
Lymphocyte Function at Baseline Could Be a New Predictor of Tumor Burden following Six Cycles of Radium-223 Therapy in Patients with Metastasized, Castration-Resistant Prostate Cancer


 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Lymphocyte Transformation Test
2.3. ELISpot Assay
2.4. Assessment of Tumor Burden
2.5. Statistical Analysis
3. Results
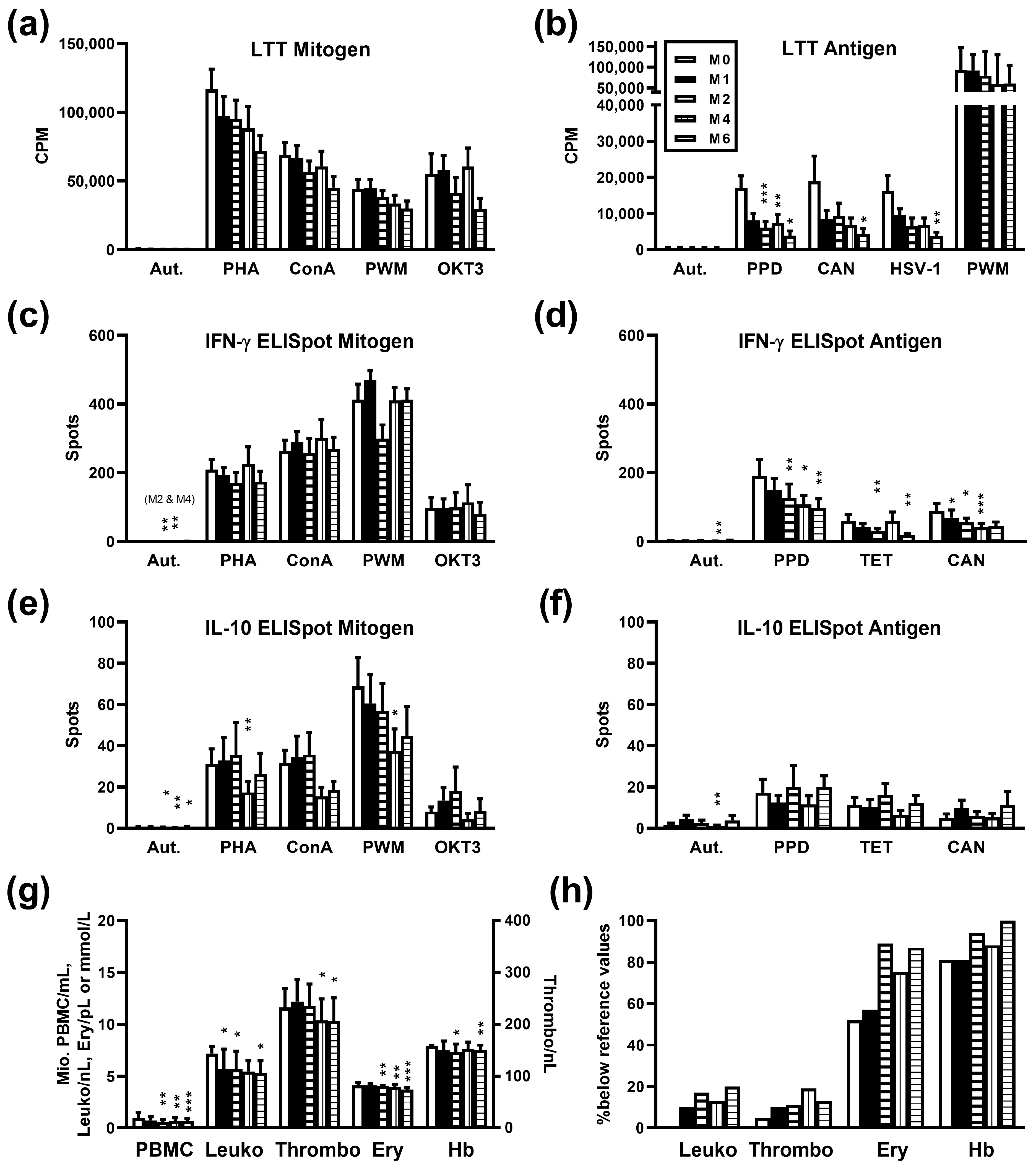
3.1. Immune Response after Radium-223 Therapy
3.2. Influence of Radium-223 Therapy on Blood Cell Counts and Hemoglobin Concentration
