Google Scholar] [CrossRef]
- Zhu, Y.X.; Braggio, E.; Shi, C.X.; Bruins, L.A.; Schmidt, J.E.; Van Wier, S.; Chang, X.B.; Bjorklund, C.C.; Fonseca, R.; Bergsagel, P.L.; et al. Cereblon Expression Is Required for the Antimyeloma Activity of Lenalidomide and Pomalidomide. Blood 2011, 118, 4771–4779. [Google Scholar] [CrossRef]
- Hansen, J.D.; Correa, M.; Nagy, M.A.; Alexander, M.; Plantevin, V.; Grant, V.; Whitefield, B.; Huang, D.; Kercher, T.; Harris, R.; et al. Discovery of Crbn E3 Ligase Modulator Cc-92480 for the Treatment of Relapsed and Refractory Multiple Myeloma. J. Med. Chem. 2020, 63, 6648–6676. [Google Scholar] [CrossRef]
- Shortt, J. Mezigdomide and Multiple Myeloma. N. Engl. J. Med. 2023, 389, 1046–1050. [Google Scholar] [CrossRef]
- Kronke, J.; Udeshi, N.D.; Narla, A.; Grauman, P.; Hurst, S.N.; McConkey, M.; Svinkina, T.; Heckl, D.; Comer, E.; Li, X.; et al. Lenalidomide Causes Selective Degradation of Ikzf1 and Ikzf3 in Multiple Myeloma Cells. Science 2014, 343, 301–305. [Google Scholar] [CrossRef]
- Lu, G.; Middleton, R.E.; Sun, H.; Naniong, M.; Ott, C.J.; Mitsiades, C.S.; Wong, K.K.; Bradner, J.E.; Kaelin, W.G., Jr. The Myeloma Drug Lenalidomide Promotes the Cereblon-Dependent Destruction of Ikaros Proteins. Science 2014, 343, 305–309. [Google Scholar] [CrossRef]
- John, L.B.; Ward, A.C. The Ikaros Gene Family: Transcriptional Regulators of Hematopoiesis and Immunity. Mol. Immunol. 2011, 48, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Fedele, P.L.; Willis, S.N.; Liao, Y.; Low, M.S.; Rautela, J.; Segal, D.H.; Gong, J.N.; Huntington, N.D.; Shi, W.; Huang, D.C.S.; et al. Imids Prime Myeloma Cells for Daratumumab-Mediated Cytotoxicity through Loss of Ikaros and Aiolos. Blood 2018, 132, 2166–2178. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, A.K.; Kang, J.; Havens, C.G.; Conklin, T.; Ning, Y.; Wu, L.; Ito, T.; Ando, H.; Waldman, M.F.; Thakurta, A.; et al. Immunomodulatory Agents Lenalidomide and Pomalidomide Co-Stimulate T Cells by Inducing Degradation of T Cell Repressors Ikaros and Aiolos Via Modulation of the E3 Ubiquitin Ligase Complex CRL4CRBN. Br. J. Haematol. 2014, 164, 811–821. [Google Scholar] [CrossRef]
- Matyskiela, M.E.; Zhang, W.; Man, H.W.; Muller, G.; Khambatta, G.; Baculi, F.; Hickman, M.; LeBrun, L.; Pagarigan, B.; Carmel, G.; et al. A Cereblon Modulator (Cc-220) with Improved Degradation of Ikaros and Aiolos. J. Med. Chem. 2018, 61, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Watson, E.R.; Novick, S.; Matyskiela, M.E.; Chamberlain, P.P.; de la Pena, A.J.; Zhu, J.; Tran, E.; Griffin, P.R.; Wertz, I.E.; Lander, G.C. Molecular Glue Celmod Compounds Are Regulators of Cereblon Conformation. Science 2022, 378, 549–553. [Google Scholar] [CrossRef]
- Bourgeois, W.; Aubrey, B.J.; Cutler, J.A.; Donovan, K.A.; Hatton, C.; Theall, A.C.P.; Nowak, R.P.; McGeehan, G.M.; Fischer, E.S.; Armstrong, S.A. Potent Ikaros Degradation by the Cereblon E3 Ligase Modulator Cc-92480 Is Effective in Combination with Menin-Mll1 Inhibition in Mll1-Rearranged and Npm1-Mutant Aml. Blood 2021, 138 (Suppl. S1), 208. [Google Scholar] [CrossRef]
