
Prognostic Factors and Nomogram for Choroid Plexus Tumors: A Population-Based Retrospective Surveillance, Epidemiology, and End Results Database Analysis

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Cohort Selection
2.2. Statistical Analyses
3. Results
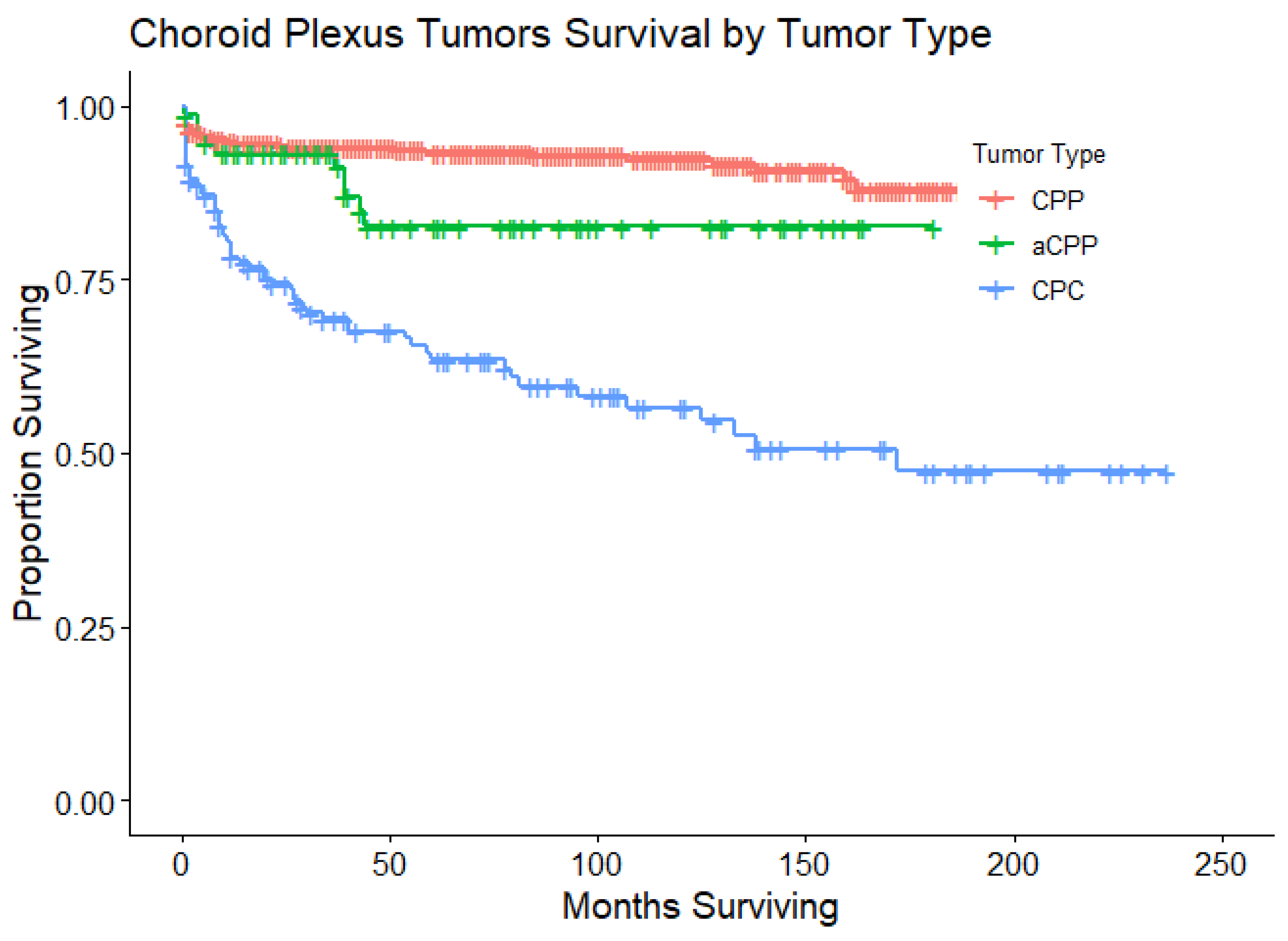
3.1. Overall Cohort Survival Statistics
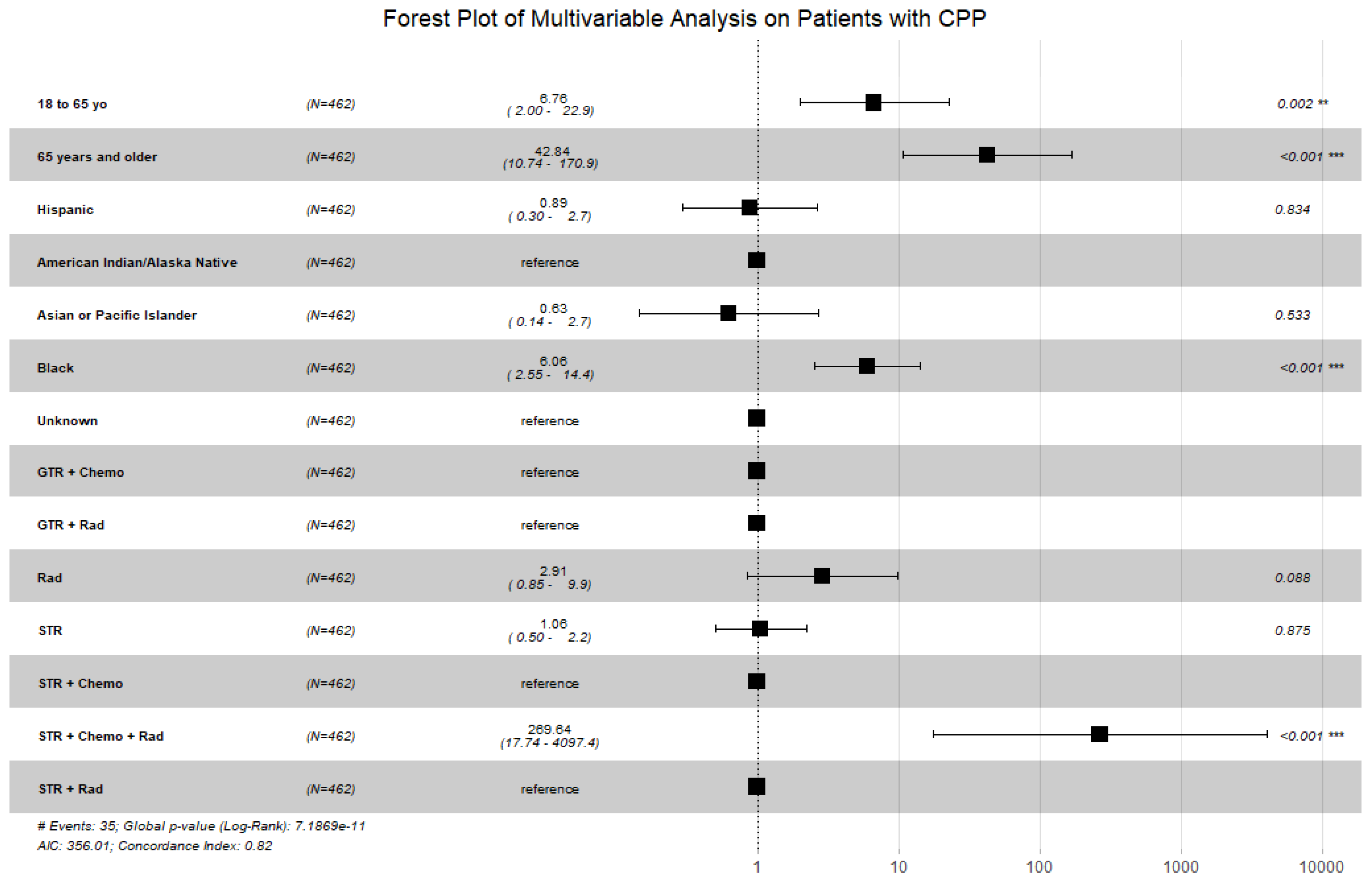
3.2. Choroid Plexus Papilloma
3.3. Atypical Choroid Plexus Papilloma
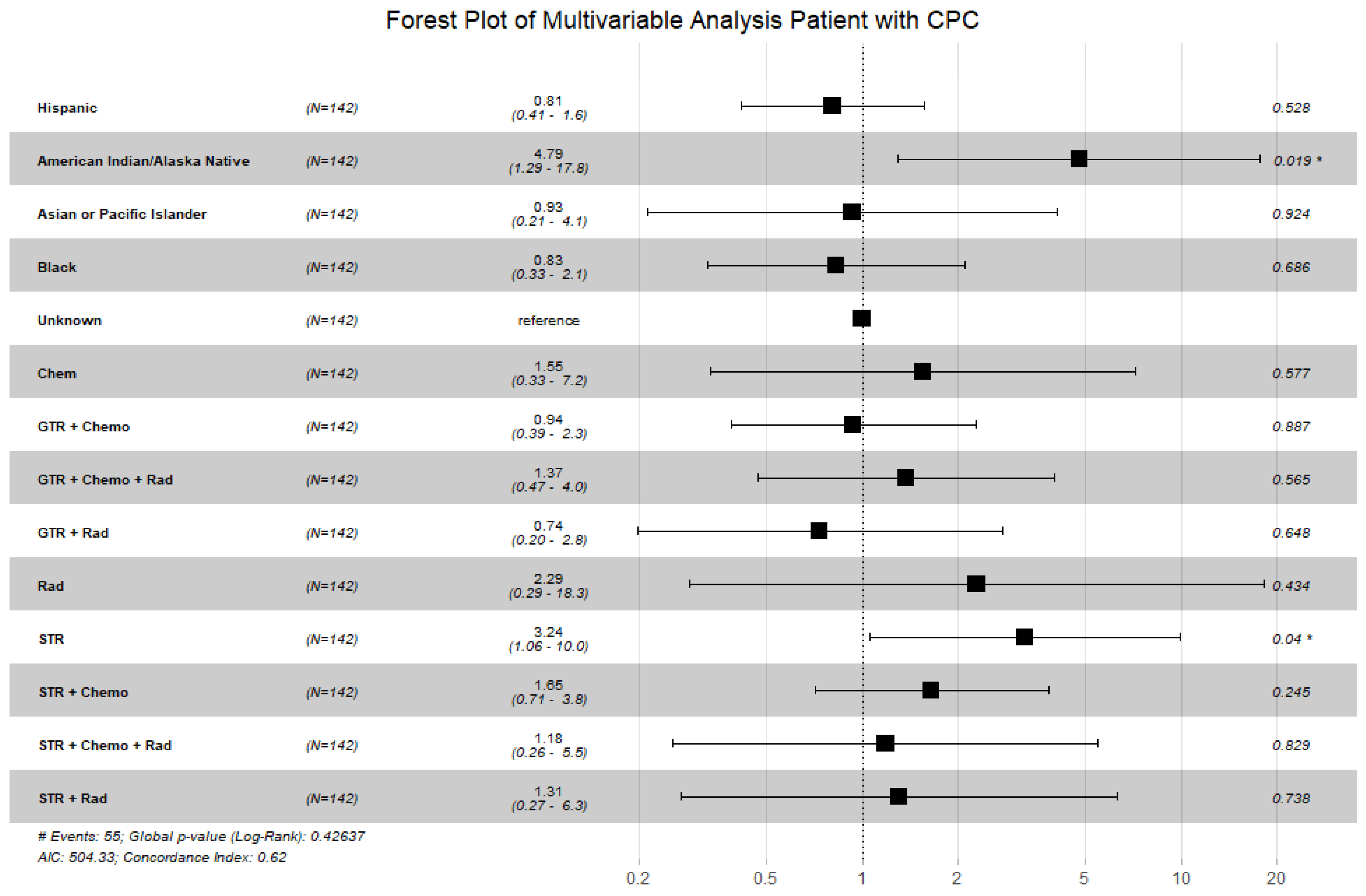
3.4. Choroid Plexus Carcinoma
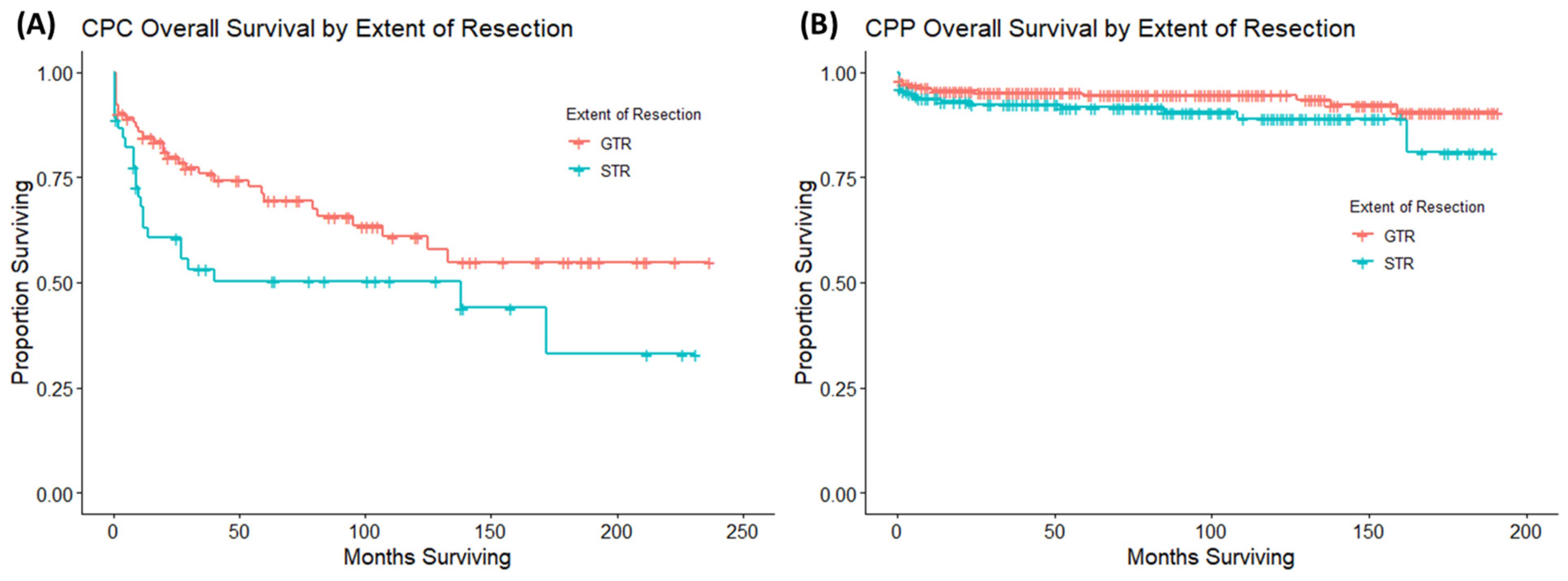
3.5. Gross Total Resection Versus Subtotal Resection
3.6. Nomogram
4. Discussion
4.1. Choroid Plexus Papilloma
4.2. Choroid Plexus Carcinoma
4.3. Nomogram
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bettegowda, C.; Adogwa, O.; Mehta, V.; Chaichana, K.L.; Weingart, J.; Carson, B.S.; Jallo, G.I.; Ahn, E.S. Treatment of choroid plexus tumors: A 20-year single institutional experience. J. Neurosurg. Pediatr. 2012, 10, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Asai, A.; Hoffman, H.J.; Hendrick, E.B.; Humphreys, R.P.; Becker, L.E. Primary intracranial neoplasms in the first year of life. Childs Nerv. Syst. 1989, 5, 230–233. [Google Scholar] [CrossRef] [PubMed]
- Jooma, R.; Hayward, R.D.; Grant, N.D. Intracranial neoplasms during the first year of life: Analysis of one hundred consecutive cases. Neurosurgery 1984, 14, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Lafay-Cousin, L.; Mabbott, D.J.; Halliday, W.; Taylor, M.D.; Tabori, U.; Kamaly-Asl, I.D.; Kulkarni, A.V.; Bartels, U.; Greenberg, M.; Bouffet, E. Use of ifosfamide, carboplatin, and etoposide chemotherapy in choroid plexus carcinoma. J. Neurosurg. Pediatr. 