
Retrospective Observational Study to Determine the Epidemiology and Treatment Patterns of Patients with Triple-Negative Breast Cancer

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population and Timeline
2.2.1. Inclusion Criteria
- Confirmed diagnosis of TNBC (as per ASCO criteria) with ER, PR, and HER2 documented in medical notes or histopathology reports. TNBC status was confirmed following ASCO/CAP (College of American Pathologists) guidelines [16], where ER and PR expression below 1% determined by immunohistochemistry (IHC) was considered negative. For HER2, ratios between 0 and 1+ by IHC or IHC ratio 2+ with negative fluorescence in situ hybridisation (FISH) were considered negative. The status of ER, PR, and HER2 was manually verified based on available medical documentation.
- Treated at MSCI between 1 January 2015 and 30 December 2020.
- Newly admitted to MSCI between 1 January 2015 and 30 December 2020, and not treated prior to admission to MSCI.
- Stage I to stage IIIB at the first evaluation at MSCI. Each patient had their clinical anatomical staging (cTNM) assessed as the baseline, within the first 6 months of the first admission date.
2.2.2. Exclusion Criteria
- Admitted for consultation only (i.e., only one outpatient visit with C50 code).
- Not treated in MSCI during the index period of 1 January 2015, to 30 December 2020 (i.e., no surgery, chemotherapy, or radiotherapy).
2.2.3. Follow-Up
2.2.4. Data Source
2.3. Study Procedures
2.3.1. Data Handling, Validation and Quality Assurance
2.3.2. Data Extraction
2.3.3. Software
2.3.4. Data Quality Control
2.3.5. Statistical Analysis
3. Results
3.1. Study Population
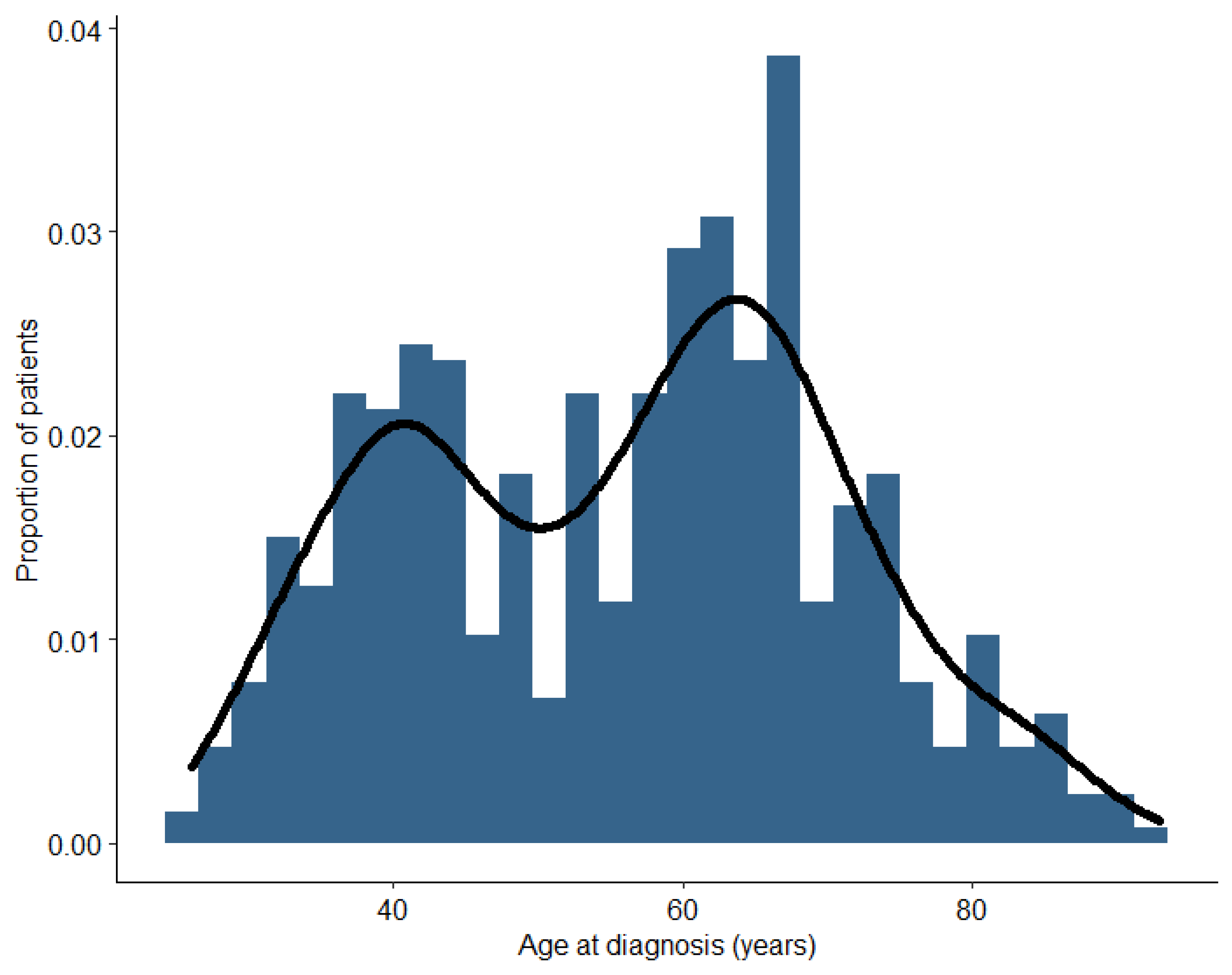
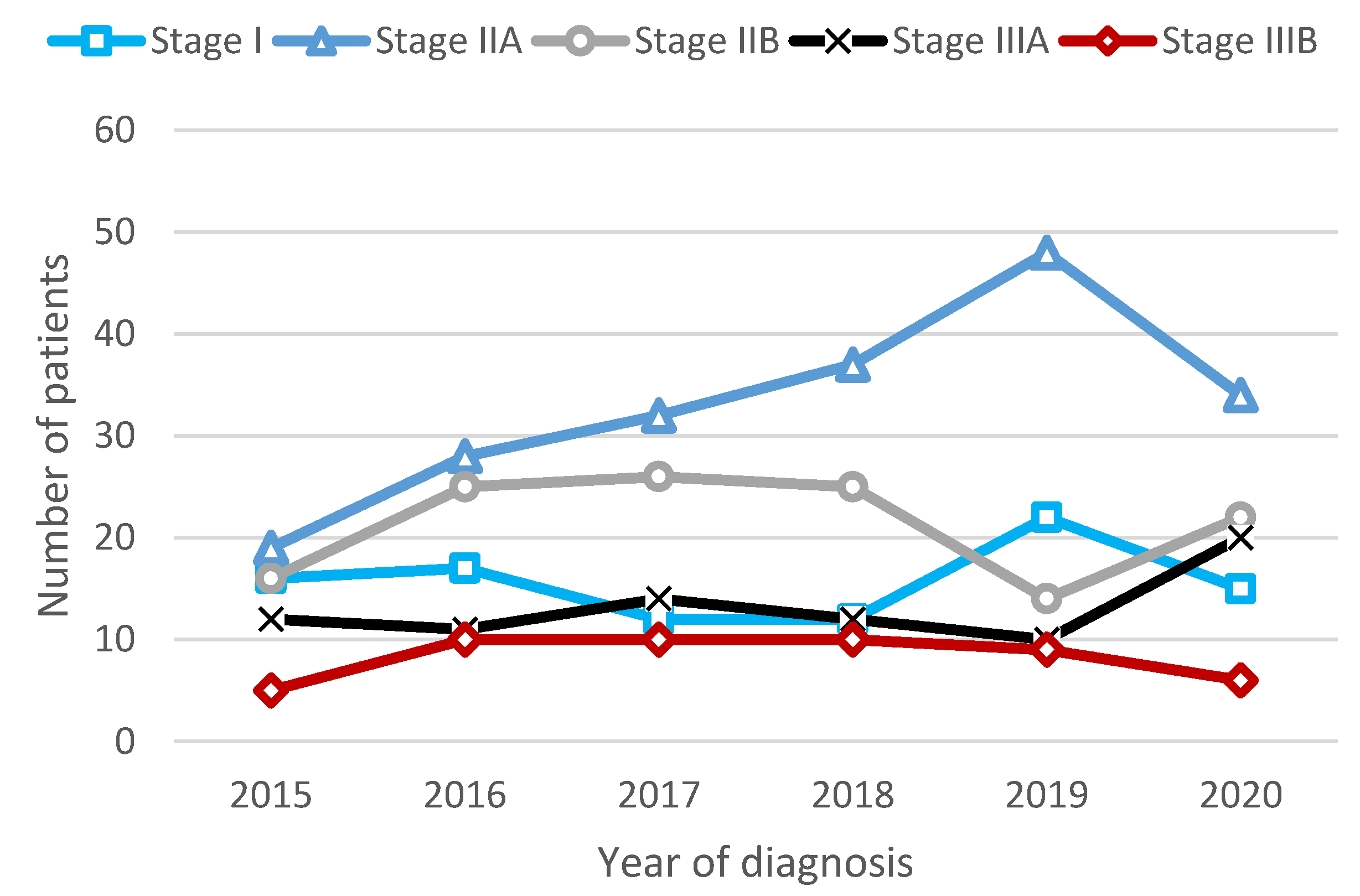
3.2. Characteristics of Early-Stage or Locally Advanced TNBC Cases
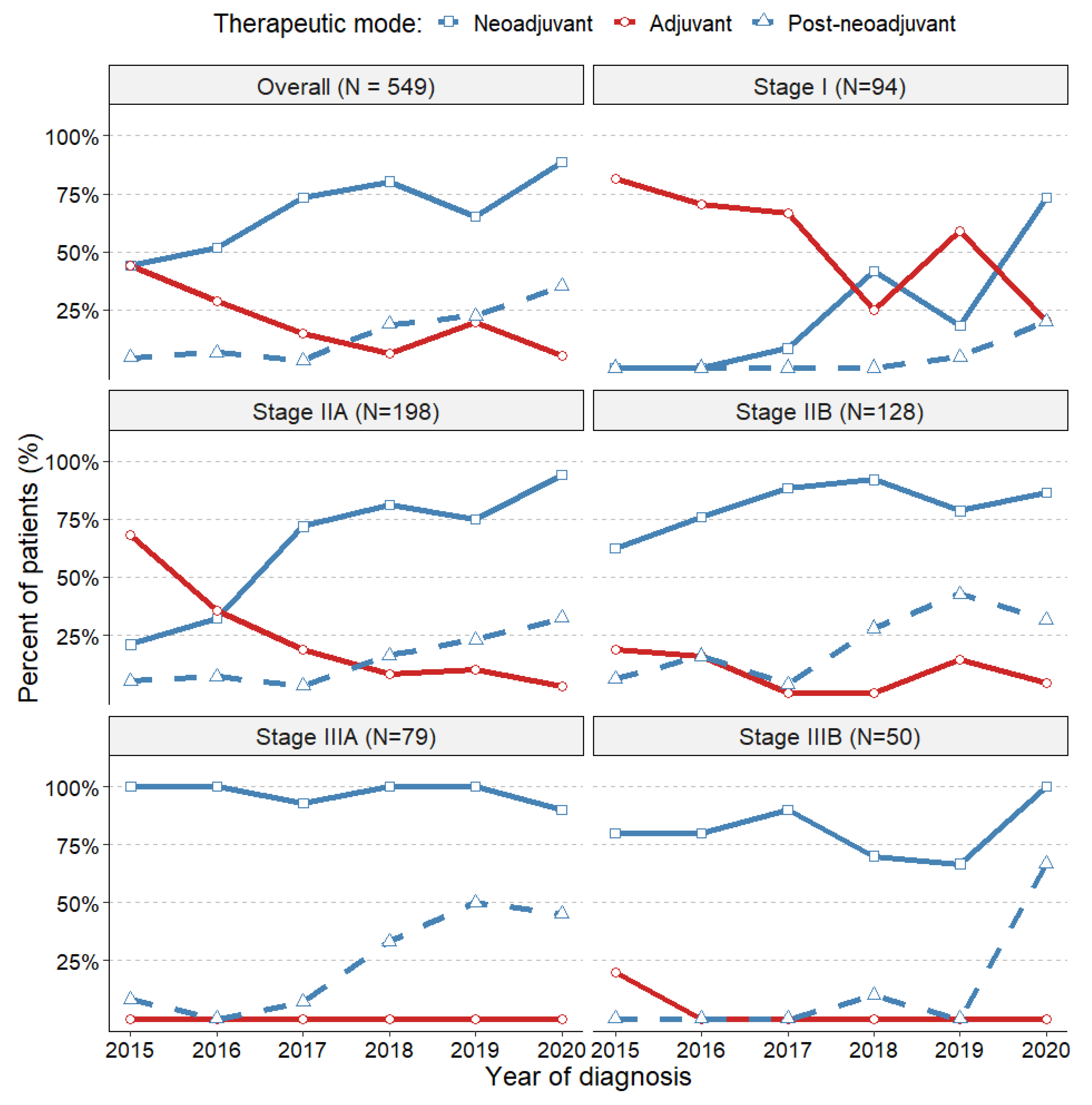
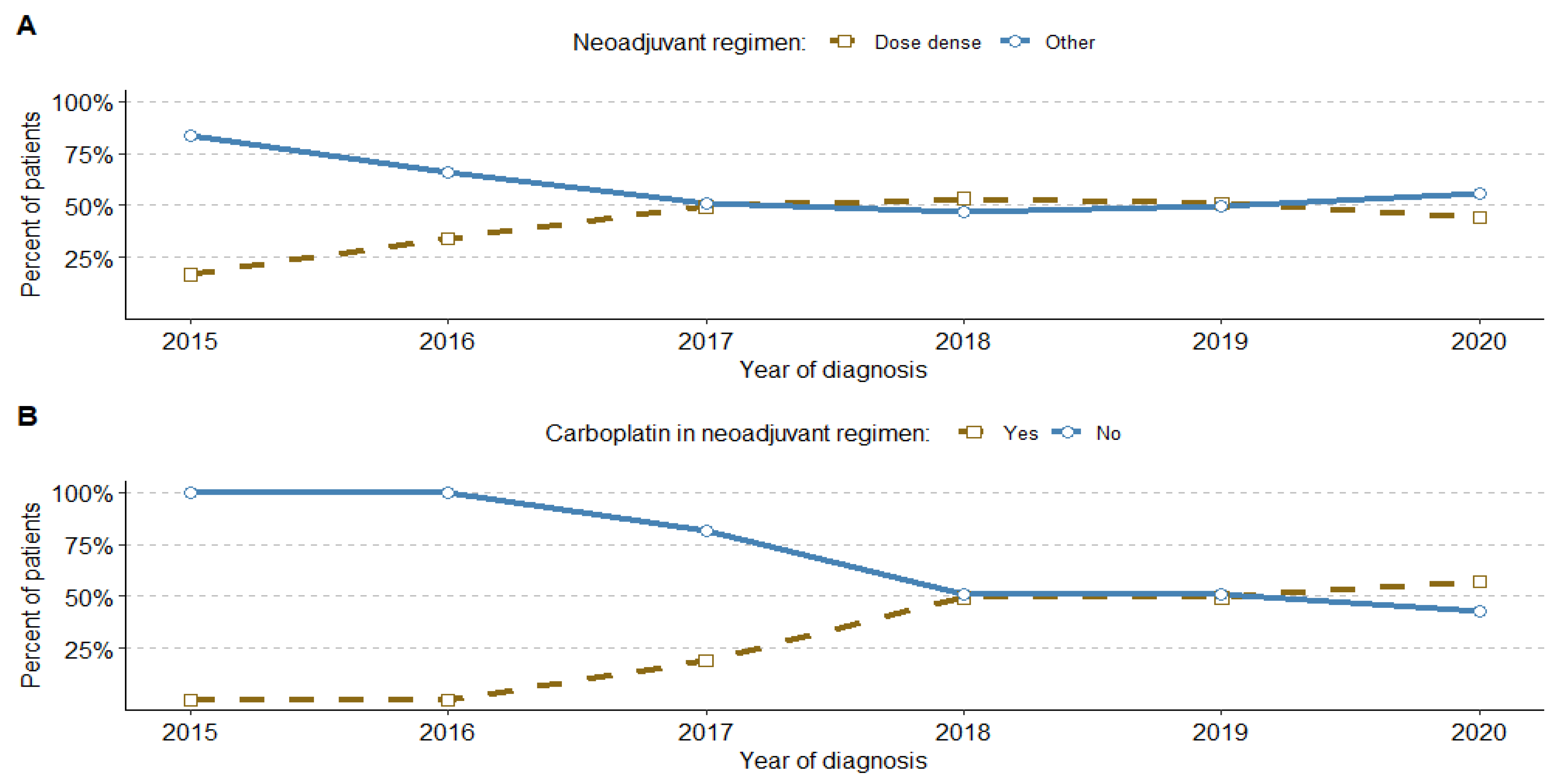
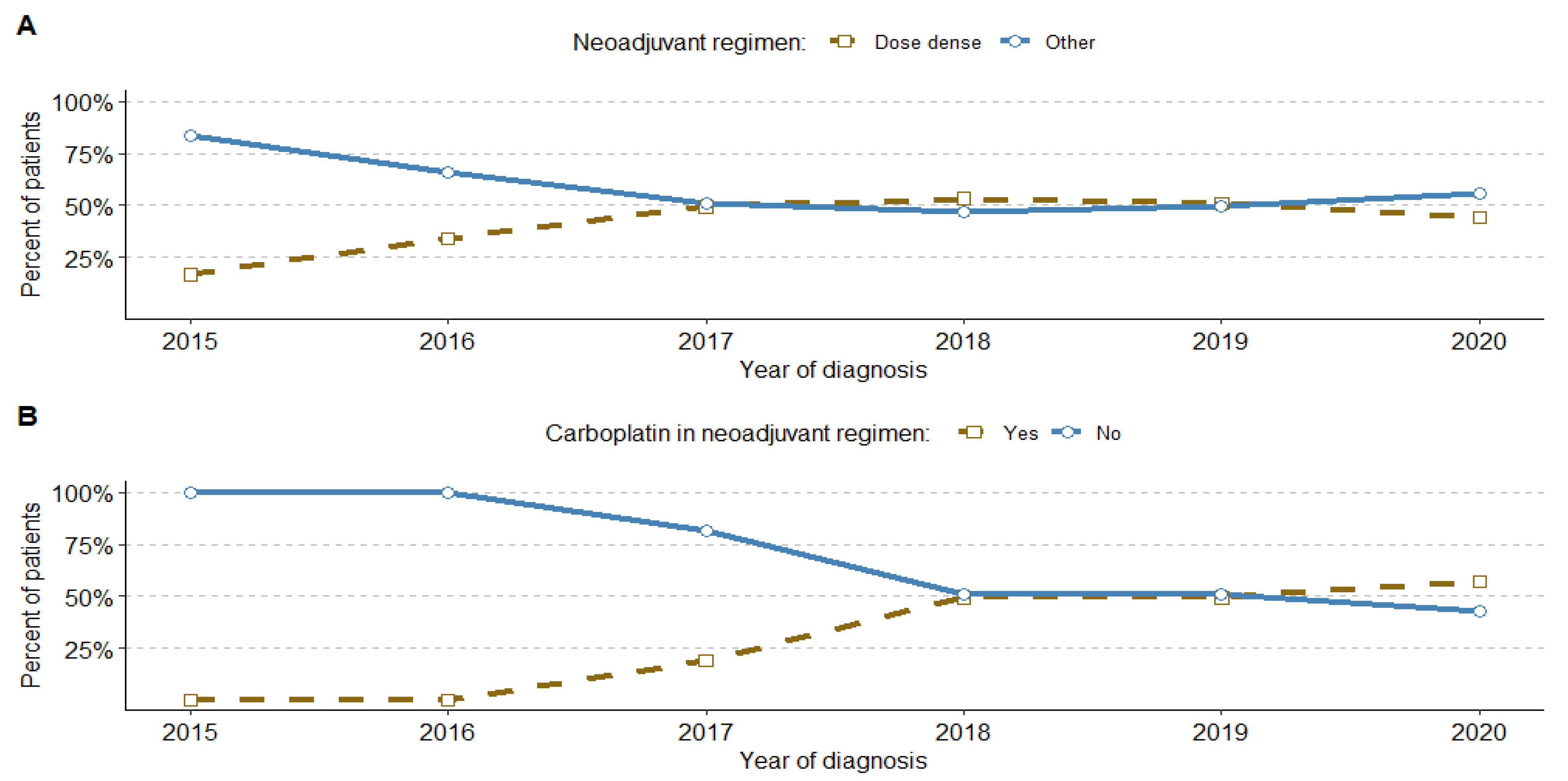
3.3. Systemic Treatment Trends
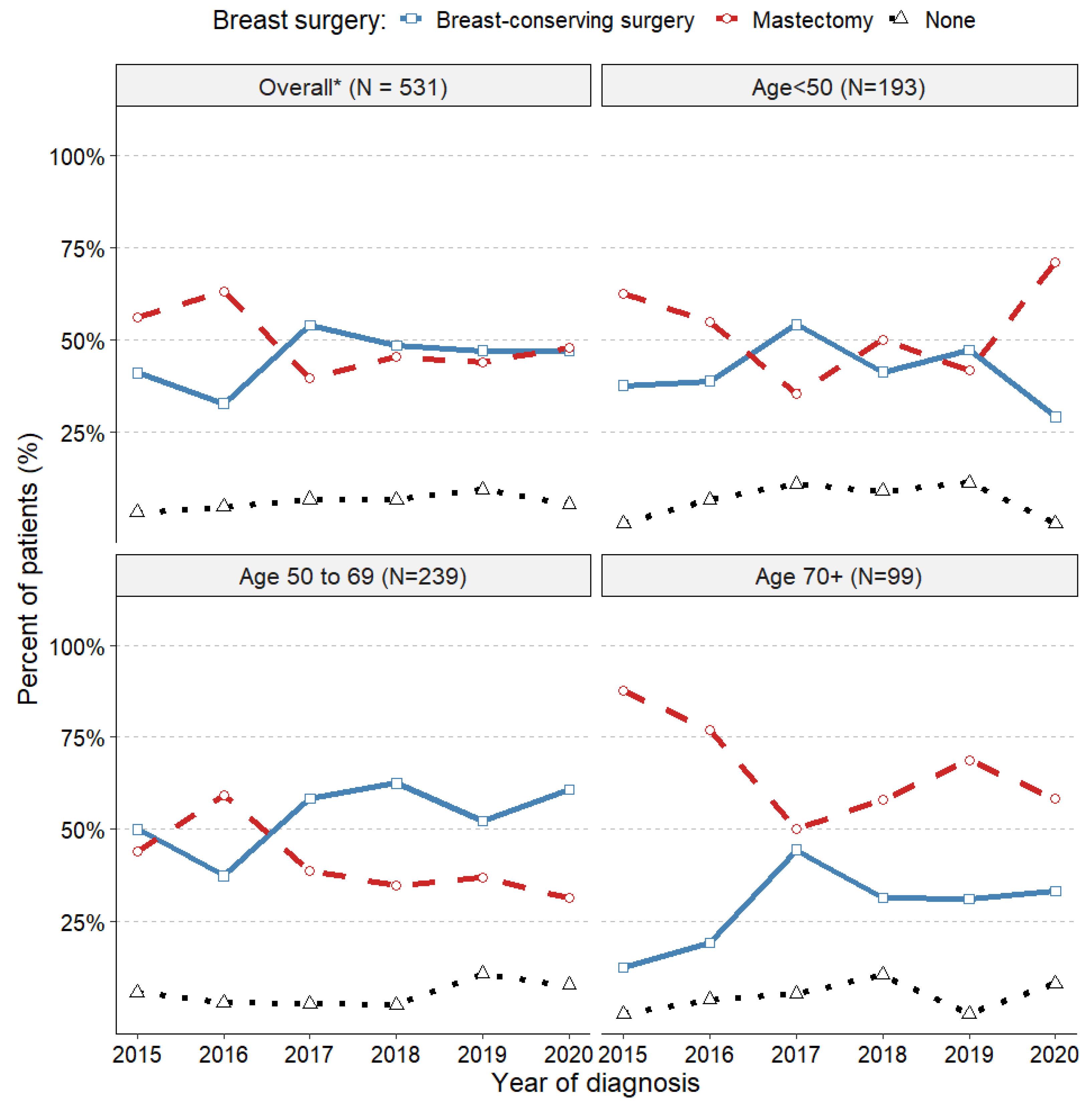
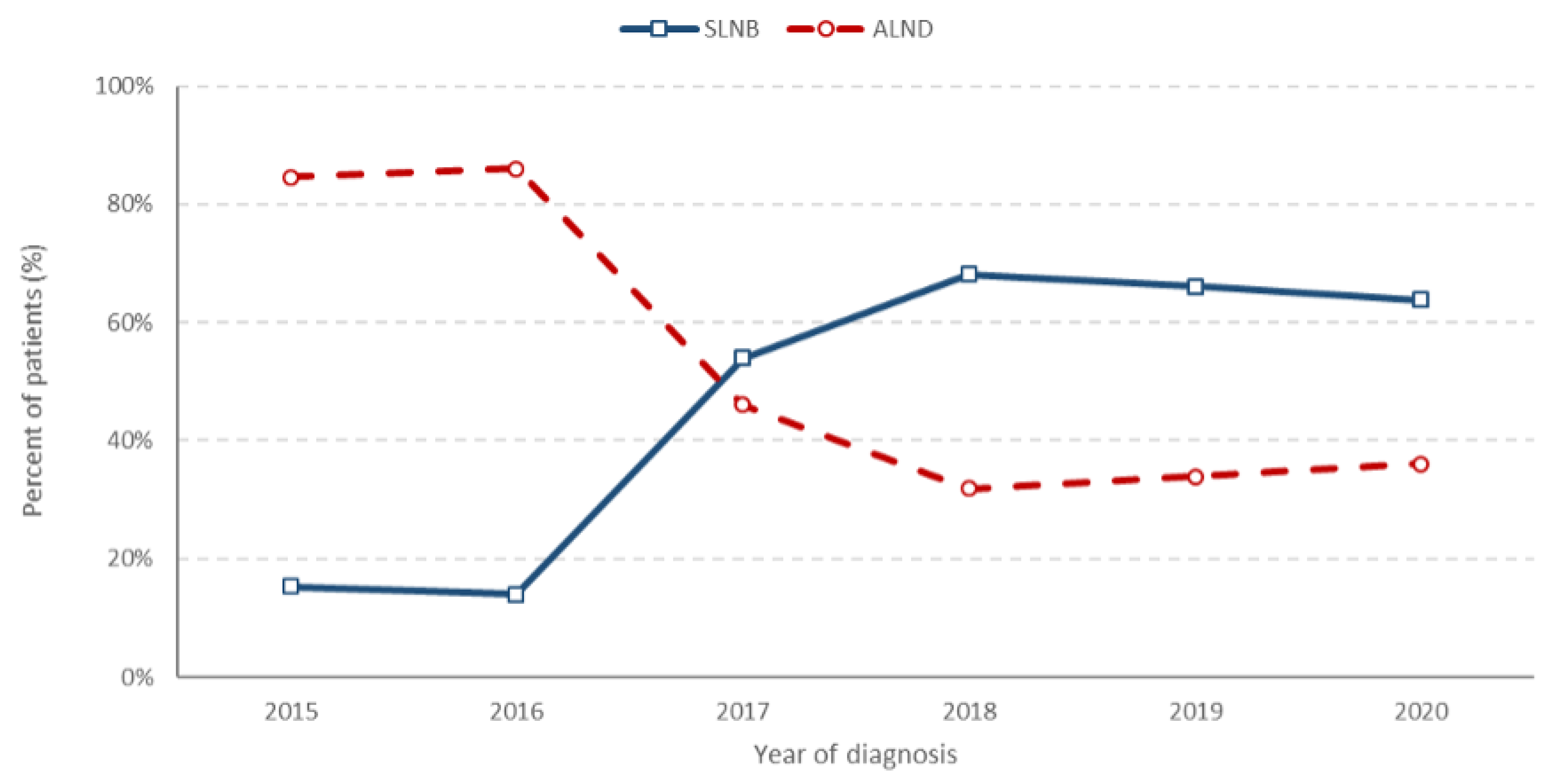
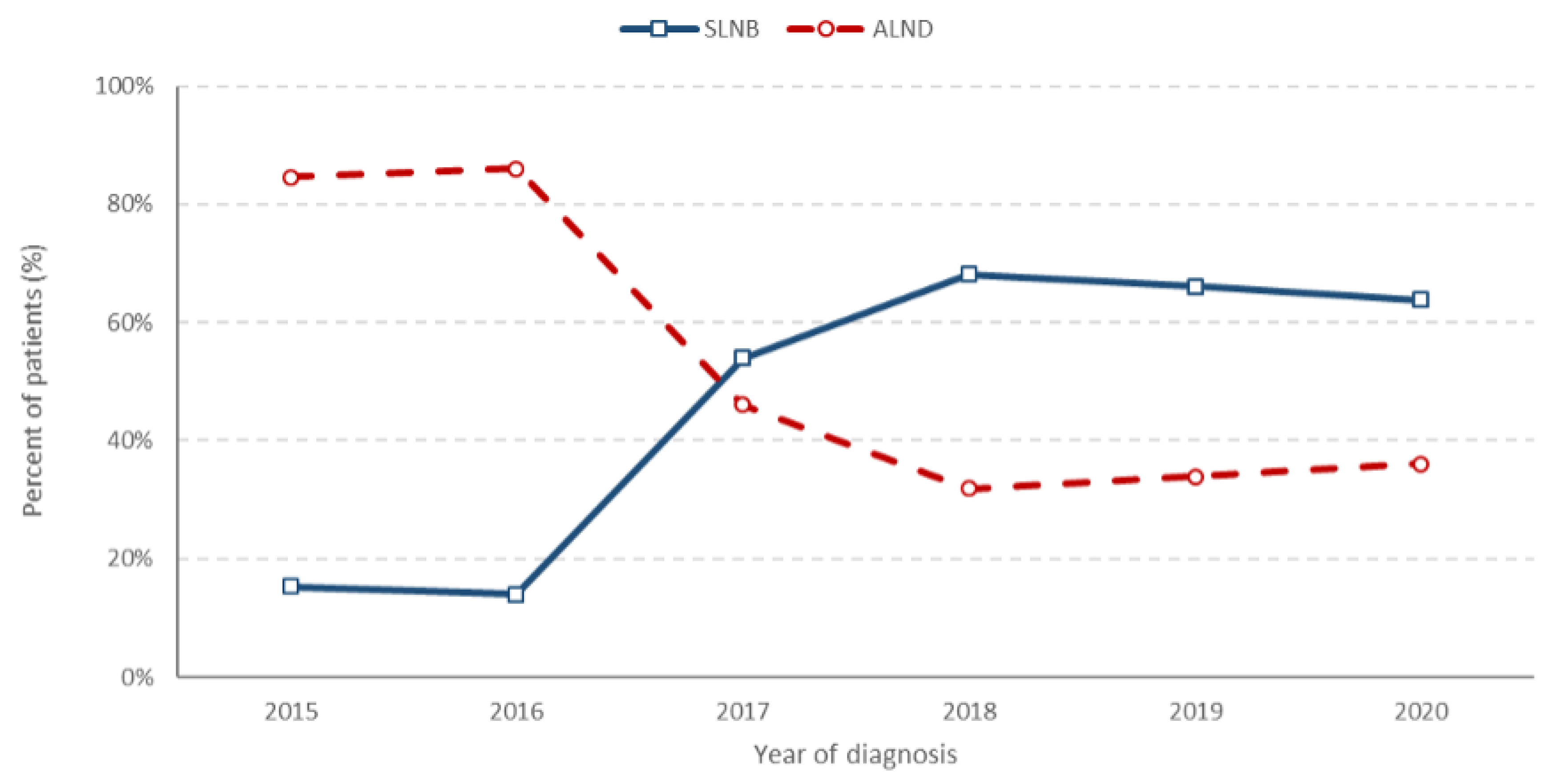
3.4. Trends in Surgical Treatments
4. Discussion
4.1. Limitations
4.2. Summary
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coates, A.S.; Winer, E.P.; Goldhirsch, A.; Gelber, R.D.; Gnant, M.; Piccart-Gebhart, M.; Thurlimann, B.; Senn, H.J.; Panel, M. Tailoring therapies—Improving the management of early breast cancer: St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann. Oncol. 2015, 26, 1533–1546. [Google Scholar] [CrossRef] [PubMed]
