
Real-World Data on Clinical Outcomes and Treatment Management of Advanced Melanoma Patients: Single-Center Study of a Tertiary Cancer Center in Switzerland

 , , , , , ,
, , , , , ,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
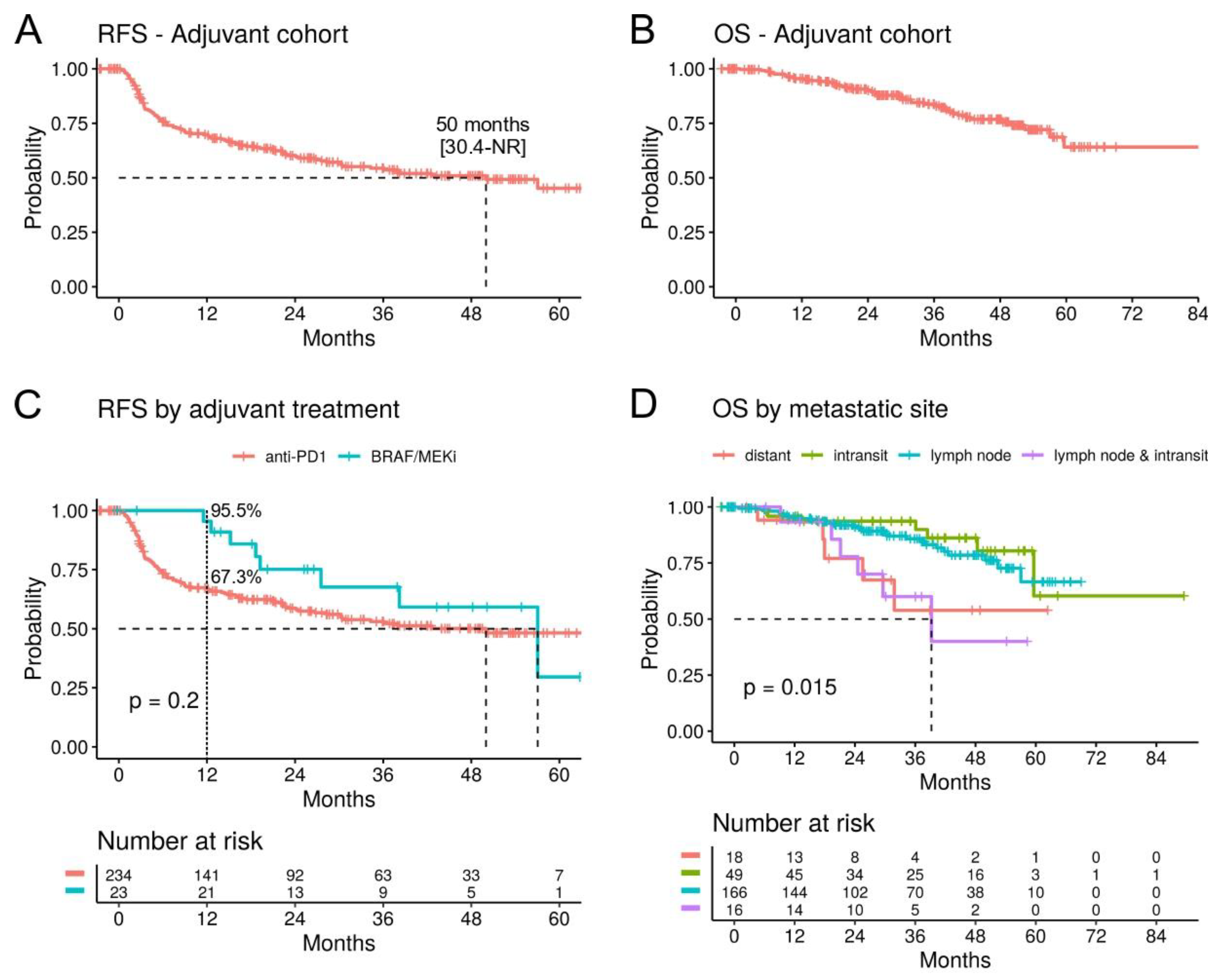
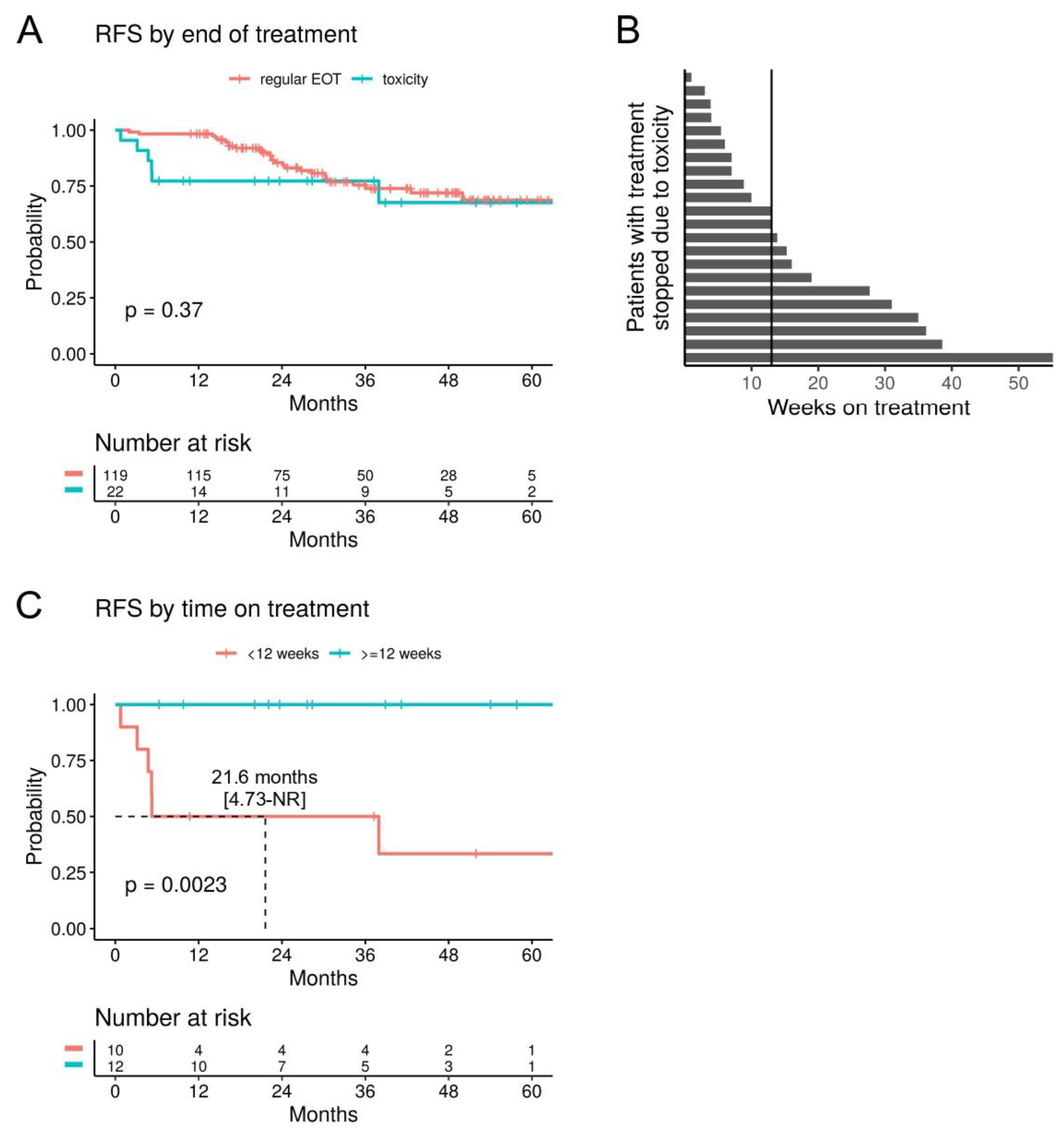
3.1. Resectable Setting: Adjuvant Treatment
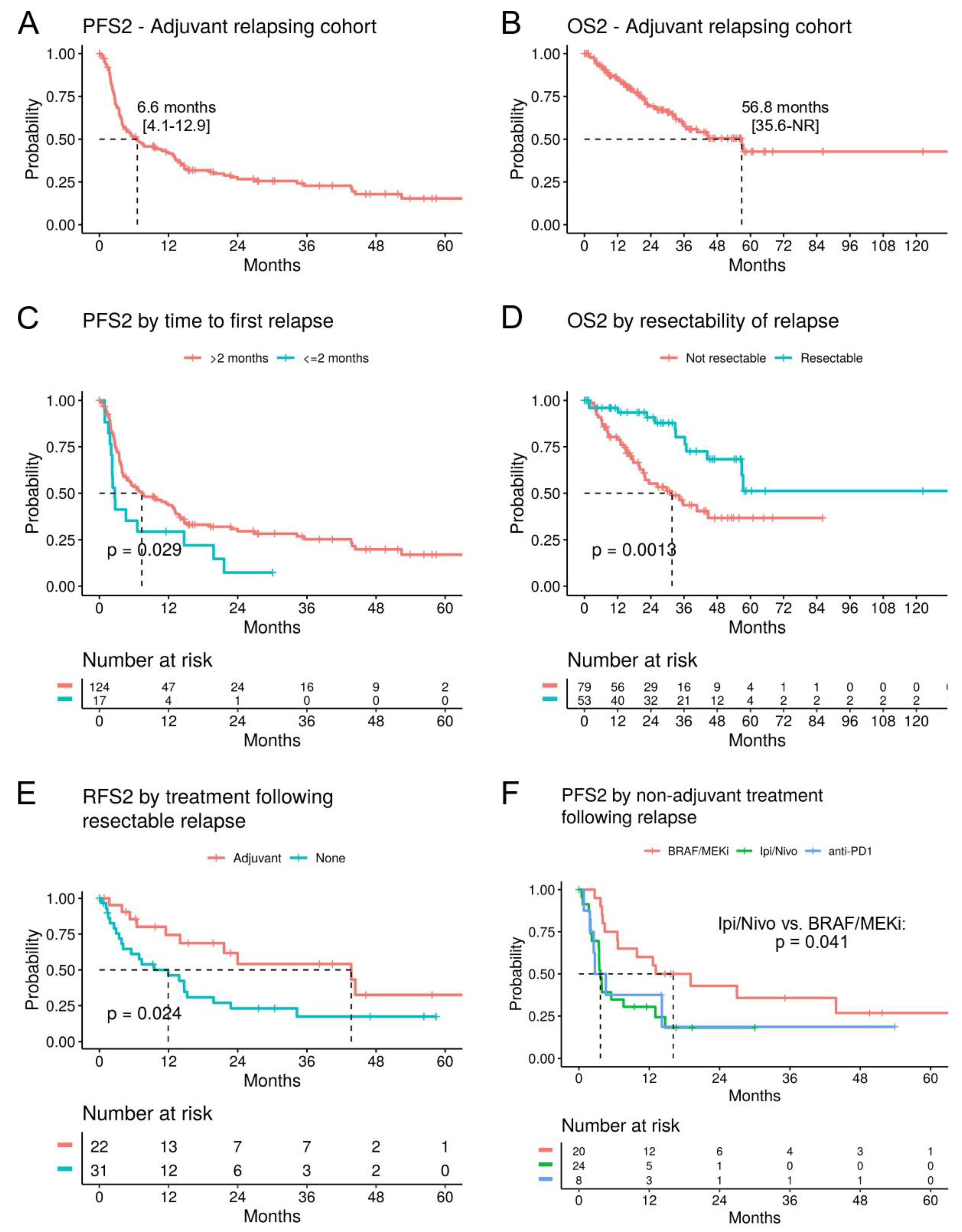
3.2. Relapsing Disease after Adjuvant Treatment
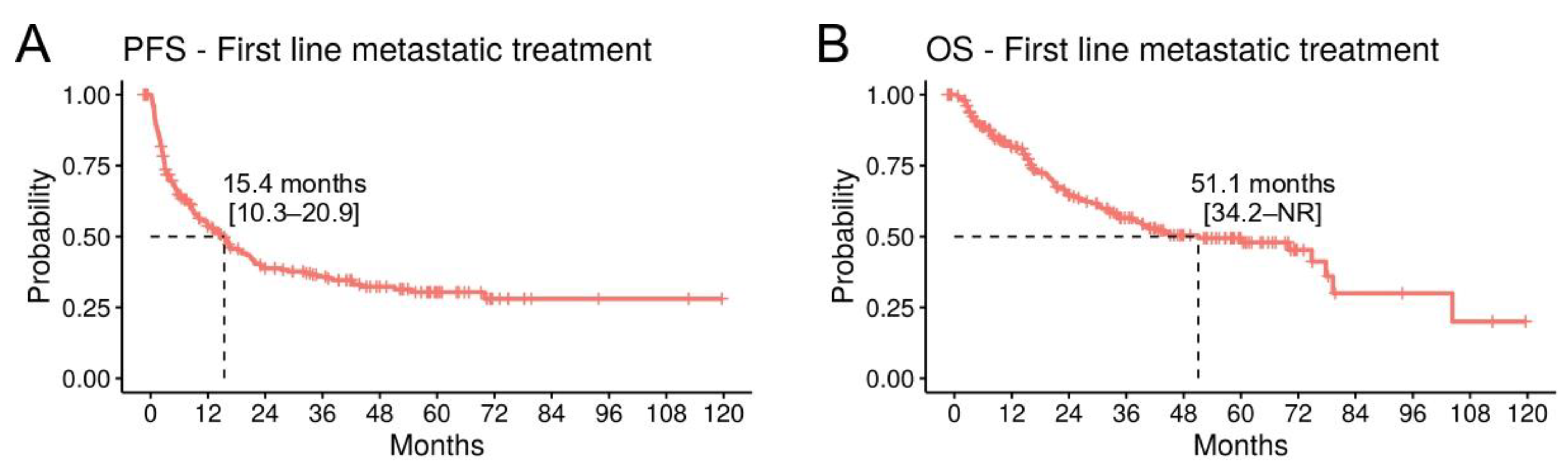
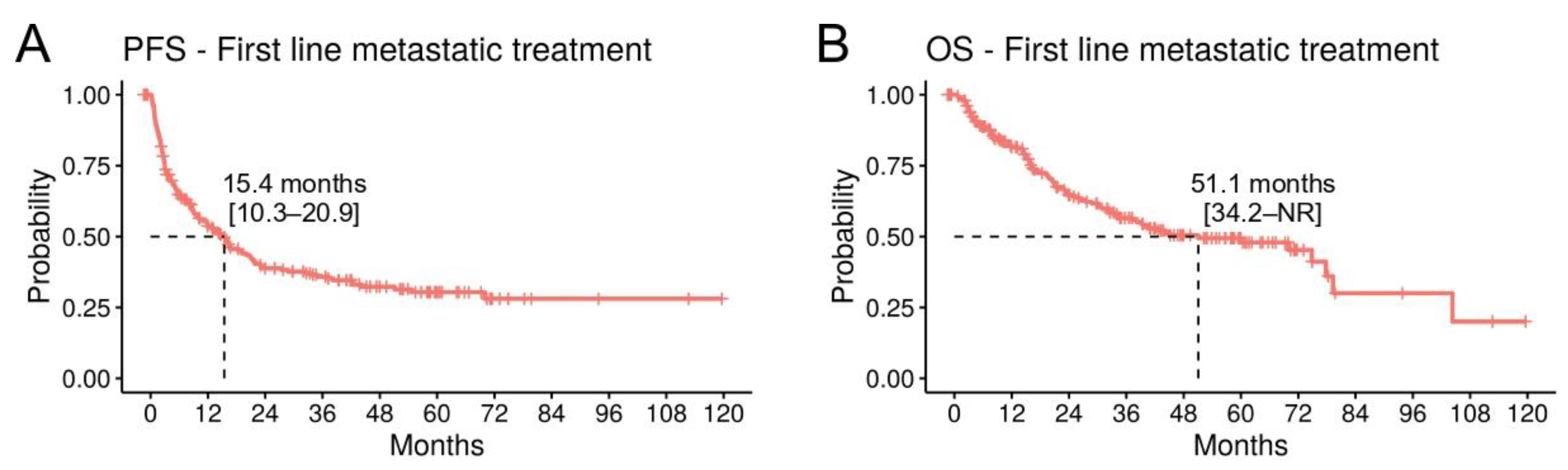
3.3. Unresectable Setting: First-Line Metastatic Treatment
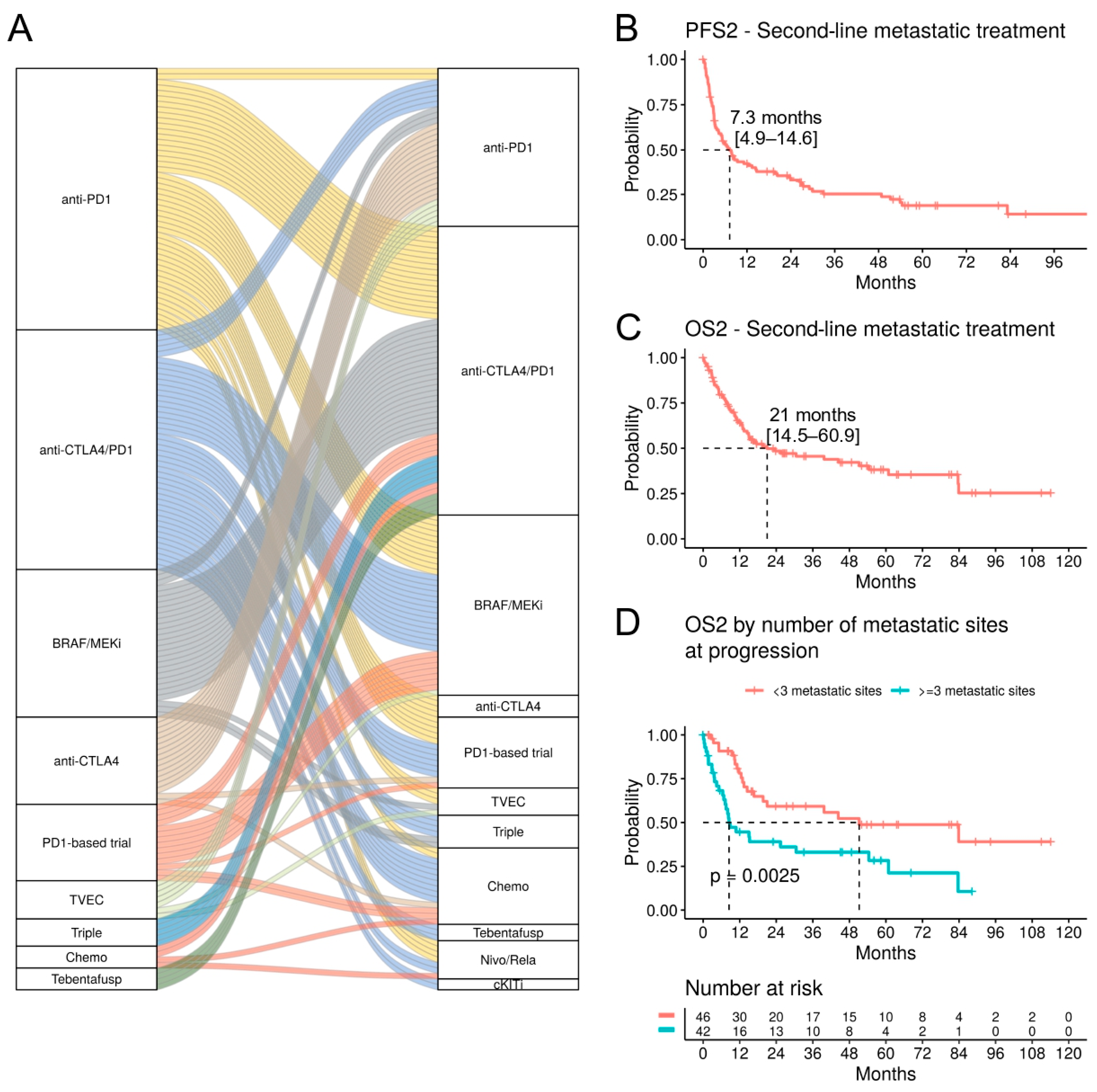
3.4. Unresectable Setting: Second-Line Metastatic Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 1L | First line |
| 2L | Second line |
| BRAF/MEKi | BRAF/MEK inhibitor |
| CI | Confidence interval |
| CTLA4 | Cytotoxic T-lymphocyte-associated protein 4 |
| HR | Hazard ratio |
| ICI | Immune checkpoint inhibitor |
| LAG3 | Lymphocyte activation gene 3 |
| MUP | Melanoma of unknown primary |
| NR | Not reached |
| OS | Overall survival |
| PD1 | Programmed cell death protein 1 |
| PFS | Progression-free survival |
| RFS | Relapse-free survival |
| TT | Targeted therapy |
References
- Ascierto, P.A.; Dreno, B.; Larkin, J.; Ribas, A.; Liszkay, G.; Maio, M.; Mandala, M.; Demidov, L.; Stroyakovskiy, D.; Thomas, L.; et al. 5-Year Outcomes with Cobimetinib plus Vemurafenib in BRAFV600 Mutation-Positive Advanced Melanoma: Extended Follow-up of the coBRIM Study. Clin. Cancer Res. 2021, 27, 5225–5235. [Google Scholar] [CrossRef]
- Dummer, R.; Ascierto, P.A.; Gogas, H.J.; Arance, A.; Mandala, M.; Liszkay, G.; Garbe, C.; Schadendorf, D.; Krajsova, I.; Gutzmer, R.; et al. Encorafenib plus binimetinib versus vemurafenib or encorafenib in patients with BRAF-mutant melanoma (COLUMBUS): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2018, 19, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Carolino, M.S.; Atkinson, V.; Cebon, J.; Jameson, M.; Fitzharris, B.; McNeil, C.; Hill, A.; Ribas, A.; Thompson, J.A.; et al. Early findings from the Keynote-029 study: Pembrolizumab + Low-Dose Ipilimumab for Advanced Melanoma. In Proceedings of the SMR Congress, San Francisco, CA, USA, 18–21 November 2015. [Google Scholar]
- Long, G.V.; Stroyakovskiy, D.; Gogas, H.; Levchenko, E.; de Braud, F.; Larkin, J.; Garbe, C.; Jouary, T.; Hauschild, A.; Grob, J.J.; et al. Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: A multicentre, double-blind, phase 3 randomised controlled trial. Lancet 2015, 386, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Grob, J.J.; Stroyakovskiy, D.; Karaszewska, B.; Hauschild, A.; Levchenko, E.; Chiarion Sileni, V.; Schachter, J.; Garbe, C.; Bondarenko, I.; et al. Five-Year Outcomes with Dabrafenib plus Trametinib in Metastatic Melanoma. N. Engl. J. Med. 2019, 381, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Ribas, A.; Schachter, J.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.M.; Lotem, M.; et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): Post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol. 2019, 20, 1239–1251. [Google Scholar] [CrossRef] [PubMed]
- Tawbi, H.A.; Schadendorf, D.; Lipson, E.J.; Ascierto, P.A.; Matamala, L.; Castillo Gutierrez, E.; Rutkowski, P.; Gogas, H.J.; Lao, C.D.; De Menezes, J.J.; et al. Relatlimab and Nivolumab versus Nivolumab in Untreated Advanced Melanoma. N. Engl. J. Med. 2022, 386, 24–34. [Google Scholar] [CrossRef]
- Weber, J.S.; D’Angelo, S.P.; Minor, D.; Hodi, F.S.; Gutzmer, R.; Neyns, B.; Hoeller, C.; Khushalani, N.I.; Miller, W.H., Jr.; Lao, C.D.; et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): A randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2015, 16, 375–384. [Google Scholar] [CrossRef]
