

Sexuality as a Prognostic Factor—Results of an Individual Patient Data NOGGO (North-Eastern German Society of Gynecological Oncology)-Meta-Analysis of 644 Recurrent Ovarian Cancer Patients Prior to Chemotherapy

 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Tower Study
2.2. TRIAS Study
2.3. Hector Study
2.4. Treosulfan Study
2.5. EORTC questionnaires QLQ-C30 and EORTC QLQ-OV28
2.6. Statistics
3. Results
3.1. Association with Patients’ Characteristics
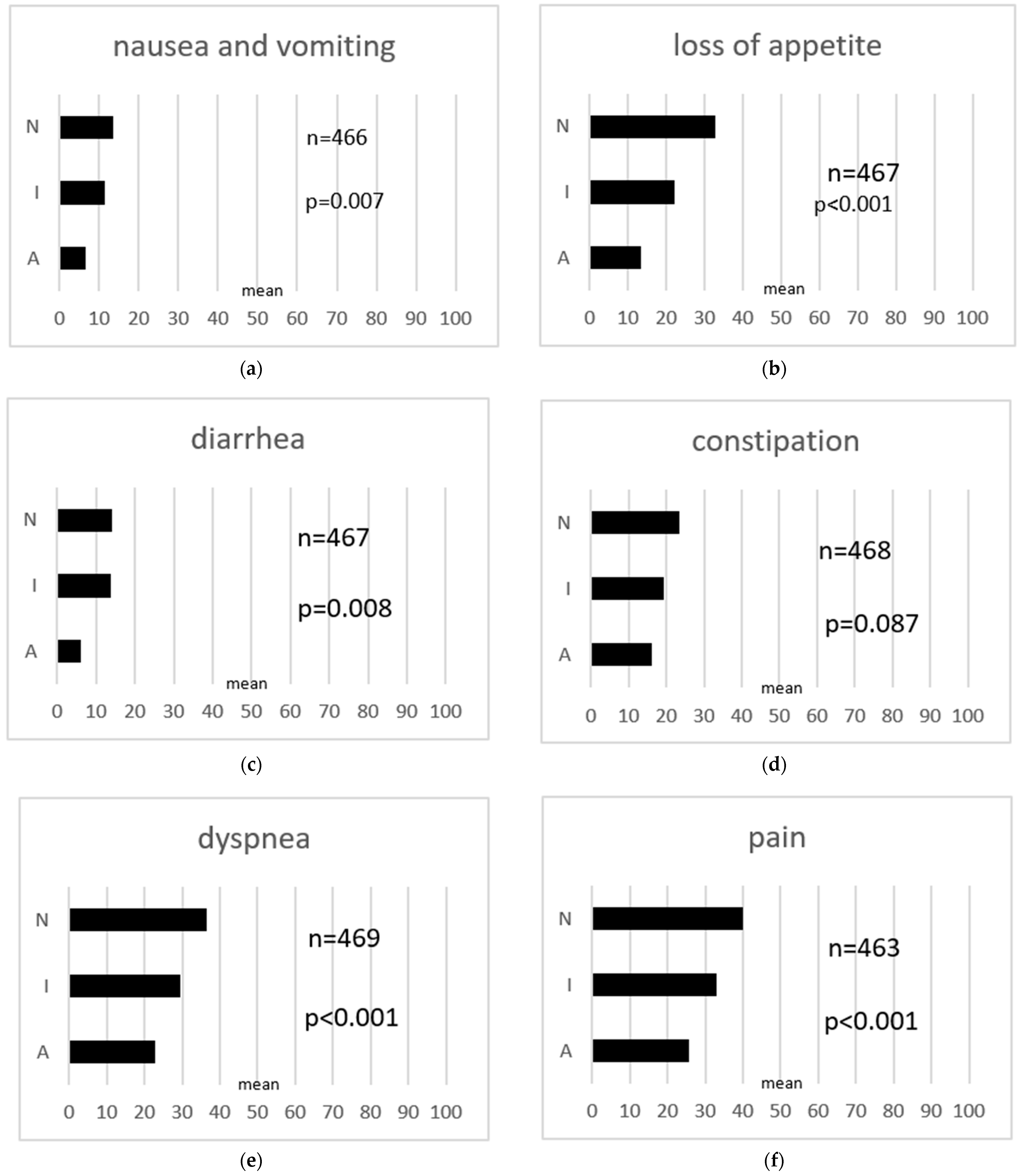
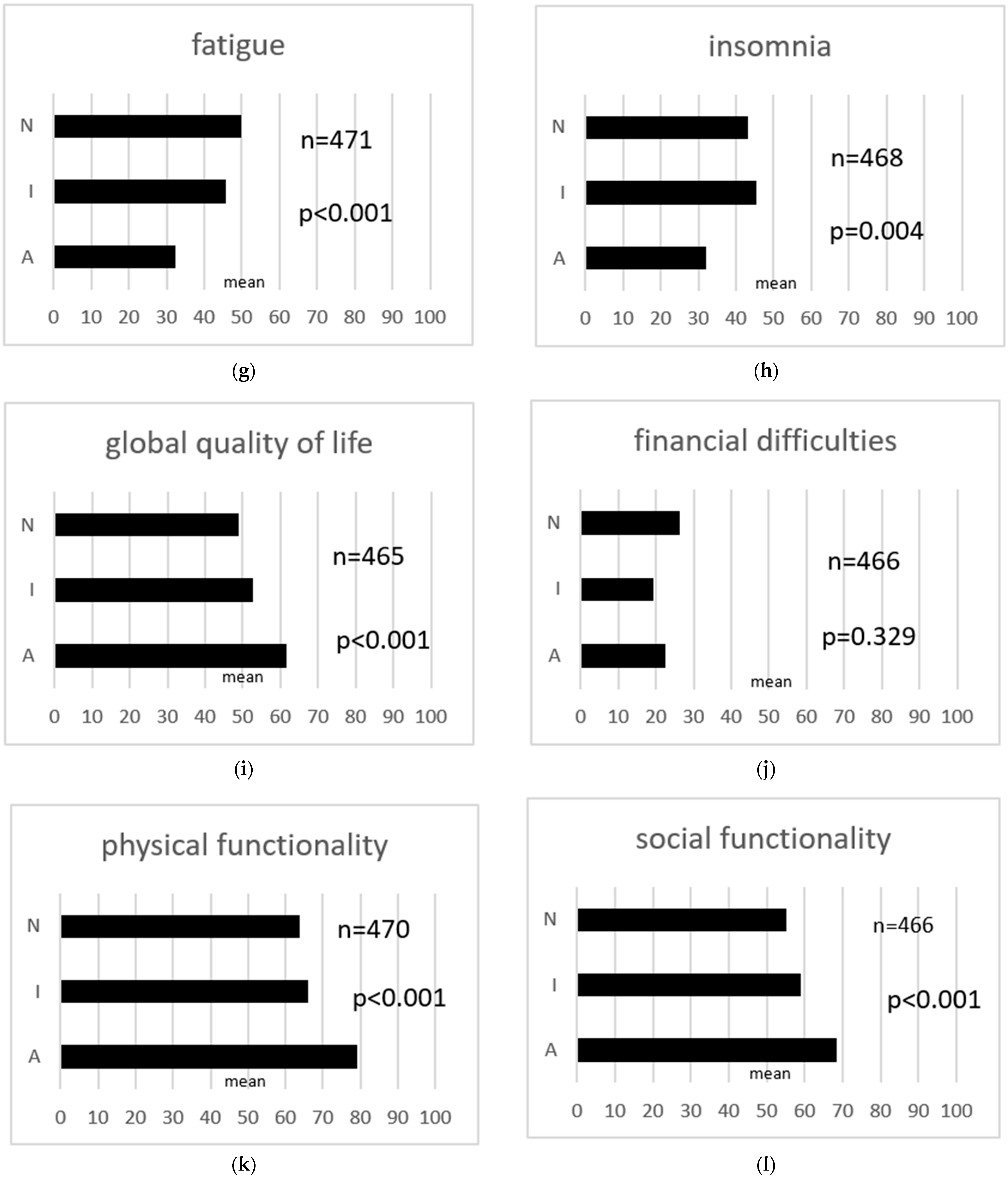
