
The Efficacy and Safety of Immune Checkpoint Inhibitors in Adrenocortical Carcinoma: A Systematic Review and Meta-Analysis
 , , ,
, , ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Methodology
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Quality Assessment
2.4. Statistical Analyses
3. Results
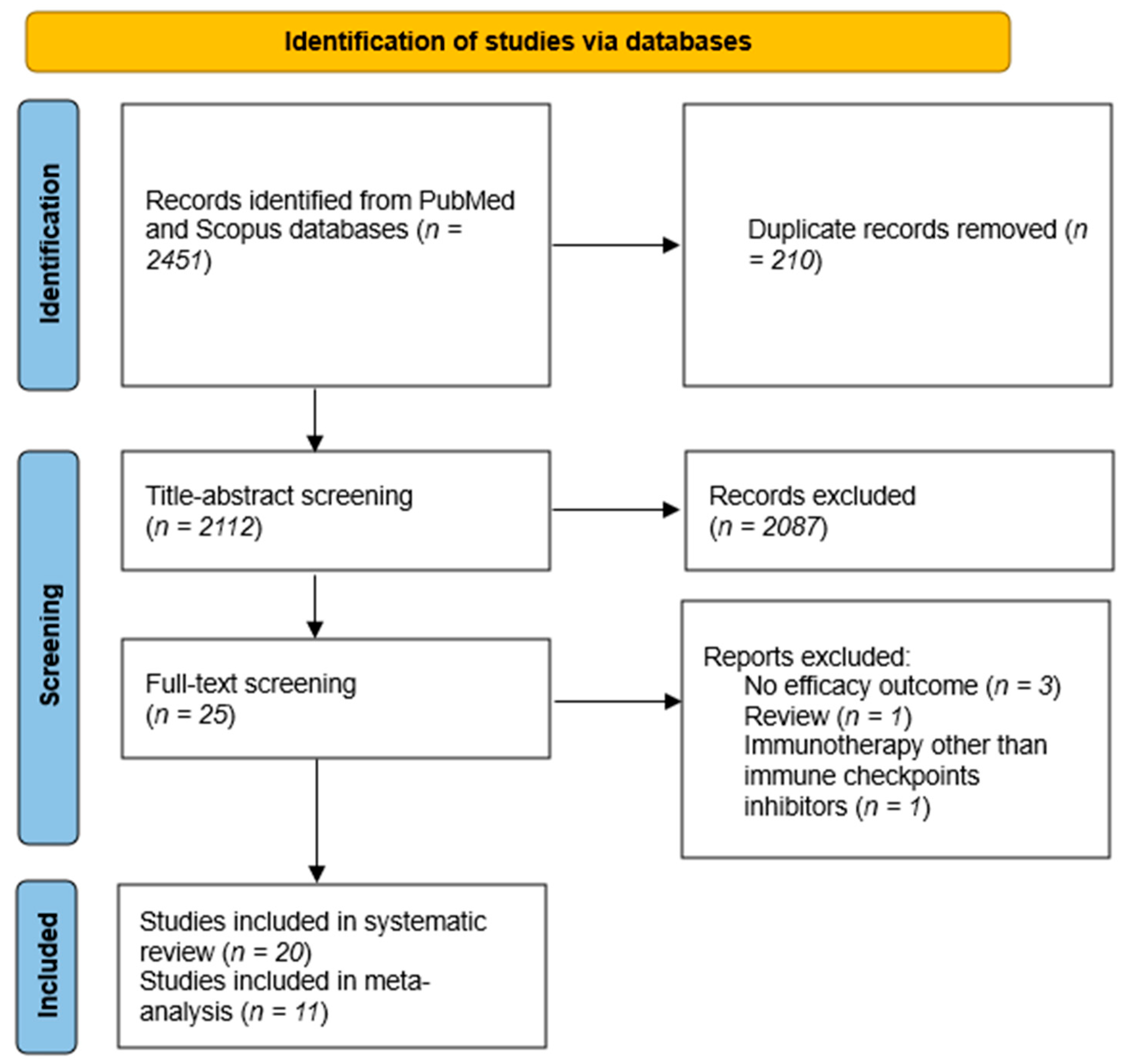
3.1. Search Results and Characteristics of the Included Trials
3.2. Risk of Bias Assessment
3.3. Meta-Analysis
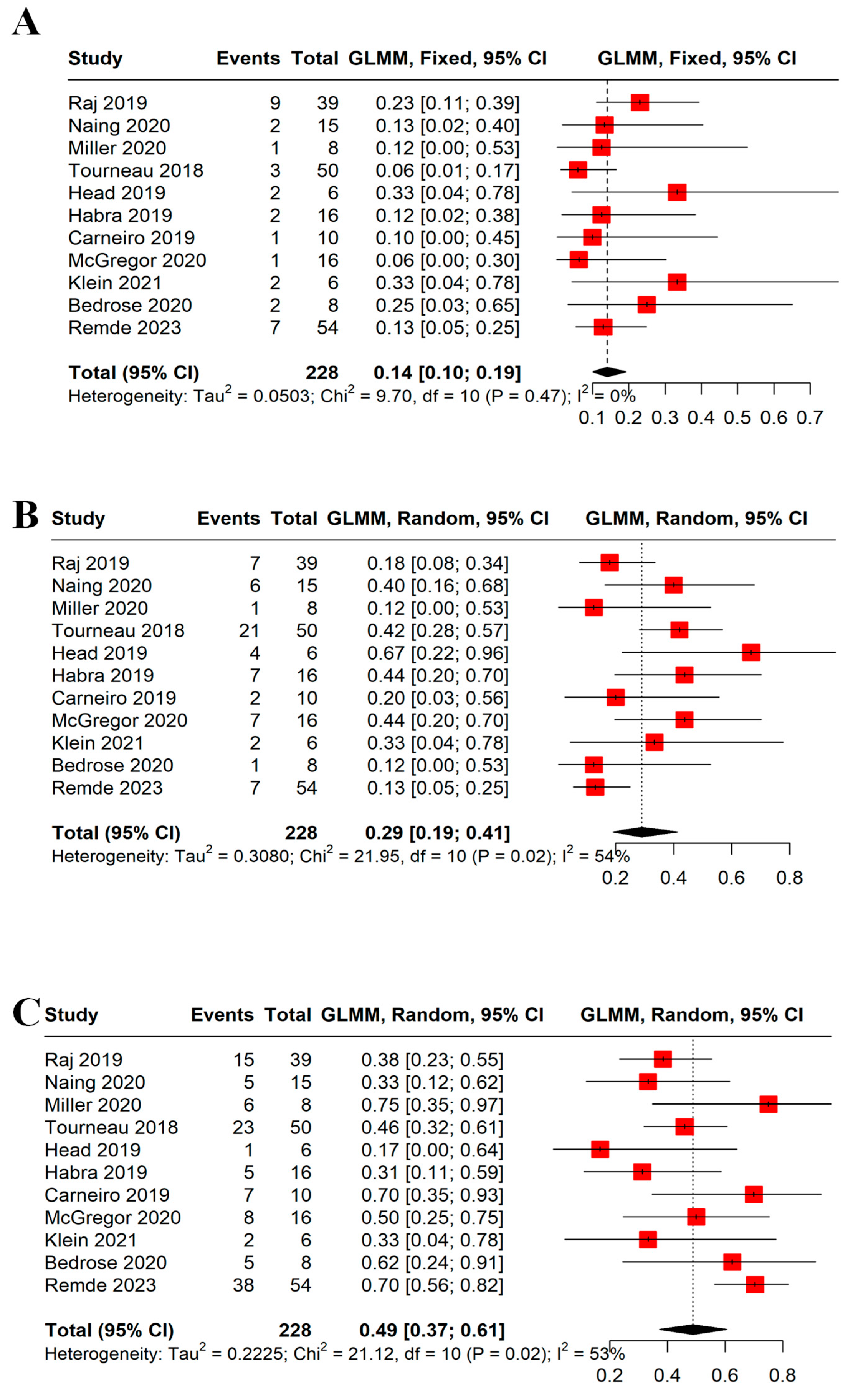
3.3.1. ORR and DCR
3.3.2. Best Overall Response
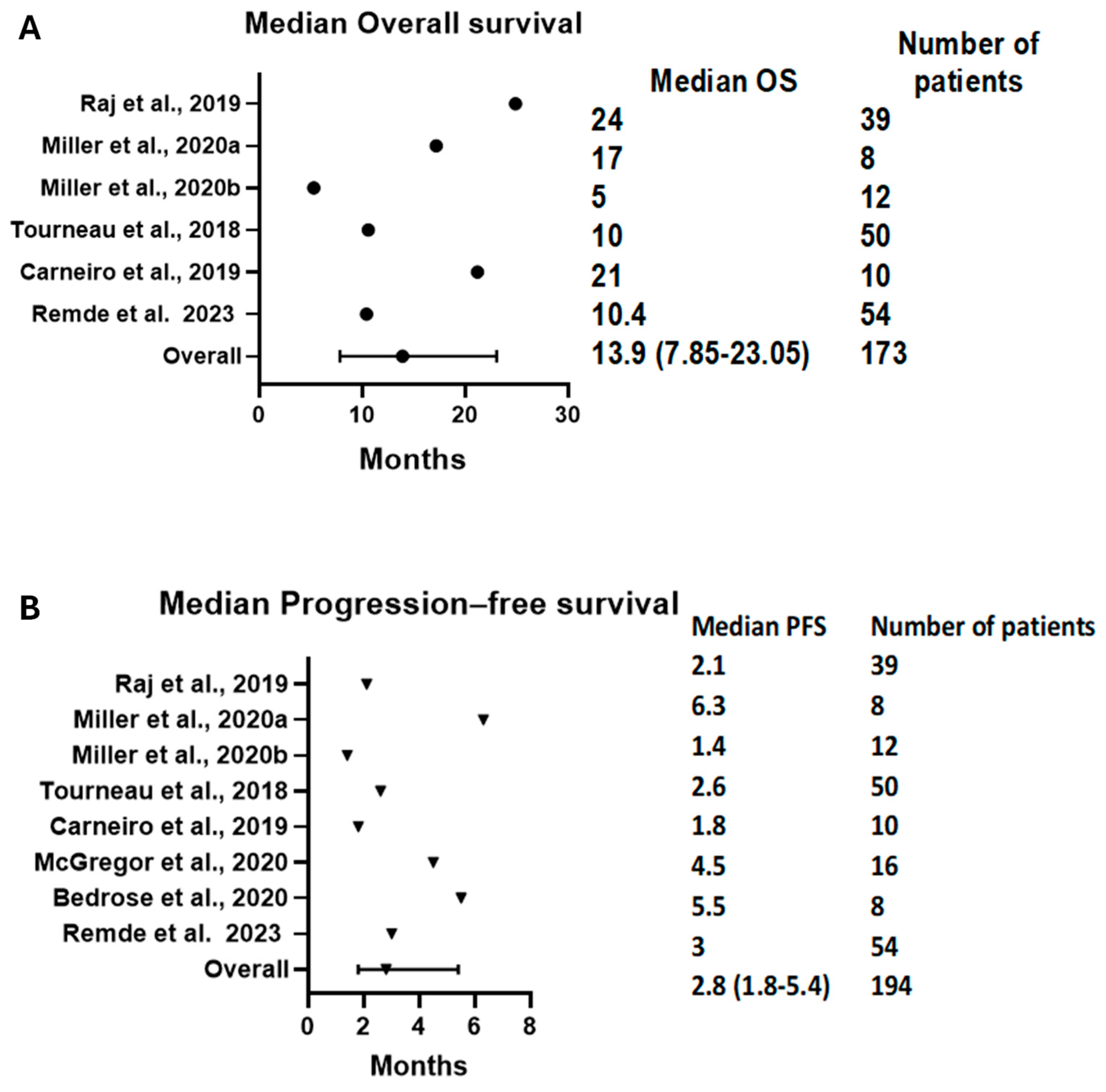
3.3.3. PFS and OS Results
3.3.4. Adverse Events
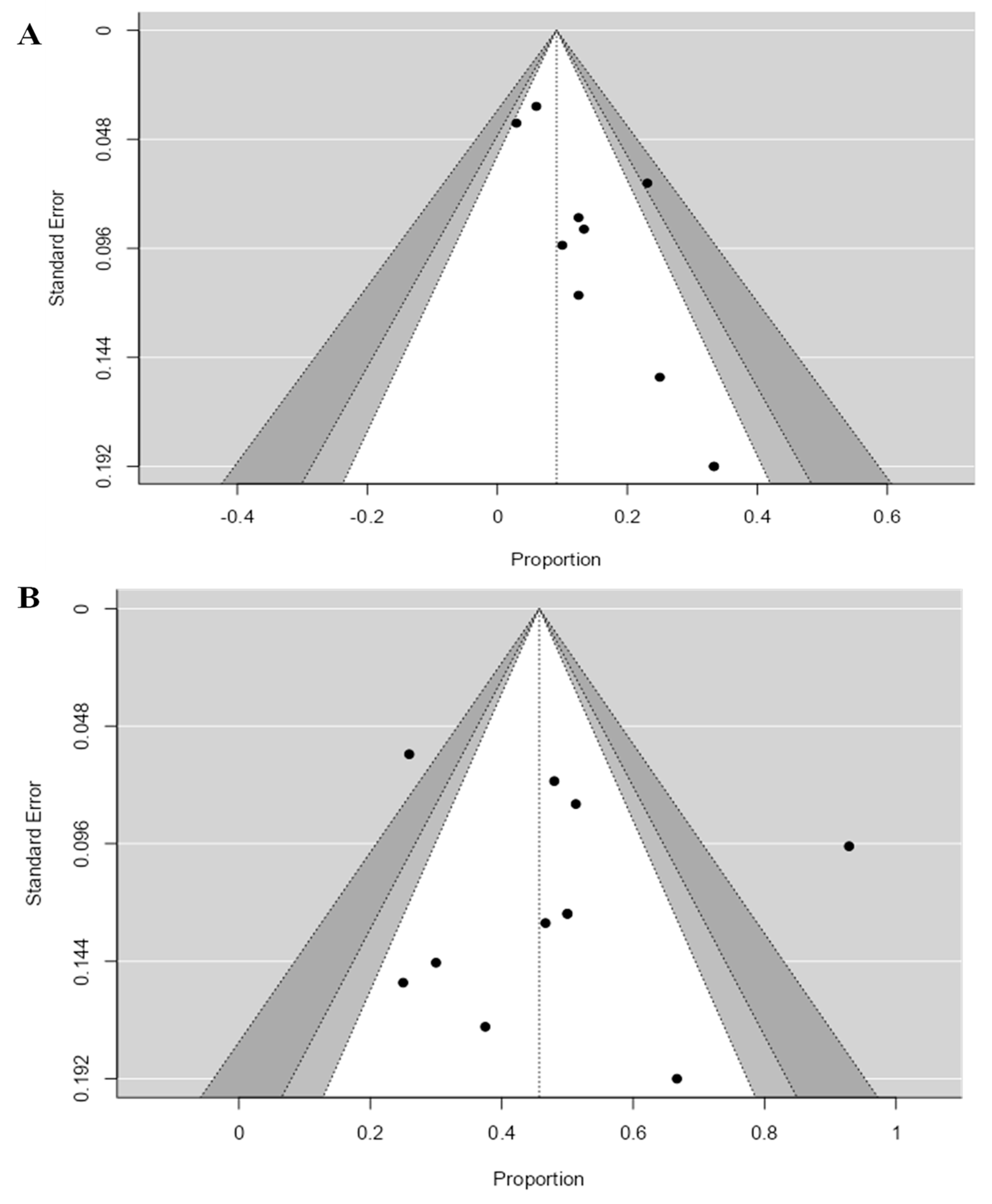
3.3.5. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Else, T.; Kim, A.C.; Sabolch, A.; Raymond, V.M.; Kandathil, A.; Caoili, E.M.; Jolly, S.; Miller, B.S.; Giordano, T.J.; Hammer, G.D. Adrenocortical carcinoma. Endocr. Rev. 2014, 35, 282–326. [Google Scholar] [CrossRef]
- Fassnacht, M.; Dekkers, O.M.; Else, T.; Baudin, E.; Berruti, A.; de Krijger, R.R.; Haak, H.R.; Mihai, R.; Assie, G.; Terzolo, M. European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors. Eur. J. Endocrinol. 2018, 179, G1–G46. [Google Scholar] [CrossRef]
- Fassnacht, M.; Terzolo, M.; Allolio, B.; Baudin, E.; Haak, H.; Berruti, A.; Welin, S.; Schade-Brittinger, C.; Lacroix, A.; Jarzab, B.; et al. Combination Chemotherapy in Advanced Adrenocortical Carcinoma. N. Engl. J. Med. 2012, 366, 2189–2197. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, T.J.; Gillis, A.; Alobuia, W.M.; Wild, H.; Kebebew, E. Surgery for adrenocortical carcinoma: When and how? Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101408. [Google Scholar] [CrossRef] [PubMed]
- Paragliola, R.M.; Torino, F.; Papi, G.; Locantore, P.; Pontecorvi, A.; Corsello, S.M. Role of Mitotane in Adrenocortical Carcinoma—Review and State of the art. Eur. Endocrinol. 2018, 14, 62. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, A.; Nehs, M.; Kilbridge, K. Treatment of Adrenocortical Carcinoma. Surg. Pathol. Clin. 2019, 12, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Haider, M.S.; Ahmad, T.; Groll, J.; Scherf-Clavel, O.; Kroiss, M.; Luxenhofer, R. The Challenging Pharmacokinetics of Mitotane: An Old Drug in Need of New Packaging. Eur. J. Drug Metab. Pharmacokinet. 2021, 46, 575. [Google Scholar] [CrossRef] [PubMed]
- Domènech, M.; Grau, E.; Solanes, A.; Izquierdo, A.; del Valle, J.; Carrato, C.; Pineda, M.; Dueñas, N.; Pujol, M.; Lázaro, C.; et al. Characteristics of Adrenocortical Carcinoma Associated with Lynch Syndrome. J. Clin. Endocrinol. Metab. 2021, 106, 318–325. [Google Scholar] [CrossRef]
