
Prognostic Value of Inflammatory Burden Index in Advanced Gastric Cancer Patients Undergoing Multimodal Treatment

 , ,
, ,  , , , , , ,
, , , , , ,  ,
,  and
and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
2.2. Neoadjuvant Chemotherapy
2.3. Inflammatory Response Markers
2.4. Textbook Outcome
2.5. Tumor Regression Grade
2.6. Endpoints of the Study
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Comparison of IBI Depending on Selected Demographic and Clinical Variables
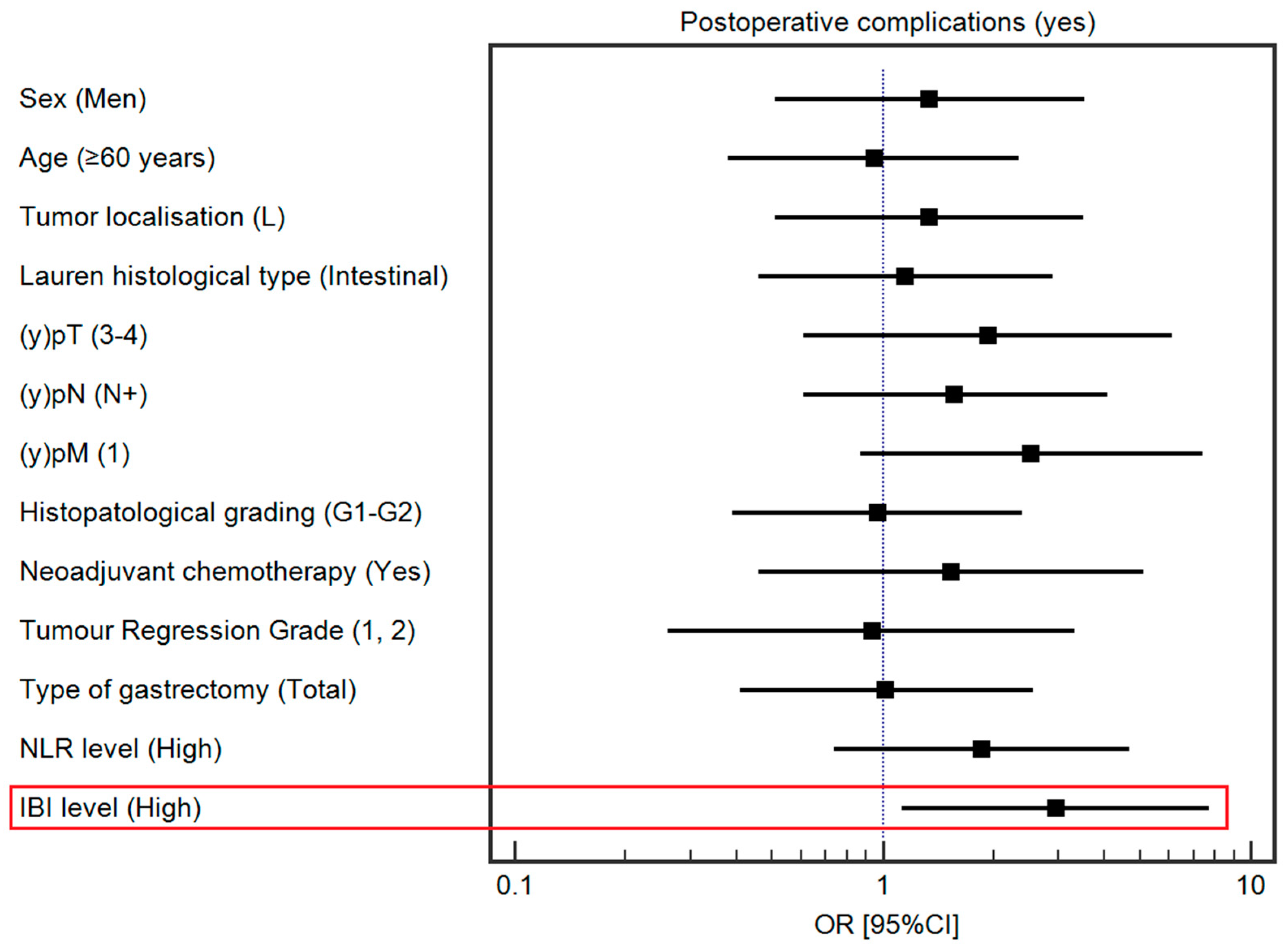
3.3. Influence of Selected Demographic and Clinical Variables on the Postoperative Complications
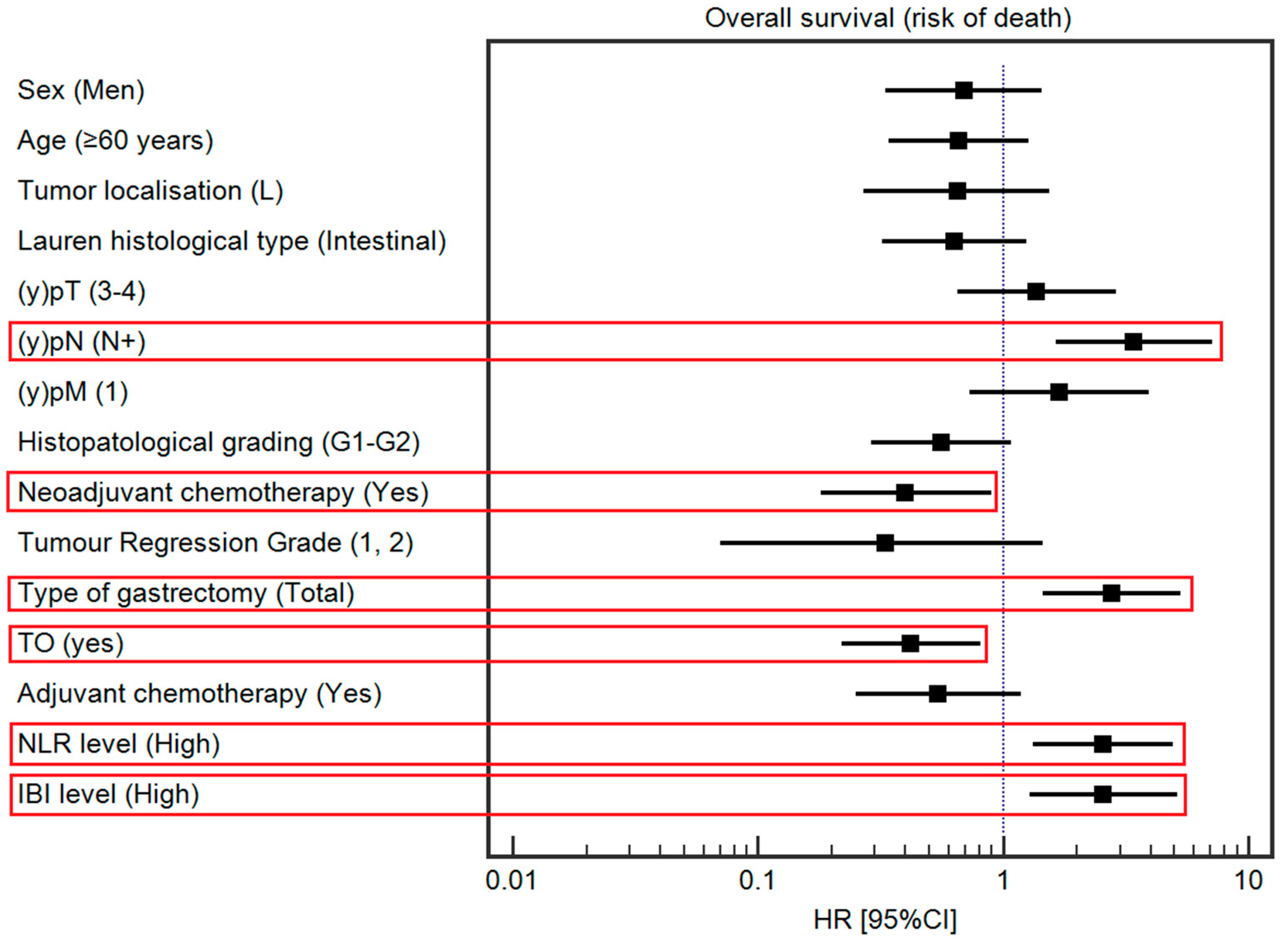
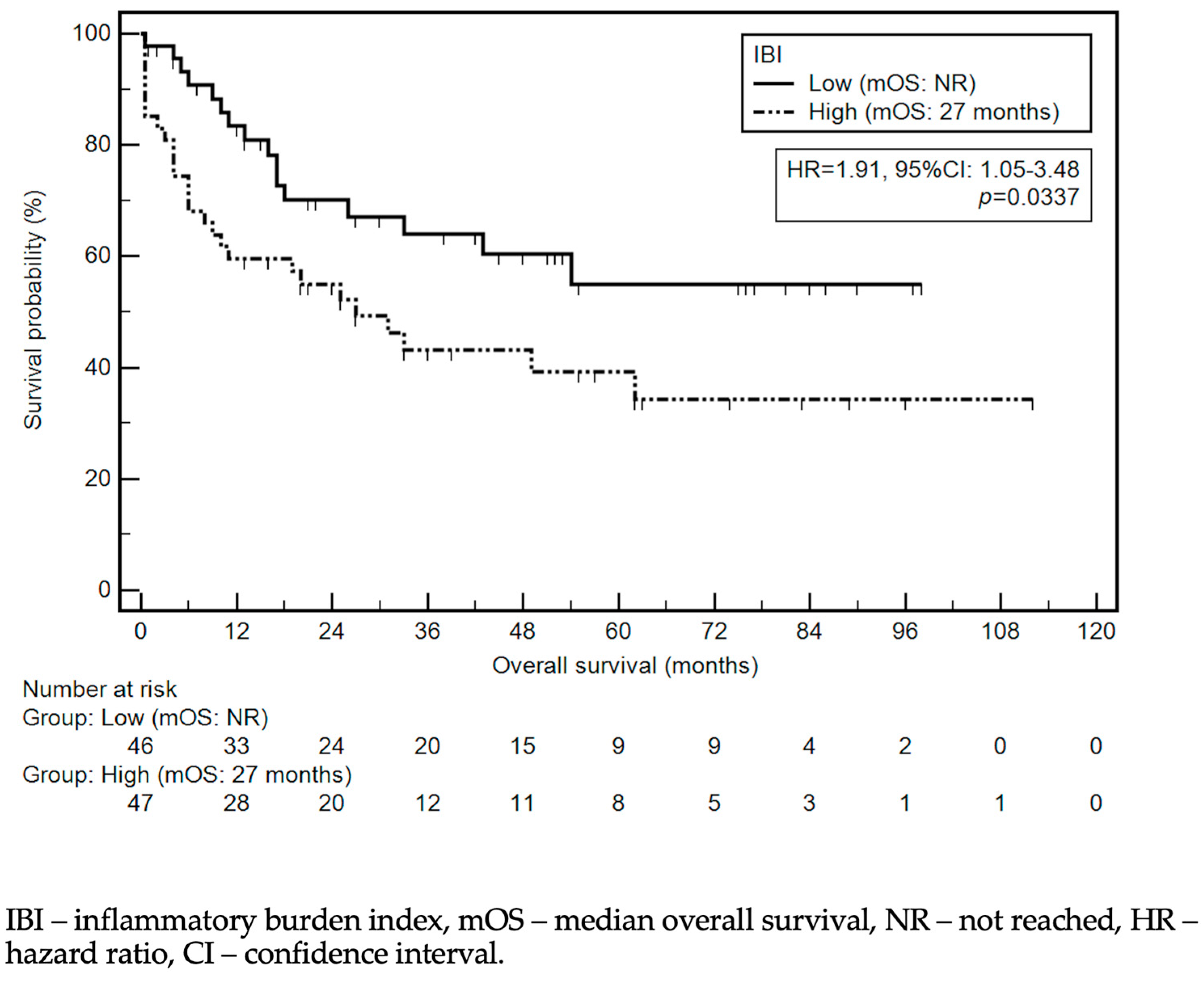
3.4. Influence of Selected Demographic and Clinical Variables on Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Etemadi, A.; Safiri, S.; Sepanlou, S.G.; Ikuta, K.; Bisignano, C.; Shakeri, R.; Amani, M.; Fitzmaurice, C.; Nixon, M.; Abbasi, N.; et al. The global, regional, and national burden of stomach cancer in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 42–54. [Google Scholar] [CrossRef] [PubMed]
- Lordick, F.; Carneiro, F.; Cascinu, S.; Fleitas, T.; Haustermans, K.; Piessen, G.; Vogel, A.; Smyth, E.C.; ESMO Guidelines Committee. Gastric cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 1005–1020. [Google Scholar] [CrossRef] [PubMed]
- Ajani, J.A.; D’Amico, T.A.; Bentrem, D.J.; Chao, J.; Cooke, D.; Corvera, C.; Das, P.; Enzinger, P.C.; Enzler, T.; Fanta, P.; et al. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2023, 20, 167–192. [Google Scholar] [CrossRef] [PubMed]
- Japanese Gastric Cancer Association. Japanese Gastric Cancer Treatment Guidelines 2021 (6th edition). Gastric Cancer 2023, 26, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Smyth, E.C.; Nilsson, M.; Grabsch, H.I.; van Grieken, N.C.; Lordick, F. Gastric cancer. Lancet 2020, 396, 635–648. [Google Scholar] [CrossRef]
- Crusz, S.M.; Balkwill, F.R. Inflammation and cancer: Advances and new agents. Nat. Rev. Clin. Oncol. 2015, 12, 584–596. [Google Scholar] [CrossRef]