- Liang, H.C.; Elenitoba-Johnson, K.S.J. Targeting Imid-Resistant T-Cell Lymphoma. Blood 2022, 139, 1932–1933. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Nelson, G.M.; Koch, R.; Donovan, K.A.; Nowak, R.P.; Heavican-Foral, T.B.; Nirmal, A.J.; Liu, H.; Yang, L.; Duffy, J.; et al. Overcoming Imid Resistance in T-Cell Lymphomas through Potent Degradation of Zfp91 and Ikzf1. Blood 2022, 139, 2024–2037. [Google Scholar] [CrossRef] [PubMed]
- Barankiewicz, J.; Salomon-Perzynski, A.; Misiewicz-Krzeminska, I.; Lech-Maranda, E. CRL4CRBN E3 Ligase Complex as a Therapeutic Target in Multiple Myeloma. Cancers 2022, 14, 4492. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, C.; Prince, H.M.; Neeson, P.J. Understanding the Role of T-Cells in the Antimyeloma Effect of Immunomodulatory Drugs. Front. Immunol. 2021, 12, 632399. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Girona, A.; Havens, C.G.; Lu, G.; Rychak, E.; Mendy, D.; Gaffney, B.; Surka, C.; Lu, C.-C.; Matyskiela, M.; Khambatta, G.; et al. Cc-92480 Is a Novel Cereblon E3 Ligase Modulator with Enhanced Tumoricidal and Immunomodulatory Activity against Sensitive and Resistant Multiple Myeloma Cells. Blood 2019, 134 (Suppl. S1), 1812. [Google Scholar] [CrossRef]
- Paiva, B.; Gaffney, B.; Burnett, K.; Castiglioni, P.; Angelo, M.; Pierce, D.W.; Boss, I.W. Synergistic Antitumor Activity of Alnuctamab (Alnuc; Bms-986349; Cc-93269), a Bcma 2+1 T Cell Engager (Tce), and Celmod Agents in Multiple Myeloma (Mm) Preclinical Models. Blood 2022, 140 (Suppl. S1), 7054–7055. [Google Scholar] [CrossRef]
- Van Oekelen, O.; Amatangelo, M.; Guo, M.; Upadhyaya, B.; Kelly, G.; Patel, M.; Kim-Schulze, S.; Lagana, A.; Gooding, S.; Jagannath, S.; et al. Large-Scale Mass Cytometry Reveals Significant Activation of Innate and Adaptive Immunity in Bone Marrow Tumor Microenvironment of Iberdomide-Treated Myeloma Patients. Blood 2021, 138 (Suppl. S1), 730. [Google Scholar] [CrossRef]
- Chen, L.Y.; Van Oekelen, O.; Amatangelo, M.; Chow, T.T.; Upadhyaya, B.; Lagana, A.; Kelly, G.; Kim-Schulze, S.; Aleman, A.; Kurtova, A.; et al. Mezigdomide Treatment in Relapsed-Refractory Myeloma Patients Shifts Bone Marrow Nk and T Cell Populations from Exhaustion to Activation. Blood 2023, 142 (Suppl. S1), 4686. [Google Scholar] [CrossRef]
- Chiu, H.; Zhao, J.; Ortiz Estevez, M.; Hagner, P.R.; Gandhi, A.K. Mezigdomide Reverses T-Cell Exhaustion through Degradation of Aiolos/Ikaros and Reinvigoration of Cytokine Production Pathways. Blood 2023, 142 (Suppl. S1), 335. [Google Scholar] [CrossRef]
- Thakurta, A.; Pierceall, W.E.; Amatangelo, M.D.; Flynt, E.; Agarwal, A. Developing Next Generation Immunomodulatory Drugs and Their Combinations in Multiple Myeloma. Oncotarget 2021, 12, 1555–1563. [Google Scholar] [CrossRef]
- Wong, L.; Krishna Narla, R.; Leisten, J.; Bauer, D.; Groza, M.; Gaffney, B.; Havens, C.G.; Choi, J.; Houston, J.; Lopez-Girona, A.; et al. Cc-92480, a Novel Cereblon E3 Ligase Modulator, Is Synergistic with Dexamethasone, Bortezomib, and Daratumumab in Multiple Myeloma. Blood 2019, 134 (Suppl. S1), 1815. [Google Scholar] [CrossRef]
