
Physiotherapy Interventions in Lung Cancer Patients: A Systematic Review

 ,
, 
Simple Summary
Abstract
1. Introduction
- (1)
- To highlight the effects of physiotherapy in improving dyspnea, pain, and fatigue in lung cancer patients.
- (2)
- To describe which interventions are performed the most in lung cancer patients.
2. Materials and Methods
2.1. Study Design
2.2. Information Sources
2.3. Search Strategy
2.4. Inclusion Criteria
2.5. Exclusion Criteria
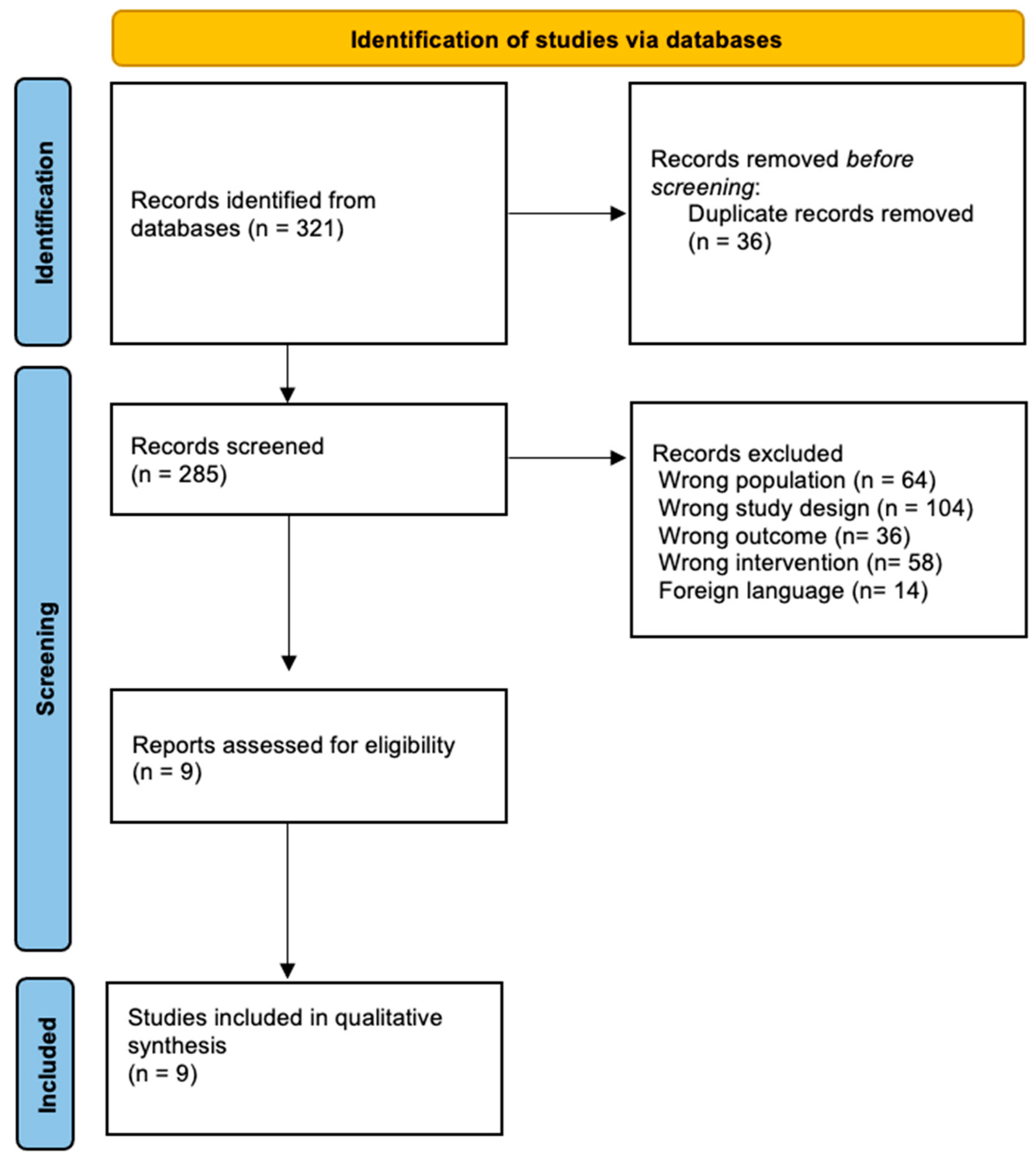
2.6. Selection Process
2.7. Data Extraction
2.8. Risk of Bias
3. Results
3.1. Descriptive Study
3.2. Participants’ Characteristics
3.3. Interventions
3.3.1. Experimental Group
3.3.2. Control Group
3.4. Studied Outcomes
3.5. Effects of the Interventions
3.6. Risk of Bias
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bade, B.C.; Dela Cruz, C.S. Lung Cancer 2020: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Chansky, K.; Detterbeck, F.C.; Nicholson, A.G.; Rusch, V.W.; Vallières, E.; Groome, P.; Kennedy, C.; Krasnik, M.; Peake, M.; Shemanski, L.; et al. The IASLC Lung Cancer Staging Project: External Validation of the Revision of the TNM Stage Groupings in the Eighth Edition of the TNM Classification of Lung Cancer. J. Thorac. Oncol. 2017, 12, 1109–1121. [Google Scholar] [CrossRef] [PubMed]
- Menéndez, P.; Sánchez-Torres, J.M.; Bartolomé, A.; Bravo, J.L.; Caballero-Guerra, P.; Calzas-Rodríguez, J.; Cortés-Funes, H.; Díaz-Hellín, V.; Doñado-Uña, J.R.; Enguita, A.B.; et al. OncoSur Guía Clínica de Diagnóstico y Tratamiento Del Cáncer de Pulmón; Grupo de trabajo oncológico de centros hospitalarios del sur de Madrid: Madrid, Spain, 2009. [Google Scholar]
- Pirker, R. Chemotherapy Remains a Cornerstone in the Treatment of Nonsmall Cell Lung Cancer. Curr. Opin. Oncol. 2020, 32, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Vinod, S.K.; Hau, E. Radiotherapy Treatment for Lung Cancer: Current Status and Future Directions. Respirology 2020, 25, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Hanna, N.H.; Robinson, A.G.; Temin, S.; Baker, S.; Brahmer, J.R.; Ellis, P.M.; Gaspar, L.E.; Haddad, R.Y.; Hesketh, P.J.; Jain, D.; et al. Therapy for Stage IV Non-Small-Cell Lung Cancer with Driver Alterations: ASCO and OH (CCO) Joint Guideline Update. J. Clin. Oncol. 2021, 39, 1040–1091. [Google Scholar] [CrossRef] [PubMed]
- Molassiotis, A.; Yates, P.; Yorke, J. Editorial: Quality of Life and Side Effects Management in Lung Cancer Treatment. Front. Oncol. 2021, 11, 651797. [Google Scholar] [CrossRef]
- Cjl, M.; Rooijen, V.S.; Hjp, F.; Rmh, R.; Janssen, L.; Slooter, G.D. Cochrane Library Cochrane Database of Systematic Reviews Prehabilitation versus No Prehabilitation to Improve Functional Capacity, Reduce Postoperative Complications and Improve Quality of Life in Colorectal Cancer Surgery. Emergencias 2022, 2022, CD013259. [Google Scholar] [CrossRef]
