
Upper Tract Urothelial Cancer: Guideline of Guidelines

 ,
,  ,
,  ,
,  , , ,
, , ,  ,
,  , ,
, ,  ,
,  , ,
, ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Guideline Evaluation
2.3. Data Synthesis
3. Results
3.1. International Guidelines on UTUC
3.1.1. EAU Guidelines
3.1.2. AUA/SUO Guidelines
3.1.3. NCCN Guidelines
3.2. Assessment of Guidelines (AGREE II)
3.3. Epidemiology and Risk Factor
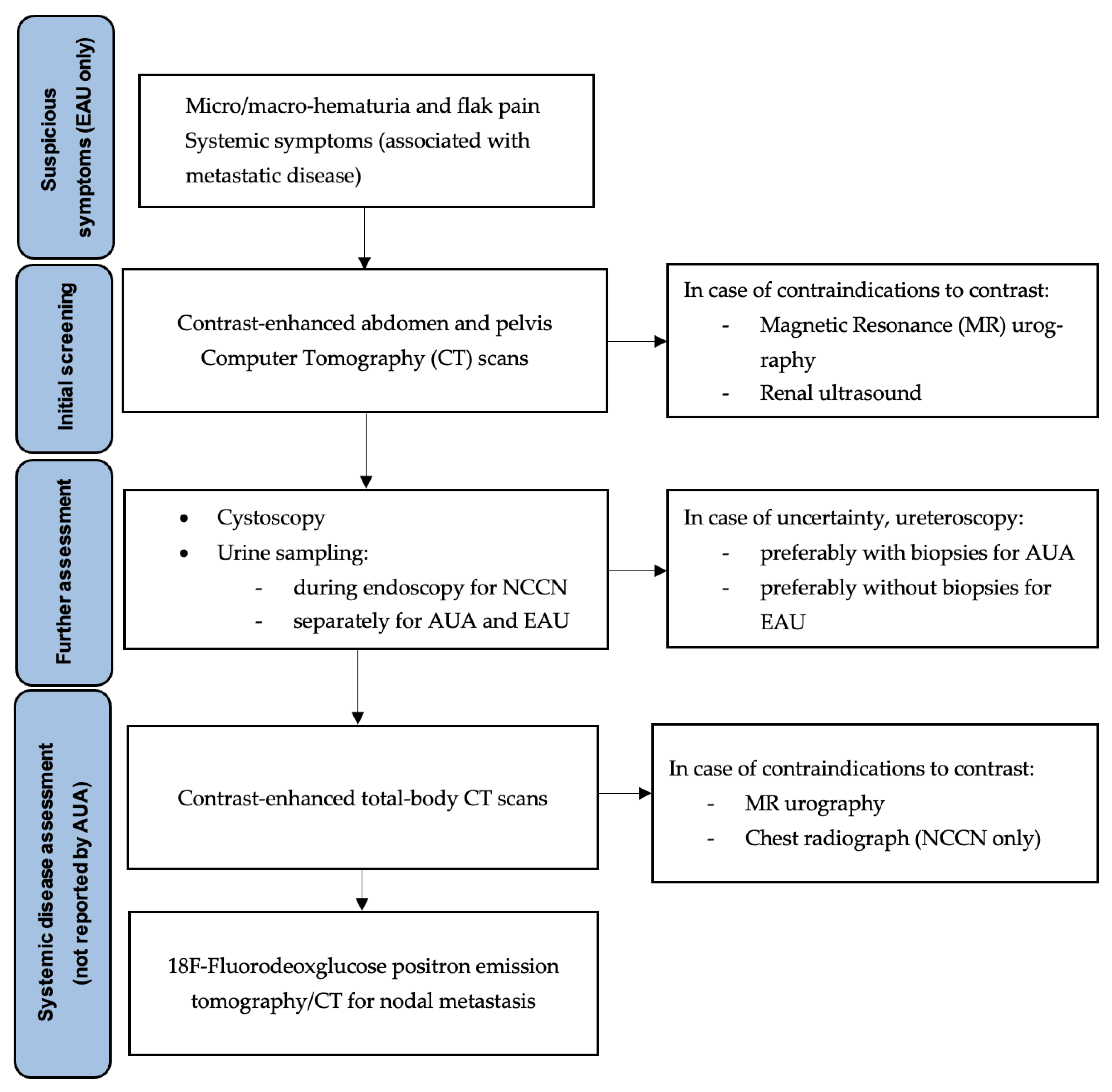
3.4. Diagnosis
3.5. Risk Stratification and Prognosis
3.6. Disease Management
3.6.1. Endoscopic and Surgical Approaches
3.6.2. Medical Therapy
Neoadjuvant Chemotherapy
Adjuvant Chemotherapy
Immunotherapy
3.7. Staging and Classification
3.8. Follow-Up
- <T2N0M0, scans of abdomen and pelvis within 6 months and then annually (EO).
- >T2N0M0, multiphasic contrast-enhanced CT urography every three to six months for two years, every six months in the third year, and annually thereafter. A chest CT is indicated every 6–12 months for the first 5 years (EO).