3.3. Influence of Radium-223 Therapy on Tumor Burden
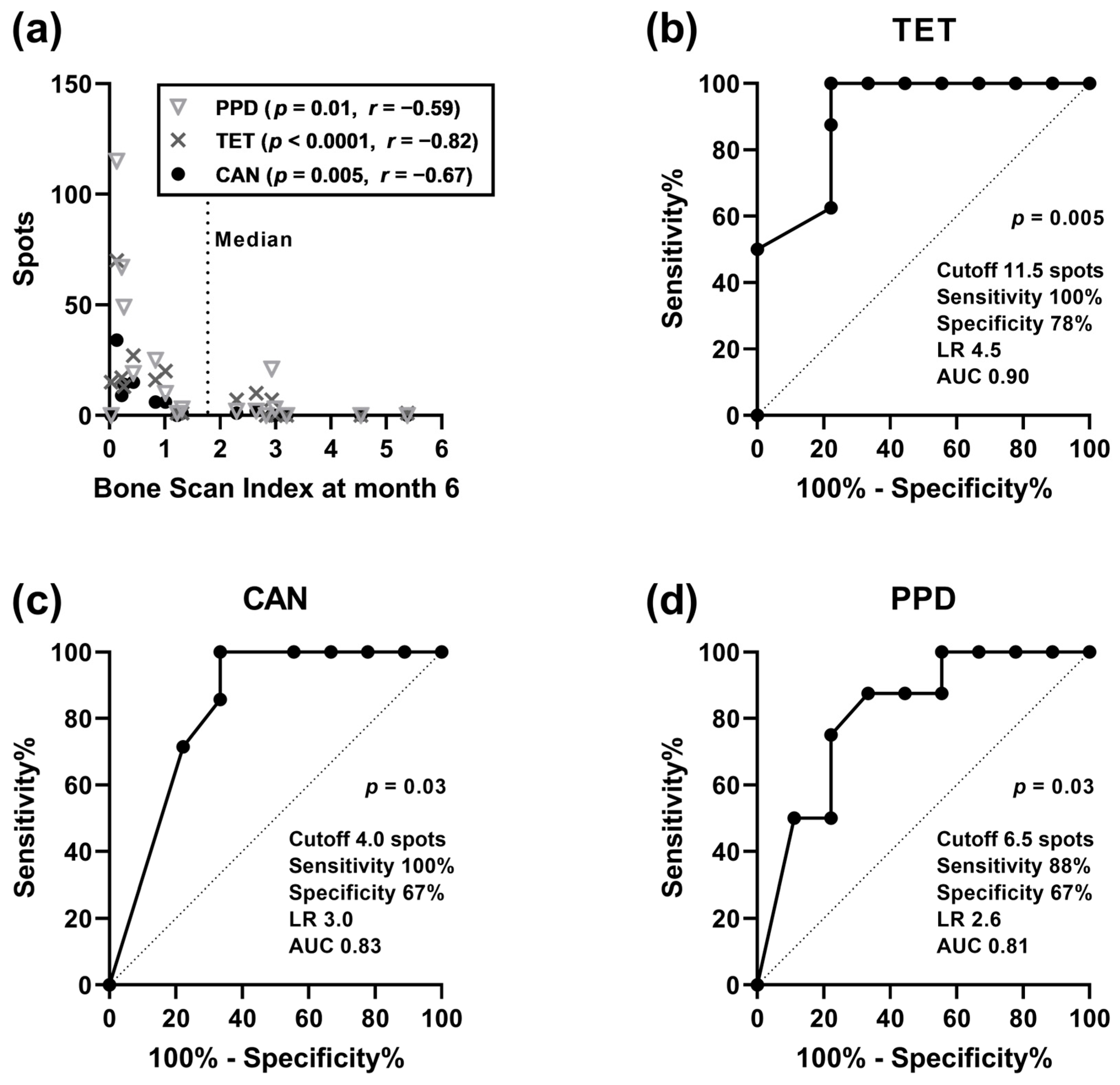
3.4. Correlation Analysis of Clinical Parameters and Cellular In Vitro Immune Responses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Archer Goode, E.; Wang, N.; Munkley, J. Prostate cancer bone metastases biology and clinical management (Review). Oncol. Lett. 2023, 25, 163. [Google Scholar] [CrossRef]
- EMA. Xofigo. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/xofigo#ema-inpage-item-product-info (accessed on 30 January 2024).