- Eggermont, A.M.M.; Blank, C.U.; Mandala, M.; Long, G.V.; Atkinson, V.G.; Dalle, S.; Haydon, A.M.; Meshcheryakov, A.; Khattak, A.; Carlino, M.S.; et al. Adjuvant pembrolizumab versus placebo in resected stage III melanoma (EORTC 1325-MG/KEYNOTE-054): Distant metastasis-free survival results from a double-blind, randomised, controlled, phase 3 trial. Lancet Oncol. 2021, 22, 643–654. [Google Scholar] [CrossRef]
- Weber, J.; Mandala, M.; Del Vecchio, M.; Gogas, H.J.; Arance, A.M.; Cowey, C.L.; Dalle, S.; Schenker, M.; Chiarion-Sileni, V.; Marquez-Rodas, I.; et al. Adjuvant Nivolumab versus Ipilimumab in Resected Stage III or IV Melanoma. N. Engl. J. Med. 2017, 377, 1824–1835. [Google Scholar] [CrossRef]
- Long, G.V.; Luke, J.J.; Khattak, M.A.; de la Cruz Merino, L.; Del Vecchio, M.; Rutkowski, P.; Spagnolo, F.; Mackiewicz, J.; Chiarion-Sileni, V.; Kirkwood, J.M.; et al. Pembrolizumab versus placebo as adjuvant therapy in resected stage IIB or IIC melanoma (KEYNOTE-716): Distant metastasis-free survival results of a multicentre, double-blind, randomised, phase 3 trial. Lancet Oncol. 2022, 23, 1378–1388. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Hauschild, A.; Santinami, M.; Atkinson, V.; Mandala, M.; Chiarion-Sileni, V.; Larkin, J.; Nyakas, M.; Dutriaux, C.; Haydon, A.; et al. Adjuvant Dabrafenib plus Trametinib in Stage III BRAF-Mutated Melanoma. N. Engl. J. Med. 2017, 377, 1813–1823. [Google Scholar] [CrossRef] [PubMed]
- Kirkwood, J.M.; Del Vecchio, M.; Weber, J.; Hoeller, C.; Grob, J.J.; Mohr, P.; Loquai, C.; Dutriaux, C.; Chiarion-Sileni, V.; Mackiewicz, J.; et al. Adjuvant nivolumab in resected stage IIB/C melanoma: Primary results from the randomized, phase 3 CheckMate 76K trial. Nat. Med. 2023, 29, 2835–2843. [Google Scholar] [CrossRef] [PubMed]