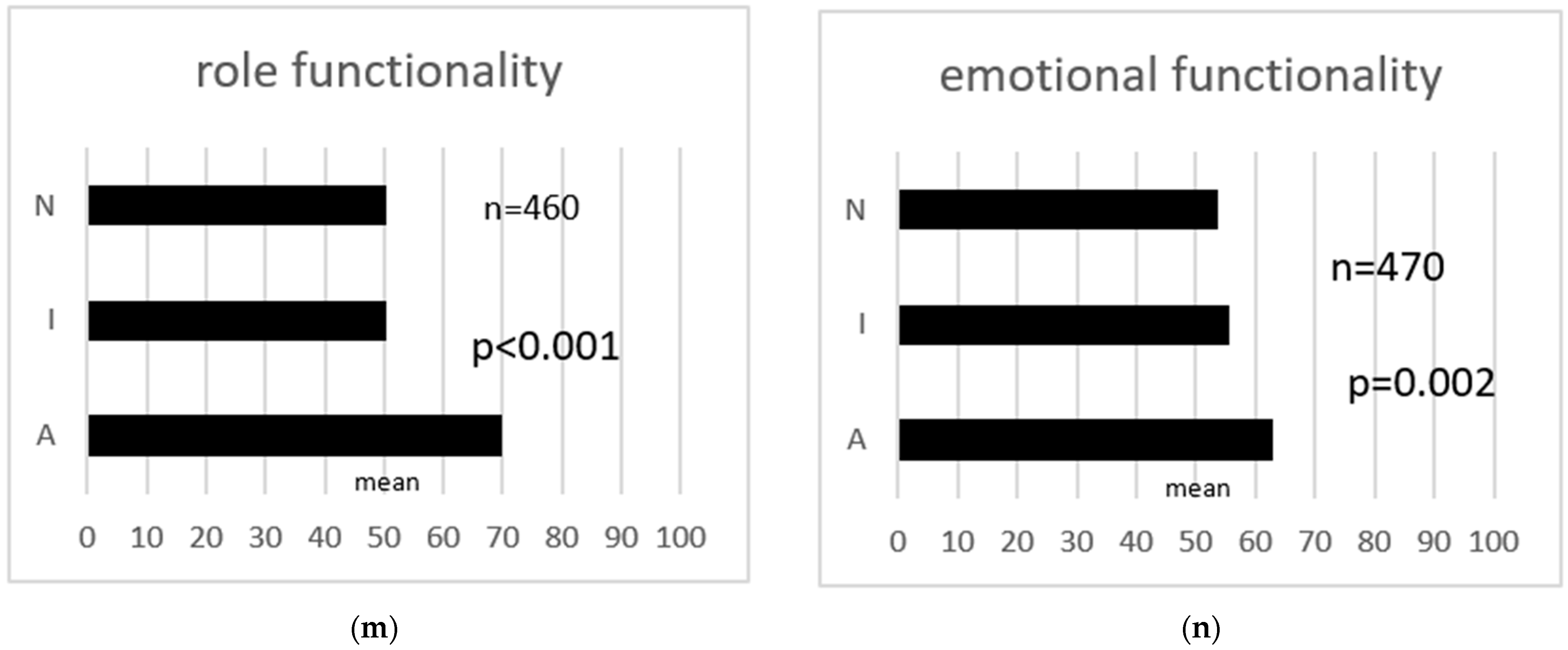
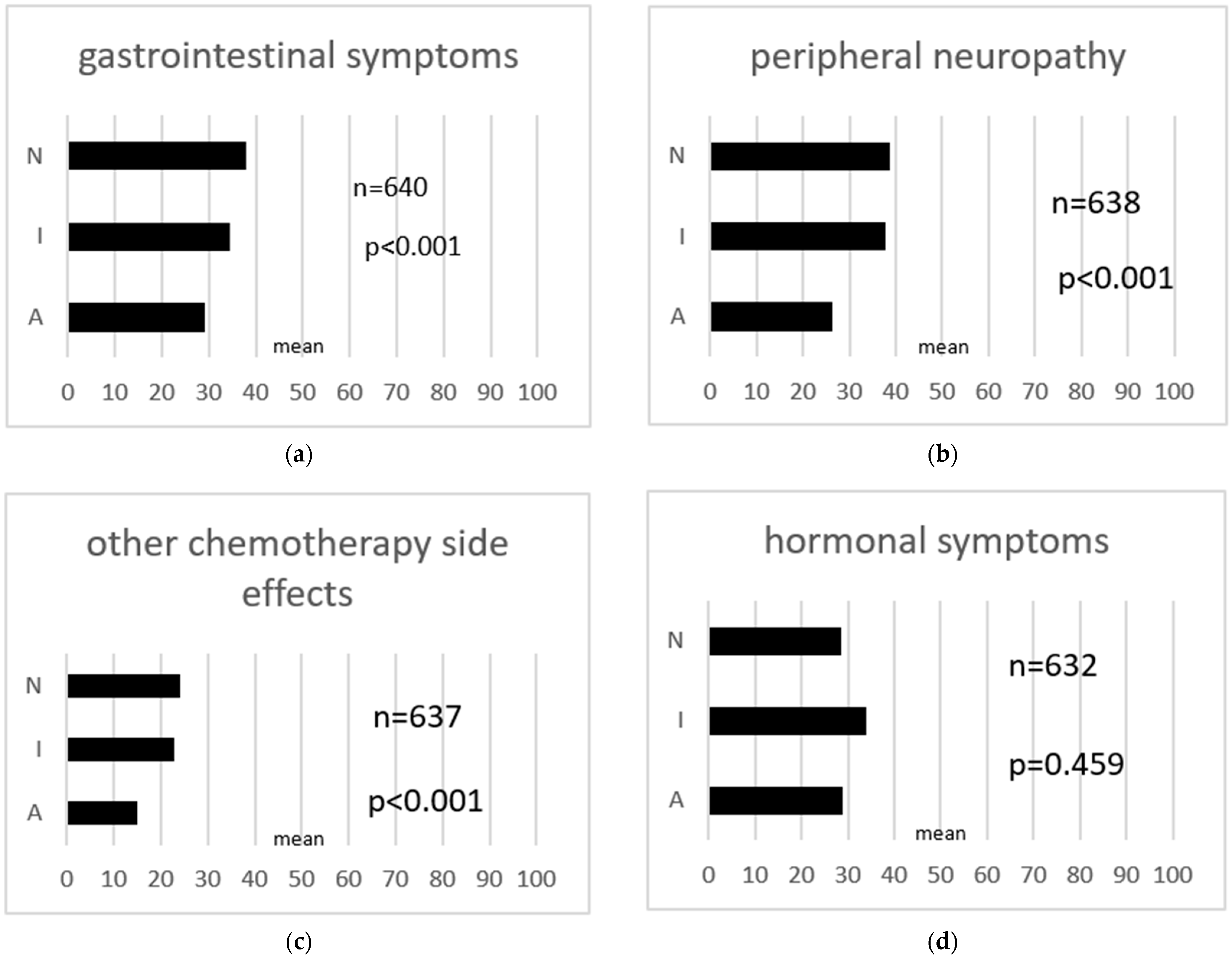
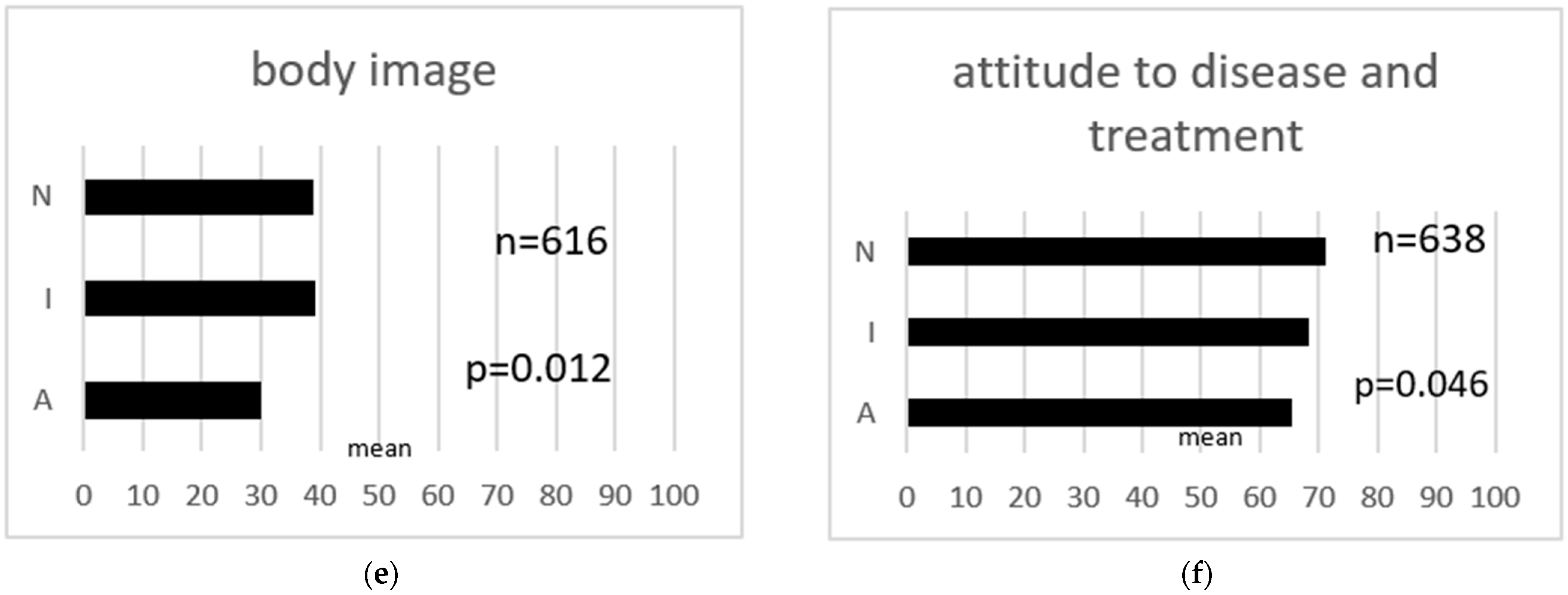
3.2. Association with Quality of Life
3.3. Discontinuation of Chemotherapy
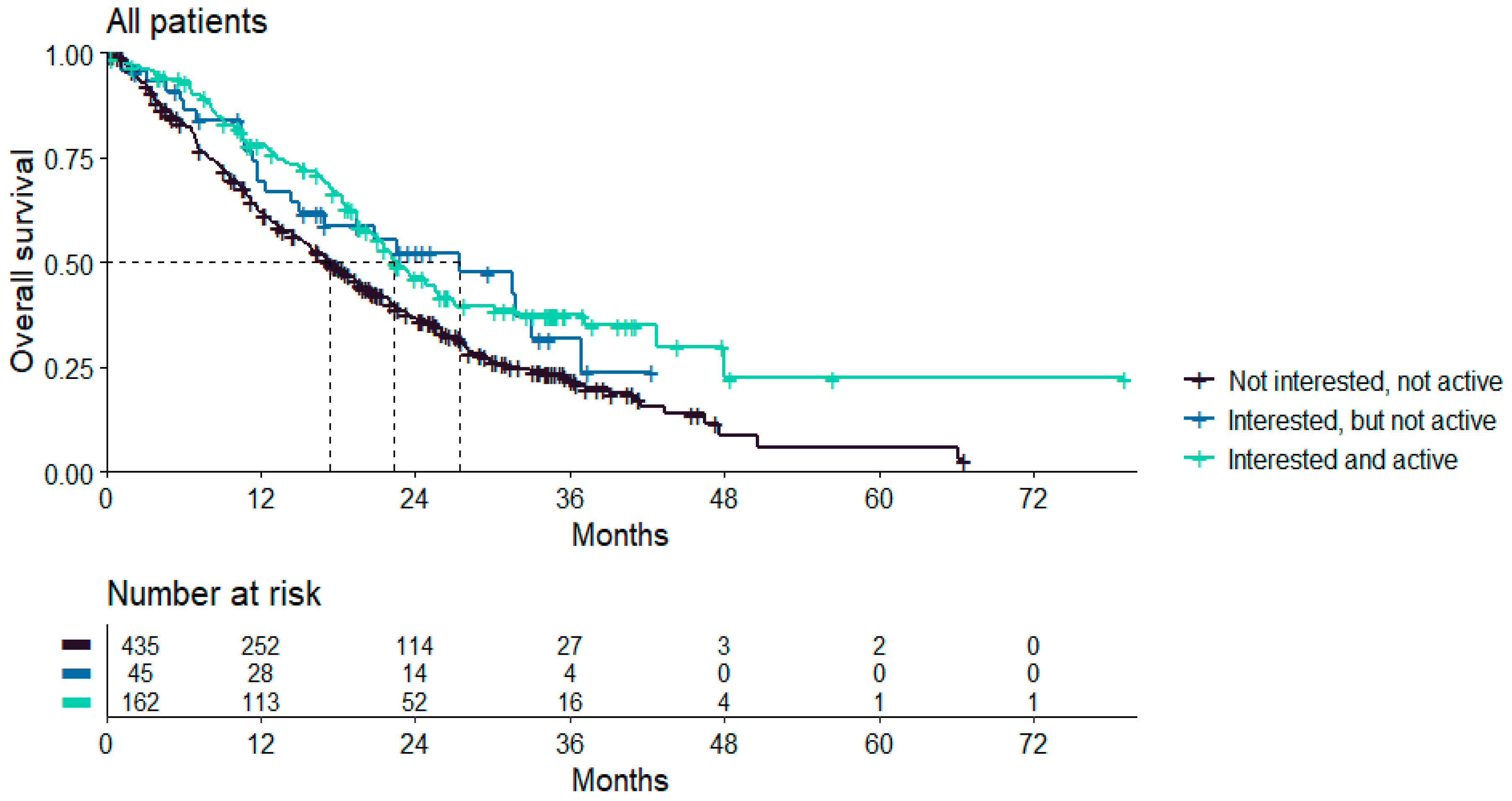
3.4. Association with Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- S3-Leitlinie Maligne Ovarialtumoren|Version 5.1|Mai 2022/AWMF-Register nummer: 032/035OL. Available online: https://register.awmf.org/de/leitlinien/detail/032-035OL (accessed on 8 June 2022).