- Miederer, M.; Thomas, C.; Beck, J.; Hampel, C.; Krieger, C.; Baque, P.E.; Helisch, A.; Schreckenberger, M. Haematopoietic toxicity of radium-223 in patients with high skeletal tumour burden. Nuklearmedizin 2015, 54, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Humm, J.L.; Sartor, O.; Parker, C.; Bruland, O.S.; Macklis, R. Radium-223 in the treatment of osteoblastic metastases: A critical clinical review. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 898–906. [Google Scholar] [CrossRef] [PubMed]
- Parker, C.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Fossa, S.D.; Chodacki, A.; Wiechno, P.; Logue, J.; Seke, M.; et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N. Engl. J. Med. 2013, 369, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Kuronya, Z.; Sinkovics, I.; Agoston, P.; Biro, K.; Bodrogi, I.; Bode, I.; Dank, M.; Gyergyay, F.; Vajdics, T.; Kolonics, Z.; et al. A Retrospective Analysis of the First 41 mCRPC Patients with Bone Pain Treated with Radium-223 at the National Institute of Oncology in Hungary. Pathol. Oncol. Res. 2017, 23, 777–783. [Google Scholar] [CrossRef]
- Wilson, J.M.; Parker, C. The safety and efficacy of radium-223 dichloride for the treatment of advanced prostate cancer. Expert. Rev. Anticancer. Ther. 2016, 16, 911–918. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Harrison, M.R.; Wong, T.Z.; Armstrong, A.J.; George, D.J. Radium-223 chloride: A potential new treatment for castration-resistant prostate cancer patients with metastatic bone disease. Cancer Manag. Res. 2013, 5, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Carrasquillo, J.A.; Donoghue, J.A.O.; Pandit-Taskar, N.; Rathkopf, D.E.; Aksnes, A.; Viner, C.L.; Hong, C.T.; Larson, S.M.; Scher, H.I.; Morris, M.J. Phase I pharmacokinetic (PK) and biodistribution study of radium-223 chloride in patients with castration resistant prostate cancer (CRPC) metastatic to bone. J. Clin. Oncol. 2010, 28, 4680. [Google Scholar] [CrossRef]
- Barsegian, V.; Müller, S.P.; Horn, P.A.; Bockisch, A.; Lindemann, M. Lymphocyte function following radioiodine therapy in patients with thyroid carcinoma. Nuklearmedizin 2011, 50, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Barsegian, V.; Hueben, C.; Mueller, S.P.; Poeppel, T.D.; Horn, P.A.; Bockisch, A.; Lindemann, M. Impairment of lymphocyte function following yttrium-90 DOTATOC therapy. Cancer Immunol. Immunother. 2015, 64, 755–764. [Google Scholar] [CrossRef]
- Stevenson, A.F.; Daculsi, R.; Monig, H. Haematological studies on 90Sr-90Y-toxicity: II. Femoral CFU-s kinetics and mitogen response of spleen cells. Radiat. Environ. Biophys. 1982, 20, 275–287. [Google Scholar] [CrossRef]
- Domouchtsidou, A.; Barsegian, V.; Mueller, S.P.; Best, J.; Ertle, J.; Bedreli, S.; Horn, P.A.; Bockisch, A.; Lindemann, M. Impaired lymphocyte function in patients with hepatic malignancies after selective internal radiotherapy. Cancer Immunol. Immunother. 2018, 67, 843–853. [Google Scholar] [CrossRef]
- Domouchtsidou, A.; Barsegian, V.; Mueller, S.P.; Lobachevsky, P.; Best, J.; Horn, P.A.; Bockisch, A.; Lindemann, M. DNA lesions correlate with lymphocyte function after selective internal radiotherapy. Cancer Immunol. Immunother. 2019, 68, 907–915. [Google Scholar] [CrossRef]
- Barsegian, V.; Muller, S.P.; Mockel, D.; Horn, P.A.; Bockisch, A.; Lindemann, M. Lymphocyte function following radium-223 therapy in patients with metastasized, castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 242–246. [Google Scholar] [CrossRef]