- Gambichler, T.; Gambichler, T.; Finis, C.; Finis, C.; Abu Rached, N.; Abu Rached, N.; Scheel, C.H.; Scheel, C.H.; Becker, J.C.; Becker, J.C.; et al. Expression of DNA mismatch repair proteins in melanoma patients treated with immune checkpoint inhibitors. J. Cancer Res. Clin. Oncol. 2023, 149, 1241–1247. [Google Scholar] [CrossRef]
- Ellis, H.; Klempner, S.J.; Quintanilha, J.C.F.C.F.; Myer, P.; Lin, D.I.; Panarelli, N.; Fisher, V.; Li, G.; Huang, R.S.; Ross, J.S.; et al. Microsatellite instability (MSI), mismatch repair (MMR), and tumor mutational burden (TMB) as predictive biomarkers for immune checkpoint inhibitor (ICI) effectiveness in real-world patients with metastatic colorectal cancer (mCRC). J. Clin. Oncol. 2023, 41, 46. [Google Scholar] [CrossRef]
- Yamauchi, M.; Ono, A.; Amioka, K.; Fujii, Y.; Nakahara, H.; Teraoka, Y.; Uchikawa, S.; Fujino, H.; Nakahara, T.; Murakami, E.; et al. Lenvatinib activates anti-tumor immunity by suppressing immunoinhibitory infiltrates in the tumor microenvironment of advanced hepatocellular carcinoma. Commun. Med. 2023, 3, 152. [Google Scholar] [CrossRef]
- Baechle, J.J.; Hanna, D.N.; Sekhar, K.R.; Rathmell, J.C.; Rathmell, W.K.; Baregamian, N. Integrative computational immunogenomic profiling of cortisol-secreting adrenocortical carcinoma. J. Cell. Mol. Med. 2021, 25, 10061–10072. [Google Scholar] [CrossRef]
- Landwehr, L.-S.; Altieri, B.; Schreiner, J.; Sbiera, I.; Weigand, I.; Kroiss, M.; Fassnacht, M.; Sbiera, S. Interplay between glucocorticoids and tumor-infiltrating lymphocytes on the prognosis of adrenocortical carcinoma. J. Immunother. Cancer 2020, 8, 469. [Google Scholar] [CrossRef]
- Guven, D.C.; Stephen, B.; Sahin, T.K.; Cakir, I.Y.; Erul, E.; Aksoy, S. The efficacy of immune checkpoint inhibitors in rare tumors: A systematic review of published clinical trials. Crit. Rev. Oncol./Hematol. 2022, 174, 103700. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Consoli, F.; Ghidini, A.; Perego, G.; Luciani, A.; Mercurio, P.; Berruti, A.; Grisanti, S. Efficacy of Immune Checkpoint Inhibitors in Rare Tumours: A Systematic Review. Front. Immunol. 2021, 12, 720748. [Google Scholar] [CrossRef] [PubMed]
- Raj, N.; Zheng, Y.; Kelly, V.; Katz, S.S.; Chou, J.; Do, R.K.G.; Capanu, M.; Zamarin, D.; Saltz, L.B.; Ariyan, C.E.; et al. PD-1 Blockade in Advanced Adrenocortical Carcinoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 71–80. [Google Scholar] [CrossRef]
- Le Tourneau, C.; Hoimes, C.; Zarwan, C.; Wong, D.J.; Bauer, S.; Claus, R.; Wermke, M.; Hariharan, S.; von Heydebreck, A.; Kasturi, V.; et al. Avelumab in patients with previously treated metastatic adrenocortical carcinoma: Phase 1b results from the JAVELIN solid tumor trial. J. ImmunoTherapy Cancer 2018, 6, 111. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Database Syst. Rev. Implement. Rep. 2020, 18, 2127–2133. [Google Scholar] [CrossRef]