- Xu, Z.; Xu, W.; Cheng, H.; Shen, W.; Ying, J.; Cheng, F.; Xu, W. The Prognostic Role of the Platelet-Lymphocytes Ratio in Gastric Cancer: A Meta-Analysis. PLoS ONE 2016, 11, e0163719. [Google Scholar] [CrossRef]
- Jiang, X.; Hiki, N.; Nunobe, S.; Kumagai, K.; Kubota, T.; Aikou, S.; Sano, T.; Yamaguchi, T. Prognostic importance of the inflammation-based Glasgow prognostic score in patients with gastric cancer. Br. J. Cancer 2012, 107, 275–279. [Google Scholar] [CrossRef]
- Yin, X.; Fang, T.; Wang, Y.; Wang, Y.; Zhang, D.; Li, C.; Xue, Y. Prognostic significance of serum inflammation indexes in different Lauren classification of gastric cancer. Cancer Med. 2021, 10, 1103–1119. [Google Scholar] [CrossRef]
- Hirahara, N.; Matsubara, T.; Kaji, S.; Hayashi, H.; Sasaki, Y.; Kawakami, K.; Hyakudomi, R.; Yamamoto, T.; Tajima, Y. Novel inflammation-combined prognostic index to predict survival outcomes in patients with gastric cancer. Oncotarget 2023, 14, 71–82. [Google Scholar] [CrossRef]
- Ilze, S.; Tatjana, B.; Arturs, K.; Boriss, S.; Roberts, R.; Andrejs, V.; Inese, D.; Dzeina, M.; Arnis, A.; Arvids, J.; et al. Systemic Inflammatory Reaction in Gastric Cancer: Biology and Practical Implications of Neutrophil to Lymphocyte Ratio, Glasgow Prognostic Score and Related Parameters. In Gastric Cancer; Gyula, M., Oszkár, K., Eds.; IntechOpen: Rijeka, Croatia, 2017. [Google Scholar] [CrossRef]
- Kudou, K.; Kusumoto, T.; Nambara, S.; Tsuda, Y.; Kusumoto, E.; Yoshida, R.; Sakaguchi, Y.; Ikejiri, K. New index combining multiple inflammation-based prognostic scores for predicting the prognosis of gastric cancer patients. JGH Open 2022, 6, 171–178. [Google Scholar] [CrossRef]
- Jeong, J.H.; Lim, S.M.; Yun, J.Y.; Rhee, G.W.; Lim, J.Y.; Cho, J.Y.; Kim, Y.R. Comparison of two inflammation-based prognostic scores in patients with unresectable advanced gastric cancer. Oncology 2012, 83, 292–299. [Google Scholar] [CrossRef]
- Hacker, U.T.; Hasenclever, D.; Baber, R.; Linder, N.; Busse, H.; Obermannova, R.; Zdrazilova-Dubska, L.; Valik, D.; Lordick, F. Modified Glasgow prognostic score (mGPS) is correlated with sarcopenia and dominates the prognostic role of baseline body composition parameters in advanced gastric and esophagogastric junction cancer patients undergoing first-line treatment from the phase III EXPAND trial. Ann. Oncol. 