- Tiepolt, C.; Gruning, T.; Franke, W.G. Renaissance of 224 Ra for the treatment of ankylosing spondylitis: Clinical experiences. Nucl. Med. Commun. 2002, 23, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Malamas, A.S.; Gameiro, S.R.; Knudson, K.M.; Hodge, J.W. Sublethal exposure to alpha radiation (223Ra dichloride) enhances various carcinomas’ sensitivity to lysis by antigen-specific cytotoxic T lymphocytes through calreticulin-mediated immunogenic modulation. Oncotarget 2016, 7, 86937–86947. [Google Scholar] [CrossRef] [PubMed]
- Guedeney, G.; Grunwald, D.; Malarbet, J.L.; Doloy, M.T. Time dependence of chromosomal aberrations induced in human and monkey lymphocytes by acute and fractionated exposure to 60Co. Radiat. Res. 1988, 116, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.E.; Lefkovits, I. Effects of irradiation on the in vitro immune response. Exp. Cell Biol. 1980, 48, 255–278. [Google Scholar] [CrossRef] [PubMed]
- Pourfathollah, A.A.; Shaiegan, M.; Namiri, M.; Babae, G.R. Effect of gamma irradiation on lymphocyte proliferation and IL-8 production by lymphocytes isolated from platelet concentrates. Arch. Med. Res. 2008, 39, 590–593. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.Z. Radiation-induced change in lymphocyte proliferation and its neuroendocrine regulation: Dose-response relationship and pathophysiological implications. Nonlinearity Biol. Toxicol. Med. 2004, 2, 233–243. [Google Scholar] [CrossRef]
- Herr, W.; Linn, B.; Leister, N.; Wandel, E.; Meyer zum Buschenfelde, K.H.; Wolfel, T. The use of computer-assisted video image analysis for the quantification of CD8+ T lymphocytes producing tumor necrosis factor alpha spots in response to peptide antigens. J. Immunol. Methods 1997, 203, 141–152. [Google Scholar] [CrossRef]
- Cox, J.H.; Ferrari, G.; Janetzki, S. Measurement of cytokine release at the single cell level using the ELISPOT assay. Methods 2006, 38, 274–282. [Google Scholar] [CrossRef]
- Lindemann, M.; Witzke, O.; Winterhagen, T.; Ross, B.; Kreuzfelder, E.; Reinhardt, W.; Roggendorf, M.; Mann, K.; Philipp, T.; Grosse-Wilde, H. T-cell function after interleukin-2 therapy in HIV-infected patients is correlated with serum cortisol concentrations. Aids 2004, 18, 2001–2007. [Google Scholar] [CrossRef] [PubMed]
- Lindemann, M.; Virchow, S.; Ramann, F.; Barsegian, V.; Kreuzfelder, E.; Siffert, W.; Muller, N.; Grosse-Wilde, H. The G protein beta3 subunit 825T allele is a genetic marker for enhanced T cell response. FEBS Lett. 2001, 495, 82–86. [Google Scholar] [CrossRef] [PubMed]
- EXINI. aBSI—Quantification of Bone Scans. Available online: https://exini.com/software-solutions/absi/ (accessed on 22 January 2024).
- Ulmert, D.; Kaboteh, R.; Fox, J.J.; Savage, C.; Evans, M.J.; Lilja, H.; Abrahamsson, P.A.; Bjork, T.; Gerdtsson, A.; Bjartell, A.; et al. A novel automated platform for quantifying the extent of skeletal tumour involvement in prostate cancer patients using the Bone Scan Index. Eur. Urol. 2012, 62, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Erdi, Y.E.; Humm, J.L.; Imbriaco, M.; Yeung, H.; Larson, S.M. Quantitative bone metastases analysis based on image segmentation. J. Nucl. Med. 1997, 38, 1401–1406. [Google Scholar]
- Tanikawa, T.; Wilke, C.M.; Kryczek, I.; Chen, G.Y.; Kao, J.; Nunez, G.; Zou, W. Interleukin-10 ablation promotes tumor development, growth, and metastasis. Cancer Res. 2012, 72, 420–429. [Google Scholar] [CrossRef]