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Colin, P.; Koenig, P.; Ouzzane, A.; Berthon, N.; Villers, A.; Biserte, J.; Rouprêt, M. Environmental factors involved in carcinogenesis of urothelial cell carcinomas of the upper urinary tract. BJU Int. 2009, 104, 1436–1440. [Google Scholar] [CrossRef]
- Zganjar, A.J.; Thiel, D.D.; Lyon, T.D. Diagnosis, workup, and risk stratification of upper tract urothelial carcinoma. Transl. Androl. Urol. 2023, 12, 1456–1468. [Google Scholar] [CrossRef]
- GGrob, G.; Rogers, D.; Pandolfo, S.D.; Vourganti, S.; Buscarini, M.; Mehrazin, R.; Grob, B.M.; Mir, M.C.; Perdonà, S.; Derweesh, I.H.; et al. Oncologic outcomes following radical nephroureterectomy for upper tract urothelial carcinoma: A literature review. Transl. Androl. Urol. 2023, 12, 1351–1362. [Google Scholar] [CrossRef]
- Wu, Z.; Li, M.; Wang, L.; Paul, A.; Raman, J.D.; Necchi, A.; Psutka, S.P.; Buonerba, C.; Zargar, H.; Black, P.C.; et al. Neoadjuvant systemic therapy in patients undergoing nephroureterectomy for urothelial cancer: A multidisciplinary systematic review and critical analysis. Minerva Urol. Nephrol. 2022, 74, 518–527. Available online: https://www.minervamedica.it/index2.php?show=R19Y2022N05A0518 (accessed on 2 May 2023). [CrossRef]
- Kumar, R.; Kumar Airon, R.; Mittal, A.; Singal, R.; Sharma, K.; Singal, S. Evaluation of Multidetector Computed Tomography in Haematuria. Maedica 2017, 12, 87–94. [Google Scholar]
- Calace, F.P.; Napolitano, L.; Arcaniolo, D.; Stizzo, M.; Barone, B.; Crocetto, F.; Olivetta, M.; Amicuzi, U.; Cirillo, L.; Rubinacci, A.; et al. Micro-Ultrasound in the Diagnosis and Staging of Prostate and Bladder Cancer: A Comprehensive Review. Medicina 2022, 58, 1624. [Google Scholar] [CrossRef] [PubMed]
- Rouprêt, M.; Seisen, T.; Birtle, A.J.; Capoun, O.; Compérat, E.M.; Dominguez-Escrig, J.L.; Gürses Andersson, I.; Liedberg, F.; Mariappan, P.; Hugh Mostafid, A.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2023 Update. Eur. Urol. 2023, 84, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J.A.; Clark, P.E.; Bixler, B.R.; Buckley, D.I.; Chang, S.S.; Chou, R.; Hoffman-Censits, J.; Kulkarni, G.S.; Matin, S.F.; Pierorazio, P.M.; et al. Diagnosis and Management of Non-Metastatic Upper Tract Urothelial Carcinoma: AUA/SUO Guideline. J. Urol. 2023, 209, 1071–1081. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in health care. Can. Med Assoc. J. 2010, 182, E839–E842. [Google Scholar] [CrossRef]
- Brouwers, M.C.; Kerkvliet, K.; Spithoff, K.; AGREE Next Steps Consortium. The AGREE Reporting Checklist: A tool to improve reporting of clinical practice guidelines. BMJ 2016, 352, i1152. [Google Scholar] [CrossRef] [PubMed]
- Flaig, T.W.; Spiess, P.E.; Abern, M.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Chan, K.; Chang, S.; Friedlander, T.; et al. NCCN Guidelines® Insights: Bladder Cancer, Version 2.2022. J. Natl. Compr. Can. Netw. 2022, 20, 866–878. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Shariat, S.F.; Favaretto, R.L.; Gupta, A.; Fritsche, H.M.; Matsumoto, K.; Kassouf, W.; Walton, T.J.; Tritschler, S.; Baba, S.; Matsushita, K.; et al. Gender differences in radical nephroureterectomy for upper tract urothelial carcinoma. World J. Urol. 2011, 29, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Soria, F.; Shariat, S.F.; Lerner, S.P.; Fritsche, H.-M.; Rink, M.; Kassouf, W.; Spiess, P.E.; Lotan, Y.; Ye, D.; Fernández, M.I.; et al. Epidemiology, diagnosis, preoperative evaluation and prognostic assessment of upper-tract urothelial carcinoma (UTUC). World J. Urol. 2017, 35, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Almås, B.; Halvorsen, O.J.; Johannesen, T.B.; Beisland, C. Higher than expected and significantly increasing incidence of upper tract urothelial carcinoma. A population based study. World J. Urol. 2021, 39, 3385–3391. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, N.; Hotta, H.; Takahashi, A.; Yanase, M.; Itoh, N.; Tachiki, H.; Miyao, N.; Matsukawa, M.; Kunishima, Y.; Taguchi, K.; et al. Upper tract urothelial carcinoma following intravesical bacillus Calmette-Guérin therapy for nonmuscle-invasive bladder cancer: Results from a multi-institutional retrospective study. Urol. Oncol. 2018, 36, 306.e9–306.e15. [Google Scholar] [CrossRef] [PubMed]
- Sanderson, K.M.; Rouprêt, M. Upper urinary tract tumour after radical cystectomy for transitional cell carcinoma of the bladder: An update on the risk factors, surveillance regimens and treatments. BJU Int. 2007, 100, 11–16. [Google Scholar] [CrossRef]
- Uroweb–European Association of Urology. EAU Guidelines on Upper Urinary Tract Urothelial Cell Carcinoma–INTRODUCTION–Uroweb. Available online: https://uroweb.org/guidelines/upper-urinary-tract-urothelial-cell-carcinoma/chapter/introduction (accessed on 4 December 2023).
- Diagnosis and Management of Non-Metastatic Upper Tract Urothelial Carcinoma: AUA/SUO Guideline–American Urological Association. Available online: https://www.auanet.org/guidelines-and-quality/guidelines/non-metastatic-upper-tract-urothelial-carcinoma (accessed on 4 December 2023).