2022, 33, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Wei, W.; Hou, H.; Ning, S.; Li, J.; Huang, B.; Liu, K.; Zhang, L. Prognostic Value of C-Reactive Protein, Glasgow Prognostic Score, and C-Reactive Protein-to-Albumin Ratio in Colorectal Cancer. Front. Cell Dev. Biol. 2021, 9, 637650. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Ruan, G.; Ge, Y.; Zhang, Q.; Zhang, H.; Lin, S.; Song, M.; Zhang, X.; Liu, X.; Li, X.; et al. Inflammatory burden as a prognostic biomarker for cancer. Clin. Nutr. 2022, 41, 1236–1243. [Google Scholar] [CrossRef]
- Ding, P.; Wu, H.; Liu, P.; Sun, C.; Yang, P.; Tian, Y.; Guo, H.; Liu, Y.; Zhao, Q. The inflammatory burden index: A promising prognostic predictor in patients with locally advanced gastric cancer. Clin. Nutr. 2023, 42, 247–248. [Google Scholar] [CrossRef] [PubMed]
- In, H.; Solsky, I.; Palis, B.; Langdon-Embry, M.; Ajani, J.; Sano, T. Validation of the 8th Edition of the AJCC TNM Staging System for Gastric Cancer using the National Cancer Database. Ann. Surg. Oncol. 2017, 24, 3683–3691. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Al-Batran, S.E.; Hofheinz, R.D.; Pauligk, C.; Kopp, H.G.; Haag, G.M.; Luley, K.B.; Meiler, J.; Homann, N.; Lorenzen, S.; Schmalenberg, H.; et al. Histopathological regression after neoadjuvant docetaxel, oxaliplatin, fluorouracil, and leucovorin versus epirubicin, cisplatin, and fluorouracil or capecitabine in patients with resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4-AIO): Results from the phase 2 part of a multicentre, open-label, randomised phase 2/3 trial. Lancet Oncol. 2016, 17, 1697–1708. [Google Scholar] [CrossRef]
- Kolfschoten, N.E.; Kievit, J.; Gooiker, G.A.; van Leersum, N.J.; Snijders, H.S.; Eddes, E.H.; Tollenaar, R.A.; Wouters, M.W.; Marang-van de Mheen, P.J. Focusing on desired outcomes of care after colon cancer resections; hospital variations in ‘textbook outcome’. Eur. J. Surg. Oncol. 2013, 39, 156–163. [Google Scholar] [CrossRef]