- Mayer, S.; Iborra, S.; Grimm, D.; Steinsiek, L.; Mahner, S.; Bossart, M.; Woelber, L.; Voss, P.J.; Gitsch, G.; Hasenburg, A. Sexual activity and quality of life in patients after treatment for breast and ovarian cancer. Arch. Gynecol. Obstet. 2019, 299, 191–201. [Google Scholar] [CrossRef]
- Hasenburg, A.; Sehouli, J.; Lampe, B.; Reuss, A.; Schmalfeld, B.; Belau, A.K.; Bossart, M.; Mahner, S.; Hillemanns, P.; Petry, U.; et al. LION-PAW (lymphadenectomy in ovarian neoplasm) sexual function assessment: A prospective sub-study of the LION trial. Int. J. Gynecol. Cancer 2020, 30, 1548–1553. [Google Scholar] [CrossRef]
- Cianci, S.; Tarascio, M.; Rosati, A.; Caruso, S.; Uccella, S.; Cosentino, F.; Scaletta, G.; Gueli Alletti, S.; Scambia, G. Sexual function and quality of life of patients affected by ovarian cancer. Minerva Med. 2019, 110, 320–329. [Google Scholar] [CrossRef]
- Whicker, M.; Black, J.; Altwerger, G.; Menderes, G.; Feinberg, J.; Ratner, E. Management of sexuality, intimacy, and menopause symptoms in patients with ovarian cancer. Am. J. Obs. Gynecol. 2017, 217, 395–403. [Google Scholar] [CrossRef]
- Rolf, C.; Woopen, H.; Richter, R.; Sehouli, A.P.; Braicu, E.I.; Schnuppe, K.; Sehouli, J. Assesment of sexuality in longterm survivors with ovarian cancer. Geburtshilfe Frauenheilkd 2018, 78, 190. [Google Scholar] [CrossRef]
- Robert Koch-Institut und die Gesellschaft der Epidemiologischen Krebsregister in Deutschland, e.V. Krebs in Deutschland 2011/2012, 10. Ausgabe. 2015. Available online: https://www.krebsdaten.de/Krebs/DE/Content/Publikationen/Krebs_in_Deutschland/kid_2015/krebs_in_deutschland_2015.pdf?__blob=publicationFile (accessed on 18 August 2016).