2010, 5, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Emerich, D.F.; Skinner, S.J.; Borlongan, C.V.; Vasconcellos, A.V.; Thanos, C.G. The choroid plexus in the rise, fall and repair of the brain. Bioessays 2005, 27, 262–274. [Google Scholar] [CrossRef]
- Wolburg, H.; Paulus, W. Choroid plexus: Biology and pathology. Acta Neuropathol. 2010, 119, 75–88. [Google Scholar] [CrossRef]
- Torp, S.H.; Solheim, O.; Skjulsvik, A.J. The WHO 2021 Classification of Central Nervous System tumours: A practical update on what neurosurgeons need to know-a minireview. Acta Neurochir. 2022, 164, 2453–2464. [Google Scholar] [CrossRef]
- Lozier, A.P.; Arbaje, Y.M.; Scheithauer, B.W. Supratentorial, extraventricular choroid plexus carcinoma in an adult: Case report. Neurosurgery 2009, 65, E816–E817. [Google Scholar] [CrossRef]
- Wolff, J.E.; Sajedi, M.; Brant, R.; Coppes, M.J.; Egeler, R.M. Choroid plexus tumours. Br. J. Cancer 2002, 87, 1086–1091. [Google Scholar] [CrossRef]
- McCall, T.; Binning, M.; Blumenthal, D.T.; Jensen, R.L. Variations of disseminated choroid plexus papilloma: 2 case reports and a review of the literature. Surg. Neurol. 2006, 66, 62–67; discussion 67–68. [Google Scholar] [CrossRef]
- Wrede, B.; Hasselblatt, M.; Peters, O.; Thall, P.F.; Kutluk, T.; Moghrabi, A.; Mahajan, A.; Rutkowski, S.; Diez, B.; Wang, X.; et al. Atypical choroid plexus papilloma: Clinical experience in the CPT-SIOP-2000 study. J. Neurooncol. 2009, 95, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef]