- van der Kaaij, R.T.; de Rooij, M.V.; van Coevorden, F.; Voncken, F.E.M.; Snaebjornsson, P.; Boot, H.; van Sandick, J.W. Using textbook outcome as a measure of quality of care in oesophagogastric cancer surgery. Br. J. Surg. 2018, 105, 561–569. [Google Scholar] [CrossRef]
- Busweiler, L.A.; Schouwenburg, M.G.; van Berge Henegouwen, M.I.; Kolfschoten, N.E.; de Jong, P.C.; Rozema, T.; Wijnhoven, B.P.; van Hillegersberg, R.; Wouters, M.W.; van Sandick, J.W.; et al. Textbook outcome as a composite measure in oesophagogastric cancer surgery. Br. J. Surg. 2017, 104, 742–750. [Google Scholar] [CrossRef]
- Becker, K.; Mueller, J.D.; Schulmacher, C.; Ott, K.; Fink, U.; Busch, R.; Böttcher, K.; Siewert, J.R.; Höfler, H. Histomorphology and grading of regression in gastric carcinoma treated with neoadjuvant chemotherapy. Cancer 2003, 98, 1521–1530. [Google Scholar] [CrossRef] [PubMed]
- Baiocchi, G.L.; D’Ugo, D.; Coit, D.; Hardwick, R.; Kassab, P.; Nashimoto, A.; Marrelli, D.; Allum, W.; Berruti, A.; Chandramohan, S.M.; et al. Follow-up after gastrectomy for cancer: The Charter Scaligero Consensus Conference. Gastric Cancer 2016, 19, 15–20. [Google Scholar] [CrossRef]
- Kim, M.R.; Kim, A.S.; Choi, H.I.; Jung, J.H.; Park, J.Y.; Ko, H.J. Inflammatory markers for predicting overall survival in gastric cancer patients: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0236445. [Google Scholar] [CrossRef]
- Kuroda, K.; Toyokawa, T.; Miki, Y.; Yoshii, M.; Tamura, T.; Tanaka, H.; Lee, S.; Muguruma, K.; Yashiro, M.; Ohira, M. Prognostic impact of postoperative systemic inflammatory response in patients with stage II/III gastric cancer. Sci. Rep. 2022, 12, 3025. [Google Scholar] [CrossRef]
- Sun, Y.; Yang, L.; Wang, C.; Zhao, D.; Cai, J.; Li, W.; Zhang, W.; Huang, J.; Zhou, A. Prognostic factors associated with locally advanced gastric cancer patients treated with neoadjuvant chemotherapy followed by surgical resection. Oncotarget 2017, 8, 75186–75194. [Google Scholar] [CrossRef][Green Version]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.Y.; Yim, H.W.; Park, C.H.; Song, K.Y. C-reactive protein can be an early predictor of postoperative complications after gastrectomy for gastric cancer. Surg. Endosc. 2017, 31, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Wu, Z.; Wang, Q.; Zhang, Y.; Shan, F.; Hou, S.; Ying, X.; Huangfu, L.; Li, Z.; Ji, J. Clinical predictive efficacy of C-reactive protein for diagnosing infectious complications after gastric surgery. Therap Adv. Gastroenterol. 2020, 13, 1756284820936542. [Google Scholar] [CrossRef] [PubMed]
