
Focal Minimally Invasive Treatment in Localized Prostate Cancer: Comprehensive Review of Different Possible Strategies

 ,
, 

Abstract
Simple Summary
Abstract
1. Introduction
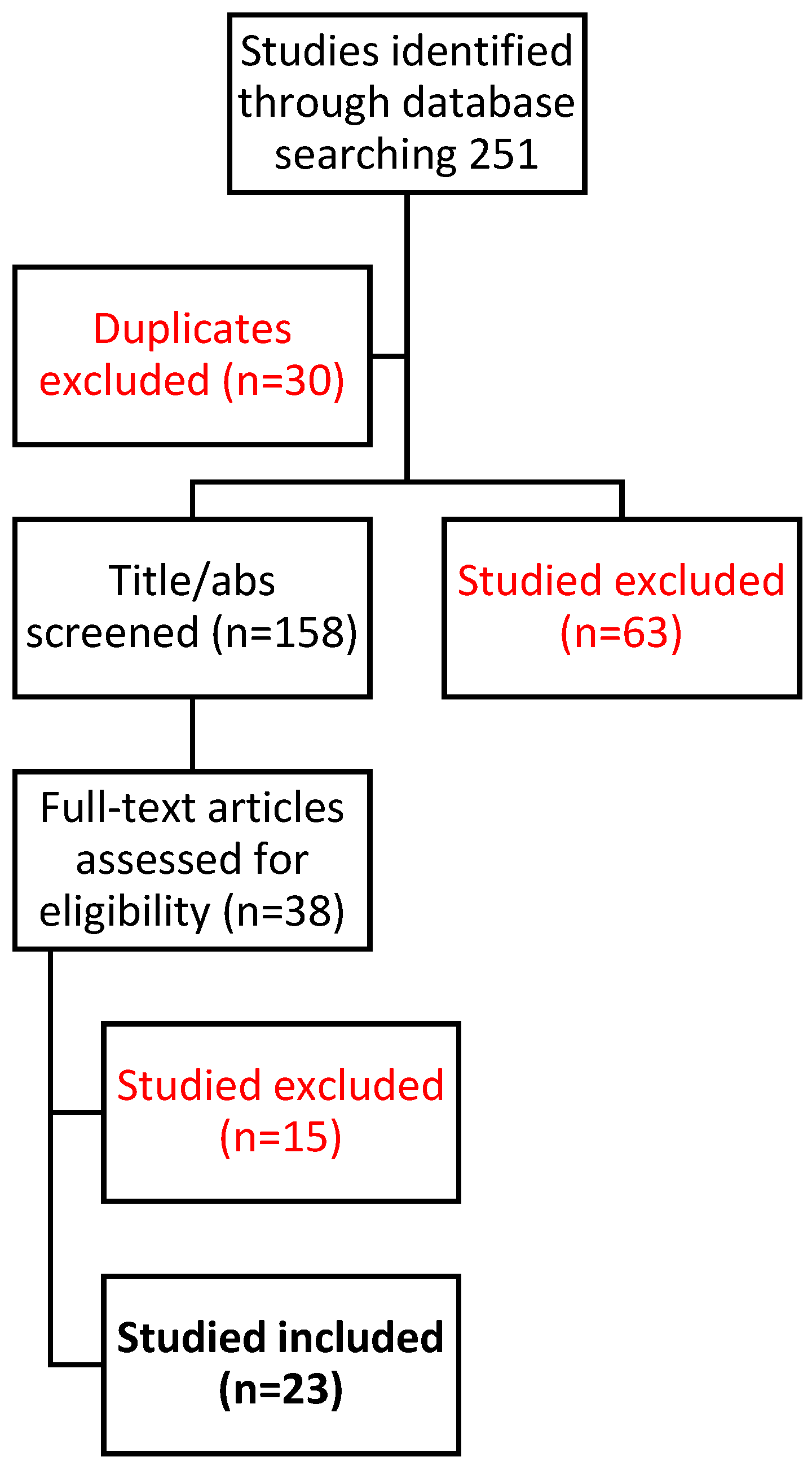
2. Materials and Methods
3. Results
3.1. Cryoablation (CRA)
3.2. Irreversible Electroporation (IRE)
3.3. Microwave Ablation (MWA)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer—2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2020, 79, 243–262. [Google Scholar] [CrossRef]
- Wilt, T.J.; MacDonald, R.; Rutks, I.; Shamliyan, T.A.; Taylor, B.C.; Kane, R.L. Systematic review: Comparative effectiveness and harms of treatments for clinically localized prostate cancer. Ann. Intern. Med. 2008, 148, 435–448. [Google Scholar] [CrossRef]
- Yu, J.S.; Roach, M. Quality of life and satisfaction with outcome among prostate-cancer survivors. N. Engl. J. Med. 2008, 359, 200–202. [Google Scholar] [CrossRef]
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Mason, M.; Metcalfe, C.; Holding, P.; Davis, M.; Peters, T.J.; Turner, E.L.; Martin, R.M.; et al. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. N. Engl. J. Med. 2016, 375, 1415–1424. [Google Scholar] [CrossRef]
- Ahmed, H.U. The index lesion and the origin of prostate cancer. N. Engl. J. Med. 2009, 361, 1704–1706. [Google Scholar] [CrossRef]
- Tay, K.J.; Scheltema, M.J.; Ahmed, H.U.; Barret, E.; Coleman, J.A.; Dominguez-Escrig, J.; Ghai, S.; Huang, J.; Jones, J.S.; Klotz, L.H.; et al. Patient selection for prostate focal therapy in the era of active surveillance: An International Delphi Consensus Project. Prostate Cancer Prostatic Dis. 2017, 20, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, M.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Valerio, M.; Cerantola, Y.; Eggener, S.E.; Lepor, H.; Polascik, T.J.; Villers, A.; Emberton, M. New and Established Technology in Focal Ablation of the Prostate: A Systematic Review. Eur. Urol. 2016, 71, 17–34. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.P.; Kotamarti, S.; Chen, E.; Mahle, R.; Arcot, R.; Chang, A.; Ayala, A.; Michael, Z.; Seguier, D.; Polascik, T.J. Oncological and functional outcomes of men undergoing primary whole gland cryoablation of the prostate: A 20-year experience. Cancer 2022, 128, 3824–3830. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.P.; Chang, A.; Sze, C.; Polascik, T.J. Oncological and Functional Outcomes of Patients Undergoing Individualized Partial Gland Cryoablation of the Prostate: A Single-Institution Experience. J. Endourol. 2021, 35, 1290–1299. [Google Scholar] [CrossRef] [PubMed]
- Chuang, R.; Kinnaird, A.; Kwan, L.; Sisk, A.; Barsa, D.; Felker, E.; Delfin, M.; Marks, L. Hemigland Cryoablation of Clinically Significant Prostate Cancer: Intermediate-Term Followup via Magnetic Resonance Imaging Guided Biopsy. J. Urol. 2020, 204, 941–949. [Google Scholar] [CrossRef]