- Duffner, P.K.; Kun, L.E.; Burger, P.C.; Horowitz, M.E.; Cohen, M.E.; Sanford, R.A.; Krischer, J.P.; Mulhern, R.K.; James, H.E.; Rekate, H.L.; et al. Postoperative chemotherapy and delayed radiation in infants and very young children with choroid plexus carcinomas. The Pediatric Oncology Group. Pediatr. Neurosurg. 1995, 22, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.E.; Sajedi, M.; Coppes, M.J.; Anderson, R.A.; Egeler, R.M. Radiation therapy and survival in choroid plexus carcinoma. Lancet 1999, 353, 2126. [Google Scholar] [CrossRef]
- Fitzpatrick, L.K.; Aronson, L.J.; Cohen, K.J. Is there a requirement for adjuvant therapy for choroid plexus carcinoma that has been completely resected? J. Neurooncol. 2002, 57, 123–126. [Google Scholar] [CrossRef]
- Martin, B.; Garman, T.; Laramee, M.; Wang, A.; Zhang, X.; Beck, E.; Wilson, K.; Klumpp-Thomas, C.; McKnight, C.; Xu, X.; et al. Preclinical validation of a novel therapeutic strategy for choroid plexus carcinoma. J. Control. Release 2023, 357, 580–590. [Google Scholar] [CrossRef] [PubMed]
- Schell, T.D.; Tevethia, S.S. Control of advanced choroid plexus tumors in SV40 T antigen transgenic mice following priming of donor CD8(+) T lymphocytes by the endogenous tumor antigen. J. Immunol. 2001, 167, 6947–6956. [Google Scholar] [CrossRef]