- Medeiros Torres, D.; Koifman, R.J.; da Silva Santos, S. Impact on Fatigue of Different Types of Physical Exercise during Adjuvant Chemotherapy and Radiotherapy in Breast Cancer: Systematic Review and Meta-Analysis. Support. Care Cancer 2022, 30, 4651–4662. [Google Scholar] [CrossRef]
- Smith, S.R.; Zheng, J.Y.; Silver, J.; Haig, A.J.; Cheville, A. Cancer Rehabilitation as an Essential Component of Quality Care and Survivorship from an International Perspective. Disabil. Rehabil. 2020, 42, 8–13. [Google Scholar] [CrossRef]
- Stout, N.L.; Santa Mina, D.; Lyons, K.D.; Robb, K.; Silver, J.K. A Systematic Review of Rehabilitation and Exercise Recommendations in Oncology Guidelines. CA. Cancer J. Clin. 2021, 71, 149–175. [Google Scholar] [CrossRef] [PubMed]
- Shallwani, S.M.; King, J.; Thomas, R.; Thevenot, O.; De Angelis, G.; Aburub, A.S.; Brosseau, L. Methodological Quality of Clinical Practice Guidelines with Physical Activity Recommendations for People Diagnosed with Cancer: A Systematic Critical Appraisal Using the AGREE II Tool. PLoS ONE 2019, 14, e0214846. [Google Scholar] [CrossRef] [PubMed]
- Driessen, E.J.; Peeters, M.E.; Bongers, B.C.; Maas, H.A.; Bootsma, G.P.; Van Meeteren, N.L.; Janssen-Heijnen, M.L. Effects of Prehabilitation and Rehabilitation Including a Home-Based Component on Physical Fitness, Adherence, Treatment Tolerance, and Recovery in Patients with Non-Small Cell Lung Cancer: A Systematic Review. Crit. Rev. Oncol. Hematol. 2017, 114, 63–76. [Google Scholar] [CrossRef] [PubMed]
- Codima, A.; das Neves Silva, W.; de Souza Borges, A.P.; de Castro, G. Exercise Prescription for Symptoms and Quality of Life Improvements in Lung Cancer Patients: A Systematic Review. Support. Care Cancer 2021, 29, 445–457. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Q.; Liu, X.; Yin, Y.Y.; Ma, R.C.; Yang, Z.; Cao, H.P.; Xie, J. Effects of Home-Based Exercise Training for Patients With Lung Cancer. Oncol. Nurs. Forum 2019, 46, E119–E134. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Jonsson, M.; Ahlsson, A.; Hurtig-Wennlöf, A.; Vidlund, M.; Cao, Y.; Westerdahl, E. In-Hospital Physiotherapy and Physical Recovery 3 Months After Lung Cancer Surgery: A Randomized Controlled Trial. Integr. Cancer Ther. 2019, 18, 1534735419876346. [Google Scholar] [CrossRef]
- Jonsson, M.; Hurtig-Wennlöf, A.; Ahlsson, A.; Vidlund, M.; Cao, Y.; Westerdahl, E. In-Hospital Physiotherapy Improves Physical Activity Level after Lung Cancer Surgery: A Randomized Controlled Trial. Physiother 2019, 105, 434–441. [Google Scholar] [CrossRef]