- Bossier, R.; Sanguedolce, F.; Territo, A.; Vanacore, D.; Martínez, C.; Regis, F.; Gallioli, A.; Mercade, A.; Mosquera, L.; Aumatell, J.; et al. Crioablación total o hemiglandular para el cáncer de próstata primario localizado: Resultados oncológicos y funcionales a corto y medio plazo. Actas Urol. Esp. 2020, 44, 172–178. [Google Scholar] [CrossRef]
- Khan, A.; Khan, A.U.; Siref, L.; Feloney, M. Focal Cryoablation of the Prostate: Primary Treatment in 163 Patients With Localized Prostate Cancer. Cureus 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Selvaggio, O.; Finati, M.; Falagario, U.G.; Silecchia, G.; Recchia, M.; Checchia, A.A.; Milillo, P.; Sanguedolce, F.; Cindolo, L.; Busetto, G.M.; et al. Treatment of localized prostate cancer in elderly patients: The role of partial cryoablation. Int. Urol. Nephrol. 2023, 55, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wysock, J.S.; Rapoport, E.; Hernandez, H.; Gogaj, R.; Lepor, H. Biopsy Assessment of Oncologic Control 3 Years Following Primary Partial Gland Cryoablation: A Prospective Cohort Study of Men with Intermediate-risk Prostate Cancer. J. Urol. 2023, 210, 454–464. [Google Scholar] [CrossRef]
- Smigelski, M.B.; Wysock, J.S.; Taneja, S.S.; Lepor, H. Salvage Cryoablation and Robotic Seminal Vesiculectomy: A Novel Salvage Treatment for Locally Recurrent Prostate Cancer. J. Endourol. 2023, 37, 876–881. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.P.; Kotamarti, S.; Ayala, A.; Mahle, R.; Chen, E.; Arcot, R.; Chang, A.; Michael, Z.; Seguier, D.; Polascik, T.J. Oncological and Functional Outcomes for Men Undergoing Salvage Whole-gland Cryoablation for Radiation-resistant Prostate Cancer. Eur. Urol. Oncol. 2023, 6, 289–294. [Google Scholar] [CrossRef]
- Nair, S.M.; Warner, A.; Lavi, A.; Rodrigues, G.; Chin, J. Does adding local salvage ablation therapy provide survival advantage for patients with locally recurrent prostate cancer following radiotherapy? Can. Urol. Assoc. J. 2020, 15, 123–129. [Google Scholar] [CrossRef]
- Wang, N.; Ye, Y.; Deng, M.; Zhao, D.; Jiang, L.; Chen, D.; Wu, Z.; Wang, Y.; Li, Z.; Yang, Z.; et al. Prostate cryoablation combined with androgen deprivation therapy for newly diagnosed metastatic prostate cancer: A propensity score-based study. Prostate Cancer Prostatic Dis. 2021, 24, 837–844. [Google Scholar] [CrossRef]
- Gregg, J.R.; Borregales, L.D.; Choi, H.; Lozano, M.; McRae, S.E.; Venkatesan, A.M.; Davis, J.W.; Nogueras-Gonzalez, G.M.; Pisters, L.L.; Ward, J.F. Prospective trial of regional (hockey-stick) prostate cryoablation: Oncologic and quality of life outcomes. World J. Urol. 2021, 39, 3259–3264. [Google Scholar] [CrossRef]
- Misuraca, L.; Lugnani, F.; Brassetti, A.; Cacciatore, L.; Tedesco, F.; Anceschi, U.; Bove, A.M.; D’annunzio, S.; Ferriero, M.; Guaglianone, S.; et al. Single-Setting 3D MRI/US-Guided Frozen Sectioning and Cryoablation of the Index Lesion: Mid-Term Oncologic and Functional Outcomes from a Pilot Study. J. Pers. Med. 2023, 13, 978. [Google Scholar] [CrossRef]