- Bjorklund, C.C.; Amatangelo, M.; Chiu, H.; Kang, J.; Civardi, T.; Katz, J.; Maciag, P.; Hagner, P.; Pourdehnad, M.; Bahlis, N.J.; et al. Pre-Clinical and Clinical Immunomodulatory Effects of Pomalidomide or Cc-92480 in Combination with Bortezomib in Multiple Myeloma. Blood 2021, 138 (Suppl. S1), 1613. [Google Scholar] [CrossRef]
- Bjorklund, C.C.; Amatangelo, M.; Kang, J.; Chiu, H.; Mukhopadhyay, A.; Wollerman, K.; Pourdehnad, M.; Hagner, P.; Thakurta, A. Cc-92480 Enhances Cell-Autonomous Cytotoxicity through Blockade of G 2/M Transition When Combined with Bortezomib/Dexamethasone in Pre-Clinical Multiple Myeloma. Blood 2021, 138 (Suppl. S1), 2669. [Google Scholar] [CrossRef]
- Amatangelo, M.; Bjorklund, C.C.; Hagner, P.; Koo, P.; Civardi, T.; Ghiddi, A.; Katz, J.; Richardson, P.; Bahlis, N.; Gandhi, A. P-230: Preclinical and Translational Biomarker Analysis to Support Further Clinical Development and Dose Optimization of Mezigdomide (Mezi; Cc-92480) in Combination with Either Bortezomib or Carfilzomib. Clin. Lymphoma Myeloma Leuk. 2022, 22 (Suppl. S1), S161–S162. [Google Scholar] [CrossRef]
- Chow, T.T.; Amatangelo, M.; Ma, P.; Bjorklund, C.C.; Wollerman, K.; Civardi, T.; Koo, P.; Zhu, Y.; Maciag, P.; Katz, J.; et al. Preclinical and Translational Biomarker Analyses to Inform Clinical Development of Mezigdomide (Cc-92480) in Combination with Dexamethasone and Daratumumab in Multiple Myeloma. Blood 2023, 142 (Suppl. S1), 3318. [Google Scholar] [CrossRef]
- Gaffney, B.; Shi, Y.; de Jong, P.; Sanchez, M.; Fontanillo, C.; Lopez-Girona, A.; Boss, I.W.; Kurtova, A.; Carrancio, S.; Wong, L.; et al. Mezigdomide (Cc-92480), a Novel Cereblon E3 Ligase Modulator, Induces Vulnerability of Multiple Myeloma Cells to T-Cell-Mediated Killing. Blood 2022, 140 (Suppl. S1), 7108–7109. [Google Scholar] [CrossRef]
- Landgren, O.; Nadeem, O. Bispecific Monoclonal Antibodies in Multiple Myeloma: Data from Ash 2022: A Podcast. Adv. Ther. 2023, 40, 3291–3303. [Google Scholar] [CrossRef] [PubMed]
- Eckmann, J.; Hage, C.; Stefanie, L.; Bayer, C.; Klein, C.; Umana, P. Early Intervention with Celmods, but Not Imids, Prevents Relapse to Forimtamig Driven by Gprc5d-Negative Myeloma Cells. Blood 2023, 142, 4659. [Google Scholar] [CrossRef]
- Jeyaraju, D.V.; Alapa, M.; O’Donohue, A.; La Motte-Mohs, R.; Boss, I.W.; Hagner, P.; Pourdehnad, M.; Burgess, M.R.; Pierceall, W.R.; Thakurta, A. Suppression of Myeloid Cell-Derived Proinflammatory Cytokines with Celmod Agents: Implications for Crs with T-Cell Engagers (Tces). Blood 2022, 140 (Suppl. S1), 7070–7071. [Google Scholar] [CrossRef]
- Ahsan, A.; Polonskaia, A.; Hsu, C.-C.; Bjorklund, C.C.; Ortiz Estevez, M.; Towfic, F.; Bahlis, N.J.; Pourdehnad, M.; Flynt, E.; Ahsan, A.; et al. Super-Enhancer Driven Regulation of Cks1b in Multiple Myeloma: Implications in Mediating Response to Bet Inhibitor and Celmod Agent Combination. Blood 2021, 138 (Suppl. S1), 2658. [Google Scholar] [CrossRef]
- Bird, S.; Pawlyn, C. IMiD Imid Resistance in Multiple Myeloma: Current Understanding of the Underpinning Biology and Clinical Impact. Blood 2023, 142, 131–140. [Google Scholar] [CrossRef]
- Bird, S.A.; Barber, A.; Sialana, F.J.; Licciardello, M.P.; Che, H.; Bouguenina, H.; Grabovska, Y.; Liu, E.; Chrisochoidou, Y.; Martin, S.; et al. Multiomics Analysis of Imid/Celmod Resistant Multiple Myeloma Models Uncovers Novel and Targetable Vulnerabilities in the Srebp Lipid Synthesis Pathway. Blood 2022, 140 (Suppl. S1), 600–601. [Google Scholar] [CrossRef]