- McGrath, S.; Sohn, H.; Steele, R.; Benedetti, A. Meta-analysis of the difference of medians. Biom. J. Biom. Z. 2020, 62, 69–98. [Google Scholar] [CrossRef]
- Naing, A.; Meric-Bernstam, F.; Stephen, B.; Karp, D.D.; Hajjar, J.; Ahnert, J.R.; Piha-Paul, S.A.; Colen, R.R.; Jimenez, C.; Raghav, K.P.; et al. Phase 2 study of pembrolizumab in patients with advanced rare cancers. J. ImmunoTherapy Cancer 2020, 8, e000347. [Google Scholar] [CrossRef] [PubMed]
- Habra, M.A.; Stephen, B.; Campbell, M.; Hess, K.; Tapia, C.; Xu, M.; Rodon Ahnert, J.; Jimenez, C.; Lee, J.E.; Perrier, N.D.; et al. Phase II clinical trial of pembrolizumab efficacy and safety in advanced adrenocortical carcinoma. J. ImmunoTherapy Cancer 2019, 7, 253. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, B.A.; Konda, B.; Costa, R.B.; Costa, R.L.B.; Sagar, V.; Gursel, D.B.; Kirschner, L.S.; Chae, Y.K.; Abdulkadir, S.A.; Rademaker, A.; et al. Nivolumab in Metastatic Adrenocortical Carcinoma: Results of a Phase 2 Trial. J. Clin. Endocrinol. Metab. 2019, 104, 6193–6200. [Google Scholar] [CrossRef] [PubMed]
- McGregor, B.A.; Campbell, M.T.; Xie, W.; Farah, S.; Bilen, M.A.; Schmidt, A.L.; Sonpavde, G.P.; Kilbridge, K.L.; Choudhury, A.D.; Mortazavi, A.; et al. Results of a multicenter, phase 2 study of nivolumab and ipilimumab for patients with advanced rare genitourinary malignancies. Cancer 2021, 127, 840–849. [Google Scholar] [CrossRef]
- Klein, O.; Senko, C.; Carlino, M.S.; Markman, B.; Jackett, L.; Gao, B.; Lum, C.; Kee, D.; Behren, A.; Palmer, J.; et al. Combination immunotherapy with ipilimumab and nivolumab in patients with advanced adrenocortical carcinoma: A subgroup analysis of CA209-538. Oncoimmunology 2021, 10, 1908771. [Google Scholar] [CrossRef]
- Geoerger, B.; Kang, H.J.; Yalon-Oren, M.; Marshall, L.V.; Vezina, C.; Pappo, A.; Laetsch, T.W.; Petrilli, A.S.; Ebinger, M.; Toporski, J.; et al. Pembrolizumab in paediatric patients with advanced melanoma or a PD-L1-positive, advanced, relapsed, or refractory solid tumour or lymphoma (KEYNOTE-051): Interim analysis of an open-label, single-arm, phase 1–2 trial. Lancet Oncol. 2020, 21, 121–133. [Google Scholar] [CrossRef]
- Edenfield, W.J.; Chung, K.; O’Rourke, M.; Cull, E.; Martin, J.; Bowers, H.; Smith, W.; Gluck, W.L. A Phase II Study of Durvalumab in Combination with Tremelimumab in Patients with Rare Cancers. Oncologist 2021, 26, e1499–e1507. [Google Scholar] [CrossRef]
- Sakamuri, D.; Glitza, I.C.; Cuellar, S.L.B.; Subbiah, V.; Fu, S.; Tsimberidou, A.M.; Wheler, J.J.; Hong, D.S.; Naing, A.; Falchook, G.S.; et al. Phase I dose-escalation study of anti–ctla-4 antibody ipilimumab and lenalidomide in patients with advanced cancers. Mol. Cancer Ther. 2018, 17, 671–676. [Google Scholar] [CrossRef]