- Blazevski, A.; Scheltema, M.J.; Amin, A.; Thompson, J.E.; Lawrentschuk, N.; Stricker, P.D. Irreversible electroporation (IRE): A narrative review of the development of IRE from the laboratory to a prostate cancer treatment. BJU Int. 2019, 125, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Scheltema, M.J.; Geboers, B.; Blazevski, A.; Doan, P.; Katelaris, A.; Agrawal, S.; Barreto, D.; Shnier, R.; Delprado, W.; Thompson, J.E.; et al. Median 5-year outcomes of primary focal irreversible electroporation for localised prostate cancer. BJU Int. 2022, 131, 6–13. [Google Scholar] [CrossRef] [PubMed]
- de la Rosette, J.; Dominguez-Escrig, J.; Zhang, K.; Teoh, J.; Barret, E.; Ramon-Borja, J.C.; Muir, G.; Bohr, J.; de Reijke, T.; Ng, C.-F.; et al. A Multicenter, Randomized, Single-blind, 2-Arm Intervention Study Evaluating the Adverse Events and Quality of Life after Irreversible Electroporation for the Ablation of Localized Low-intermediate Risk Prostate Cancer. J. Urol. 2023, 209, 347–353. [Google Scholar] [CrossRef]
- Gielchinsky, I.; Lev-Cohain, N. Focal Irreversible Electroporation for Localized Prostate Cancer–Oncological and Safety Outcomes Using mpMRI and Transperineal Biopsy Follow-Up. Res. Rep. Urol. 2023, 15, 27–35. [Google Scholar] [CrossRef]
- López, B.M.; Boville, G.A.; Bernardos, G.B.; Marckert, X.A.; Roca, M.T.; Huerta, L.L.; Aubá, F.V.; Chillón, F.R.d.F.; Ortega, J.S.; Muela, M.A.; et al. Focal Therapy of Prostate Cancer Index Lesion With Irreversible Electroporation. A Prospective Study With a Median Follow-up of 3 Years. J. Urol. 2023, 209, 261–270. [Google Scholar] [CrossRef]
- Wang, H.; Xue, W.; Yan, W.; Yin, L.; Dong, B.; He, B.; Yu, Y.; Shi, W.; Zhou, Z.; Lin, H.; et al. Extended Focal Ablation of Localized Prostate Cancer With High-Frequency Irreversible Electroporation. JAMA Surg. 2022, 157, 693–700. [Google Scholar] [CrossRef]
- Kizil, P.G.; Altan, S.A.; Tarhan, N.C.; Adsan, O. Evaluation of clinical and mpMRI findings of irreversible electroporation therapy for the treatment of localized prostate cancer: Preliminary results. Urol. Res. Pract. 2021, 47, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Oderda, M.; Marquis, A.; Calleris, G.; D’Agate, D.; Faletti, R.; Gatti, M.; Marra, G.; Gontero, P. Safety and Feasibility of Transperineal Targeted Microwave Ablation for Low- to Intermediate-risk Prostate Cancer. Eur. Urol. Open Sci. 2022, 46, 3–7. [Google Scholar] [CrossRef]
- Delongchamps, N.B.; Schull, A.; Anract, J.; Abecassis, J.-P.; Zerbib, M.; Sibony, M.; Jilet, L.; Abdoul, H.; Goffin, V.; Peyromaure, M. Feasibility and safety of targeted focal microwave ablation of the index tumor in patients with low to intermediate risk prostate cancer: Results of the FOSTINE trial. PLoS ONE 2021, 16, e0252040. [Google Scholar] [CrossRef]