- Geyer, F.C.; Pareja, F.; Weigelt, B.; Rakha, E.; Ellis, I.O.; Schnitt, S.J.; Reis-Filho, J.S. The Spectrum of Triple-Negative Breast Disease: High- and Low-Grade Lesions. Am. J. Pathol. 2017, 187, 2139–2151. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Duan, J.J.; Bian, X.W. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Res. 2020, 22, 61. [Google Scholar] [CrossRef] [PubMed]
- Kummel, A.; Kummel, S.; Barinoff, J.; Heitz, F.; Holtschmidt, J.; Weikel, W.; Lorenz-Salehi, F.; du Bois, A.; Harter, P.; Traut, A.; et al. Prognostic Factors for Local, Loco-regional and Systemic Recurrence in Early-stage Breast Cancer. Geburtshilfe Frauenheilkd. 2015, 75, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Tzikas, A.K.; Nemes, S.; Linderholm, B.K. A comparison between young and old patients with triple-negative breast cancer: Biology, survival and metastatic patterns. Breast Cancer Res. Treat. 2020, 182, 643–654. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; Andre, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef] [PubMed]
- Hallett, R.M.; Dvorkin-Gheva, A.; Bane, A.; Hassell, J.A. A gene signature for predicting outcome in patients with basal-like breast cancer. Sci. Rep. 2012, 2, 227. [Google Scholar] [CrossRef] [PubMed]
- O’Halloran, N.; Lowery, A.; Curran, C.; McLaughlin, R.; Malone, C.; Sweeney, K.; Keane, M.; Kerin, M. A Review of the Impact of Neoadjuvant Chemotherapy on Breast Surgery Practice and Outcomes. Clin. Breast Cancer 2019, 19, 377–382. [Google Scholar] [CrossRef]
- Golshan, M.; Cirrincione, C.T.; Sikov, W.M.; Berry, D.A.; Jasinski, S.; Weisberg, T.F.; Somlo, G.; Hudis, C.; Winer, E.; Ollila, D.W.; et al. Impact of neoadjuvant chemotherapy in stage II-III triple negative breast cancer on eligibility for breast-conserving surgery and breast conservation rates: Surgical results from CALGB 40603 (Alliance). Ann. Surg. 2015, 262, 434–439; discussion 438–439. [Google Scholar] [CrossRef]
- Marra, A.; Curigliano, G. Adjuvant and Neoadjuvant Treatment of Triple-Negative Breast Cancer with Chemotherapy. Cancer J. 2021, 27, 41–49. [Google Scholar] [CrossRef]