- Miller, K.C.; Chintakuntlawar, A.V.; Hilger, C.; Bancos, I.; Morris, J.C.; Ryder, M.; Smith, C.Y.; Jenkins, S.M.; Bible, K.C. Salvage Therapy with Multikinase Inhibitors and Immunotherapy in Advanced Adrenal Cortical Carcinoma. J. Endocr. Soc. 2020, 4, bvaa069. [Google Scholar] [CrossRef]
- Head, L.; Kiseljak-Vassiliades, K.; Clark, T.J.; Somerset, H.; King, J.; Raeburn, C.; Albuja-Cruz, M.; Weyant, M.; Cleveland, J.; Wierman, M.E.; et al. Response to Immunotherapy in Combination with Mitotane in Patients with Metastatic Adrenocortical Cancer. J. Endocr. Soc. 2019, 3, 2295–2304. [Google Scholar] [CrossRef]
- Remde, H.; Schmidt-Pennington, L.; Reuter, M.; Landwehr, L.-S.; Jensen, M.; Lahner, H.; Kimpel, O.; Altieri, B.; Laubner, K.; Schreiner, J.; et al. Outcome of immunotherapy in adrenocortical carcinoma: A retrospective cohort study. Eur. J. Endocrinol. 2023, 188, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Bedrose, S.; Miller, K.C.; Altameemi, L.; Ali, M.S.; Nassar, S.; Garg, N.; Daher, M.; Eaton, K.D.; Yorio, J.T.; Daniel, D.B.; et al. Combined lenvatinib and pembrolizumab as salvage therapy in advanced adrenal cortical carcinoma. J. ImmunoTherapy Cancer 2020, 8, e001009. [Google Scholar] [CrossRef] [PubMed]
- Mota, J.M.; Sousa, L.G.; Braghiroli, M.I.; Siqueira, L.T.; Neto, J.E.B.; Chapchap, P.; De Oliveira Hoff, A.A.; Hoff, P.M. Pembrolizumab for metastatic adrenocortical carcinoma with high mutational burden Two case reports. Medicine 2018, 97, e13517. [Google Scholar] [CrossRef] [PubMed]
- Casey, R.; Giger, O.; Seetho, I.; Marker, A.; Pitfield, D.; Boyle, L.; Gurnell, M.; Shaw, A.; Tischkowitz, M.; Maher, E.; et al. Rapid disease progression in a patient with mismatch repair-deficient and cortisol secreting adrenocortical carcinoma treated with pembrolizumab. Semin. Oncol. 2018, 45, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Caccese, M.; Ceccato, F.; Fassan, M.; Fassina, A.; Padovan, M.; Mammi, I.; Iacobone, M.; Scaroni, C.; Zagonel, V.; Lombardi, G. Letter to Editor: Reply to R.T. Casey (Semin Oncol. 2018 Jun;45(3):151-155). Semin. Oncol. 2019, 46, 104–105. [Google Scholar] [CrossRef] [PubMed]
- Alam, W.; Bouferraa, Y.; Haibe, Y.; Shamseddine, A. Complete Radiological Response of Recurrent Metastatic Adrenocortical Carcinoma to Pembrolizumab and Mitotane. Clin. Med. Insights Oncol. 2021, 15, 11795549211007682. [Google Scholar] [CrossRef] [PubMed]
- Weng, Y.; Wang, L.; Wang, X.-Y.; Fan, X.-X.; Yan, L.; Li, Z.-H.; Zhang, S.-L. Case report: Remarkable response to a novel combination of mitotane, etoposide, paraplatin, and sintilimab in a patient with metastatic adrenocortical carcinoma. Front. Endocrinol. 2023, 14, 1115893. [Google Scholar] [CrossRef]