- Eggermont, A.M.; Chiarion-Sileni, V.; Grob, J.J.; Dummer, R.; Wolchok, J.D.; Schmidt, H.; Hamid, O.; Robert, C.; Ascierto, P.A.; Richards, J.M.; et al. Adjuvant ipilimumab versus placebo after complete resection of high-risk stage III melanoma (EORTC 18071): A randomised, double-blind, phase 3 trial. Lancet Oncol. 2015, 16, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Casula, M.; Bulgarelli, J.; Pisano, M.; Piccinini, C.; Piccin, L.; Cossu, A.; Mandala, M.; Ferrucci, P.F.; Guidoboni, M.; et al. Sequential immunotherapy and targeted therapy for metastatic BRAF V600 mutated melanoma: 4-year survival and biomarkers evaluation from the phase II SECOMBIT trial. Nat. Commun. 2024, 15, 146. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Mandala, M.; Ferrucci, P.F.; Guidoboni, M.; Rutkowski, P.; Ferraresi, V.; Arance, A.; Guida, M.; Maiello, E.; Gogas, H.; et al. Sequencing of Ipilimumab Plus Nivolumab and Encorafenib Plus Binimetinib for Untreated BRAF-Mutated Metastatic Melanoma (SECOMBIT): A Randomized, Three-Arm, Open-Label Phase II Trial. J. Clin. Oncol. 2023, 41, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Atkins, M.B.; Lee, S.J.; Chmielowski, B.; Tarhini, A.A.; Cohen, G.I.; Truong, T.G.; Moon, H.H.; Davar, D.; O’Rourke, M.; Stephenson, J.J.; et al. Combination Dabrafenib and Trametinib Versus Combination Nivolumab and Ipilimumab for Patients with Advanced BRAF-Mutant Melanoma: The DREAMseq Trial-ECOG-ACRIN EA6134. J. Clin. Oncol. 2023, 41, 186–197. [Google Scholar] [CrossRef]
- Mangana, J.; Cheng, P.F.; Kaufmann, C.; Amann, V.C.; Frauchiger, A.L.; Stogner, V.; Held, U.; von Moos, R.; Michielin, O.; Braun, R.P.; et al. Multicenter, real-life experience with checkpoint inhibitors and targeted therapy agents in advanced melanoma patients in Switzerland. Melanoma Res. 2017, 27, 358–368. [Google Scholar] [CrossRef]
- Brunson, J.C.; Read, Q.D. ggalluvial: Alluvial Plots in ‘ggplot2’. 2023. Available online: https://corybrunson.github.io/ggalluvial (accessed on 30 January 2024).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Therneau, T.M. A Package for Survival Analysis in R. 2020. Available online: https://CRAN.R-project.org/package=survival (accessed on 30 January 2024).