- Dickman, K.G.; Fritsche, H.M.; Grollman, A.P.; Thalmann, G.N.; Catto, J. Epidemiology and Risk Factors for Upper Urinary Urothelial Cancers. In Upper Tract Urothelial Carcinoma; Shariat, S.F., Xylinas, E., Eds.; Springer: New York, NY, USA, 2015; pp. 1–30. [Google Scholar] [CrossRef]
- Zaitsu, M.; Kawachi, I.; Takeuchi, T.; Kobayashi, Y. Alcohol consumption and risk of upper-tract urothelial cancer. Cancer Epidemiol. 2017, 48, 36–40. [Google Scholar] [CrossRef]
- Cerrato, C.; Pandolfo, S.D.; Autorino, R.; Panunzio, A.; Tafuri, A.; Porcaro, A.B.; Veccia, A.; De Marco, V.; Cerruto, M.A.; Antonelli, A.; et al. Gender-specific counselling of patients with upper tract urothelial carcinoma and Lynch syndrome. World J. Urol. 2023, 41, 1741–1749. [Google Scholar] [CrossRef]
- Metcalfe, M.J.; Petros, F.G.; Rao, P.; Mork, M.E.; Xiao, L.; Broaddus, R.R.; Matin, S.F. Universal Point of Care Testing for Lynch Syndrome in Patients with Upper Tract Urothelial Carcinoma. J. Urol. 2018, 199, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Umar, A.; Boland, C.R.; Terdiman, J.P.; Syngal, S.; Chapelle, A.D.L.; Rüschoff, J.; Fishel, R.; Lindor, N.M.; Burgart, L.J.; Hamelin, R.; et al. Revised Bethesda Guidelines for hereditary nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite instability. J. Natl. Cancer Inst. 2004, 96, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Rai, B.P.; Escrig, J.L.D.; Vale, L.; Kuusk, T.; Capoun, O.; Soukup, V.; Bruins, H.M.; Yuan, Y.; Violette, P.D.; Santesso, N.; et al. Systematic Review of the Incidence of and Risk Factors for Urothelial Cancers and Renal Cell Carcinoma Among Patients with Haematuria. Eur. Urol. 2022, 82, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Baard, J.; Cormio, L.; Cavadas, V.; Alcaraz, A.; Shariat, S.F.; de la Rosette, J.; Laguna, M.P. Contemporary patterns of presentation, diagnostics and management of upper tract urothelial cancer in 101 centres: The Clinical Research Office of the Endourological Society Global upper tract urothelial carcinoma registry. Curr. Opin. Urol. 2021, 31, 354–362. [Google Scholar] [CrossRef]
- Jakus, D.; Šolić, I.; Borovac, J.A.; Šitum, M. The influence of the initial clinical presentation of upper tract urothelial carcinoma on histopathological tumor features. Int. Urol. Nephrol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Rud, E.; Galtung, K.F.; Lauritzen, P.M.; Baco, E.; Flatabø, T.; Sandbæk, G. Examining the upper urinary tract in patients with hematuria-time to revise the CT urography protocol? Eur. Radiol. 2020, 30, 1664–1670. [Google Scholar] [CrossRef] [PubMed]
- Janisch, F.; Shariat, S.F.; Baltzer, P.; Fajkovic, H.; Kimura, S.; Iwata, T.; Korn, P.; Yang, L.; Glybochko, P.V.; Rink, M.; et al. Diagnostic performance of multidetector computed tomographic (MDCTU) in upper tract urothelial carcinoma (UTUC): A systematic review and meta-analysis. World J. Urol. 2020, 38, 1165–1175. [Google Scholar] [CrossRef]
- Tsikitas, L.A.; Hopstone, M.D.; Raman, A.; Duddalwar, V. Imaging in Upper Tract Urothelial Carcinoma: A Review. Cancers 2023, 15, 5040. [Google Scholar] [CrossRef]
- Razavi, S.A.; Sadigh, G.; Kelly, A.M.; Cronin, P. Comparative effectiveness of imaging modalities for the diagnosis of upper and lower urinary tract malignancy: A critically appraised topic. Acad. Radiol. 2012, 19, 1134–1140. [Google Scholar] [CrossRef]
- Potretzke, A.M.; Knight, B.A.; Vetter, J.M.; Anderson, B.G.; Hardi, A.C.; Bhayani, S.B.; Figenshau, R.S. Diagnostic Utility of Selective Upper Tract Urinary Cytology: A Systematic Review and Meta-analysis of the Literature. Urology 2016, 96, 35–43. [Google Scholar] [CrossRef]
- Vashistha, V.; Shabsigh, A.; Zynger, D.L. Utility and diagnostic accuracy of ureteroscopic biopsy in upper tract urothelial carcinoma. Arch. Pathol. Lab. Med. 2013, 137, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Katayama, S.; Laukhtina, E.; Schuettfort, V.M.; Pradere, B.; Quhal, F.; Motlagh, R.S.; Mostafaei, H.; Grossmann, N.C.; Rajwa, P.; et al. Discordance Between Clinical and Pathological Staging and Grading in Upper Tract Urothelial Carcinoma. Clin. Genitourin. Cancer. 2022, 20, 95.e1–95.e6. [Google Scholar] [CrossRef]
- Voskuilen, C.S.; Schweitzer, D.; Jensen, J.B.; Nielsen, A.M.; Joniau, S.; Muilwijk, T.; Necchi, A.; Azizi, M.; Spiess, P.E.; Briganti, A.; et al. Diagnostic Value of 18F-fluorodeoxyglucose Positron Emission Tomography with Computed Tomography for Lymph Node Staging in Patients with Upper Tract Urothelial Carcinoma. Eur. Urol. Oncol. 2020, 3, 73–79. [Google Scholar] [CrossRef]