- Wenzel, L.; Osann, K.; McKinney, C.; Cella, D.; Fulci, G.; Scroggins, M.J.; Lankes, H.A.; Wang, V.; Nephew, K.P.; Maxwell, G.L.; et al. Quality of Life and Adverse Events: Prognostic Relationships in Long-Term Ovarian Cancer Survival. J. Natl. Cancer Inst. 2021, 113, 1369–1378. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.I.; Lee, Y.; Lim, M.C.; Joo, J.; Park, K.; Lee, D.O.; Park, S.Y. Quality of life and sexuality comparison between sexually active ovarian cancer survivors and healthy women. J. Gynecol. Oncol. 2015, 26, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Harter, P.; Schrof, I.; Karl, L.M.; Hils, R.; Kullmann, V.; Traut, A.; Scheller, H.; du Bois, A. Sexual Function, Sexual Activity and Quality of Life in Women with Ovarian and Endometrial Cancer. Geburtshilfe Frauenheilkd 2013, 73, 428–432. [Google Scholar] [CrossRef]
- Domenici, L.; Palaia, I.; Giorgini, M.; Piscitelli, V.P.; Tomao, F.; Marchetti, C.; Di Donato, V.; Perniola, G.; Musella, A.; Monti, M.; et al. Sexual Health and Quality of Life Assessment among Ovarian Cancer Patients during Chemotherapy. Oncology 2016, 91, 205–210. [Google Scholar] [CrossRef]
- Nho, J.H.; Kim, S.R.; Choi, W.K. Relationships among sexual function, marital intimacy, type D personality and quality of life in patients with ovarian cancer, with spouses. Eur. J. Cancer Care 2022, 31, e13760. [Google Scholar] [CrossRef] [PubMed]
- Mamguem Kamga, A.; Bengrine-Lefevre, L.; Quipourt, V.; Favier, L.; Darut-Jouve, A.; Marilier, S.; Arveux, P.; Desmoulins, I.; Dabakuyo-Yonli, T.S. Long-term quality of life and sexual function of elderly people with endometrial or ovarian cancer. Health Qual. Life Outcomes 2021, 19, 56. [Google Scholar] [CrossRef] [PubMed]
- Fischer, O.J.; Marguerie, M.; Brotto, L.A. Sexual Function, Quality of Life, and Experiences of Women with Ovarian Cancer: A Mixed-Methods Study. Sex Med. 2019, 7, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Klaus, M.B.; Kurt, L. Praxisleitfaden Sexualmedizin, 1st ed.; Springer: Berlin/Heidelberg, Germany, 2011; p. 12. [Google Scholar]
- Pizetta, L.M.; Reis, A.D.C.; Méxas, M.P.; Guimarães, V.A.; de Paula, C.L. Management Strategies for Sexuality Complaints after Gynecologic Cancer: A Systematic Review. Rev. Bras. Ginecol. Obstet. 2022, 44, 962–971. [Google Scholar] [CrossRef] [PubMed]
- Hajimirzaie, S.S.; Tehranian, N.; Razavinia, F.; Khosravi, A.; Keramat, A.; Haseli, A.; Mirzaii, M.; Mousavi, S.A. Evaluation of Couple’s Sexual Function after Childbirth with the Biopsychosocial Model: A Systematic Review of Systematic Reviews and Meta-Analysis. Iran. J. Nurs. Midwifery Res. 2021, 26, 469–478. [Google Scholar] [PubMed]
- Myers Virtue, S.; Manne, S.L.; Ozga, M.; Kissane, D.W.; Rubin, S.; Heckman, C.; Rosenblum, N.; Graff, J.J. Cancer-related concerns among women with a new diagnosis of gynecological cancer: An exploration of age group differences. Int. J. Gynecol. Cancer 2014, 24, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Nowosielski, K.; Pałka, A. Couples’ sexual health after gynaecological cancer diagnosis—An unexplored area for further research. Contemp. Oncol. 2023, 27, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Logue, C.A.; Pugh, J.; Jayson, G. Psychosexual morbidity in women with ovarian cancer. Int. J. Gynecol. Cancer 2020, 30, 1983–1989. [Google Scholar] [CrossRef] [PubMed]
- Ferrell, B.R.; Smith, S.L.; Ervin, K.S.; Itano, J.; Melancon, C. A qualitative analysis of social concerns of women with ovarian cancer. Psychooncology 2003, 12, 647–663. [Google Scholar] [CrossRef] [PubMed]
- Hubbs, J.L.; Dickson Michelson, E.L.; Vogel, R.I.; Rivard, C.L.; Teoh, D.G.K.; Geller, M.A. Sexual quality of life after the treatment of gynecologic cancer: What women want. Support. Care Cancer 2019, 27, 4649–4654. [Google Scholar] [CrossRef]
- Pilger, A.; Richter, R.; Fotopoulou, C.; Beteta, C.; Klapp, C.; Sehouli, J. Quality of life and sexuality of patients after treatment for gynaecological malignancies: Results of a prospective study in 55 patients. Anticancer Res. 2012, 32, 5045–5049. [Google Scholar] [PubMed]
- Sehouli, J.; Stengel, D.; Harter, P.; Kurzeder, C.; Belau, A.; Bogenrieder, T.; Markmann, S.; Mahner, S.; Mueller, L.; Lorenz, R.; et al. Topotecan Weekly Versus Conventional 5-Day Schedule in Patients With Platinum-Resistant Ovarian Cancer: A randomized multicenter phase II trial of the North-Eastern German Society of Gynecological Oncology Ovarian Cancer Study Group. J. Clin. Oncol. 2011, 29, 242–248. [Google Scholar] [CrossRef]
- Chekerov, R.; Hilpert, F.; Mahner, S.; El-Balat, A.; Harter, P.; De Gregorio, N.; Fridrich, C.; Markmann, S.; Potenberg, J.; Lorenz, R.; et al. Sorafenib plus topotecan versus placebo plus topotecan for platinum-resistant ovarian cancer (TRIAS): A multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2018, 19, 1247–1258. [Google Scholar] [CrossRef]
- Sehouli, J.; Chekerov, R.; Reinthaller, A.; Richter, R.; Gonzalez-Martin, A.; Harter, P.; Woopen, H.; Petru, E.; Hanker, L.C.; Keil, E.; et al. Topotecan plus carboplatin versus standard therapy with paclitaxel plus carboplatin (PC) or gemcitabine plus carboplatin (GC) or pegylated liposomal doxorubicin plus carboplatin (PLDC): A randomized phase III trial of the NOGGO-AGO-Study Group-AGO Austria and GEICO-ENGOT-GCIG intergroup study (HECTOR). Ann. Oncol. 2016, 27, 2236–2241. [Google Scholar] [CrossRef]