- Kassambara, A.; Kosinski, M.; Biecek, P. Survminer: Drawing Survival Curves Using ‘ggplot2’. 2021. Available online: https://CRAN.R-project.org/package=survminer (accessed on 30 January 2024).
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef]
- Dummer, R.; Flaherty, K.T.; Robert, C.; Arance, A.; de Groot, J.W.B.; Garbe, C.; Gogas, H.J.; Gutzmer, R.; Krajsova, I.; Liszkay, G.; et al. COLUMBUS 5-Year Update: A Randomized, Open-Label, Phase III Trial of Encorafenib Plus Binimetinib Versus Vemurafenib or Encorafenib in Patients with BRAF V600-Mutant Melanoma. J. Clin. Oncol. 2022, 40, 4178–4188. [Google Scholar] [CrossRef]
- Long, G.V.; Grob, J.J.; Nathan, P.; Ribas, A.; Robert, C.; Schadendorf, D.; Lane, S.R.; Mak, C.; Legenne, P.; Flaherty, K.T.; et al. Factors predictive of response, disease progression, and overall survival after dabrafenib and trametinib combination treatment: A pooled analysis of individual patient data from randomised trials. Lancet Oncol. 2016, 17, 1743–1754. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Long-Term Outcomes with Nivolumab Plus Ipilimumab or Nivolumab Alone Versus Ipilimumab in Patients With Advanced Melanoma. J. Clin. Oncol. 2022, 40, 127–137. [Google Scholar] [CrossRef]
- Michielin, O.; van Akkooi, A.; Lorigan, P.; Ascierto, P.A.; Dummer, R.; Robert, C.; Arance, A.; Blank, C.U.; Chiarion Sileni, V.; Donia, M.; et al. ESMO consensus conference recommendations on the management of locoregional melanoma: Under the auspices of the ESMO Guidelines Committee. Ann. Oncol. 2020, 31, 1449–1461. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Del Vecchio, M.; Mandala, M.; Gogas, H.; Arance, A.M.; Dalle, S.; Cowey, C.L.; Schenker, M.; Grob, J.J.; Chiarion-Sileni, V.; et al. Adjuvant nivolumab versus ipilimumab in resected stage IIIB-C and stage IV melanoma (CheckMate 238): 4-year results from a multicentre, double-blind, randomised, controlled, phase 3 trial. Lancet Oncol. 2020, 21, 1465–1477. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, L.; Livingstone, E.; Hassel, J.C.; Fluck, M.; Eigentler, T.; Loquai, C.; Haferkamp, S.; Gutzmer, R.; Meier, F.; Mohr, P.; et al. Adjuvant nivolumab plus ipilimumab or nivolumab alone versus placebo in patients with resected stage IV melanoma with no evidence of disease (IMMUNED): Final results of a randomised, double-blind, phase 2 trial. Lancet 2022, 400, 1117–1129. [Google Scholar] [CrossRef]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Gogas, H.; Del Vecchio, M.; Maio, M.; Arenberger, P.; Arance, A.M.; Grob, J.-J.; Chiarion-Sileni, V.; Lewis, K.D.; Mortier, L.; et al. Analysis of patients (pts) with in-transit metastases treated with nivolumab (NIVO) or ipilimumab (IPI) in CheckMate 238. J. Clin. Oncol. 2021, 39, 9569. [Google Scholar] [CrossRef]
- Rigo, R.; Ding, P.Q.; Batuyong, E.; Cheung, W.Y.; Walker, J.; Monzon, J.G.; Cheng, T. Adjuvant Systemic Therapies for Resected Stages III and IV Melanoma: A Multi-Center Retrospective Clinical Study. Oncologist 2024, 29, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Schumann, K.; Mauch, C.; Klespe, K.C.; Loquai, C.; Nikfarjam, U.; Schlaak, M.; Akcetin, L.; Kolblinger, P.; Hoellwerth, M.; Meissner, M.; et al. Real-world outcomes using PD-1 antibodies and BRAF + MEK inhibitors for adjuvant melanoma treatment from 39 skin cancer centers in Germany, Austria and Switzerland. J. Eur. Acad. Dermatol. Venereol. 2023, 37, 894–906. [Google Scholar] [CrossRef]
- Dimitriou, F.; Staeger, R.; Ak, M.; Maissen, M.; Kudura, K.; Barysch, M.J.; Levesque, M.P.; Cheng, P.F.; Dummer, R.; Mangana, J. Frequency, Treatment and Outcome of Immune-Related Toxicities in Patients with Immune-Checkpoint Inhibitors for Advanced Melanoma: Results from an Institutional Database Analysis. Cancers 2021, 13, 2931. [Google Scholar] [CrossRef]
- Owen, C.N.; Shoushtari, A.N.; Chauhan, D.; Palmieri, D.J.; Lee, B.; Rohaan, M.W.; Mangana, J.; Atkinson, V.; Zaman, F.; Young, A.; et al. Management of early melanoma recurrence despite adjuvant anti-PD-1 antibody therapy. Ann. Oncol. 2020, 31, 1075–1082. [Google Scholar] [CrossRef]