- Liu, Z.; Qiu, T.; Pei, L.; Zhang, Y.; Xu, L.; Cui, Y.; Liang, N.; Li, S.; Chen, W.; Huang, Y. Two-Week Multimodal Prehabilitation Program Improves Perioperative Functional Capability in Patients Undergoing Thoracoscopic Lobectomy for Lung Cancer: A Randomized Controlled Trial. Anesth. Analg. 2020, 131, 840–849. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.B.; Liu, X.; Wang, Y.Q.; Cao, H.P.; Ma, R.C.; Yin, Y.Y.; Song, C.Y.; Yang, T.T.; Xie, J. Active Cycle of Breathing Technique: A Respiratory Modality to Improve Perioperative Outcomes in Patients With Lung Cancer. Clin. J. Oncol. Nurs. 2022, 26, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Edbrooke, L.; Aranda, S.; Granger, C.L.; Mcdonald, C.F.; Krishnasamy, M.; Mileshkin, L.; Clark, R.A.; Gordon, I.; Irving, L.; Denehy, L. Multidisciplinary Home-Based Rehabilitation in Inoperable Lung Cancer: A Randomised Controlled Trial. Thorax 2019, 74, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Gravier, F.E.; Smondack, P.; Boujibar, F.; Prieur, G.; Medrinal, C.; Combret, Y.; Muir, J.F.; Baste, J.M.; Cuvelier, A.; Debeaumont, D.; et al. Prehabilitation Sessions Can Be Provided More Frequently in a Shortened Regimen with Similar or Better Efficacy in People with Non-Small Cell Lung Cancer: A Randomised Trial. J. Physiother. 2022, 68, 43–50. [Google Scholar] [CrossRef]
- Rutkowska, A.; Jastrzebski, D.; Rutkowski, S.; Zebrowska, A.; Stanula, A.; Szczegielniak, J.; Ziora, D.; Casaburi, R. Exercise Training in Patients With Non-Small Cell Lung Cancer During In-Hospital Chemotherapy Treatment: A Randomized Controlled Trial. J. Cardiopulm. Rehabil. Prev. 2019, 39, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Blanco, R.; Rincón-García, D.; Valero-Alcaide, R.; Atín-Arratibel, M.A.; De Miguel-Diez, J.; Corrochano-Cardona, R.; Torres-Castro, R.; Moro-Tejedor, M.N. Preoperative Respiratory Therapy in Patients Undergoing Surgery for Lung Cancer: A Randomized Controlled Trial. Physiother. Res. Int. 2023, 28, e1973. [Google Scholar] [CrossRef]
- Liu, J.F.; Kuo, N.Y.; Fang, T.P.; Chen, J.O.; Lu, H.I.; Lin, H.L. A Six-Week Inspiratory Muscle Training and Aerobic Exercise Improves Respiratory Muscle Strength and Exercise Capacity in Lung Cancer Patients after Video-Assisted Thoracoscopic Surgery: A Randomized Controlled Trial. Clin. Rehabil. 2021, 35, 840–850. [Google Scholar] [CrossRef]