- Chaudhary, L.N. Early stage triple negative breast cancer: Management and future directions. Semin. Oncol. 2020, 47, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative, G. Increasing the dose intensity of chemotherapy by more frequent administration or sequential scheduling: A patient-level meta-analysis of 37 298 women with early breast cancer in 26 randomised trials. Lancet 2019, 393, 1440–1452. [Google Scholar] [CrossRef]
- Deng, H.; Wang, L.; Wang, N.; Zhang, K.; Zhao, Y.; Qiu, P.; Qi, X.; Zhang, D.; Xu, F.; Liu, J. Neoadjuvant checkpoint blockade in combination with Chemotherapy in patients with tripe-negative breast cancer: Exploratory analysis of real-world, multicenter data. BMC Cancer 2023, 23, 29. [Google Scholar] [CrossRef]
- Polish National Cancer Registry. Available online: https://onkologia.org.pl/en/report (accessed on 7 December 2023).
- Hammond, M.E.; Hayes, D.F.; Wolff, A.C.; Mangu, P.B.; Temin, S. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J. Oncol. Pract. 2010, 6, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; Hammond, M.E.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; Ballman, K.V.; McCall, L.; Beitsch, P.D.; Brennan, M.B.; Kelemen, P.R.; Ollila, D.W.; Hansen, N.M.; Whitworth, P.W.; Blumencranz, P.W.; et al. Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA 2017, 318, 918–926. [Google Scholar] [CrossRef] [PubMed]
- Donker, M.; van Tienhoven, G.; Straver, M.E.; Meijnen, P.; van de Velde, C.J.; Mansel, R.E.; Cataliotti, L.; Westenberg, A.H.; Klinkenbijl, J.H.; Orzalesi, L.; et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): A randomised, multicentre, open-label, phase 3 non-inferiority trial. Lancet Oncol. 2014, 15, 1303–1310. [Google Scholar] [CrossRef]
- Boughey, J.C.; Suman, V.J.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Leitch, A.M.; Kuerer, H.M.; Bowling, M.; Flippo-Morton, T.S.; et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: The ACOSOG Z1071 (Alliance) clinical trial. JAMA 2013, 310, 1455–1461. [Google Scholar] [CrossRef]
- Howard, F.M.; Olopade, O.I. Epidemiology of Triple-Negative Breast Cancer: A Review. Cancer J. 2021, 27, 8–16. [Google Scholar] [CrossRef]
- Li, X.; Yang, J.; Peng, L.; Sahin, A.A.; Huo, L.; Ward, K.C.; O’Regan, R.; Torres, M.A.; Meisel, J.L. Triple-negative breast cancer has worse overall survival and cause-specific survival than non-triple-negative breast cancer. Breast Cancer Res. Treat. 2017, 161, 279–287. [Google Scholar] [CrossRef]