- Chekerov, R.; Harter, P.; Fuxius, S.; Hanker, L.C.; Woelber, L.; Müller, L.; Klare, P.; Abenhardt, W.; Nedkova, Y.; Yalcinkaya, I.; et al. Preference of elderly patients’ to oral or intravenous chemotherapy in heavily pre-treated recurrent ovarian cancer: Final results of a prospective multicenter trial. Gynecol. Oncol. Res. Pract. 2017, 4, 6. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Greimel, E.; Bottomley, A.; Cull, A.; Waldenstrom, A.C.; Arraras, J.; Chauvenet, L.; Holzner, B.; Kuljanic, K.; Lebrec, J.; D’haese, S.; et al. An international field study of the reliability and validity of a disease-specific questionnaire module (the QLQ-OV28) in assessing the quality of life of patients with ovarian cancer. Eur. J. Cancer 2003, 39, 1402–1408. [Google Scholar] [CrossRef] [PubMed]
- Roncolato, F.T.; Gibbs, E.; Lee, C.K.; Asher, R.; Davies, L.C.; Gebski, V.J.; Friedlander, M.; Hilpert, F.; Wenzel, L.; Stockler, M.R.; et al. Quality of life predicts overall survival in women with platinum-resistant ovarian cancer: An AURELIA substudy. Ann. Oncol. 2017, 28, 1849–1855. [Google Scholar] [CrossRef] [PubMed]
- Woopen, H.; Richter, R.; Inci, G.; Alavi, S.; Chekerov, R.; Sehouli, J. The prognostic and predictive role of pain before systemic chemotherapy in recurrent ovarian cancer: An individual participant data meta-analysis of the North-Eastern German Society of Gynecological Oncology (NOGGO) of 1226 patients. Support. Care Cancer 2020, 28, 1997–2003. [Google Scholar] [CrossRef] [PubMed]
- Sloan, J.A.; Liu, H.; Satele, D.V.; Puttabasavaiah, S.; Kaur, J.S.; Hubbard, J.; Dueck, A.; Stella, P.J.; Singh, J.A. Prognostic significance of baseline fatigue for overall survival: A patient-level meta-analysis of 43 oncology clinical trials with 3915 patients. Trends Cancer Res. 2017, 12, 97–110. [Google Scholar] [PubMed]
- Dhillon, H.M.; van der Ploeg, H.P.; Bell, M.L.; Boyer, M.; Clarke, S.; Vardy, J. The impact of physical activity on fatigue and quality of life in lung cancer patients: A randomised controlled trial protocol. BMC Cancer 2012, 12, 572. [Google Scholar] [CrossRef]
- Bower, J.E.; Bak, K.; Berger, A.; Breitbart, W.; Escalante, C.P.; Ganz, P.A.; Schnipper, H.H.; Lacchetti, C.; Ligibel, J.A.; Lyman, G.H.; et al. Screening, assessment, and management of fatigue in adult survivors of cancer: An American Society of Clinical oncology clinical practice guideline adaptation. J. Clin. Oncol. 2014, 32, 1840–1850. [Google Scholar] [CrossRef]
- Meneses-Echávez, J.F.; González-Jiménez, E.; Ramírez-Vélez, R. Effects of supervised exercise on cancer-related fatigue in breast cancer survivors: A systematic review and meta-analysis. BMC Cancer 2015, 15, 77. [Google Scholar] [CrossRef]
- Bennedsgaard, K.; Ventzel, L.; Themistocleous, A.C.; Bennett, D.L.; Jensen, A.B.; Jensen, A.R.; Andersen, N.T.; Jensen, T.S.; Tankisi, H.; Finnerup, N.B. Long-term symptoms of polyneuropathy in breast and colorectal cancer patients treated with and without adjuvant chemotherapy. Cancer Med. 2020, 9, 5114–5123. [Google Scholar] [CrossRef]
- S3-Leitlinie Supportive Therapie bei onkologischen PatientInnen, Langversion 1.3—Februar 2020, AWMF-Register Nummer: 032/054OL. Available online: https://register.awmf.org/de/leitlinien/detail/032-054OL (accessed on 23 July 2020).
- Streckmann, F.; Zopf, E.M.; Lehmann, H.C.; May, K.; Rizza, J.; Zimmer, P.; Gollhofer, A.; Bloch, W.; Baumann, F.T. Exercise intervention studies in patients with peripheral neuropathy: A systematic review. Sports Med. 2014, 44, 1289–1304. [Google Scholar] [CrossRef]
- Quinten, C.; Martinelli, F.; Coens, C.; Sprangers, M.A.; Ringash, J.; Gotay, C.; Bjordal, K.; Greimel, E.; Reeve, B.B.; Maringwa, J.; et al. A global analysis of multitrial data investigating quality of life and symptoms as prognostic factors for survival in different tumor sites. Cancer 2014, 120, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Meinhold-Heerlein, I.; Fotopoulou, C.; Harter, P.; Kurzeder, C.; Mustea, A.; Wimberger, P.; Hauptmann, S.; Sehouli, J.; Kommission Ovar of the AGO. Statement by the Kommission Ovar of the AGO: The New FIGO and WHO Classifications of Ovarian, Fallopian Tube and Primary Peritoneal Cancer. Geburtshilfe Frauenheilkd 2015, 75, 1021–1027. [Google Scholar] [CrossRef] [PubMed]
- Zeppernick, F.; Meinhold-Heerlein, I. The new FIGO staging system for ovarian, fallopian tube, and primary peritoneal cancer. Arch. Gynecol. Obstet. 2014, 290, 839–842. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.K.; Pujade-Lauraine, E.; Aoki, D.; Mirza, M.R.; Lorusso, D.; Oza, A.M.; du Bois, A.; Vergote, I.; Reuss, A.; Bacon, M.; et al. Fifth Ovarian Cancer Consensus Conference of the Gynecologic Cancer InterGroup: Recurrent disease. Ann. Oncol. 2017, 28, 727–732. [Google Scholar] [CrossRef]
- Thieme Praxis Report 05/2016; 8 (5): 1–12 Aktueller Stand der Therapie des Ovarialkarzinomrezidivs. Available online: https://www.thieme-connect.com/products/ejournals/pdf/10.1055/s-0036-1584233.pdf (accessed on 29 October 2023).