- Schmidt, K.; Vogt, L.; Thiel, C.; Jäger, E.; Banzer, W. Validity of the Six-Minute Walk Test in Cancer Patients. Int. J. Sports Med. 2013, 34, 631–636. [Google Scholar] [CrossRef]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An Official European Respiratory Society/American Thoracic Society Technical Standard: Field Walking Tests in Chronic Respiratory Disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Zhao, N.; Wu, F.; Peng, J.; Zheng, Y.; Tian, H.; Yang, H.; Deng, Z.; Wang, Z.; Li, H.; Wen, X.; et al. Preserved Ratio Impaired Spirometry Is Associated with Small Airway Dysfunction and Reduced Total Lung Capacity. Respir. Res. 2022, 23, 298. [Google Scholar] [CrossRef]
- Rivero-Yeverino, D. Spirometry: Basic Concepts. Rev. Alerg. Mex. 2019, 66, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Sunjaya, A.; Poulos, L.; Reddel, H.; Jenkins, C. Qualitative Validation of the Modified Medical Research Council (MMRC) Dyspnoea Scale as a Patient-Reported Measure of Breathlessness Severity. Respir. Med. 2022, 203, 106984. [Google Scholar] [CrossRef] [PubMed]
- D’silva, A.; Gardiner, P.A.; Boyle, T.; Bebb, D.G.; Johnson, S.T.; Vallance, J.K. Associations of Objectively Assessed Physical Activity and Sedentary Time with Health-Related Quality of Life among Lung Cancer Survivors: A Quantile Regression Approach. Lung Cancer 2018, 119, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Dowman, L.; Hill, C.J.; May, A.; Holland, A.E. Pulmonary Rehabilitation for Interstitial Lung Disease. Cochrane Database Syst. Rev. 2021, 2021, CD006322. [Google Scholar] [CrossRef] [PubMed]
- Reis, A.D.; Pereira, P.T.V.T.; Diniz, R.R.; de Castro Filha, J.G.L.; dos Santos, A.M.; Ramallo, B.T.; Filho, F.A.A.; Navarro, F.; Garcia, J.B.S. Effect of Exercise on Pain and Functional Capacity in Breast Cancer Patients. Health Qual. Life Outcomes 2018, 16, 58. [Google Scholar] [CrossRef] [PubMed]
- Samuel, S.R.; Maiya, A.G.; Fernandes, D.J.; Guddattu, V.; Saxena, P.P.; Kurian, J.R.; Lin, P.-J.; Mustian, K.M. Effectiveness of Exercise-Based Rehabilitation on Functional Capacity and Quality of Life in Head and Neck Cancer Patients Receiving Chemo-Radiotherapy. Support. Care Cancer 2019, 27, 3913. [Google Scholar] [CrossRef] [PubMed]
- Sancho, A.; Carrera, S.; Arietaleanizbeascoa, M.; Arce, V.; Gallastegui, M.M.; March, A.G.; Sanz-Guinea, A.; Eskisabel, A.; Rodriguez, L.L.; Martín, R.A.; et al. Supervised Physical Exercise to Improve the Quality of Life of Cancer Patients: The Eficancer Randomised Controlled Trial. BMC Cancer 2015, 15, 40. [Google Scholar] [CrossRef] [PubMed]
- Mendizabal-Gallastegui, N.; Arietaleanizbeaskoa, M.S.; Latorre, P.M.; García-Álvarez, A.; Sancho, A.; Iruarrizaga, E.; López-Vivanco, G.; Grandes, G. Nurse-Supervised Exercise for People with Stage IV Cancer: The EFICANCER Randomized Clinical Trial. Semin. Oncol. Nurs. 2023, 39, 151448. [Google Scholar] [CrossRef]
- Rodrigues, A.; Castro, G.M.; Jácome, C.; Langer, D.; Parry, S.M.; Burtin, C. Current Developments and Future Directions in Respiratory Physiotherapy. Eur. Respir. Rev. 2020, 29, 200264. [Google Scholar] [CrossRef]