- Cannon, D.M.; Mohindra, P.; Gondi, V.; Kruser, T.J.; Kozak, K.R. Choroid plexus tumor epidemiology and outcomes: Implications for surgical and radiotherapeutic management. J. Neurooncol. 2015, 121, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.; Lin, Y.; Cherian, J.; Qadri, U.; Harris, D.A.; Melkonian, S.; Jea, A. Choroid plexus tumors in children: A population-based study. Pediatr. Neurosurg. 2013, 49, 331–338. [Google Scholar] [CrossRef]
- Liu, Q.; Leisenring, W.M.; Ness, K.K.; Robison, L.L.; Armstrong, G.T.; Yasui, Y.; Bhatia, S. Racial/Ethnic Differences in Adverse Outcomes Among Childhood Cancer Survivors: The Childhood Cancer Survivor Study. J. Clin. Oncol. 2016, 34, 1634–1643. [Google Scholar] [CrossRef] [PubMed]
- Curry, W.T., Jr.; Carter, B.S.; Barker, F.G., 2nd. Racial, ethnic, and socioeconomic disparities in patient outcomes after craniotomy for tumor in adult patients in the United States, 1988–2004. Neurosurgery 2010, 66, 427–437; discussion 437–438. [Google Scholar] [CrossRef] [PubMed]
- Curry, W.T., Jr.; Barker, F.G., 2nd. Racial, ethnic and socioeconomic disparities in the treatment of brain tumors. J. Neurooncol. 2009, 93, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, S. Influence of race and socioeconomic status on outcome of children treated for childhood acute lymphoblastic leukemia. Curr. Opin. Pediatr. 2004, 16, 9–14. [Google Scholar] [CrossRef]
- Krishnan, S.; Brown, P.D.; Scheithauer, B.W.; Ebersold, M.J.; Hammack, J.E.; Buckner, J.C. Choroid plexus papillomas: A single institutional experience. J. Neurooncol. 2004, 68, 49–55. [Google Scholar] [CrossRef]