- Rouprêt, M.; Colin, P.; Yates, D.R. A new proposal to risk stratify urothelial carcinomas of the upper urinary tract (UTUCs) in a predefinitive treatment setting: Low-risk versus high-risk UTUCs. Eur. Urol. 2014, 66, 181–183. [Google Scholar] [CrossRef] [PubMed]
- Seisen, T.; Colin, P.; Rouprêt, M. Risk-adapted strategy for the kidney-sparing management of upper tract tumours. Nat. Rev. Urol. 2015, 12, 155–166. [Google Scholar] [CrossRef]
- Messer, J.C.; Terrell, J.D.; Herman, M.P.; Ng, C.K.; Scherr, D.S.; Scoll, B.; Boorjian, S.A.; Uzzo, R.G.; Wille, M.; Eggener, S.E.; et al. Multi-institutional validation of the ability of preoperative hydronephrosis to predict advanced pathologic tumor stage in upper-tract urothelial carcinoma. Urol. Oncol. 2013, 31, 904–908. [Google Scholar] [CrossRef]
- Foerster, B.; Abufaraj, M.; Mari, A.; Seisen, T.; Bandini, M.; Schweitzer, D.; Czech, A.K.; Moschini, M.; D’andrea, D.; Bianchi, M.; et al. The Performance of Tumor Size as Risk Stratification Parameter in Upper Tract Urothelial Carcinoma (UTUC). Clin. Genitourin. Cancer. 2021, 19, 272.e1–272.e7. [Google Scholar] [CrossRef]
- Zeng, S.; Ying, Y.; Yu, X.; Wang, L.; Zhang, Z.; Xu, C. Impact of previous, simultaneous or intravesical recurrence bladder cancer on prognosis of upper tract urothelial carcinoma after nephroureterectomy: A large population-based study. Transl. Androl. Urol. 2021, 10, 4365–4375. [Google Scholar] [CrossRef]
- Ma, R.; Xia, H.; Qiu, M.; Tao, L.; Lu, M.; Huang, R.; Lu, J.; Ma, L. A Diagnostic Nomogram of Pathologic Grade for Preoperative Risk Stratification in Upper Tract Urothelial Carcinoma. Clin. Med. Insights Oncol. 2020, 14, 1179554920927662. [Google Scholar] [CrossRef] [PubMed]
- Cerrato, C.; Patel, D.; Autorino, R.; Simone, G.; Yang, B.; Uzzo, R.; Porpiglia, F.; Capitanio, U.; Porter, J.; Beksac, A.T.; et al. Partial or radical nephrectomy for complex renal mass: A comparative analysis of oncological outcomes and complications from the ROSULA (Robotic Surgery for Large Renal Mass) Collaborative Group. World J. Urol. 2023, 41, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Shigeta, K.; Kikuchi, E.; Abe, T.; Hagiwara, M.; Ogihara, K.; Anno, T.; Umeda, K.; Baba, Y.; Sanjo, T.; Shojo, K.; et al. A Novel Risk-based Approach Simulating Oncological Surveillance after Radical Nephroureterectomy in Patients with Upper Tract Urothelial Carcinoma. Eur. Urol. Oncol. 2020, 3, 756–763. [Google Scholar] [CrossRef]
- Cerrato, C.; Meagher, M.F.; Autorino, R.; Simone, G.; Yang, B.; Uzzo, R.G.; Kutikov, A.; Porpiglia, F.; Capitanio, U.; Montorsi, F.; et al. Partial versus radical nephrectomy for complex renal mass: Multicenter comparative analysis of functional outcomes (Rosula collaborative group). Minerva Urol. Nephrol. 2023, 75, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Aziz, A.; Fritsche, H.-M.; Gakis, G.; Kluth, L.A.; Hassan, F.A.-S.; Engel, O.; Dahlem, R.; Otto, W.; Gierth, M.; Denzinger, S.; et al. Comparative analysis of comorbidity and performance indices for prediction of oncological outcomes in patients with upper tract urothelial carcinoma who were treated with radical nephroureterectomy. Urol. Oncol. 2014, 32, 1141–1150. [Google Scholar] [CrossRef]
- Nardelli, C.; Aveta, A.; Pandolfo, S.D.; Tripodi, L.; Russo, F.; Imbimbo, C.; Castaldo, G.; Pastore, L. Microbiome Profiling in Bladder Cancer Patients Using the First-morning Urine Sample. Eur. Urol. Open Sci. 2024, 59, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Kaag, M.; Trost, L.; Thompson, R.H.; Favaretto, R.; Elliott, V.; Shariat, S.F.; Maschino, A.; Vertosick, E.; Raman, J.D.; Dalbagni, G. Preoperative predictors of renal function decline after radical nephroureterectomy for upper tract urothelial carcinoma. BJU Int. 2014, 114, 674–679. [Google Scholar] [CrossRef]
- Lughezzani, G.; Jeldres, C.; Isbarn, H.; Sun, M.; Shariat, S.F.; Alasker, A.; Pharand, D.; Widmer, H.; Arjane, P.; Graefen, M.; et al. Nephroureterectomy and segmental ureterectomy in the treatment of invasive upper tract urothelial carcinoma: A population-based study of 2299 patients. Eur. J. Cancer. 2009, 45, 3291–3297. [Google Scholar] [CrossRef]