- Chiu, P.K.-F.; Chan, C.-H.; Yee, C.-H.; Lau, S.-Y.; Teoh, J.Y.-C.; Wong, H.-F.; Lo, K.-L.; Yuen, T.-Y.; Hung, H.-Y.; Cho, C.C.-M.; et al. Transperineal Targeted Microwave Ablation (TMA) of localized prostate cancer guided by MRI-Ultrasound fusion and organ-based tracking: A pilot study. Prostate Cancer Prostatic Dis. 2022, 26, 736–742. [Google Scholar] [CrossRef] [PubMed]
- Mendez, M.H.; Passoni, N.M.; Pow-Sang, J.; Jones, J.S.; Polascik, T.J. Comparison of Outcomes Between Preoperatively Potent Men Treated with Focal Versus Whole Gland Cryotherapy in a Matched Population. J. Endourol. 2015, 29, 1193–1198. [Google Scholar] [CrossRef] [PubMed]
- Tourinho-Barbosa, R.R.; Sanchez-Salas, R.; Claros, O.R.; Collura-Merlier, S.; Bakavicius, A.; Carneiro, A.; Stabile, A.; Moschini, M.; Cathala, N.; Tobias-Machado, M.; et al. Focal Therapy for Localized Prostate Cancer with Either High Intensity Focused Ultrasound or Cryoablation: A Single Institution Experience. J. Urol. 2020, 203, 320–330. [Google Scholar] [CrossRef]
- Blazevski, A.; Scheltema, M.J.; Yuen, B.; Masand, N.; Nguyen, T.V.; Delprado, W.; Shnier, R.; Haynes, A.-M.; Cusick, T.; Thompson, J.; et al. Oncological and Quality-of-life Outcomes Following Focal Irreversible Electroporation as Primary Treatment for Localised Prostate Cancer: A Biopsy-monitored Prospective Cohort. Eur. Urol. Oncol. 2020, 3, 283–290. [Google Scholar] [CrossRef] [PubMed]
- He, B.-M.; Xue, W.; Yan, W.-G.; Yin, L.; Dong, B.-J.; Zhou, Z.-E.; Lin, H.-Z.; Zhou, Y.; Wang, Y.-Q.; Shi, Z.-K.; et al. A Multicenter Single-Arm Objective Performance Criteria Trial to Determine the Efficacy and Safety of High-Frequency Irreversible Electroporation as Primary Treatment for Localized Prostate Cancer: A Study Protocol. Front. Oncol. 2021, 11, 760003. [Google Scholar] [CrossRef] [PubMed]
- Erinjeri, J.P.; Clark, T.W. Cryoablation: Mechanism of action and devices. J. Vasc. Interv. Radiol. 2010, 21, S187–S191. [Google Scholar] [CrossRef]
- Guenther, E.; Klein, N.; Zapf, S.; Weil, S.; Schlosser, C.; Rubinsky, B.; Stehling, M.K. Prostate cancer treatment with Irreversible Electroporation (IRE): Safety, efficacy and clinical experience in 471 treatments. PLoS ONE 2019, 14, e0215093. [Google Scholar] [CrossRef]
- Kumar, P.; Nagarajan, A.; Uchil, P.D. Electroporation. Cold Spring Harb. Protoc. 2019, 2019. [Google Scholar] [CrossRef]
- Simon, C.J.; Dupuy, D.E.; Mayo-Smith, W.W. Microwave ablation: Principles and applications. Radiographics 2005, 25, S69–S83. [Google Scholar] [CrossRef]
- Eastham, J.A.; Auffenberg, G.B.; Barocas, D.A.; Chou, R.; Crispino, T.; Davis, J.W.; Eggener, S.; Horwitz, E.M.; Kane, C.J.; Kirkby, E.; et al. Clinically localized prostate cancer: AUA/ASTRO guideline, Part I: Introduction, Risk Assessment, Staging, and Risk-Based Management. J. Urol. 2022, 208, 10–18. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Cryoablation | Study Year | Study Design | Stage/Grading | Type of Ablation | Biopsy | Imaging | Patients (n) | Primitive or Recurrence | Functional Outcomes | Oncological Outcomes | Complications | Disease-Free Survival | Overall Survival |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [9] | 2022 | Retrospective cohort study. | N/A. | WGC. | N/A. | N/A. | 260 | Primitive. | erectile dysfunction (1 post cryoablation vs. 7 before), 2 stress incontinence | BRFS 84%, FFS 66%, MFS 96%. | 2.3% Clavien—dindo > 2. | 84% BRFS. | N/A. |