- Sharma, P. Biology and Management of Patients with Triple-Negative Breast Cancer. Oncologist 2016, 21, 1050–1062. [Google Scholar] [CrossRef]
- Tariq, K.; Farhangi, A.; Rana, F. TNBC vs non-TNBC: A retrospective review of differences in mean age, family history, smoking history, and stage at diagnosis. Clin. Adv. Hematol. Oncol. 2014, 12, 377–381. [Google Scholar]
- Vihervuori, H.; Korpinen, K.; Autere, T.A.; Repo, H.; Talvinen, K.; Kronqvist, P. Varying outcomes of triple-negative breast cancer in different age groups-prognostic value of clinical features and proliferation. Breast Cancer Res. Treat. 2022, 196, 471–482. [Google Scholar] [CrossRef]
- Schilling, J.; Busch, S.; Heinrich, G.; Heinig, K.; Martin Kurbacher, C.; Klare, P.; Pollinger, B. Treatment patterns, health care resource use and outcomes in metastatic triple-negative breast cancer in Germany: Retrospective chart review study (OBTAIN). Curr. Med. Res. Opin. 2019, 35, 1405–1414. [Google Scholar] [CrossRef]
- Engel, C.; Rhiem, K.; Hahnen, E.; Loibl, S.; Weber, K.E.; Seiler, S.; Zachariae, S.; Hauke, J.; Wappenschmidt, B.; Waha, A.; et al. Prevalence of pathogenic BRCA1/2 germline mutations among 802 women with unilateral triple-negative breast cancer without family cancer history. BMC Cancer 2018, 18, 265. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.; Knapp, G.; Quan, M.L.; Bouchard-Fortier, A. Cancer-Specific Outcomes in the Elderly with Triple-Negative Breast Cancer: A Systematic Review. Curr. Oncol. 2021, 28, 2337–2345. [Google Scholar] [CrossRef] [PubMed]
- Harborg, S.; Zachariae, R.; Olsen, J.; Johannsen, M.; Cronin-Fenton, D.; Boggild, H.; Borgquist, S. Overweight and prognosis in triple-negative breast cancer patients: A systematic review and meta-analysis. NPJ Breast Cancer 2021, 7, 119. [Google Scholar] [CrossRef]
- Sun, H.; Zou, J.; Chen, L.; Zu, X.; Wen, G.; Zhong, J. Triple-negative breast cancer and its association with obesity. Mol. Clin. Oncol. 2017, 7, 935–942. [Google Scholar] [CrossRef]
- Parise, C.A.; Caggiano, V. The influence of comorbidity on treatment and survival of triple-negative breast cancer. Breast J. 2020, 26, 1729–1735. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Wu, J.; Zhang, Z.; Tang, Y.; Li, X.; Liu, S.; Cao, S.; Li, X. Association Between BRCA Status and Triple-Negative Breast Cancer: A Meta-Analysis. Front. Pharmacol. 2018, 9, 909. [Google Scholar] [CrossRef]