- Messaggi-Sartor, M.; Marco, E.; Martínez-Téllez, E.; Rodriguez-Fuster, A.; Palomares, C.; Chiarella, S.; Muniesa, J.M.; Orozco-Levi, M.; Barreiro, E.; Güell, M.R. Combined Aerobic Exercise and High-Intensity Respiratory Muscle Training in Patients Surgically Treated for Non-Small Cell Lung Cancer: A Pilot Randomized Clinical Trial. Eur. J. Phys. Rehabil. Med. 2019, 55, 113–122. [Google Scholar] [CrossRef]
- Shin, J.A.; Kosiba, J.D.; Traeger, L.; Greer, J.A.; Temel, J.S.; Pirl, W.F. Dyspnea and Panic Among Patients With Newly Diagnosed Non-Small Cell Lung Cancer. J. Pain Symptom Manage. 2014, 48, 465. [Google Scholar] [CrossRef]
- Gül, Ş.K.; Tepetam, H.; Gül, H.L. Duloxetine and Pregabalin in Neuropathic Pain of Lung Cancer Patients. Brain Behav. 2020, 10, e01527. [Google Scholar] [CrossRef]
- Matsuoka, H.; Iwase, S.; Miyaji, T.; Kawaguchi, T.; Ariyoshi, K.; Oyamada, S.; Satomi, E.; Ishiki, H.; Hasuo, H.; Sakuma, H.; et al. Additive Duloxetine for Cancer-Related Neuropathic Pain Nonresponsive or Intolerant to Opioid-Pregabalin Therapy: A Randomized Controlled Trial (JORTC-PAL08). J. Pain Symptom Manag. 2019, 58, 645–653. [Google Scholar] [CrossRef]


{kind=link}
| Database | Search Strategy |
|---|---|
| SCOPUS | ((“lung cancer” OR “carcinoma non small-cell lung” OR “carcinoma small-cell lung”) AND (“physiotherapy”)) |
| PUBMED | (((“lung cancer”) OR (“carcinoma non small-cell lung”)) OR (“carcinoma small-cell lung”)) AND (physiotherapy) |
| WEB OF SCIENCE | lung cancer (All Fields) OR carcinoma small-cell lung (All Fields) OR carcinoma non small-cell lung (All Fields) AND physiotherapy (All Fields) |
| COCHRANE | (lung cancer):ti,ab,kw OR (carcinoma small-cell lung):ti,ab,kw OR (carcinoma non small-cell lung):ti,ab,kw AND (physiotherapy):ti,ab,kw |
| PEDRO | [(lung cancer) OR (carcinoma small-cell lung) OR (carcinoma non small-cell lung)] AND [(physiotherapy)] |
| Author (Year) | Sample Size | Gender (Age, Years ± SD) | Cancer Type (Stage) | Medical Treatment |
|---|---|---|---|---|
| Edbrooke et al. (2019) [24] | 92 | Male: 55.4% Female: 45.6% (CG: 62.5 ± 10.9 EG: 64.6 ± 13.4) | LC | CT and/or RT |
| Gravier et al. (2022) [25] | 36 | Male: 64% Female: 36% 65–68 ± 8 | NSCLC | Neoadjuvant RCT |
| Fernández-Blanco et al. (2022) [27] | 71 | Male: 61.97% Female: 38.03% (CG: 61.1 ± 11.9; EG: 64.1 ± 15.4) | LC | Surgery |
| Jonsson et al. (2019) [21] | 94 | Male: 47.9% Female: 52.1% (CG: 68 ± 8; EG: 69 ± 8) | NSCLC | Surgery |
| Jonsson et al. (2019) [20] | 107 | Male: 43.9% Female: 56.1% (CG: 68.4 ± 8.3; EG: 68.7 ± 7.4) | LC | Surgery |