- Shishido, Y.; Fujitani, K.; Yamamoto, K.; Hirao, M.; Tsujinaka, T.; Sekimoto, M. C-reactive protein on postoperative day 3 as a predictor of infectious complications following gastric cancer resection. Gastric Cancer 2016, 19, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Luo, B.; Liao, Q.; Zheng, J.; Hu, W.; Yao, X.; Li, Y.; Wang, J. The ratio of serum C-reactive protein level on postoperative day 3 to day 2 is a good marker to predict postoperative complications after laparoscopic radical gastrectomy for gastric cancer. Langenbecks Arch. Surg. 2022, 407, 1451–1460. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, S.; Yan, C.; Chen, J.; Shan, F. Perioperative Use of Glucocorticoids and Intraoperative Hypotension May Affect the Incidence of Postoperative Infection in Patients with Gastric Cancer: A Retrospective Cohort Study. Cancer Manag. Res. 2021, 13, 7723–7734. [Google Scholar] [CrossRef]
- McSorley, S.T.; Horgan, P.G.; McMillan, D.C. The impact of preoperative corticosteroids on the systemic inflammatory response and postoperative complications following surgery for gastrointestinal cancer: A systematic review and meta-analysis. Crit. Rev. Oncol./Hematol. 2016, 101, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Cao, S.; Liu, X.; Li, Z.; Tian, Y.; Zhang, X.; Zhong, H.; Zhou, Y. Effect of perioperative probiotic supplements on postoperative short-term outcomes in gastric cancer patients receiving neoadjuvant chemotherapy: A double-blind, randomized controlled trial. Nutrition 2022, 96, 111574. [Google Scholar] [CrossRef]
- Magnin, J.; Fournel, I.; Doussot, A.; Régimbeau, J.-M.; Zerbib, P.; Piessen, G.; Beyer-Berjot, L.; Deguelte, S.; Lakkis, Z.; Schwarz, L.; et al. Benefit of a flash dose of corticosteroids in digestive surgical oncology: A multicenter, randomized, double blind, placebo-controlled trial (CORTIFRENCH). BMC Cancer 2022, 22, 913. [Google Scholar] [CrossRef]