- Charles, R.; Madhu, D.; Powles, A.; Boyde, A.; Hughes, O.; Kumar, N.; Moorcraft, S.Y. Case Report: Response to ipilimumab and nivolumab in a patient with adrenocortical carcinoma. Front. Oncol. 2023, 13, 1242560. [Google Scholar] [CrossRef]
- Marcus, L.; Lemery, S.J.; Keegan, P.; Pazdur, R. FDA approval summary: Pembrolizumab for the treatment of microsatellite instability-high solid tumors. Clin. Cancer Res. 2019, 25, 3753–3758. [Google Scholar] [CrossRef]
- Brabo, E.P.; Moraes, A.B.; Neto, L.V. The role of immune checkpoint inhibitor therapy in advanced adrenocortical carcinoma revisited: Review of literature. J. Endocrinol. Investig. 2020, 43, 1531–1542. [Google Scholar] [CrossRef]
- Alsaab, H.O.; Sau, S.; Alzhrani, R.; Tatiparti, K.; Bhise, K.; Kashaw, S.K.; Iyer, A.K. PD-1 and PD-L1 checkpoint signaling inhibition for cancer immunotherapy: Mechanism, combinations, and clinical outcome. Front. Pharmacol. 2017, 8, 273409. [Google Scholar] [CrossRef] [PubMed]
- Tartarone, A.; Roviello, G.; Lerose, R.; Roudi, R.; Aieta, M.; Zoppoli, P. Anti-PD-1 versus anti-PD-L1 therapy in patients with pretreated advanced non-small-cell lung cancer: A meta-analysis. Future Oncol. 2019, 15, 2423–2433. [Google Scholar] [CrossRef]
- Tierney, J.F.; Vogle, A.; Poirier, J.; Min, I.M.; Finnerty, B.; Zarnegar, R.; Pappas, S.G.; Scognamiglio, T.; Ghai, R.; Gattuso, P.; et al. Expression of programmed death ligand 1 and 2 in adrenocortical cancer tissues: An exploratory study. Surgery 2019, 165, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Fay, A.P.; Signoretti, S.; Callea, M.; Telό, G.H.; McKay, R.R.; Song, J.; Carvo, I.; Lampron, M.E.; Kaymakcalan, M.D.; Poli-De-Figueiredo, C.E.; et al. Programmed death ligand-1 expression in adrenocortical carcinoma: An exploratory biomarker study. J. ImmunoTherapy Cancer 2015, 3, 3. [Google Scholar] [CrossRef]
- Marcus, L.; Fashoyin-Aje, L.A.; Donoghue, M.; Yuan, M.; Rodriguez, L.; Gallagher, P.S.; Philip, R.; Ghosh, S.; Theoret, M.R.; Beaver, J.A.; et al. FDA Approval Summary: Pembrolizumab for the Treatment of Tumor Mutational Burden-High Solid Tumors. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2021, 27, 4685–4689. [Google Scholar] [CrossRef]
- Grisanti, S.; Cosentini, D.; Laganà, M.; Volta, A.D.; Palumbo, C.; Tiberio, G.A.M.; Sigala, S.; Berruti, A. The long and winding road to effective immunotherapy in patients with adrenocortical carcinoma. Future Oncol. 2020, 16, 3017–3020. [Google Scholar] [CrossRef]
- Fiorentini, C.; Grisanti, S.; Cosentini, D.; Abate, A.; Rossini, E.; Berruti, A.; Sigala, S. Molecular Drivers of Potential Immunotherapy Failure in Adrenocortical Carcinoma. J. Oncol. 2019, 2019, 6072863. [Google Scholar] [CrossRef] [PubMed]