- Berger, C.; Thiesse, P.; Lellouch-Tubiana, A.; Kalifa, C.; Pierre-Kahn, A.; Bouffet, E. Choroid plexus carcinomas in childhood: Clinical features and prognostic factors. Neurosurgery 1998, 42, 470–475. [Google Scholar] [CrossRef]
- Wolff, J.E.; Van Gool, S.W.; Kutluk, T.; Diez, B.; Kebudi, R.; Timmermann, B.; Garami, M.; Sterba, J.; Fuller, G.N.; Bison, B.; et al. Final results of the Choroid Plexus Tumor study CPT-SIOP-2000. J. Neurooncol. 2022, 156, 599–613. [Google Scholar] [CrossRef] [PubMed]
- Tabori, U.; Shlien, A.; Baskin, B.; Levitt, S.; Ray, P.; Alon, N.; Hawkins, C.; Bouffet, E.; Pienkowska, M.; Lafay-Cousin, L.; et al. TP53 alterations determine clinical subgroups and survival of patients with choroid plexus tumors. J. Clin. Oncol. 2010, 28, 1995–2001. [Google Scholar] [CrossRef]
- Adhikari, S.; Bhutada, A.S.; Ladner, L.; Cuoco, J.A.; Entwistle, J.J.; Marvin, E.A.; Rogers, C.M. Prognostic indicators for H3K27M-mutant diffuse midline glioma: A population-based retrospective Surveillance, Epidemiology, and End Results database analysis. World Neurosurg. 2023, 178, e113–e121. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CPP (n = 462) | aCPP (n = 75) | CPC (n = 142) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Category | Subcategory | Number of Patients | Percentage | Deaths | Number of Patients | Percentage | Deaths | Number of Patients | Percentage | Deaths |
| Sex | Female | 239 | 52 | 15 | 34 | 43 | 6 | 57 | 40 | 23 |
| Male | 223 | 48 | 20 | 41 | 52 | 3 | 85 | 60 | 32 | |
| Age | [0–18] | 213 | 46 | 4 | 45 | 57 | 3 | 113 | 143 | 44 |