| Liu et al. (2020) [28] | 54 | Male: 40.74% Female: 59.26% (CG: 66.3 ± 7.9; EG: 64.2 ± 5.9) | LC (IA-IIIA stages) | Surgery |
| Liu Z et al. (2020) [22] | 73 | Male: 31.5% Female: 68.5% (CG: 56.2 ± 8.7; EG:56.2 ± 10.3) | LC | Surgery |
| Lu et al. (2022) [23] | 68 | Male: 41.18% Female: 58.82% (CG: 57.03 ± 12.34; EG: 62.12 ± 8.03) | LC | Surgery |
| Rutkowska et al. (2019) [26] | 40 | Male: 100% (CG: 59.1 ± 6.8; EG: 61.3 ± 8.8) | NSCLC (IIIB-IV stages) | CT |
| Author (Year) | Sample Size | Control Group | Experimental Group | Duration | Outcomes | Results |
|---|---|---|---|---|---|---|
| Edbrooke et al. (2019) [24] | 92 | Usual care | Monitored home-based rehabilitation:
| 2–3 sessions a week during 8 weeks | FC (6MWT) QoL (HrQol) Symptoms (MDADI) | Between groups FC: EG = CG (p > 0.05) QoL: EG > CG (p = 0.001) Symptoms: EG > CG (p = 0.001) Within groups Not reported |
| Gravier et al. (2022) [25] | 36 | Long regimen prehabilitation sessions (3 90′ sessions per week for 5 weeks) | Short regimen of prehabilitation multimodal sessions:
| 5 90′ sessions per week for 3 weeks | FC (CPET) LCap (spirometry) QoL (EORTC-QLQ-C30/LC13) | No significant changes in any of the assessed outcomes (p > 0.05) |
| Fernández-Blanco et al. (2022) [27] | 71 | Usual care | Preoperative respiratory physiotherapy:
| 5 sessions per week for 4 weeks | Pain (VAS) PAL | Between groups Pain: EG > CG (p = 0.005) PAL: EG > CG (p < 0.05) Within groups Not reported |
| Jonsson, et al. (2019) [21] | 94 | Usual care | In-hospital physiotherapy:
| 5 20–30′ sessions during their hospital stay | FC (6MWT, IPAQ-E) LCap (spirometry) Dyspnea (mMRC) Pain (NRS) | Between groups No significant changes in any of the assessed outcomes (p > 0.05) Within groups FC: IPAQ-E improved in EG (p = 0.047) |
| Jonsson et al. (2019) [20] | 107 | Usual care | Pre- and postoperative in-hospital physiotherapy + standard care:
| 1–2 sessions of 10–30′ per day, 6 days a week, during their hospital stay | FC (6MWT) LCap (spirometry) Dyspnea (mMRC) Pain (VAS) | No significant changes in any of the assessed outcomes (p > 0.05) |
| Liu et al. (2020) [28] | 54 | Usual Care | Multimodal intervention:
| Respiratory physiotherapy: twice a day for 6 weeksAerobic exercise: 80′ a day for 6 weeks | FC (6MWT) LCap (MEP, MIP, LEV) | Between groups FC: EG > CG (p < 0.01) LCAP: EG > CG (p < 0.05) Within groups Not reported |
| Liu Z et al. (2020) [22] | 73 | Usual Care | Multimodal prehabilitation intervention:
| Exercise training: 30′ 3 days a week for 2 weeksRespiratory physiotherapy: 10′ twice daily for 2 weeks | FC (6MWT) LCap (spirometry) Functional disability (WHODAS 2.0) Anxiety and depression (HADS) Short-term recovery quality (QoR-9) | Between groups FC: EG > CG (p < 0.001) LCap (FVC): EG > CG (p = 0.021) Within groups Not reported |