| [10] | 2021 | Retrospective cohort study. | N/A. | WGC/hemi/focal. | N/A | N/A | 82 | Both. | no stress incontinence. Erectile dysfunction | FFS 5 years 75% (primary group), 40% (salvage group). | 1 fistula in the salvage group. | FFS 5 years 75% (primary group), 40% (salvage group). | N/A. |
| [11] | 2020 | Prospective observational trial. | N/A. | Hemigland. | Yes: 3, 6, 18 months. | MRI. | 61 | Primitive. | N/A | No CsPCa at 6 months MRGB for 82%. | No Clavien dindo > 2. | 82% RFS at 18 months. | N/A. |
| [12] | 2020 | Retrospective cohort study. | 2b. | Combination. | Sys and target. | mpMRI. | Hemi: 26. | Primitive. | Urinary incontinence 17% (1 year) in both groups; impotency 75% (WGC) 46% (HC) | 4y FFS 73%. | N/A. | N/A. | N/A. |
| [13] | 2023 | Retrospective cohort study. | All grades. | Focal. | PSA. | MRI. | 163 | Recurrence. | Urinary incontinence 1.8%; erectile dysfunction in 3.1% of patients. | BRFS 78%, 74%, and 55% for low, intermediate, and high-grade cancers. | N/A. | N/A. | N/A. |
| [14] | 2023 | Retrospective cohort study. | All grades. | Focal and hemi. | 30 days, then every 3 months for the first 2 years, every 6 months from the third to the 50th year, and once a year until the 10th year. | 110 | Primitive. | N/A. | BCS and TFS of 68.5% and 71.5%. | N/A. | N/A. | N/A. | |
| [15] | 2023 | Retrospective cohort study. | N/A. | Focal/hemi. | Biopsy at 2 year | MRI at 2 years. | 132 | Primitive. | N/A. | TFS in-field and out-of-field: 97% and 86%. | N/A. | TFS in-field and out-of-field: 97% and 86%. | N/A. |
| [16] | 2023 | Prospective cohort study | N/A. | Salvage focal ablation. | Biopsy | mpMRI. | 7 | Recurrence. | Erectile function was preserved. | 5/7 disease-free at the most recent MRI control. | N/A. | 5/7 disease-free at the most recent MRI control. | N/A. |
| [17] | 2023 | Retrospective cohort study. | N/A. | SWGC. | N/A. | N/A. | 110 | Primitive. | IIEF post cryoablation 1. Stress urinary incontinence post cryoablation (2%). | BRFS, FFS, and MFS at 10 years were 84%, 66%, and 96%, respectively. | Grade > 2 Clavien–Dindo adverse events: (2.3%) patients. | BRFS, FFS, and MFS at 10 years were 84%, 66%, and 96%, respectively. | N/A. |
| [18] | 2021 | Retrospective cohort study. | All grades. | WGC. | N/A. | N/A. | sCT = 186; sHIFU = 113; NST = 982. | Recurrence. | N/A. | N/A. | sCT: rectourethral fistulas (3%) and severe incontinence (7%). | CSS (p < 0.001) for CT. | OS (p < 0.001) for CT. |