- Balint, N.; Pirmorady-Sehouli, A.; Richter, R.; Zocholl, D.; Woopen, H.; Pietzner, K.; Sehouli, J. Sexuality as a prognostic factor: Results of an individual participant data NOGGO-meta-analysis of 1,041 recurrent ovarian cancer patients before starting chemotherapy. J. Clin. Oncol. 2023, 41 (Suppl. S16), e24128. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. of Patients n | Group A 1 n | Group I 2 n | Group N 3 n | Significance | |
|---|---|---|---|---|---|
| Median age at first diagnosis in years (range) | 644 | 162 53 years (24–80) | 45 58 years (range: 35–76) | 437 62 years (range: 32–85) | p < 0.001 |
| Median age at randomization in years (range) | 664 | 162 57 years (25–81) | 45 60 years (37–78) | 437 65 years (33–87) | p < 0.001 |
| ECOG 0 * | 298 | 94 (31.5%) | 20 (6.7%) | 184 (61.7%) | |
| ECOG 1 * | 300 | 61 (20.3%) | 24 (8.0%) | 215 (71.7%) | p < 0.001 |
| ECOG 2 * | 43 | 6 (14.0%) | 1 (2.3%) | 36 (83.7%) | |
| No. of recurrences 1 | 416 | 115 (27.6%) | 35 (8.4%) | 266 (63.9%) | |
| No. of recurrences 2 | 164 | 41 (25.0%) | 7 (4.3%) | 116 (70.7%) | p < 0.001 |
| No. of recurrences >2 | 64 | 6 (9.4%) | 3 (4.7%) | 55 (85.9%) | |
| Presence of Ascites | 168 | 30 (17.9%) | 12 (7.1%) | 126 (75%) | p = 0.002 |
| BMI (median) | 644 | 162 (24.8) | 45 (25.2) | 437 (25.8) | p = 0.282 |
| FIGO I + II | 71 | 20 (28.2%) | 8 (11.3%) | 43 (60.6%) | |
| FIGO III | 444 | 106 (23.9%) | 31 (7.0%) | 307 (69.1%) | p = 0.438 |
| FIGO IV | 108 | 29 (26.9%) | 4 (3.7%) | 75 (69.4%) | |
| Grading G1 | 27 | 12 (44.4%) | 0 (0.0%) | 15 (55.6%) | |
| Grading G2 | 183 | 47 (25.7%) | 15 (8.2%) | 121 (66.1%) | p = 0.182 |
| Grading G3 | 384 | 91 (23.7%) | 27 (7.0%) | 266 (69.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balint, N.; Woopen, H.; Richter, R.; Pirmorady-Sehouli, A.; Pietzner, K.; Sehouli, J. Sexuality as a Prognostic Factor—Results of an Individual Patient Data NOGGO (North-Eastern German Society of Gynecological Oncology)-Meta-Analysis of 644 Recurrent Ovarian Cancer Patients Prior to Chemotherapy. Cancers 2024, 16, 811. https://doi.org/10.3390/cancers16040811
Balint N, Woopen H, Richter R, Pirmorady-Sehouli A, Pietzner K, Sehouli J. Sexuality as a Prognostic Factor—Results of an Individual Patient Data NOGGO (North-Eastern German Society of Gynecological Oncology)-Meta-Analysis of 644 Recurrent Ovarian Cancer Patients Prior to Chemotherapy. Cancers. 2024; 16(4):811. https://doi.org/10.3390/cancers16040811
Chicago/Turabian StyleBalint, Nicole, Hannah Woopen, Rolf Richter, Adak Pirmorady-Sehouli, Klaus Pietzner, and Jalid Sehouli. 2024. "Sexuality as a Prognostic Factor—Results of an Individual Patient Data NOGGO (North-Eastern German Society of Gynecological Oncology)-Meta-Analysis of 644 Recurrent Ovarian Cancer Patients Prior to Chemotherapy" Cancers 16, no. 4: 811. https://doi.org/10.3390/cancers16040811
APA StyleBalint, N., Woopen, H., Richter, R., Pirmorady-Sehouli, A., Pietzner, K., & Sehouli, J. (2024). Sexuality as a Prognostic Factor—Results of an Individual Patient Data NOGGO (North-Eastern German Society of Gynecological Oncology)-Meta-Analysis of 644 Recurrent Ovarian Cancer Patients Prior to Chemotherapy. Cancers, 16(4), 811. https://doi.org/10.3390/cancers16040811