- Zhang, R.; Hu, C.; Zhang, J.; Zhang, Y.; Yuan, L.; Yu, P.; Wang, Y.; Bao, Z.; Cao, M.; Ruan, R.; et al. Prognostic significance of inflammatory and nutritional markers in perioperative period for patients with advanced gastric cancer. BMC Cancer 2023, 23, 5. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Study Group (n = 93) n (%) or Median (Range) |
|---|---|
| Sex | |
| Men | 60 (64.5%) |
| Women | 33 (35.5%) |
| Age | 61 (32–83) |
| Lauren’s type | |
| Intestinal | 45 (49.5%) |
| Mixed | 22 (24.2%) |
| Diffuse | 24 (26.4%) |
| Tumor localization | |
| U | 22 (23.66%) |
| M | 43 (46.2%) |
| L | 28 (30.1%) |
| (y)pT | |
| 0 | 4 (4.3%) |
| 1 | 7 (7.6%) |
| 2 | 19 (20.4%) |
| 3 | 48 (51.6%) |
| 4 | 15 (16.1%) |
| (y)pN | |
| 0 | 41 (44.1%) |
| 1 | 14 (15.1%) |
| 2 | 13 (14%) |
| 3a | 9 (9.7%) |
| 3b | 16 (17.2%) |
| Grading | |
| G1 | 5 (5.4%) |
| G2 | 42 (45.2%) |
| G3 | 46 (49.5%) |
| Neoadjuvant chemotherapy | |
| Yes | 79 (84.9%) |
| No | 14 (15.1%) |
| No. of neoadjuvant chemotherapy cycles | 3 (2–8) |
| Tumor regression grade | |
| 1 | 4 (5.2%) |
| 2 | 12 (15.6%) |
| 3 | 36 (46.8%) |
| 4 | 25 (32.5%) |
| N/A: n = 14 | |
| No data: n = 2 | |
| Type of gastrectomy | |
| Proximal | 21 (22.6%) |
| Distal | 33 (35.5%) |
| Total | 39 (41.9%) |
| Surgical margin | |
| R0 | 85 (91.4%) |
| R1 | 8 (8.6%) |
| CCI | 20.9 (0–100) |
| Postoperative complications | |
| No | 67 (72%) |
| Yes | 26 (28%) |
| Unplanned ICU | |
| No | 77 (82.8%) |
| Yes | 16 (17.2%) |
| ICU stay [days] | 2.5 (1–9) |
| TO | |
| No | 44 (47.8%) |
| Yes | 48 (52.2%) |
| No data: n = 1 | |
| Adjuvant chemotherapy | |
| No | 28 (35%) |
| Yes | 52 (65%) |
| No data: n = 13 |
| Variable | IBI Median [Interquartile Range] | p |
|---|---|---|
| Sex | ||
| Men | 10.7 [2.9–144.95] | 0.319 |
| Women | 19.2 [3.2–281.1] | |
| Age | ||
| <75 years | 9.97 [2.85–181.10] | 0.078 |
| ≥75 years | 59.06 [20.06–848.65] | |
| Tumor localization | ||
| U | 19.2 [3.9–128.9] | 0.268 |
| M | 15.3 [3–156.5] | |
| L | 7.5 [1.7–241.7] | |
| Lauren’s type | ||
| Intestinal | 10.0 [2.3–72.1] | 0.245 |
| Mixed | 8.6 [3.2–157.6] | |
| Diffuse | 56.2 [4.6–441.9] | |
| (y)pT | ||