| [19] | 2021 | Retrospective cohort study. | All grades. | WGC. | N/A. | MRI every 6–12 months. | 108 | Recurrence. | Group A: better clinical relief of urinary symptoms. | Reduced the risk of FFS by 45.8%. | Clavien—dindo Grade I: 13 (24.1%). | Reduced the risk of FFS by 45.8%. | No difference in the 2 groups. |
| [20] | 2021 | Prospective controlled trial. | GG 1–2. | Ipsilateral hemigland and contralateral anterior prostate. | 6, 18, 36 months. | 23 pt 6 month, 16 pt 18 months, 12 pt 36 months. | 23 | Primitive. | Sexual improvement after 6 months; 52% preserved urinary continence. | 8/23 (34.8%) positive out of field biopsy within 3 years. | N/A. | N/A. | N/A. |
| [21] | 2023 | Pilot study design. | Gleason 6 and 7. | Focal. | Day 1 with cryoablation. | 3 months and 1 year post-operative MRI. | N/A. | Primitive. | IIEF-5: 18/I-PSS score: 9. | At 3 months complete ablation index lesion, no signs of recurrence at 1 year. | N/A. | N/A. | N/A. |
| Irreversible Electroporation | |||||||||||||
| [22] | 2021 | Prospective cohort study. | GG 1–2. | IRE. | Biopsy (TTMB) at 12 mo. | MRI 12 months. | 50 | Primitive. | EPIC urinary or bowel QoL domain, decline in EPIC sexual QoL. | 2.5% residual disease at 12 mo. | No Clavien–Dindo grade 3 events or higher. | N/A. | N/A. |
| [23] | 2023 | Retrospective cohort study. | Intermediate–high risk. | IRE localized cancer. | 12 months biopsy. | MRI 6 months. | 229 | Primitive. | Erections sufficient for intercourse (71 to 58). Short-term urinary continence was preserved (99% 12 mo). | Kaplan–Meier FFS: 91% at 3 years, 84% at 5 years and 69% at 8 years. | N/A. | N/A. | PCa specific and overall survival were 100%. |
| [24] | 2023 | Prospective cohort study. | Low–intermediate. | IRE focal and extended. | 6 months. | N/A. | 106 (51 focal, 55 extended). | Primitive. | IIEF score and EPIC score was better in the focal group. | Rate of residual prostate cancer without significant difference in the 2 groups. | N/A. | N/A. | N/A. |
| [25] | 2023 | Retrospective cohort study. | ISUP 1–3 grade. | IRE focal. | 12 months biopsy. | MRI 6 months. | 45 | Both. | Quality of life (QoL) no significant changes; mild decrease in sexual QoL. | FFS at 3 years was 96.75%, metastasis free survival in 99% and overall survival 100%. | No Clavien–Dindo > 1 complications were reported. | FFS 3 years 91.3%. | OS 3 years 100%. |
| [26] | 2023 | Retrospective cohort study. | ISUP 1–2 grade. | IRE focal. | 12 months biopsy. | N/A. | 41 | Primitive. | All patients preserved urinary continence. Potency was maintained in 91.8%. | Recurrence was observed in 16 of 41 (39%) of the whole cohort. | N/A. | Median recurrence-free survival: 32 months (95% CI: 6.7–57.2). | N/A. |
| [27] | 2022 | Nonrandomized controlled trial—retrospective. | T2c or low, Gleason 7 or less. | Extended focal H-FIRE | 6 months biopsy. | MRI 1 and 6 months. | 109 | Primitive. | International Prostate Symptom Score was 4.5. International Index of Erectile Function 5 score was 2.0. | csPCa AT 6 mo 6.0% (95% CI, 2.2%–12.6%; p < 0.001; 1 in the treatment zone and 5 outside the treatment zone). | Clavien–Dindo grade I (33 cases), II (7 cases), III (1). | N/A. | N/A. |