- Yakoubi, R.; Colin, P.; Seisen, T.; Léon, P.; Nison, L.; Bozzini, G.; Shariat, S.; Rouprêt, M. Radical nephroureterectomy versus endoscopic procedures for the treatment of localised upper tract urothelial carcinoma: A meta-analysis and a systematic review of current evidence from comparative studies. Eur. J. Surg. Oncol. 2014, 40, 1629–1634. [Google Scholar] [CrossRef] [PubMed]
- Matin, S.F.; Pierorazio, P.M.; Kleinmann, N.; Gore, J.L.; Shabsigh, A.; Hu, B.; Chamie, K.; Godoy, G.; Hubosky, S.G.; Rivera, M.; et al. Durability of Response to Primary Chemoablation of Low-Grade Upper Tract Urothelial Carcinoma Using UGN-101, a Mitomycin-Containing Reverse Thermal Gel: OLYMPUS Trial Final Report. J. Urol. 2022, 207, 779–788. [Google Scholar] [CrossRef]
- Gallioli, A.; Boissier, R.; Territo, A.; Reyes, H.V.; Sanguedolce, F.; Gaya, J.M.; Regis, F.; Subiela, J.D.; Palou, J.; Breda, A. Adjuvant Single-Dose Upper Urinary Tract Instillation of Mitomycin C After Therapeutic Ureteroscopy for Upper Tract Urothelial Carcinoma: A Single-Centre Prospective Non-Randomized Trial. J. Endourol. 2020, 34, 573–580. [Google Scholar] [CrossRef]
- Kleinmann, N.; Matin, S.F.; Pierorazio, P.M.; Gore, J.L.; Shabsigh, A.; Hu, B.; Chamie, K.; Godoy, G.; Hubosky, S.; Rivera, M.; et al. Primary chemoablation of low-grade upper tract urothelial carcinoma using UGN-101, a mitomycin-containing reverse thermal gel (OLYMPUS): An open-label, single-arm, phase 3 trial. Lancet Oncol. 2020, 21, 776–785. [Google Scholar] [CrossRef]
- Fontanet, S.; Gallioli, A.; Baboudjian, M.; Huguet, J.; Territo, A.; Gaya, J.M.; Gavrilov, P.; Izquierdo, P.; Verri, P.; Algaba, F.; et al. Topical instillation of BCG immunotherapy for biopsy-proven primary upper urinary tract carcinoma in situ: A single institution series and systematic review. Urol. Oncol. 2023, 41, 274–283. [Google Scholar] [CrossRef]
- Ha, Y.-S.; Chung, J.-W.; Choi, S.H.; Lee, J.N.; Kim, B.S.; Kim, T.-H.; Yoo, E.S.; Kwon, T.G.; Byun, S.-S.; Choi, Y.D.; et al. Impact of a bladder cuff excision during radical nephroureterectomy on cancer specific survival in patients with upper tract urothelial cancer in Korea: A retrospective, multi-institutional study. Minerva Urol. Nefrol. 2017, 69, 466–474. [Google Scholar] [CrossRef]
- Rouprêt, M.; Smyth, G.; Irani, J.; Guy, L.; Davin, J.-L.; Saint, F.; Pfister, C.; Wallerand, H.; Rozet, F. Oncological risk of laparoscopic surgery in urothelial carcinomas. World J. Urol. 2009, 27, 81–88. [Google Scholar] [CrossRef]
- Piszczek, R.; Nowak, Ł.; Krajewski, W.; Chorbińska, J.; Poletajew, S.; Moschini, M.; Kaliszewski, K.; Zdrojowy, R. Oncological Outcomes of Laparoscopic Nephroureterectomy Versus Open Radical Nephroureterectomy for Upper Tract Urothelial Carcinoma: An European Association of Urology Guidelines Systematic Review. Eur. Urol. Focus. 2019, 5, 205–223. [Google Scholar]
- Xylinas, E.; Rink, M.; Cha, E.K.; Clozel, T.; Lee, R.K.; Fajkovic, H.; Comploj, E.; Novara, G.; Margulis, V.; Raman, J.D.; et al. Impact of distal ureter management on oncologic outcomes following radical nephroureterectomy for upper tract urothelial carcinoma. Eur. Urol. 2014, 65, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Hwang, E.C.; Sathianathen, N.J.; Jung, J.H.; Kim, M.H.; Dahm, P.; Risk, M.C. Single-dose intravesical chemotherapy after nephroureterectomy for upper tract urothelial carcinoma. Cochrane Database Syst. Rev. 2019, 5, CD013160. [Google Scholar] [CrossRef] [PubMed]
- Freifeld, Y.; Ghandour, R.; Singla, N.; Woldu, S.; Bagrodia, A.; Lotan, Y.; Rapoport, L.M.; Gazimiev, M.; Delafuente, K.; Kulangara, R.; et al. Intraoperative prophylactic intravesical chemotherapy to reduce bladder recurrence following radical nephroureterectomy. Urol. Oncol. 2020, 38, 737.e11–737.e16. [Google Scholar] [CrossRef]
- Yoo, S.H.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Choo, M.S.; Ku, J.H. Intravesical Chemotherapy after Radical Nephroureterectomy for Primary Upper Tract Urothelial Carcinoma: A Systematic Review and Network Meta-Analysis. J. Clin. Med. 2019, 8, 1059. [Google Scholar] [CrossRef]
- Margulis, V.; Puligandla, M.; Trabulsi, E.J.; Plimack, E.R.; Kessler, E.R.; Matin, S.F.; Godoy, G.; Alva, A.; Hahn, N.M.; Carducci, M.A.; et al. Phase II Trial of Neoadjuvant Systemic Chemotherapy Followed by Extirpative Surgery in Patients with High Grade Upper Tract Urothelial Carcinoma. J. Urol. 2020, 203, 690–698. [Google Scholar] [CrossRef]