- Sporikova, Z.; Koudelakova, V.; Trojanec, R.; Hajduch, M. Genetic Markers in Triple-Negative Breast Cancer. Clin. Breast Cancer 2018, 18, e841–e850. [Google Scholar] [CrossRef]
- Pavese, F.; Capoluongo, E.D.; Muratore, M.; Minucci, A.; Santonocito, C.; Fuso, P.; Concolino, P.; Di Stasio, E.; Carbognin, L.; Tiberi, G.; et al. BRCA Mutation Status in Triple-Negative Breast Cancer Patients Treated with Neoadjuvant Chemotherapy: A Pivotal Role for Treatment Decision-Making. Cancers 2022, 14, 4571. [Google Scholar] [CrossRef]
- Caramelo, O.; Silva, C.; Caramelo, F.; Frutuoso, C.; Pinto, L.; Almeida-Santos, T. Efficacy of different neoadjuvant treatment regimens in BRCA-mutated triple negative breast cancer: A systematic review and meta-analysis. Hered. Cancer Clin. Pract. 2022, 20, 34. [Google Scholar] [CrossRef]
- Ye, F.; He, M.; Huang, L.; Lang, G.; Hu, X.; Shao, Z.; Di, G.; Cao, A. Insights Into the Impacts of BRCA Mutations on Clinicopathology and Management of Early-Onset Triple-Negative Breast Cancer. Front. Oncol. 2020, 10, 574813. [Google Scholar] [CrossRef]
- Ain, Q.; Richardson, C.; Mutebi, M.; George, A.; Kemp, Z.; Rusby, J.E. Does mainstream BRCA testing affect surgical decision-making in newly-diagnosed breast cancer patients? Breast 2023, 67, 30–35. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group. Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: Meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018, 19, 27–39. [Google Scholar] [CrossRef]
- Masuda, N.; Lee, S.J.; Ohtani, S.; Im, Y.H.; Lee, E.S.; Yokota, I.; Kuroi, K.; Im, S.A.; Park, B.W.; Kim, S.B.; et al. Adjuvant Capecitabine for Breast Cancer after Preoperative Chemotherapy. N. Engl. J. Med. 2017, 376, 2147–2159. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Ding, K.; Yang, H.; He, X.; Mo, W.; Ding, X. Does dose-dense neoadjuvant chemotherapy have clinically significant prognostic value in breast cancer?: A meta-analysis of 3724 patients. PLoS ONE 2020, 15, e0234058. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; O’Shaughnessy, J.; Zhao, J.; Haiderali, A.; Cortes, J.; Ramsey, S.D.; Briggs, A.; Hu, P.; Karantza, V.; Aktan, G.; et al. Association of Pathologic Complete Response with Long-Term Survival Outcomes in Triple-Negative Breast Cancer: A Meta-Analysis. Cancer Res. 2020, 80, 5427–5434. [Google Scholar] [CrossRef] [PubMed]