- Bruland, O.S.; Nilsson, S.; Fisher, D.R.; Larsen, R.H. High-linear energy transfer irradiation targeted to skeletal metastases by the alpha-emitter Ra-223: Adjuvant or alternative to conventional modalities? Clin. Cancer Res. 2006, 12, 6250s–6257s. [Google Scholar] [CrossRef]
- Pöppel, T.D.; Andreeff, M.; Becherer, A.; Bockisch, A.; Fricke, E.; Geworski, L.; Heinzel, A.; Krause, B.J.; Krause, T.; Mitterhauser, M.; et al. Radionuklidtherapie von Knochenmetastasen mittels Radium-223. Nuklearmedizin 2016, 55, 177–186. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ID | Age | BSI 0 | BSI M3 | BSI M6 | % Change M6 vs. 0 |
|---|---|---|---|---|---|
| 1 | 78 | 3.85 | 2.55 | 2.83 | 74 |
| 2 | 76 | 2.64 | 3.27 | 2.30 | 87 |
| 3 | 83 | 4.62 | 3.51 | 4.54 | 98 |
| 4 | 57 | 0.87 | 0.78 | 0.83 | 95 |
| 5 | 66 | 0.39 | 0.73 | 1.22 | 313 |
| 6 | 66 | 3.32 | 2.75 | 2.65 | 80 |
| 7 | 66 | 1.12 | 0.37 | 0.03 | 3 |
| 8 | 77 | 5.54 | 4.53 | 2.93 | 53 |
| 9 | 75 | 0.35 | 0.26 | 0.22 | 63 |
| 10 | 70 | 2.56 | 2.75 | 3.20 | 125 |
| 11 | 60 | 7.12 | N.A. | N.A. | N.A. |
| 12 | 77 | 0.10 | 0.34 | 0.26 | 260 |
| 13 | 76 | 0.55 | 2.79 | 2.99 | 544 |
| 14 | 71 | 1.27 | 1.35 | 0.43 | 34 |
| 15 | 53 | 0.30 | 0.15 | 0.13 | 43 |
| 16 | 56 | 3.89 | 4.45 | 5.38 | 138 |
| 17 | 78 | 2.63 | N.A. | N.A. | N.A. |
| 18 | 65 | 6.68 | 10.98 | 1.31 | 20 |
| 19 | 68 | 1.01 | 1.07 | 1.01 | 100 |
| 20 | 80 | 1.59 | 2.04 | STOP | N.A. |
| 21 | 75 | 2.44 | 2.87 | 2.2 | 90 |
| IL-10 ELISpot at Baseline | BSI 0 | (n = 20) | BSI M3 | (n = 18) | BSI M6 | (n = 16–17) |
|---|---|---|---|---|---|---|
| p | r | p | r | p | r | |
| Autologous | 0.06 | −0.43 | 0.02 | −0.54 | 0.01 | −0.60 |
| Tuberculin | 0.01 | −0.55 | 0.07 | −0.43 | 0.01 | −0.59 |
| Tetanus toxoid | 0.03 | −0.49 | 0.008 | −0.60 | <0.0001 | −0.82 |
| Candida albicans | 0.02 | −0.54 | 0.01 | −0.59 | 0.005 | −0.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barsegian, V.; Möckel, D.; Buehler, S.; Müller, S.P.; Kreissl, M.C.; Ostheim, P.; Horn, P.A.; Lindemann, M. Lymphocyte Function at Baseline Could Be a New Predictor of Tumor Burden following Six Cycles of Radium-223 Therapy in Patients with Metastasized, Castration-Resistant Prostate Cancer. Cancers 2024, 16, 886. https://doi.org/10.3390/cancers16050886
Barsegian V, Möckel D, Buehler S, Müller SP, Kreissl MC, Ostheim P, Horn PA, Lindemann M. Lymphocyte Function at Baseline Could Be a New Predictor of Tumor Burden following Six Cycles of Radium-223 Therapy in Patients with Metastasized, Castration-Resistant Prostate Cancer. Cancers. 2024; 16(5):886. https://doi.org/10.3390/cancers16050886
Chicago/Turabian StyleBarsegian, Vahé, Daniel Möckel, Sebastian Buehler, Stefan P. Müller, Michael C. Kreissl, Patrick Ostheim, Peter A. Horn, and Monika Lindemann. 2024. "Lymphocyte Function at Baseline Could Be a New Predictor of Tumor Burden following Six Cycles of Radium-223 Therapy in Patients with Metastasized, Castration-Resistant Prostate Cancer" Cancers 16, no. 5: 886. https://doi.org/10.3390/cancers16050886
APA StyleBarsegian, V., Möckel, D., Buehler, S., Müller, S. P., Kreissl, M. C., Ostheim, P., Horn, P. A., & Lindemann, M. (2024). Lymphocyte Function at Baseline Could Be a New Predictor of Tumor Burden following Six Cycles of Radium-223 Therapy in Patients with Metastasized, Castration-Resistant Prostate Cancer. Cancers, 16(5), 886. https://doi.org/10.3390/cancers16050886