- Kim, D.K.; Lee, J.Y.; Kim, J.W.; Hah, Y.S.; Cho, K.S. Effect of neoadjuvant chemotherapy on locally advanced upper tract urothelial carcinoma: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2019, 135, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Audenet, F.; Yates, D.R.; Cussenot, O.; Rouprêt, M. The role of chemotherapy in the treatment of urothelial cell carcinoma of the upper urinary tract (UUT-UCC). Urol. Oncol. 2013, 31, 407–413. [Google Scholar] [CrossRef]
- Meng, X.; Chao, B.; Vijay, V.; Silver, H.; Margolin, E.J.; Balar, A.; Taneja, S.S.; Shah, O.; Bjurlin, M.A.; Anderson, C.B.; et al. High Response Rates to Neoadjuvant Chemotherapy in High-Grade Upper Tract Urothelial Carcinoma. Urology 2019, 129, 146–152. [Google Scholar] [CrossRef]
- Kubota, Y.; Hatakeyama, S.; Tanaka, T.; Fujita, N.; Iwamura, H.; Mikami, J.; Yamamoto, H.; Tobisawa, Y.; Yoneyama, T.; Yoneyama, T.; et al. Oncological outcomes of neoadjuvant chemotherapy in patients with locally advanced upper tract urothelial carcinoma: A multicenter study. Oncotarget 2017, 8, 101500–101508. [Google Scholar] [CrossRef] [PubMed]
- Hosogoe, S.; Hatakeyama, S.; Kusaka, A.; Hamano, I.; Iwamura, H.; Fujita, N.; Yamamoto, H.; Tobisawa, Y.; Yoneyama, T.; Yoneyama, T.; et al. Platinum-based Neoadjuvant Chemotherapy Improves Oncological Outcomes in Patients with Locally Advanced Upper Tract Urothelial Carcinoma. Eur. Urol. Focus. 2018, 4, 946–953. [Google Scholar] [CrossRef] [PubMed]
- Leow, J.J.; Chong, Y.L.; Chang, S.L.; Valderrama, B.P.; Powles, T.; Bellmunt, J. Neoadjuvant and Adjuvant Chemotherapy for Upper Tract Urothelial Carcinoma: A 2020 Systematic Review and Meta-analysis, and Future Perspectives on Systemic Therapy. Eur. Urol. 2021, 79, 635–654. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J.A.; Yip, W.; Wong, N.C.; Sjoberg, D.D.; Bochner, B.H.; Dalbagni, G.; Donat, S.M.; Herr, H.W.; Cha, E.K.; Donahue, T.F.; et al. Multicenter Phase II Clinical Trial of Gemcitabine and Cisplatin as Neoadjuvant Chemotherapy for Patients With High-Grade Upper Tract Urothelial Carcinoma. J. Clin. Oncol. 2023, 41, 1618–1625. [Google Scholar] [CrossRef]
- Crocerossa, F.; Fiori, C.; Capitanio, U.; Minervini, A.; Carbonara, U.; Pandolfo, S.D.; Loizzo, D.; Eun, D.D.; Larcher, A.; Mari, A.; et al. Estimated Glomerular Filtration Rate Decline at 1 Year after Minimally Invasive Partial Nephrectomy: A Multimodel Comparison of Predictors. Eur. Urol. Open Sci. 2022, 38, 52–59. [Google Scholar] [CrossRef]
- Lane, B.R.; Smith, A.K.; Larson, B.T.; Gong, M.C.; Campbell, S.C.; Raghavan, D.; Dreicer, R.; Hansel, D.E.; Stephenson, A.J. Chronic kidney disease after nephroureterectomy for upper tract urothelial carcinoma and implications for the administration of perioperative chemotherapy. Cancer 2010, 116, 2967–2973. [Google Scholar] [CrossRef]
- De Santis, M.; Bellmunt, J.; Mead, G.; Kerst, J.M.; Leahy, M.; Maroto, P.; Skoneczna, I.; Marreaud, S.; de Wit, R.; Sylvester, R. Randomized phase II/III trial assessing gemcitabine/carboplatin and methotrexate/carboplatin/vinblastine in patients with advanced urothelial cancer «unfit» for cisplatin-based chemotherapy: Phase II––Results of EORTC study 30986. J. Clin. Oncol. 2009, 27, 5634–5639. [Google Scholar] [CrossRef] [PubMed]
- Bajorin, D.F.; Witjes, J.A.; Gschwend, J.E.; Schenker, M.; Valderrama, B.P.; Tomita, Y.; Bamias, A.; Lebret, T.; Shariat, S.F.; Park, S.H.; et al. Adjuvant Nivolumab versus Placebo in Muscle-Invasive Urothelial Carcinoma. N. Engl. J. Med. 2021, 384, 2102–2114. [Google Scholar] [CrossRef] [PubMed]
- Laukhtina, E.; Sari Motlagh, R.; Mori, K.; Katayama, S.; Rajwa, P.; Yanagisawa, T.; Quhal, F.; Mostafaei, H.; Grossmann, N.C.; König, F.; et al. Chemotherapy is superior to checkpoint inhibitors after radical surgery for urothelial carcinoma: A systematic review and network meta-analysis of oncologic and toxicity outcomes. Crit. Rev. Oncol. Hematol. 2022, 169, 103570. [Google Scholar] [CrossRef] [PubMed]
- Board WC of TE. Urinary and Male Genital Tumours. Available online: https://publications.iarc.fr/Book-And-Report-Series/Who-Classification-Of-Tumours/Urinary-And-Male-Genital-Tumours-2022 (accessed on 11 January 2024).
- Wiley.com. TNM Classification of Malignant Tumours, 8th ed.; Wiley: Hoboken, NJ, USA; Available online: https://www.wiley.com/en-us/TNM+Classification+of+Malignant+Tumours%2C+8th+Edition-p-9781119263579 (accessed on 11 January 2024).