- Headon, H.L.; Kasem, A.; Mokbel, K. The Oncological Safety of Nipple-Sparing Mastectomy: A Systematic Review of the Literature with a Pooled Analysis of 12,358 Procedures. Arch. Plast. Surg. 2016, 43, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Verreck, E.E.F.; van Steenhoven, J.E.C.; Kuijer, A.; van Maaren, M.C.; Simons, J.M.; Siesling, S.; van Dalen, T. Trends of Axillary Treatment in Sentinel Node-Positive Breast Cancer Patients Undergoing Mastectomy. Ann. Surg. Oncol. 2023, 30, 5623–5632. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | % | ||
|---|---|---|---|
| Age group at diagnosis (years) | <50 | 205 | 37.4% |
| 50–69 | 244 | 44.4% | |
| 70+ | 100 | 18.2% | |
| Sex | Female | 548 | 99.8% |
| Male | 1 | 0.2% | |
| Year of diagnosis | 2015 | 68 | 12.4% |
| 2016 | 91 | 16.6% | |
| 2017 | 94 | 17.1% | |
| 2018 | 96 | 17.5% | |
| 2019 | 103 | 18.8% | |
| 2020 | 97 | 17.6% | |
| ECOG at diagnosis | 0 | 491 | 89.5% |
| 1 | 48 | 8.7% | |
| 2+ | 9 | 1.6% | |
| Undocumented | 1 | 0.2% | |
| BMI at diagnosis | <18.5 | 6 | 1.1% |
| 18.5–24.9 | 235 | 42.8% | |
| 25–29.9 | 114 | 20.8% | |
| ≥30 | 66 | 12.0% | |
| Undocumented | 128 | 23.3% | |
| BRCA1/2 status | Negative | 164 | 29.9% |
| Positive | 109 | 19.9% | |
| Undocumented | 276 | 50.2% | |
| BRCA1/2 status among aged <50 (N = 205) | Negative | 80 | 39.0% |
| Positive | 81 | 39.5% | |
| Undocumented | 44 | 21.5% | |
| BRCA1/2 status among aged 50+ (N = 344) | Negative | 84 | 24.4% |
| Positive | 28 | 8.1% | |
| Undocumented | 232 | 67.5% | |
| Menopause status at diagnosis | Premenopausal | 96 | 17.5% |
| Postmenopausal | 319 | 58.1% | |
| Undocumented | 134 | 24.4% | |
| Any coexisting condition * | No | 166 | 30.2% |
| Yes | 325 | 59.2% | |
| Undocumented | 58 | 10.6% | |
| Histological type | Invasive carcinoma of no special type (NOS) | 466 | 84.9% |
| Lobular | 7 | 1.3% | |
| Metaplastic | 29 | 5.3% | |
| Other | 6 | 1.1% | |
| Undocumented | 41 | 7.4% | |
| Grade | G1 | 15 | 2.7% |
| G2 | 155 | 28.2% | |
| G3 | 309 | 56.3% | |
| Undocumented | 70 | 12.8% | |
| Stage | I | 94 | 17.1% |
| IIA | 198 | 36.1% | |
| IIB | 128 | 23.3% | |
| IIIA | 79 | 14.4% | |
| IIIB | 50 | 9.1% |
| Initial Tumour Stage | The Mode of Systemic Treatment | Use of Post-Neoadjuvant Among Patients Treated with Neoadjuvant | ||||
|---|---|---|---|---|---|---|
| N | Neoadjuvant | Adjuvant Only | Other * | No Post-Neoadjuvant Used | Post-Neoadjuvant Used | |