- Taylor, A.M.; Galea, C.; Lo, S.N.; Dimitriou, F.; Jacques, S.; Allayous, C.; Yeoh, H.-L.; Ressler, J.M.; Kahler, K.C.; Festino, L.; et al. Efficacy and safety of "second adjuvant" therapy with BRAF/MEK inhibitors after resection of recurrent melanoma following adjuvant PD-1–based immunotherapy. J. Clin. Oncol. 2022, 40, 9575. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 331) | Cutaneous Melanoma (n= 301) | Melanoma of Unknown Primary (n = 24) | Mucosal Melanoma (n = 6) | |
|---|---|---|---|---|
| Age | ||||
| Median [Min, Max] | 62.0 [15.0, 87.0] | 61.0 [15.0, 87.0] | 67.5 [17.0, 79.0] | 69.0 [33.0, 79.0] |
| Sex | ||||
| f | 130 (39.3%) | 120 (39.9%) | 6 (25.0%) | 4 (66.7%) |
| m | 201 (60.7%) | 181 (60.1%) | 18 (75.0%) | 2 (33.3%) |
| BRAF mutation | ||||
| V600 | 141 (42.6%) | 131 (43.5%) | 9 (37.5%) | 1 (16.7%) |
| non-V600 | 18 (5.4%) | 17 (5.6%) | 1 (4.2%) | 0 (0%) |
| wildtype | 131 (39.6%) | 115 (38.2%) | 13 (54.2%) | 3 (50.0%) |
| unknown | 41 (12.4%) | 38 (12.6%) | 1 (4.2%) | 2 (33.3%) |
| Stage | ||||
| Stage 1b | 2 (0.6%) | 0 (0%) | 0 (0%) | 2 (33.3%) |
| Stage 2a | 1 (0.3%) | 1 (0.3%) | 0 (0%) | 0 (0%) |
| Stage 2b | 6 (1.8%) | 6 (2.0%) | 0 (0%) | 0 (0%) |
| Stage 2c | 7 (2.1%) | 6 (2.0%) | 0 (0%) | 1 (16.7%) |
| Stage 3a | 28 (8.5%) | 27 (9.0%) | 0 (0%) | 1 (16.7%) |
| Stage 3b | 118 (35.6%) | 110 (36.5%) | 8 (33.3%) | 0 (0%) |
| Stage 3c | 138 (41.7%) | 124 (41.2%) | 13 (54.2%) | 1 (16.7%) |
| Stage 3d | 8 (2.4%) | 8 (2.7%) | 0 (0%) | 0 (0%) |
| Stage 4 | 23 (6.9%) | 19 (6.3%) | 3 (12.5%) | 1 (16.7%) |
| Metastatic sites | ||||
| distant | 21 (6.3%) | 18 (6.0%) | 3 (12.5%) | 0 (0%) |
| In transit | 64 (19.3%) | 61 (20.3%) | 3 (12.5%) | 0 (0%) |
| lymph node | 210 (63.4%) | 194 (64.5%) | 14 (58.3%) | 2 (33.3%) |
| lymph node & in transit | 19 (5.7%) | 15 (5.0%) | 4 (16.7%) | 0 (0%) |
| Missing | 17 (5.1%) | 13 (4.3%) | 0 (0%) | 4 (66.7%) |
| Adjuvant treatment | ||||
| anti-PD1 | 248 (74.9%) | 229 (76.1%) | 16 (66.7%) | 3 (50.0%) |
| Clinical trial | 28 (8.5%) | 26 (8.6%) | 2 (8.3%) | 0 (0%) |
| BRAF/MEKi | 24 (7.3%) | 21 (7.0%) | 3 (12.5%) | 0 (0%) |
| anti-CTLA4 | 23 (6.9%) | 20 (6.6%) | 3 (12.5%) | 0 (0%) |
| anti-CTLA4/PD1 | 8 (2.4%) | 5 (1.7%) | 0 (0%) | 3 (50.0%) |
| End of Treatment reason | ||||
| regular | 151 (45.6%) | 137 (45.5%) | 11 (45.8%) | 3 (50.0%) |
| progression | 79 (23.9%) | 72 (23.9%) | 6 (25.0%) | 1 (16.7%) |
| toxicity | 36 (10.9%) | 30 (10.0%) | 5 (20.8%) | 1 (16.7%) |
| other | 18 (5.4%) | 17 (5.6%) | 0 (0%) | 1 (16.7%) |
| Missing | 47 (14.2%) | 45 (15.0%) | 2 (8.3%) | 0 (0%) |
| Adjuvant Treatment | ||
|---|---|---|
| Anti-PD1 (n = 234) | BRAF/MEKi (n = 23) | |
| Median RFS (95% CI) | 50 months (28.3-NR) | 57 months (27.5-NR) |
| HR 0.63 (0.30–1.29), p = 0.2 | ||
| 1-year RFS (95% CI) | 67.3% (61.4–73.7) | 95.5% (87.1–100) |
| 3-year RFS (95% CI) | 53.0% (46.4–60.6) | 67.6% (48.8–93.8) |
| Median OS (95% CI) | NR (NR-NR) | 57 (57-NR) |
| HR 1.10 (0.43–2.79), p = 0.84 | ||
| 1-year OS (95% CI) | 95.0% (92.2–98.0) | 100% (100–100) |
| 3-year OS (95% CI) | 83.2% (77.7–89.0) | 89.1% (75.8–100) |
| Total (n = 143) | |
|---|---|
| Age | |
| Median [Min, Max] | 60.0 [17.0, 88.0] |
| Sex | |
| f | 53 (37.1%) |
| m | 90 (62.9%) |
| Type | |
| Cutaneous | 130 (90.9%) |
| Unknown primary | 11 (7.7%) |
| Mucosal | 2 (1.4%) |
| BRAF mutation | |
| V600 | 79 (55.2%) |
| non-V600 | 9 (6.3%) |
| wildtype | 55 (38.5%) |
| unknown | 0 (0%) |
| Time until relapse | |
| <3 months | 39 (27.3%) |
| 3–12 months | 53 (37.1%) |
| >12 months | 51 (35.7%) |
| Resectable relapse | |
| Unresectable | 81 (56.6%) |
| Resectable | 53 (37.1%) |
| Missing | 9 (6.3%) |
| Subsequent systemic treatment | |
| Adjuvant | 22 (15.4%) |
| Non-adjuvant | 74 (51.7%) |
| None | 47 (32.9%) |
| Clinical stage at relapse | |
| Stage 3b | 15 (10.5%) |
| Stage 3c | 50 (35.0%) |
| Stage 3d | 3 (2.1%) |
| Stage 4 | 75 (52.4%) |
| Site of relapse | |
| distant | 73 (51.0%) |
| In transit | 33 (23.1%) |
| lymph node | 26 (18.2%) |
| lymph node & in transit | 11 (7.7%) |
| Locoregional metastatic sites | |
| Mean (SD) | 1.16 (0.373) |
| Median [Min, Max] | 1.00 [1.00, 2.00] |
| Distant metastatic sites | |
| Mean (SD) | 1.64 (0.948) |
| Median [Min, Max] | 1.00 [1.00, 5.00] |
| LDH levels | |
| normal | 87 (60.8%) |
| elevated | 6 (4.2%) |
| Missing | 50 (35.0%) |