- Tilmont, R.; Maity, R.; Leblay, N.; Lee, H.; Barakat, E.; Neri, P.; Bahlis, N.J. Crbn Structural Changes, Copy Number Changes and Cop9 Signalosome Subunits Gene Expression Mediate Sensitivity to New Celmod Compound Cc-92480 in Multiple Myeloma Patients. Blood 2022, 140 (Suppl. S1), 9964–9965. [Google Scholar] [CrossRef]
- Chrisochoidou, Y.; LeBihan, Y.-V.; Morales, S.; Martin, S.; Walker, B.A.; Li, Y.; Bird, S.; Pawlyn, C. Investigating the Functional Impact of Crbn Mutations on Response to Imid/Celmod Agents in Myeloma. Blood 2023, 142 (Suppl. S1), 753. [Google Scholar] [CrossRef]
- Gooding, S.; Ansari-Pour, N.; Towfic, F.; Ortiz Estevez, M.; Chamberlain, P.P.; Tsai, K.T.; Flynt, E.; Hirst, M.; Rozelle, D.; Dhiman, P.; et al. Multiple Cereblon Genetic Changes Are Associated with Acquired Resistance to Lenalidomide or Pomalidomide in Multiple Myeloma. Blood 2021, 137, 232–237. [Google Scholar] [CrossRef]
- Nguyen, T.V. USP15 Antagonizes CRL4CRBN-Mediated Ubiquitylation of Glutamine Synthetase and Neosubstrates. Proc. Natl. Acad. Sci. USA 2021, 118, e2111391118. [Google Scholar] [CrossRef]
- Oriol, A.; Sandhu, I.; Raab, M.; White, D.; LeBlanc, R.; Raje, N.; Ocio, E.; Perrot, A.; Facon, T.; Rodriguez, C.; et al. Oa-49 Mezigdomide (Mezi) Plus Dexamethasone (Dex) and Bortezomib (Bort) or Carfilzomib (Cfz) in Patients (Pts) with Relapsed/Refractory Multiple Myeloma (Rrmm): Results from the Cc-92480-Mm-002 Trial. Clin. Lymphoma Myeloma Leuk. 2023, 23 (Suppl. S2), S31. [Google Scholar] [CrossRef]
- Goldsmith, S.; Oriol, A.; Anttila, P.; Bahlis, N.; Berdeja, J.; Cowan, A.; Dimopoulos, M.; Foster, L.; Hillengass, J.; Louzada, M.; et al. P-265 Mezigdomide (Mezi) Monotherapy in Relapsed/Refractory Multiple Myeloma (Rrmm): Results from the Cc-92480-Mm-001 Trial. Clin. Lymphoma Myeloma Leuk. 2023, 23 (Suppl. S2), S181–S182. [Google Scholar] [CrossRef]
- Richardson, P.G.; Sandhu, I.; Hofmeister, C.C.; Orlowski, R.Z.; White, D.; Belotti, A.; Toftmann Hansen, C.; Raje, N.S.; Chow, T.T.; Zhou, Z.; et al. Mezigdomide (Mezi) Plus Dexamethasone (Dex) and Daratumumab (Dara) or Elotuzumab (Elo) in Patients (Pts) with Relapsed/Refractory Multiple Myeloma (Rrmm): Results from the Cc-92480-Mm-002 Trial. Blood 2023, 142 (Suppl. S1), 1013. [Google Scholar] [CrossRef]
- Wu, F.; Liu, L.; Gaudy, A.; Wang, X.; Carayannopoulos, L.; Pourdehnad, M.; Lamba, M. Model Based Assessment of Food and Acid Reducing Agent Effects on Oral Absorption of Mezigdomide (Cc-92480), a Novel Cereblon E3 Ligase Modulator. CPT Pharmacomet. Syst. Pharmacol. 2023, 12, 1473–1484. [Google Scholar] [CrossRef]
- Wong, L.; Lamba, M.; Jiménez Nuñez, M.D.; Bauer, D.; Richardson, P.G.; Bahlis, N.J.; Vangsted, A.J.; Ramasamy, K.; Trudel, S.; Martínez-Lopez, J.; et al. Dose- and Schedule-Dependent Immunomodulatory Effects of the Novel Celmod Agent Cc-92480 in Patients with Relapsed/Refractory Multiple Myeloma. Blood 2020, 136 (Suppl. S1), 47–48. [Google Scholar] [CrossRef]