| Stage I | 94 | 21 (22.3%) | 52 (55.4%) | 21 (22.3%) | 17 (81.0%) | 4 (19.0%) |
| Stage IIA | 198 | 134 (67.7%) | 38 (19.2%) | 26 (13.1%) | 102 (76.1%) | 32 (23.9%) |
| Stage IIB | 128 | 105 (82.0%) | 10 (7.8%) | 13 (10.2%) | 79 (75.2%) | 26 (24.8%) |
| State IIIA | 79 | 76 (96.2%) | 0 (0.0%) | 3 (3.8%) | 56 (73.7%) | 20 (26.3%) |
| Stage IIIB | 50 | 40 (80.0%) | 1 (2.0%) | 9 (18.0%) | 35 (87.5%) | 5 (12.5%) |
| Total | 549 | 376 (68.5%) | 101 (18.4%) | 72 (13.1%) | 289 (76.9%) | 87 (23.1%) |
| Treatment Modality | Regimen | N | % |
|---|---|---|---|
| Patient receiving neoadjuvant therapy (N = 376) | |||
| Neoadjuvant regimen | Doxorubicin, cyclophosphamide -> paclitaxel | 105 | 27.90% |
| dd Doxorubicin, cyclophosphamide -> paclitaxel, carboplatin | 91 | 24.20% | |
| dd Doxorubicin, cyclophosphamide -> paclitaxel | 77 | 20.50% | |
| Doxorubicin, cyclophosphamide -> paclitaxel, carboplatin | 31 | 8.20% | |
| Paclitaxel | 30 | 8.00% | |
| Paclitaxel, carboplatin | 11 | 2.90% | |
| Doxorubicin, cyclophosphamide | 8 | 2.10% | |
| Docetaxel, doxorubicin | 7 | 1.90% | |
| Docetaxel, cyclophosphamide | 4 | 1.10% | |
| Docetaxel, doxorubicin, cyclophosphamide | 2 | 0.50% | |
| Other | 10 | 2.70% | |
| Patient receiving neo- and post-neoadjuvant therapy (N = 87), subgroup of the Patient receiving neoadjuvant therapy group | |||
| Post-neoadjuvant regimen | Capecitabine | 75 | 86.20% |
| Other | 12 | 13.80% | |
| Patient receiving only adjuvant therapy (N = 101) | |||
| Adjuvant regimen | Doxorubicin, cyclophosphamide -> paclitaxel | 55 | 54.50% |
| Paclitaxel | 11 | 10.90% | |
| dd Doxorubicin, cyclophosphamide -> paclitaxel | 11 | 10.90% | |
| Paclitaxel, carboplatin | 5 | 4.90% | |
| Doxorubicin, cyclophosphamide | 5 | 4.90% | |
| Docetaxel, cyclophosphamide | 4 | 4.00% | |
| Doxorubicin, cyclophosphamide -> paclitaxel, carboplatin | 2 | 2.00% | |
| dd Doxorubicin, cyclophosphamide -> paclitaxel, carboplatin | 1 | 1.00% | |
| Capecitabine | 1 | 1.00% | |
| (Randomised clinical trial) | 1 | 1.00% | |
| Other | 5 | 4.90% | |
| Number of Patients (Number of Patients with Conserving Surgery) | Percent of Conserving (95%CI) | OR * (95% CI) | Univariate p-Value | aOR * (95% CI) | Multivariate p-Value | ||
|---|---|---|---|---|---|---|---|
| Neoadjuvant use | No | 160 (85) | 53.1% (45.4%–60.7%) | Ref. | Ref. | ||