| 2nd adjuvant treatment | |
| BRAF/MEKi | 15 (10.5%) |
| anti-PD1 | 7 (4.9%) |
| 1L metastatic treatment | |
| Ipi/Nivo | 25 (17.5%) |
| BRAF/MEKi | 20 (14.0%) |
| Clinical trial | 14 (9.8%) |
| anti-PD1 | 8 (5.6%) |
| anti-CTLA4 | 4 (2.8%) |
| MEKi | 1 (0.7%) |
| TVEC | 1 (0.7%) |
| Total (n = 375) | Cutaneous Melanoma (n = 271) | Melanoma of Unknown Primary (n = 45) | Uveal Melanoma (n = 34) | Mucosal Melanoma (n = 25) | |
|---|---|---|---|---|---|
| Age | |||||
| Median [Min, Max] | 67.0 [27.0, 95.0] | 69.0 [30.0, 95.0] | 61.5 [27.0, 90.0] | 62.0 [37.0, 80.0] | 71.0 [40.0, 90.0] |
| Sex | |||||
| f | 137 (36.5%) | 101 (37.3%) | 12 (26.7%) | 10 (29.4%) | 14 (56.0%) |
| m | 238 (63.5%) | 170 (62.7%) | 33 (73.3%) | 24 (70.6%) | 11 (44.0%) |
| BRAF mutation | |||||
| V600 | 127 (33.9%) | 112 (41.3%) | 13 (28.9%) | 0 (0%) | 2 (8.0%) |
| non-V600 | 25 (6.7%) | 19 (7.0%) | 3 (6.7%) | 1 (2.9%) | 2 (8.0%) |
| wildtype | 220 (58.7%) | 137 (50.6%) | 29 (64.4%) | 33 (97.1%) | 21 (84.0%) |
| unknown | 3 (0.8%) | 3 (1.1%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Stage | |||||
| Stage 2 | 1 (0.3%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (4.0%) |
| Stage 3 | 65 (17.3%) | 54 (19.9%) | 6 (13.3%) | 0 (0%) | 5 (20.0%) |
| Stage 4 | 308 (82.1%) | 216 (79.7%) | 39 (86.7%) | 34 (100%) | 19 (76.0%) |
| Missing | 1 (0.3%) | 1 (0.4%) | 0 (0%) | 0 (0%) | 0 (0%) |
| LDH levels | |||||
| elevated | 69 (18.4%) | 49 (18.1%) | 6 (13.3%) | 11 (32.4%) | 3 (12.0%) |
| normal | 255 (68.0%) | 186 (68.6%) | 31 (68.9%) | 19 (55.9%) | 19 (76.0%) |
| Missing | 51 (13.6%) | 36 (13.3%) | 8 (17.8%) | 4 (11.8%) | 3 (12.0%) |
| Distant metastatic sites | |||||
| Median [Min, Max] | 2.00 [1.00, 14.0] | 2.00 [1.00, 14.0] | 2.00 [1.00, 12.0] | 1.00 [1.00, 8.00] | 2.00 [1.00, 4.00] |
| Lung metastasis | |||||
| no | 215 (57.3%) | 146 (53.9%) | 27 (60.0%) | 26 (76.5%) | 16 (64.0%) |
| yes | 160 (42.7%) | 125 (46.1%) | 18 (40.0%) | 8 (23.5%) | 9 (36.0%) |
| Liver metastasis | |||||
| no | 276 (73.6%) | 214 (79.0%) | 40 (88.9%) | 1 (2.9%) | 21 (84.0%) |
| yes | 99 (26.4%) | 57 (21.0%) | 5 (11.1%) | 33 (97.1%) | 4 (16.0%) |
| Brain metastasis | |||||
| no | 298 (79.5%) | 213 (78.6%) | 29 (64.4%) | 32 (94.1%) | 24 (96.0%) |
| yes | 77 (20.5%) | 58 (21.4%) | 16 (35.6%) | 2 (5.9%) | 1 (4.0%) |
| Bone metastasis | |||||
| no | 299 (79.7%) | 213 (78.6%) | 37 (82.2%) | 26 (76.5%) | 23 (92.0%) |
| yes | 76 (20.3%) | 58 (21.4%) | 8 (17.8%) | 8 (23.5%) | 2 (8.0%) |
| Treatment | |||||
| anti-PD1 | 128 (34.1%) | 100 (36.9%) | 17 (37.8%) | 3 (8.8%) | 8 (32.0%) |
| anti-CTLA4/PD1 | 117 (31.2%) | 69 (25.5%) | 15 (33.3%) | 19 (55.9%) | 14 (56.0%) |
| BRAF/MEKi | 42 (11.2%) | 34 (12.5%) | 7 (15.6%) | 0 (0%) | 1 (4.0%) |
| PD1-based trial | 33 (8.8%) | 28 (10.3%) | 5 (11.1%) | 0 (0%) | 0 (0%) |
| anti-CTLA4 | 20 (5.3%) | 19 (7.0%) | 0 (0%) | 0 (0%) | 1 (4.0%) |
| TVEC | 11 (2.9%) | 11 (4.1%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Tebentafusp | 10 (2.7%) | 0 (0%) | 0 (0%) | 10 (29.4%) | 0 (0%) |
| Triple | 9 (2.4%) | 8 (3.0%) | 1 (2.2%) | 0 (0%) | 0 (0%) |
| Chemo | 5 (1.3%) | 2 (0.7%) | 0 (0%) | 2 (5.9%) | 1 (4.0%) |
| Non-Adjuvant Treatment | |||
|---|---|---|---|
| Anti-PD1 (n = 113) | Anti-CTLA4/PD1 (n = 82) | BRAF/MEKi (n = 40) | |
| Median PFS (95% CI) | 11.8 months (8.7–21.0) | 13.5 months (5.8–35.0) | 18.3 months (15.8-NR) |
| HR 0.97 (0.68–1.4), p = 0.88 | HR 0.80 (0.51–1.27), p = 0.35 | ||
| 1-year PFS (95% CI) | 49.6% (41.0–60.0) | 52.6% (42.7–64.9) | 66.9% (53.7–83.4) |
| 3-year PFS (95% CI) | 34.1% (25.9–44.9) | 36.6% (27.1–49.5) | 40.1% (26.8–60.1) |
| 5-year PFS (95% CI) | 32.2% (23.9–43.4) | 30.2% (20.7–43.9%) | 29.7% (17.5–50.5) |
| Median OS (95% CI) | 39.6 months (27.5-NR) | NR (38.1-NR) | 42.4 (20.9-NR) |
| HR 0.76 (0.48–1.20), p = 0.24 | HR 0.93 (0.55–1.59), p = 0.8 | ||
| 1-year OS (95% CI) | 81.8% (74.7–89.6) | 84.8% (77.2–93.1) | 73.9% (61.289.3) |
| 3-year OS (95% CI) | 52.1% (42.2–64.4) | 61.9% (51.4–74.5) | 55.8% (41.5–74.9) |
| 5-year OS (95% CI) | 46.5% (36.3–59.6) | 52.4% (40.9–67.3) | 49.2% (34.9–69.3) |
| Total (n = 169) | Cutaneous Melanoma (n = 123) | Uveal Melanoma (n = 18) | Melanoma of Unknown Primary (n = 17) | Mucosal Melanoma (n = 11) | |