- Usmani, S.; Ahmadi, T.; Ng, Y.; Lam, A.; Desai, A.; Potluri, R.; Mehra, M. Analysis of Real-World Data on Overall Survival in Multiple Myeloma Patients with ≥3 Prior Lines of Therapy Including a Proteasome Inhibitor (Pi) and an Immunomodulatory Drug (Imid), or Double Refractory to a Pi and an Imid. Oncologist 2016, 21, 1355–1361. [Google Scholar] [CrossRef]
- Gandhi, U.H.; Cornell, R.F.; Lakshman, A.; Gahvari, Z.J.; McGehee, E.; Jagosky, M.H.; Gupta, R.; Varnado, W.; Fiala, M.A.; Chhabra, S.; et al. Outcomes of Patients with Multiple Myeloma Refractory to Cd38-Targeted Monoclonal Antibody Therapy. Leukemia 2019, 33, 2266–2275. [Google Scholar] [CrossRef]
- Chari, A.; Vogl, D.T.; Gavriatopoulou, M.; Nooka, A.K.; Yee, A.J.; Huff, C.A.; Moreau, P.; Dingli, D.; Cole, C.; Lonial, S.; et al. Oral Selinexor-Dexamethasone for Triple-Class Refractory Multiple Myeloma. N. Engl. J. Med. 2019, 381, 727–738. [Google Scholar] [CrossRef]
- Richardson, P.G.; Oriol, A.; Larocca, A.; Blade, J.; Cavo, M.; Rodriguez-Otero, P.; Leleu, X.; Nadeem, O.; Hiemenz, J.W.; Hassoun, H.; et al. Melflufen and Dexamethasone in Heavily Pretreated Relapsed and Refractory Multiple Myeloma. J. Clin. Oncol. 2021, 39, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Lacy, M.Q.; Hayman, S.R.; Gertz, M.A.; Dispenzieri, A.; Buadi, F.; Kumar, S.; Greipp, P.R.; Lust, J.A.; Russell, S.J.; Dingli, D.; et al. Pomalidomide (Cc4047) Plus Low-Dose Dexamethasone as Therapy for Relapsed Multiple Myeloma. J. Clin. Oncol. 2009, 27, 5008–5014. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.G.; Siegel, D.; Baz, R.; Kelley, S.L.; Munshi, N.C.; Laubach, J.; Sullivan, D.; Alsina, M.; Schlossman, R.; Ghobrial, I.M.; et al. Phase 1 Study of Pomalidomide Mtd, Safety, and Efficacy in Patients with Refractory Multiple Myeloma Who Have Received Lenalidomide and Bortezomib. Blood 2013, 121, 1961–1967. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.G.; Siegel, D.S.; Vij, R.; Hofmeister, C.C.; Baz, R.; Jagannath, S.; Chen, C.; Lonial, S.; Jakubowiak, A.; Bahlis, N.; et al. Pomalidomide Alone or in Combination with Low-Dose Dexamethasone in Relapsed and Refractory Multiple Myeloma: A Randomized Phase 2 Study. Blood 2014, 123, 1826–1832. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.G.; Oriol, A.; Beksac, M.; Liberati, A.M.; Galli, M.; Schjesvold, F.; Lindsay, J.; Weisel, K.; White, D.; Facon, T.; et al. Pomalidomide, Bortezomib, and Dexamethasone for Patients with Relapsed or Refractory Multiple Myeloma Previously Treated with Lenalidomide (Optimismm): A Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2019, 20, 781–794. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.J.; Stadtmauer, E.A.; Abonour, R.; Cohen, A.D.; Bensinger, W.I.; Gasparetto, C.; Kaufman, J.L.; Lentzsch, S.; Vogl, D.T.; Gomes, C.L.; et al. Carfilzomib, Pomalidomide, and Dexamethasone for Relapsed or Refractory Myeloma. Blood 2015, 126, 2284–2290. [Google Scholar] [CrossRef]
- Richardson, P.G.; Hofmeister, C.C.; Raje, N.S.; Siegel, D.S.; Lonial, S.; Laubach, J.; Efebera, Y.A.; Vesole, D.H.; Nooka, A.K.; Rosenblatt, J.; et al. Pomalidomide, Bortezomib and Low-Dose Dexamethasone in Lenalidomide-Refractory and Proteasome Inhibitor-Exposed Myeloma. Leukemia 2017, 31, 2695–2701. [Google Scholar] [CrossRef]