- Oge, O.; Erdem, E.; Atsü, N.; Ahin, A.; Ozen, H. Proposal for changes in cystoscopic follow-up of patients with low-grade pTa bladder tumor. Eur. Urol. 2000, 37, 271–274. [Google Scholar] [PubMed]
- Klemm, J.; Bekku, K.; Abufaraj, M.; Laukhtina, E.; Matsukawa, A.; Parizi, M.K.; Karakiewicz, P.I.; Shariat, S.F. Upper Tract Urothelial Carcinoma: A Narrative Review of Current Surveillance Strategies for Non-Metastatic Disease. Cancers 2023, 16, 44. [Google Scholar] [CrossRef] [PubMed]
- Klemm, J.; Bekku, K.; Abufaraj, M.; Laukhtina, E.; Matsukawa, A.; Parizi, M.K.; Karakiewicz, P.I.; Shariat, S.F. Early repeated ureteroscopy within 6–8 weeks after a primary endoscopic treatment in patients with upper tract urothelial cell carcinoma: Preliminary findings. World J. Urol. 2016, 34, 1201–1206. [Google Scholar]
- Holmäng, S.; Johansson, S.L. Long-term follow-up of patients with tumours of the renal pelvis and ureter: How often is a bladder tumour diagnosed after five tumour-free years? Scand. J. Urol. 2014, 48, 65–72. [Google Scholar] [CrossRef]
- Mohapatra, A.; Strope, S.A.; Liu, N.; Winer, A.; Benfante, N.E.; Coleman, J.A.; Vetter, J.; Murray, K.S. Importance of long-term follow-up after endoscopic management for upper tract urothelial carcinoma and factors leading to surgical management. Int. Urol. Nephrol. 2020, 52, 1465–1469. [Google Scholar] [CrossRef]
- Shigeta, K.; Kikuchi, E.; Hagiwara, M.; Ando, T.; Mizuno, R.; Abe, T.; Mikami, S.; Miyajima, A.; Nakagawa, K.; Oya, M. The Conditional Survival with Time of Intravesical Recurrence of Upper Tract Urothelial Carcinoma. J. Urol. 2017, 198, 1278–1285. [Google Scholar] [CrossRef]
- Martini, A.; Lonati, C.; Nocera, L.; Fallara, G.; Raggi, D.; Herout, R.; Zamboni, S.; Ploussard, G.; Predere, B.; Mattei, A.; et al. Oncologic Surveillance after Radical Nephroureterectomy for High-risk Upper Tract Urothelial Carcinoma. Eur. Urol. Oncol. 2022, 5, 451–459. [Google Scholar] [CrossRef]
- Katims, A.B.; Say, R.; Derweesh, I.; Uzzo, R.; Minervini, A.; Wu, Z.; Abdollah, F.; Sundaram, C.; Ferro, M.; Rha, K.; et al. Risk Factors for Intravesical Recurrence after Minimally Invasive Nephroureterectomy for Upper Tract Urothelial Cancer (ROBUUST Collaboration). J. Urol. 2021, 206, 568–576. [Google Scholar] [CrossRef]
- Locke, J.A.; Hamidizadeh, R.; Kassouf, W.; Rendon, R.A.; Bell, D.; Izawa, J.; Chin, J.; Kapoor, A.; Shayegan, B.; Lattouf, J.-B.; et al. Surveillance guidelines based on recurrence patterns for upper tract urothelial carcinoma. Can. Urol. Assoc. J. 2018, 12, 243–251. [Google Scholar] [CrossRef]
- Li, X.; Cui, M.; Gu, X.; Fang, D.; Li, H.; Qin, S.; Yang, K.; Zhu, T.; Li, X.; Zhou, L.; et al. Pattern and risk factors of local recurrence after nephroureterectomy for upper tract urothelial carcinoma. World J. Surg. Oncol. 2020, 18, 114. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Management Type | AUA | EAU | NCCN |
|---|---|---|---|
| Neoadjuvant platinum-based chemotherapy | Patients with local or distant invasive tumors or involved lymph nodes When GFR is expected to lower after surgical treatment | When GFR is expected to lower after surgical treatment | Patients with retroperitoneal lymphadenopathy, bulky (>3 cm) high-grade tumor, sessile histology, or suspected parenchymal invasion |
| Endoscopic management | Low-risk and high-risk favorable UTUC | Low-risk masses | Only for selected patients or those who are not suitable for RNU |
| Post-endoscopic instillation | Mitomycin C gel or BCG | Mitomycin C gel | Mitomycin C gel |
| RNU with bladder cuff and LND | Open/laparoscopic according to surgeon preference Remove en block, watertight fashion LND in high-risk UTUC | Open approach is superior for fewer risks of cells dissemination LND in high-risk UTUC | No specific indication |
| Post-RNU bladder instillation (Mitomycin C or Gemcitabine) | According to availability | Gemcitabine preferred in case of risk of extravasation | No specific indication |
| Adjuvant chemotherapy | Up to a GFR of 60 mL/min | Up to a GFR of 45 mL/min | Up to a GFR of 60 mL/min |
| Immunotherapy in high-risk muscle-invasive UTUC, undergone RNU and cell PD-L1 expression > 1% | No specific indication | No specific indication | No specific indication |
| LOW-RISK UTUC | |||||||
|---|---|---|---|---|---|---|---|
| Diagnostic Procedure | Guideline | Early Second-Look | First Year | Second Year | Third Year | Fourth–Fifth Years | Further Assessment |
| Cystoscopy and cytology | AUA | Within 4–8 weeks | At 6 to 9 months | At 6 to 9 months | Yearly | Yearly | Decision made between the patient and clinician |
| EAU | Within 6–8 weeks | 3 and 9 months | Yearly | Yearly | Yearly | Stop after 5 years | |
| NCCN | NA | Every 3-months | Not specified | Not specified | Not specified | Not specified | |