|---|---|---|---|---|---|
| Age | |||||
| Median [Min, Max] | 65.0 [30.0, 91.0] | 65.0 [31.0, 91.0] | 61.0 [40.0, 74.0] | 59.0 [30.0, 88.0] | 69.0 [43.0, 77.0] |
| Sex | |||||
| f | 61 (36.1%) | 46 (37.4%) | 7 (38.9%) | 3 (17.6%) | 5 (45.5%) |
| m | 108 (63.9%) | 77 (62.6%) | 11 (61.1%) | 14 (82.4%) | 6 (54.5%) |
| BRAF mutation | |||||
| V600 | 71 (42.0%) | 63 (51.2%) | 0 (0%) | 6 (35.3%) | 2 (18.2%) |
| non-V600 | 13 (7.7%) | 9 (7.3%) | 1 (5.6%) | 1 (5.9%) | 2 (18.2%) |
| wildtype | 85 (50.3%) | 51 (41.5%) | 17 (94.4%) | 10 (58.8%) | 7 (63.6%) |
| unknown | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Stage | |||||
| Stage 3 | 19 (11.2%) | 16 (13.0%) | 0 (0%) | 3 (17.6%) | 0 (0%) |
| Stage 4 | 150 (88.8%) | 107 (87.0%) | 18 (100%) | 14 (82.4%) | 11 (100%) |
| LDH levels | |||||
| elevated | 58 (34.3%) | 41 (33.3%) | 9 (50.0%) | 5 (29.4%) | 3 (27.3%) |
| normal | 97 (57.4%) | 75 (61.0%) | 8 (44.4%) | 8 (47.1%) | 6 (54.5%) |
| Missing | 14 (8.3%) | 7 (5.7%) | 1 (5.6%) | 4 (23.5%) | 2 (18.2%) |
| Distant metastatic sites | |||||
| Median [Min, Max] | 2.00 [1.00, 12.0] | 2.50 [1.00, 12.0] | 2.00 [1.00, 7.00] | 2.00 [1.00, 12.0] | 3.00 [1.00, 5.00] |
| Lung metastasis | |||||
| no | 94 (55.6%) | 64 (52.0%) | 13 (72.2%) | 12 (70.6%) | 5 (45.5%) |
| yes | 75 (44.4%) | 59 (48.0%) | 5 (27.8%) | 5 (29.4%) | 6 (54.5%) |
| Liver metastasis | |||||
| no | 109 (64.5%) | 90 (73.2%) | 0 (0%) | 14 (82.4%) | 5 (45.5%) |
| yes | 60 (35.5%) | 33 (26.8%) | 18 (100%) | 3 (17.6%) | 6 (54.5%) |
| Bone metastasis | |||||
| no | 121 (71.6%) | 88 (71.5%) | 14 (77.8%) | 13 (76.5%) | 6 (54.5%) |
| yes | 48 (28.4%) | 35 (28.5%) | 4 (22.2%) | 4 (23.5%) | 5 (45.5%) |
| Brain metastasis | |||||
| no | 125 (74.0%) | 82 (66.7%) | 18 (100%) | 15 (88.2%) | 10 (90.9%) |
| yes | 44 (26.0%) | 41 (33.3%) | 0 (0%) | 2 (11.8%) | 1 (9.1%) |
| 2L treatment | |||||
| anti-CTLA4/PD1 | 53 (31.4%) | 33 (26.8%) | 7 (38.9%) | 7 (41.2%) | 6 (54.5%) |
| BRAF/MEKi | 33 (19.5%) | 31 (25.2%) | 0 (0%) | 2 (11.8%) | 0 (0%) |
| anti-PD1 | 29 (17.2%) | 28 (22.8%) | 0 (0%) | 1 (5.9%) | 0 (0%) |
| Chemo | 14 (8.3%) | 2 (1.6%) | 7 (38.9%) | 2 (11.8%) | 3 (27.3%) |
| PD1-based trial | 13 (7.7%) | 10 (8.1%) | 1 (5.6%) | 2 (11.8%) | 0 (0%) |
| Nivo/Rela | 7 (4.1%) | 5 (4.1%) | 0 (0%) | 1 (5.9%) | 1 (9.1%) |
| Triple | 6 (3.6%) | 6 (4.9%) | 0 (0%) | 0 (0%) | 0 (0%) |
| TVEC | 5 (3.0%) | 4 (3.3%) | 0 (0%) | 1 (5.9%) | 0 (0%) |
| anti-CTLA4 | 4 (2.4%) | 3 (2.4%) | 0 (0%) | 1 (5.9%) | 0 (0%) |
| Tebentafusp | 3 (1.8%) | 0 (0%) | 3 (16.7%) | 0 (0%) | 0 (0%) |
| cKITi | 2 (1.2%) | 1 (0.8%) | 0 (0%) | 0 (0%) | 1 (9.1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Staeger, R.; Martínez-Gómez, J.M.; Turko, P.; Ramelyte, E.; Kraehenbuehl, L.; Del Prete, V.; Hasan Ali, O.; Levesque, M.P.; Dummer, R.; Nägeli, M.C.; et al. Real-World Data on Clinical Outcomes and Treatment Management of Advanced Melanoma Patients: Single-Center Study of a Tertiary Cancer Center in Switzerland. Cancers 2024, 16, 854. https://doi.org/10.3390/cancers16050854
Staeger R, Martínez-Gómez JM, Turko P, Ramelyte E, Kraehenbuehl L, Del Prete V, Hasan Ali O, Levesque MP, Dummer R, Nägeli MC, et al. Real-World Data on Clinical Outcomes and Treatment Management of Advanced Melanoma Patients: Single-Center Study of a Tertiary Cancer Center in Switzerland. Cancers. 2024; 16(5):854. https://doi.org/10.3390/cancers16050854
Chicago/Turabian StyleStaeger, Ramon, Julia M. Martínez-Gómez, Patrick Turko, Egle Ramelyte, Lukas Kraehenbuehl, Valerio Del Prete, Omar Hasan Ali, Mitchell P. Levesque, Reinhard Dummer, Mirjam C. Nägeli, and et al. 2024. "Real-World Data on Clinical Outcomes and Treatment Management of Advanced Melanoma Patients: Single-Center Study of a Tertiary Cancer Center in Switzerland" Cancers 16, no. 5: 854. https://doi.org/10.3390/cancers16050854
APA StyleStaeger, R., Martínez-Gómez, J. M., Turko, P., Ramelyte, E., Kraehenbuehl, L., Del Prete, V., Hasan Ali, O., Levesque, M. P., Dummer, R., Nägeli, M. C., & Mangana, J. (2024). Real-World Data on Clinical Outcomes and Treatment Management of Advanced Melanoma Patients: Single-Center Study of a Tertiary Cancer Center in Switzerland. Cancers, 16(5), 854. https://doi.org/10.3390/cancers16050854