| 0 | 2.3 [11–17.3] | 0.439 |
| 1a | 93 [79–178.2] | |
| 1b | 140.8 [7.9–267.5] | |
| 2 | 5.4 [1.6–258.3] | |
| 3 | 16.2 [2.9–155.4] | |
| 4a | 18.9 [6–217.4] | |
| 4b | 256.5 [39.2–816.4] | |
| (y)pN | ||
| 0 | 10 [2–159.4] | 0.284 |
| 1 | 9.3 [1.5–68.4] | |
| 2 | 22 [3.1–416.2] | |
| 3a | 6.6 [1.7–97.9] | |
| 3b | 55.4 [13.1–242.8] | |
| Histopathological grading | ||
| G1 | 31.5 [4.3–261.1] | 0.963 |
| G2 | 19.6 [2.8–182] | |
| G3 | 10.7 [3.3–153.1] | |
| Neoadjuvant chemotherapy | ||
| Yes | 7.9 [2.5–124] | 0.0002 * |
| No | 185.7 [68.5–780.7] | |
| Tumor regression grade | ||
| 1 | 2.3 [1.5–68.4] | 0.509 |
| 2 | 7.1 [1.4–189.1] | |
| 3 | 6.2 [2.6–70] | |
| 4 | 10.5 [3.6–121.8] | |
| Tumor regression grade | ||
| 1 or 2 | 4.6 [1.4–161.4] | 0.474 |
| 3 or 4 | 7.9 [2.8–72.1] | |
| Postoperative complications | ||
| No | 7.9 [2.5–171.9] | 0.0499 * |
| Yes | 32.8 [10–287.3] | |
| Unplanned ICU | ||
| No | 9.7 [2.7–184.8] | 0.199 |
| Yes | 28.7 [10.4–212.3] |
| Variable | mOS (Months) | Univariable | Multivariable | ||
|---|---|---|---|---|---|
| HR [95% CI] | p | HR [95% CI] | p | ||
| Sex | |||||
| Women | 49 | 0.90 [0.48–1.68] | 0.7288 | 0.69 [0.33–1.44] | 0.3292 |
| Men | NR | ||||
| Age | |||||
| <75 years | 43 | 0.70 [0.29–1.73] | 0.4946 | 0.69 [0.25–1.94] | 0.4853 |
| ≥75 years | NR | ||||
| Tumor localization | |||||
| U, M | 33 | 0.42 [0.22–0.78] | 0.0189 * | 0.65 [0.27–1.54] | 0.3274 |
| L | NR | ||||
| Lauren histological type | |||||
| Intestinal | NR | 0.43 [0.23–0.79] | 0.0057 * | 0.63 [0.32–1.24] | 0.1848 |
| Diffuse/Mixed | 25 | ||||
| (y)pT | |||||
| 0–3 | 54 | 1.98 [0.82–4.77] | 0.0502 * | 1.37 [0.65–2.90] | 0.4098 |
| 4 | 17 | ||||
| (y)pN | |||||
| N0 | NR | 3.54 [1.93–6.49] | 0.0001 * | 3.41 [1.64–7.12] | 0.0011 * |
| N+ | 18 | ||||
| Histopathological grading | |||||
| G3 | NR | 2.03 [1.12–3.71] | 0.0193 * | 0.56 [0.29–1.08] | 0.0844 |
| G1, G2 | 26 | ||||
| Neoadjuvant chemotherapy | |||||
| Yes | 54 | 0.45 [0.17–1.19] | 0.0593 * | 0.40 [0.18–0.90] | 0.0278 * |
| No | 8 | ||||
| Tumor regression grade | |||||
| 3, 4 | NR | 0.24 [0.10–0.55] | 0.0304 * | 0.33 [0.07–1.45] | 0.1441 |
| 1, 2 | 43 | ||||
| Type of gastrectomy | |||||