- Baechle, J.J.; Hanna, D.N.; Konjeti, S.R.; Rathmell, J.C.; Rathmell, W.K.; Baregamian, N. Multiplatform Integrative Analyses of Immunosuppressive Signatures in Cortisol-secreting Adrenocortical Carcinoma. bioRxiv 2021. [Google Scholar] [CrossRef]
- Liu, S.; Ding, G.; Zhou, Z.; Feng, C. β-Catenin-driven adrenocortical carcinoma is characterized with immune exclusion. OncoTargets Ther. 2018, 11, 2029–2036. [Google Scholar] [CrossRef]
- Ganesh, S.; Shui, X.; Craig, K.P.; Park, J.; Wang, W.; Brown, B.D.; Abrams, M.T. RNAi-Mediated β-Catenin Inhibition Promotes T Cell Infiltration and Antitumor Activity in Combination with Immune Checkpoint Blockade. Mol. Ther. 2018, 26, 2567. [Google Scholar] [CrossRef]
- Haas, M.S.; Kagey, M.H.; Heath, H.; Schuerpf, F.; Rottman, J.B.; Newman, W. mDKN-01, a Novel Anti-DKK1 mAb, Enhances Innate Immune Responses in the Tumor Microenvironment. Mol. Cancer Res. 2021, 19, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Li, F.; Cheng, X.; Wang, J.; Zhang, W.; Zhang, B.; Tang, Y.; Li, Q.; Zhou, C.; Tu, S. Wnt Inhibition Sensitizes PD-L1 Blockade Therapy by Overcoming Bone Marrow-Derived Myofibroblasts-Mediated Immune Resistance in Tumors. Front. Immunol. 2021, 12, 619209. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Yao, Z.; Yang, H.; Liang, N.; Zhang, X.; Zhang, F. Are immune-related adverse events associated with the efficacy of immune checkpoint inhibitors in patients with cancer? A systematic review and meta-analysis. BMC Med. 2020, 18, 87. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Total Number of Patients (ACC Patients) | Median Age in Years (Range) | Female Percentage | Median Follow-Up Months (Range) | Therapy/Regimen | Stage | ECOG | Cortisol Producing | MSI-H/ MMR-D | Lynch Syndrome | PD-L1 High † | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | ||||||||||||
| Tourneau et al., 2018 [17] | Open-label phase I clinical trial | 50 (50) | 50 (21–71) | 52% | 16.5 m (11.7–27.6) | Avelumab (50% of the patients received concurrent mitotane) | Metastatic | 19 | 31 | 0 | NR | NR | NR | 12 |
| Raj et al., 2019 [16] | Open-label phase II clinical trial | 39 (39) | 62 (19–87) | 61.5% | 17.8 m (5.4–34.7) | Pembrolizumab | Advanced/metastatic | 11 | 28 | 0 | NR | 6 | 2 | 7 |
| Habra et al., 2019 [22] | Open-label phase II clinical trial | 16 (16) | 48 (31–78) | 50% | NR | Pembrolizumab | Metastatic | 1 | 13 | 0 | 10 | 1 | NR | 0 |
| McGregor et al., 2020 [24] | Open-label phase II clinical trial | 55 (16) | 45 | 72.2% | 8.9 m (2.6–17.1) | Nivolumab and ipilimumab | Advanced/metastatic | 11 | 7 | 0 | NR | NR | NR | NR |
| Naing et al., 2020 [21] | Open-label phase II clinical trial | 127 (15) | 56 (22–84) | 46.5% | NR | Pembrolizumab | Advanced/metastatic | 15 | 112 | 0 | NR | NR | NR | Mixed * |