| Yes | 343 (138) | 40.2% (35.2%–45.5%) | 0.59 (0.41–0.87) | 0.0069 | 1.93 (1.07–3.5) | 0.0293 | |
| Year of diagnosis | Per year | - | - | 1.03 (0.92–1.14) | 0.6398 | 0.94 (0.82–1.08) | 0.3673 |
| Stage at diagnosis | I | 93 (70) | 75.3% (65.6%–82.9%) | Ref. | Ref. | ||
| IIA | 179 (98) | 54.8% (47.4%–61.9%) | 0.4 (0.22–0.68) | 0.0011 | 0.27 (0.14–0.51) | 0.0001 | |
| IIB | 121 (46) | 38.0% (29.9%–46.9%) | 0.2 (0.11–0.36) | <0.0001 | 0.12 (0.05–0.24) | <0.0001 | |
| III | 110 (9) | 8.2% (4.4%–14.8%) | 0.03 (0.01–0.06) | <0.0001 | 0.01 (0.00–0.04) | <0.0001 | |
| Age group | <50 | 180 (77) | 42.8% (35.8%–50.1%) | Ref. | Ref. | ||
| 50–69 | 228 (119) | 52.2% (45.7%–58.6%) | 1.46 (0.99–2.17) | 0.0592 | 1.02 (0.62–1.68) | 0.9326 | |
| 70+ | 95 (27) | 28.4% (20.3%–38.2%) | 0.53 (0.31–0.9) | 0.0204 | 0.45 (0.22–0.91) | 0.0279 | |
| BRCA | Negative | 159 (88) | 55.4% (47.6%–62.9%) | Ref. | Ref. | ||
| Positive | 89 (28) | 31.5% (22.8%–41.7%) | 0.37 (0.21–0.63) | <0.0001 | 0.22 (0.12–0.42) | <0.0001 | |
| N/D ** | 255 (107) | 42.0% (36.1%–48.1%) | 0.58 (0.39–0.87) | 0.0082 | 0.62 (0.36–1.05) | 0.078 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosińska, M.; Dubiański, R.; Konieczna, A.; Poleszczuk, J.; Pawlik, H.; Nowecki, Z.I.; Kamiński, E. Retrospective Observational Study to Determine the Epidemiology and Treatment Patterns of Patients with Triple-Negative Breast Cancer. Cancers 2024, 16, 1087. https://doi.org/10.3390/cancers16061087
Rosińska M, Dubiański R, Konieczna A, Poleszczuk J, Pawlik H, Nowecki ZI, Kamiński E. Retrospective Observational Study to Determine the Epidemiology and Treatment Patterns of Patients with Triple-Negative Breast Cancer. Cancers. 2024; 16(6):1087. https://doi.org/10.3390/cancers16061087
Chicago/Turabian StyleRosińska, Magdalena, Roman Dubiański, Aleksandra Konieczna, Jan Poleszczuk, Hubert Pawlik, Zbigniew I. Nowecki, and Eryk Kamiński. 2024. "Retrospective Observational Study to Determine the Epidemiology and Treatment Patterns of Patients with Triple-Negative Breast Cancer" Cancers 16, no. 6: 1087. https://doi.org/10.3390/cancers16061087
APA StyleRosińska, M., Dubiański, R., Konieczna, A., Poleszczuk, J., Pawlik, H., Nowecki, Z. I., & Kamiński, E. (2024). Retrospective Observational Study to Determine the Epidemiology and Treatment Patterns of Patients with Triple-Negative Breast Cancer. Cancers, 16(6), 1087. https://doi.org/10.3390/cancers16061087