| Proximal, Distal | NR | 2.32 [1.24–4.33] | 0.0041 * | 2.77 [1.45–5.31] | 0.0022 * |
| Total | 16 | ||||
| TO | |||||
| No | 31 | 0.51 [0.28–0.93] | 0.0269 * | 0.42 [0.22–0.81] | 0.0094 * |
| Yes | NR | ||||
| Adjuvant chemotherapy | |||||
| No | 49 | 0.64 [0.31–1.31] | 0.1877 | 0.54 [0.25–1.18] | 0.1246 |
| Yes | NR | ||||
| LMR | |||||
| Low | NR | 0.86 [0.47–2.57] | 0.6157 | 0.82 [0.44–1.54] | 0.5438 |
| High | 54 | ||||
| PLR | |||||
| Low | 62 | 1.46 [0.80–2.67] | 0.1975 | 1.07 [0.55–2.06] | 0.8436 |
| High | 25 | ||||
| NLR | |||||
| Low | NR | 2.58 [1.41–4.73] | 0.0017 * | 2.55 [1.32–4.94] | 0.0056 * |
| High | 18 | ||||
| IBI | |||||
| Low | NR | 1.91 [1.05–3.48] | 0.0337 * | 2.56 [1.28–5.13] | 0.0083 * |
| High | 27 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pelc, Z.; Sędłak, K.; Mlak, R.; Leśniewska, M.; Mielniczek, K.; Rola, P.; Januszewski, J.; Zhaldak, O.; Rekowska, A.; Gęca, K.; et al. Prognostic Value of Inflammatory Burden Index in Advanced Gastric Cancer Patients Undergoing Multimodal Treatment. Cancers 2024, 16, 828. https://doi.org/10.3390/cancers16040828
Pelc Z, Sędłak K, Mlak R, Leśniewska M, Mielniczek K, Rola P, Januszewski J, Zhaldak O, Rekowska A, Gęca K, et al. Prognostic Value of Inflammatory Burden Index in Advanced Gastric Cancer Patients Undergoing Multimodal Treatment. Cancers. 2024; 16(4):828. https://doi.org/10.3390/cancers16040828
Chicago/Turabian StylePelc, Zuzanna, Katarzyna Sędłak, Radosław Mlak, Magdalena Leśniewska, Katarzyna Mielniczek, Piotr Rola, Jacek Januszewski, Olena Zhaldak, Anna Rekowska, Katarzyna Gęca, and et al. 2024. "Prognostic Value of Inflammatory Burden Index in Advanced Gastric Cancer Patients Undergoing Multimodal Treatment" Cancers 16, no. 4: 828. https://doi.org/10.3390/cancers16040828
APA StylePelc, Z., Sędłak, K., Mlak, R., Leśniewska, M., Mielniczek, K., Rola, P., Januszewski, J., Zhaldak, O., Rekowska, A., Gęca, K., Skórzewska, M., Polkowski, W. P., Pawlik, T. M., & Rawicz-Pruszyński, K. (2024). Prognostic Value of Inflammatory Burden Index in Advanced Gastric Cancer Patients Undergoing Multimodal Treatment. Cancers, 16(4), 828. https://doi.org/10.3390/cancers16040828