| Ureteroscopy | AUA | Within 4–8 weeks | At 6 to 9 months | At 6 to 9 months | Yearly | Yearly | Decision made between the patient and clinician |
| EAU | Within 6–8 weeks | 3 and 6 months | Yearly | Yearly | Yearly | Stop after 5 years | |
| NCCN | NA | 3 to 12 months | Not specified | Not specified | Not specified | Not specified | |
| Imaging | AUA | NA | At 6 to 9 months | At 6 to 9 months | Yearly | Yearly | Stop after 5 years |
| EAU | NA | CT-urography at 3 and 6 months | Yearly | Yearly | Yearly | Stop after 5 years | |
| NCCN | NA | Abdominal/pelvic CT or MRI at 3 to 12 months | Not specified | Not specified | Not specified | Not specified | |
| HIGH-RISK UTUC | |||||||
| Diagnostic Procedure | Guideline | Early Second-Look | First Year | Second Year | Third Year | Fourth–Fifth Years | Further Assessment |
| Cystoscopy and cytology | AUA | Within 4–8 weeks | Every 3 to 6 months | Every 3 to 6 months | Every 3 to 6 months | Yearly | Encourage to continue follow-up |
| EAU | Within 6–8 weeks | A 3 and 9 months | Yearly | Yearly | Yearly | Continue in accordance with the patient | |
| NCCN | NA | Every 3-months | Not specified | Not specified | Not specified | Not specified | |
| Ureteroscopy | AUA | Within 4–8 weeks | At 6 and 12 months | At 6 to 9 months | Yearly | Yearly | Encourage to continue follow-up |
| EAU | Within 6–8 weeks | 3 and 6 months | Yearly | Yearly | Yearly | Continue in accordance with the patient | |
| NCCN | NA | Not specified | Not specified | Not specified | Not specified | Not specified | |
| Imaging | AUA | NA | Every 3 to 6 months | Every 3 to 6 months | Every 3 to 6 months | Yearly | Encourage to continue follow-up |
| EAU | NA | CT-urography at 3 and 6 months | Yearly | Yearly | Yearly | Continue in accordance with the patient | |
| NCCN | NA | Not specified | Not specified | Not specified | Not specified | Not specified | |
| LOW-RISK UTUC | ||||||
|---|---|---|---|---|---|---|
| Diagnostic Procedure | Guideline | First Year | Second Year | Third Year | Fourth–Fifth Years | Further Assessment |
| Cystoscopy and cytology | AUA | At 3 months and then at 6 to 9 months | At 6 to 9 months | Yearly | Yearly | Decision made between the patient and clinician |
| EAU | 3 and 9 months | Yearly | Yearly | Yearly | Stop after 5 years | |
| NCCN | Every 3-months | Not specified | Not specified | Not specified | Not specified | |
| Imaging | AUA | At 6 to 9 months | At 6 to 9 months | Yearly | Yearly | Decision made between the patient and clinician |
| EAU | CT-urography at 3 and 6 months | Yearly | Yearly | Yearly | Stop after 5 years | |
| NCCN | Abdominal/pelvic CT or MRI at 3 to 12 months | Not specified | Not specified | Not specified | Not specified | |
| HIGH-RISK UTUC | ||||||
| Diagnostic Procedure | Guideline | First Year | Second Year | Third Year | Fourth–Fifth Years | Further assessment |
| Cystoscopy and cytology | AUA | At 3 to 6 months | At 3 to 6 months | At 3 to 6 months | Yearly | Encourage to continue follow-up |
| EAU | 3 and 9 months | Yearly | Yearly | Yearly | Stop after 5 years | |
| NCCN | Every 3-months | Not specified | Not specified | Not specified | Not specified | |
| Imaging | AUA (<T2N0M0) | Abdominal/pelvic CT or MRI within 6 months | Yearly | Yearly | Yearly | Encourage to continue follow-up |
| AUA (>T2N0M0) | CT-urography every 3 to 6 months | CT-urography every 3 to 6 months | CT-urography every 6 months | |||
| EAU | CT-urography at 3 and 6 months | Yearly | Yearly | Yearly | Stop after 5 years | |
| NCCN | Abdominal/pelvic CT or MRI at 3 to 12 months | Not specified | Not specified | Not specified | Not specified | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pandolfo, S.D.; Cilio, S.; Aveta, A.; Wu, Z.; Cerrato, C.; Napolitano, L.; Lasorsa, F.; Lucarelli, G.; Verze, P.; Siracusano, S.; et al. Upper Tract Urothelial Cancer: Guideline of Guidelines. Cancers 2024, 16, 1115. https://doi.org/10.3390/cancers16061115
Pandolfo SD, Cilio S, Aveta A, Wu Z, Cerrato C, Napolitano L, Lasorsa F, Lucarelli G, Verze P, Siracusano S, et al. Upper Tract Urothelial Cancer: Guideline of Guidelines. Cancers. 2024; 16(6):1115. https://doi.org/10.3390/cancers16061115
Chicago/Turabian StylePandolfo, Savio Domenico, Simone Cilio, Achille Aveta, Zhenjie Wu, Clara Cerrato, Luigi Napolitano, Francesco Lasorsa, Giuseppe Lucarelli, Paolo Verze, Salvatore Siracusano, and et al. 2024. "Upper Tract Urothelial Cancer: Guideline of Guidelines" Cancers 16, no. 6: 1115. https://doi.org/10.3390/cancers16061115
APA StylePandolfo, S. D., Cilio, S., Aveta, A., Wu, Z., Cerrato, C., Napolitano, L., Lasorsa, F., Lucarelli, G., Verze, P., Siracusano, S., Quattrone, C., Ferro, M., Bologna, E., Campi, R., Del Giudice, F., Bertolo, R., Amparore, D., Palumbo, S., Manfredi, C., & Autorino, R. (2024). Upper Tract Urothelial Cancer: Guideline of Guidelines. Cancers, 16(6), 1115. https://doi.org/10.3390/cancers16061115