- Chari, A.; Suvannasankha, A.; Fay, J.W.; Arnulf, B.; Kaufman, J.L.; Ifthikharuddin, J.J.; Weiss, B.M.; Krishnan, A.; Lentzsch, S.; Comenzo, R.; et al. Daratumumab Plus Pomalidomide and Dexamethasone in Relapsed and/or Refractory Multiple Myeloma. Blood 2017, 130, 974–981. [Google Scholar] [CrossRef]
- Dimopoulos, M.A.; Terpos, E.; Boccadoro, M.; Delimpasi, S.; Beksac, M.; Katodritou, E.; Moreau, P.; Baldini, L.; Symeonidis, A.; Bila, J.; et al. Daratumumab Plus Pomalidomide and Dexamethasone Versus Pomalidomide and Dexamethasone Alone in Previously Treated Multiple Myeloma (Apollo): An Open-Label, Randomised, Phase 3 Trial. Lancet Oncol. 2021, 22, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Attal, M.; Richardson, P.G.; Rajkumar, S.V.; San-Miguel, J.; Beksac, M.; Spicka, I.; Leleu, X.; Schjesvold, F.; Moreau, P.; Dimopoulos, M.A.; et al. Isatuximab Plus Pomalidomide and Low-Dose Dexamethasone Versus Pomalidomide and Low-Dose Dexamethasone in Patients with Relapsed and Refractory Multiple Myeloma (Icaria-Mm): A Randomised, Multicentre, Open-Label, Phase 3 Study. Lancet 2019, 394, 2096–2107. [Google Scholar] [CrossRef]
- Richardson, P.G.; Badelita, S.N.; Besemer, B.; Boudreault, J.-S.; Byun, J.M.; Cerchione, C.; Gatt, M.E.; Gibbs, S.; Koroda, J.; Martinez-Lopez, J.; et al. Mm-372 a Phase Iii, Two-Stage, Randomized Study of Mezigdomide, Bortezomib, and Dexamethasone (Mezivd) Versus Pomalidomide, Bortezomib, and Dexamethasone (Pvd) in Relapsed/Refractory Multiple Myeloma (Rrmm): Successor-1. Clin. Lymphoma Myeloma Leuk. 2023, 23 (Suppl. S1), S495–S496. [Google Scholar] [CrossRef]
- Richardson, P.; Amatangelo, M.; Berenson, J.; Cerchione, C.; Dimopoulos, M.; Toftmann Hansen, C.; Hwang, S.; Koo, P.; Kuroda, J.; Oriol, A.; et al. A Phase 3, Two-Stage, Randomized Study of Mezigdomide, Carfilzomib, and Dexamethasone (Mezikd) Versus Carfilzomib and Dexamethasone (Kd) in Relapsed/Refractory Multiple Myeloma (Rrmm): Successor-2. J. Clin. Oncol. 2023, 42, TPS8070. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hartley-Brown, M.A.; Mo, C.C.; Nadeem, O.; Midha, S.; Laubach, J.P.; Richardson, P.G. Mezigdomide—A Novel Cereblon E3 Ligase Modulator under Investigation in Relapsed/Refractory Multiple Myeloma. Cancers 2024, 16, 1166. https://doi.org/10.3390/cancers16061166
Hartley-Brown MA, Mo CC, Nadeem O, Midha S, Laubach JP, Richardson PG. Mezigdomide—A Novel Cereblon E3 Ligase Modulator under Investigation in Relapsed/Refractory Multiple Myeloma. Cancers. 2024; 16(6):1166. https://doi.org/10.3390/cancers16061166
Chicago/Turabian StyleHartley-Brown, Monique A., Clifton C. Mo, Omar Nadeem, Shonali Midha, Jacob P. Laubach, and Paul G. Richardson. 2024. "Mezigdomide—A Novel Cereblon E3 Ligase Modulator under Investigation in Relapsed/Refractory Multiple Myeloma" Cancers 16, no. 6: 1166. https://doi.org/10.3390/cancers16061166
APA StyleHartley-Brown, M. A., Mo, C. C., Nadeem, O., Midha, S., Laubach, J. P., & Richardson, P. G. (2024). Mezigdomide—A Novel Cereblon E3 Ligase Modulator under Investigation in Relapsed/Refractory Multiple Myeloma. Cancers, 16(6), 1166. https://doi.org/10.3390/cancers16061166