| Remde et al., 2023 [31] | Retrospective cohort | 54 (54) | 46 (19–70) | 57.4% | NR | Pembrolizumab: 59% Nivolumab: 24% Avelumab: 11% Atezolizumab: 2% Ipilimumab and nivolumab: 4% | Metastatic | NR | 28 | 3 | 1 | 8 | ||
| Miller et al., 2020 [29] | Retrospective cohort | 15 (15) | 43 (19–62) | 46.7% | 83.0 m (22.5–83.0) | Pembrolizumab/MKI | Stage I: 1 patient Stage II: 4 patients Stage III: 4 patients Stage IV: 5 patients | NR | NR | NR | NR | NR | ||
| Carneiro et al., 2019 [23] | Open-label phase II clinical trial | 10 (10) | 57 (31–67) | 70% | 4.5 m (0.1–25.6) | Nivolumab | Metastatic | 5 | 3 | 2 | 4 | 0 | NR | 6 |
| Bedrose et al., 2020 [32] | Case series | 8 (8) | 38 (21–49) | 50% | NR | Pembrolizumab and lenvatinib | Stage II: 3 patients Stage III: 2 patients Stage IV: 3 patients | NR | 3 | 0 | 0 | NR | ||
| Head et al., 2019 [30] | Retrospective cohort | 6 (6) | 45 (24–65) | 100% | NR | Pembrolizumab and mitotane | Stage I: 1 patient Stage III: 3 patients Stage IV: 2 patients | 1 | 5 | 0 | 3 | 1 | 2 | NR |
| Klein et al., 2021 [25] | Open-label phase II clinical trial | 6 (6) | 48 (22–72) | 66.7% | 14.7 m | Nivolumab and ipilimumab | Stage II: 1 patient Stage III: 3 patients Stage IV: 2 patients | 5 | 1 | 0 | 2 | 2 | NR | 2 |
| Geoerger et al., 2019 [26] | Open-label phase II clinical trial | 154 (4) | 13 (8–15) | 48.1% | 8·6 m (2·5–16·4) [Mixed *] | Pembrolizumab | Mixed * | NR | NR | NR | NR | 4 | ||
| Mota et al., 2018 [33] | Case report | 2 (2) | 28 and 40 | 50% | NR | Pembrolizumab | Metastatic | NR | NR | 1 | 0 | NR | ||
| Edenfield et al., 2021 [27] | Open-label phase II clinical trial | 50 (2) | 62 (26–78) | 56% | NR | Durvalumab and tremelimumab | Advanced/metastatic | Mixed * | NR | 0 | 0 | 1 | ||
| Sakamuri et al., 2017 [28] | Open-label phase I clinical trial | 36 (2) | 56 (19–75) | 66.7% | Mixed * | Ipilimumab and lenalidomide | Advanced/metastatic | Mixed * | NR | NR | NR | NR | ||
| Casey et al., 2018 [34] | Case report | 1 (1) | 58 | 100% | NR | Pembrolizumab | Stage III | NR | 1 | 1 | 1 | 0 | ||
| Caccese et al., 2019 [35] | Case report | 1 (1) | 29 | 0% | NR | Pembrolizumab | Metastatic | NR | 1 | 1 | 0 | 0 | ||
| Alam et al., 2021 [36] | Case report | 1 (1) | 40 | 100% | NR | Pembrolizumab and mitotane | Stage IV | NR | NR | 0 | 0 | 0 | ||
| Weng et al. 2023 [37] | Case report | 1 (1) | 36 | 0% | NR | Sintilimab, mitotane, etoposide, and paraplatin | Stage IV | NR | NR | 1 | 0 | NR | ||
| Charles et al. 2023 [38] | Case report | 1 (1) | 32 | 100% | NR | Ipilimumab and nivolumab | Stage IV | NR | 0 | 0 | 0 | NR | ||
| Number of Studies | All Grades | Grade 3/4 | |
|---|---|---|---|
| Fatigue | 7 | 32/130 (24.6%) | 0 (0%) |