| (18–65] | 220 | 48 | 20 | 29 | 37 | 5 | 29 | 37 | 11 | |
| >65 | 29 | 6 | 11 | 1 | 1 | 1 | 0 | 0 | 0 | |
| Race | Non-Hispanic White | 270 | 58 | 20 | 48 | 61 | 6 | 76 | 54 | 30 |
| Hispanic (all races) | 117 | 25 | 4 | 21 | 27 | 2 | 40 | 28 | 14 | |
| Non-Hispanic American Indian/Alaska Native | 3 | 1 | 0 | 0 | 0 | 0 | 3 | 2 | 3 | |
| Non-Hispanic Asian or Pacific Islander | 33 | 7 | 3 | 2 | 3 | 0 | 7 | 5 | 2 | |
| Non-Hispanic Black | 29 | 6 | 8 | 4 | 5 | 1 | 13 | 9 | 6 | |
| Unknown | 10 | 2 | 0 | 0 | 0 | 0 | 3 | 2 | 0 | |
| Year of diagnosis | 2000–2005 | 59 | 13 | 7 | 5 | 6 | 2 | 45 | 32 | 24 |
| 2006–2010 | 145 | 31 | 14 | 23 | 29 | 6 | 30 | 21 | 13 | |
| 2010–2015 | 149 | 32 | 9 | 21 | 27 | 1 | 38 | 27 | 11 | |
| 2015–2019 | 109 | 24 | 5 | 26 | 33 | 0 | 29 | 20 | 7 | |
| Tumor Size (cm) | <3 | 204 | 44 | 13 | 23 | 29 | 3 | 19 | 13 | 4 |
| >3.0 | 154 | 33 | 9 | 40 | 51 | 6 | 81 | 57 | 27 | |
| Unknown | 104 | 23 | 13 | 12 | 15 | 0 | 42 | 30 | 24 | |
| Treatment | GTR | 273 | 59 | 16 | 46 | 58 | 5 | 30 | 20 | 10 |
| Chemo | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 3 | 2 | |
| GTR + Chemo | 1 | 0 | 0 | 1 | 1 | 1 | 39 | 26 | 11 | |
| GTR + Chemo + Rad | 0 | 0 | 0 | 0 | 0 | 0 | 11 | 7 | 6 | |
| GTR + Rad | 3 | 1 | 0 | 0 | 0 | 0 | 12 | 8 | 3 | |
| Rad | 6 | 1 | 4 | 23 | 29 | 3 | 1 | 1 | 1 | |
| STR | 172 | 37 | 14 | 2 | 3 | 0 | 8 | 5 | 5 | |
| STR + Chemo | 2 | 0 | 0 | 0 | 0 | 0 | 27 | 18 | 13 | |
| STR + Chemo + Rad | 1 | 0 | 1 | 2 | 3 | 0 | 6 | 4 | 2 | |
| STR + Rad | 4 | 1 | 0 | 0 | 0 | 0 | 4 | 3 | 2 | |