| Lu et al. (2022) [23] | 68 | Usual Care | Respiratory Physiotherapy - ACBT training:
| 20′ twice a day, during their hospital stay, before and after surgery | FC (6MWT) Dyspnea (mMRC) Anxiety and depression (HADS) | Between groups Dyspnea: EG > CG (p < 0.05) Anxiety and depression: EG > CG (p < 0.05) Within groups Not reported |
| Rutkowska et al. (2019) [26] | 40 | Usual care | Multimodal intervention:
| 5 90′ sessions per week for 6 weeks | FC (6MWT, Fullerton test) LCap (spirometry) Dyspnea (Borg scale) | Between groups FC: (6MWT, TUG); EG > CG (p = 0.01) LCap: EG > CG (p < 0.05) Dyspnea: EG > CG (p = 0.04) Within groups Not reported |
| Author, Year | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Edbrooke et al. (2019) [24] | Y | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8/10 |
| Gravier et al. (2022) [25] | Y | Y | Y | Y | Y | N | N | Y | Y | Y | N | 7/10 |
| Fernández-Blanco et al. (2022) [27] | Y | Y | Y | Y | N | N | N | Y | Y | Y | N | 6/10 |
| Jonsson et al. (2019) [21] | Y | Y | Y | Y | Y | N | Y | N | N | Y | N | 6/10 |
| Jonsson et al. (2019) [20] | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | 8/10 |
| Liu et al. (2020) [28] | Y | Y | Y | Y | N | N | Y | N | Y | Y | N | 7/10 |
| Liu Zijia et al. (2020) [22] | Y | Y | Y | Y | N | N | Y | Y | Y | Y | N | 8/10 |
| Lu et al. (2022) [23] | Y | Y | Y | Y | N | N | Y | Y | Y | Y | N | 8/10 |
| Rutkowska et al. (2019) [26] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 10/10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valdivia-Martínez, M.; Fernández-Gualda, M.Á.; Gallegos-García, E.; Postigo-Martin, P.; Fernández-González, M.; Ortiz-Comino, L. Physiotherapy Interventions in Lung Cancer Patients: A Systematic Review. Cancers 2024, 16, 924. https://doi.org/10.3390/cancers16050924
Valdivia-Martínez M, Fernández-Gualda MÁ, Gallegos-García E, Postigo-Martin P, Fernández-González M, Ortiz-Comino L. Physiotherapy Interventions in Lung Cancer Patients: A Systematic Review. Cancers. 2024; 16(5):924. https://doi.org/10.3390/cancers16050924
Chicago/Turabian StyleValdivia-Martínez, Manuel, Miguel Ángel Fernández-Gualda, Elena Gallegos-García, Paula Postigo-Martin, María Fernández-González, and Lucía Ortiz-Comino. 2024. "Physiotherapy Interventions in Lung Cancer Patients: A Systematic Review" Cancers 16, no. 5: 924. https://doi.org/10.3390/cancers16050924
APA StyleValdivia-Martínez, M., Fernández-Gualda, M. Á., Gallegos-García, E., Postigo-Martin, P., Fernández-González, M., & Ortiz-Comino, L. (2024). Physiotherapy Interventions in Lung Cancer Patients: A Systematic Review. Cancers, 16(5), 924. https://doi.org/10.3390/cancers16050924