| [28] | 2021 | Retrospective cohort study. | T2c or low. | Focal IRE | N/A. | 6 months MRI. | 10 | Primitive. | IIEF no significant changes; no new urinary incontinence developed. | 9/10 reduction of diffuse restriction at 6 months and PIRADS decrease. | N/A. | N/A. | N/A. |
| Microwave Ablation | |||||||||||||
| [29] | 2022 | Single-center, prospective, interventional phase 1–2 trial. | Grade group 1 and 2. | Focal lesion TMA. | PSA, IPSS, and IIEF5 1 w, 1, 3, 6 mo. Rebiopsy 6 mo. | MRI 5 mo. | 11 | Primitive. | IPSS (p = 0.39), or IIEF-5 scores (p = 0.18), no significant changes. | Necrosis of the index tumor on MRI 8/10. | No grade ≥ 2 complications were reported. | N/A. | N/A. |
| [30] | 2021 | Prospective cohort study. | Gleason score ≤ 3 + 4. | Focal microwave ablation. | Rebiopsy 6 mo. | MRI 7 days. | 10 | Primitive. | No significant change of median IPSS, IIEF-5, and MSHQ-EjD at 6-month | Total necrosis of the index tumor on MRI 8/10 at 7 days. | N/A. | N/A. | N/A. |
| [31] | 2022 | Single center prospective phase 2 trial. | ISUP grade 2. | Focal microwave ablation. | Biopsy 5 months. | MRI 5 months. | 15 men, 23 areas. | Primitive. | urinary symptoms, uroflowmetry, erectile function, and QOL scores. No significant difference at 6 months. | At 6 months 91.3% (21/23) no cancer; per-patient analysis 33.3% (5/15) positive. | Grade 1 complications: hematuria (33.3%), dysuria (6.7%), and perineal discomfort (13.4%). | N/A. | N/A. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faiella, E.; Santucci, D.; D’Amone, G.; Cirimele, V.; Vertulli, D.; Bruno, A.; Beomonte Zobel, B.; Grasso, R.F. Focal Minimally Invasive Treatment in Localized Prostate Cancer: Comprehensive Review of Different Possible Strategies. Cancers 2024, 16, 765. https://doi.org/10.3390/cancers16040765
Faiella E, Santucci D, D’Amone G, Cirimele V, Vertulli D, Bruno A, Beomonte Zobel B, Grasso RF. Focal Minimally Invasive Treatment in Localized Prostate Cancer: Comprehensive Review of Different Possible Strategies. Cancers. 2024; 16(4):765. https://doi.org/10.3390/cancers16040765
Chicago/Turabian StyleFaiella, Eliodoro, Domiziana Santucci, Giulia D’Amone, Vincenzo Cirimele, Daniele Vertulli, Amalia Bruno, Bruno Beomonte Zobel, and Rosario Francesco Grasso. 2024. "Focal Minimally Invasive Treatment in Localized Prostate Cancer: Comprehensive Review of Different Possible Strategies" Cancers 16, no. 4: 765. https://doi.org/10.3390/cancers16040765
APA StyleFaiella, E., Santucci, D., D’Amone, G., Cirimele, V., Vertulli, D., Bruno, A., Beomonte Zobel, B., & Grasso, R. F. (2024). Focal Minimally Invasive Treatment in Localized Prostate Cancer: Comprehensive Review of Different Possible Strategies. Cancers, 16(4), 765. https://doi.org/10.3390/cancers16040765