| Chemo + Rad | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | |
| CPP (n = 462) | aCPP (n = 75) | CPC (n = 142) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Category | Subcategory | HR | 95% CI | p-Value | HR | 95% CI | p-value | HR | 95% CI | p-Value |
| Sex | Female | reference | 0.3 | reference | 0.4 | reference | 0.9 | |||
| Male | 1.46 | [0.75–2.86] | 0.52 | [0.13–2.12] | 1.04 | [0.61–1.78] | ||||
| Age | [0–18] | reference | 5.00 × 10−15 | reference | 0.01 | reference | 0.7 | |||
| (18–65] | 5.24 | [1.79–15.4] | ** | 2.36 | [0.56–9.91] | 0.87 | [0.45–170] | |||
| >65 | 31.1 | [9.74–99.3] | *** | 16.1 | [1.61–160] | ** | NA | NA | ||
| Race | Non-Hispanic White | reference | 1.00 × 10−3 | reference | 0.8 | reference | 0.02 | |||
| Hispanic (all races) | 0.5 | [0.17–1.47] | 0.81 | [0.16–4.01] | 0.76 | [0.40–1.44] | ||||
| Non-Hispanic American Indian/Alaska Native | NA | NA | NA | NA | 5.38 | [1.60–18.1] | ** | |||
| Non-Hispanic Asian or Pacific Islander | 1.28 | [0.38–4.33] | NA | NA | 0.81 | [0.19–3.39] | ||||
| Non-Hispanic Black | 3.99 | [1.76–9.07] | *** | 2.22 | [0.27–18.5] | 0.89 | [0.36–2.14] | |||
| Unknown | NA | NA | NA | NA | NA | NA | ||||
| Year of diagnosis | 2000–2005 | reference | 1 | reference | 0.06 | reference | 0.8 | |||
| 2006–2010 | 1.01 | [0.39–2.63] | 0.59 | [0.12–2.96] | 0.81 | [0.41–1.61] | ||||
| 2010–2015 | 0.9 | [0.31–2.66] | 0.1 | [0.01–1.17] | 0.69 | [0.33–1.44] | ||||
| 2015–2019 | 0.93 | [0.26–3.23] | NA | NA | 0.93 | [0.38–2.24] | ||||
| Tumor Size (cm) | <3 | reference | 0.3 | reference | 0.3 | reference | 0.2 | |||