| Nausea/vomiting | 6 | 28/122 (23%) | 1/122 (0.8%) |
| Elevated liver enzymes/hepatitis | 9 | 27/154 (17.5%) | 6/154 (3.9%) |
| Dyspnea | 4 | 5/39 (12.8%) | 0 (0%) |
| Rash | 7 | 17/139 (12.2%) | 0 (0%) |
| Hypothyroidism | 5 | 14/160 (8.8%) | 0 (0%) |
| Anorexia | 3 | 5/61 (8.2%) | 0 (0%) |
| Diarrhea | 5 | 12/157 (7.6%) | 1/157 (0.6%) |
| Pneumonitis | 6 | 12/192 (6.3%) | 6/192 (3.1%) |
| Adrenal insufficiency | 5 | 8/146 (5.5%) | 2/146 (1.4%) |
| Anemia | 5 | 9/167 (5.4%) | 2/113 (1.2%) |
| NCT Identifier | Phase | Treatment | Tumor Type | Status | Endpoints |
|---|---|---|---|---|---|
| NCT05563467 | II | Pembrolizumab | ACC | Recruiting | ORR, AEs, QoL |
| NCT04373265 | I | Relacorilant with Pembrolizumab | ACC | Active, not recruiting | DLT, PFS, AEs |
| NCT05634577 | II | Mitotane with Pembrolizumab | ACC | Recruiting | ORR, OS, PFS, AEs |
| NCT04318730 | II | Camrelizumab with Apatinib | ACC | Recruiting | ORR |
| NCT05036434 | II | Pembrolizumab with Lenvatinib | ACC | Not yet recruiting | ORR, AEs |
| NCT06006013 | II | Cabozantinib with Atezolizumab | ACC | Not yet recruiting | ORR, OS, PFS, AEs |
| NCT04187404 | I/II | EO2401 with Nivolumab | ACC and malignant pheochromocytoma/paraganglioma | Recruiting | AEs, OS, PFS |
| NCT02834013 | II | Ipilimumab with Nivolumab | Multiple tumors | Active, not recruiting | ORR, AEs |
| NCT02637531 | I | Eganelisib with Nivolumab | Multiple tumors | Active, not recruiting | DLT, AEs, PFS, OS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ababneh, O.; Ghazou, A.; Alawajneh, M.; Alhaj Mohammad, S.; Bani-Hani, A.; Alrabadi, N.; Shreenivas, A. The Efficacy and Safety of Immune Checkpoint Inhibitors in Adrenocortical Carcinoma: A Systematic Review and Meta-Analysis. Cancers 2024, 16, 900. https://doi.org/10.3390/cancers16050900
Ababneh O, Ghazou A, Alawajneh M, Alhaj Mohammad S, Bani-Hani A, Alrabadi N, Shreenivas A. The Efficacy and Safety of Immune Checkpoint Inhibitors in Adrenocortical Carcinoma: A Systematic Review and Meta-Analysis. Cancers. 2024; 16(5):900. https://doi.org/10.3390/cancers16050900
Chicago/Turabian StyleAbabneh, Obada, Alina Ghazou, Mohmmad Alawajneh, Saleh Alhaj Mohammad, Abdullah Bani-Hani, Nasr Alrabadi, and Aditya Shreenivas. 2024. "The Efficacy and Safety of Immune Checkpoint Inhibitors in Adrenocortical Carcinoma: A Systematic Review and Meta-Analysis" Cancers 16, no. 5: 900. https://doi.org/10.3390/cancers16050900
APA StyleAbabneh, O., Ghazou, A., Alawajneh, M., Alhaj Mohammad, S., Bani-Hani, A., Alrabadi, N., & Shreenivas, A. (2024). The Efficacy and Safety of Immune Checkpoint Inhibitors in Adrenocortical Carcinoma: A Systematic Review and Meta-Analysis. Cancers, 16(5), 900. https://doi.org/10.3390/cancers16050900