| >3.0 | 0.97 | [0.41–2.27] | 1.49 | [0.37–5.98] | 1.8 | [0.63–5.14] | ||||
| Unknown | 1.64 | [0.76–3.56] | NA | NA | 2.52 | [0.87–7.29] | ||||
| Treatment | GTR | reference | 5.00 × 10−10 | reference | 0.1 | reference | 0.4 | |||
| Chemo | NA | NA | NA | NA | 1.57 | [0.34–7.26] | ||||
| GTR + Chemo | NA | NA | 11.5 | [1.28–103] | * | 0.92 | [0.39–2.21] | |||
| GTR + Chemo + Rad | NA | NA | NA | NA | 1.66 | [0.60–4.61] | ||||
| GTR + Rad | NA | NA | NA | NA | 0.73 | [0.20–2.66] | ||||
| Rad | 15.6 | [5.15–47.7] | *** | NA | NA | 2.47 | [0.31–19.5] | |||
| STR | 1.57 | [0.76–3.23] | 1.59 | [0.38–6.71] | 3.26 | [1.11–9.59] | * | |||
| STR + Chemo | NA | NA | NA | NA | 1.68 | [0.73–3.86] | ||||
| STR + Chemo + Rad | 28.6 | [3.70–220] | *** | NA | NA | 1.11 | [0.24–5.08] | |||
| STR + Rad | NA | NA | NA | NA | 1.81 | [0.39–8.32] | ||||
| Chemo + Rad | NA | NA | NA | NA | NA | NA | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhutada, A.S.; Adhikari, S.; Cuoco, J.A.; In, A.; Rogers, C.M.; Jane, J.A., Jr.; Marvin, E.A. Prognostic Factors and Nomogram for Choroid Plexus Tumors: A Population-Based Retrospective Surveillance, Epidemiology, and End Results Database Analysis. Cancers 2024, 16, 610. https://doi.org/10.3390/cancers16030610
Bhutada AS, Adhikari S, Cuoco JA, In A, Rogers CM, Jane JA Jr., Marvin EA. Prognostic Factors and Nomogram for Choroid Plexus Tumors: A Population-Based Retrospective Surveillance, Epidemiology, and End Results Database Analysis. Cancers. 2024; 16(3):610. https://doi.org/10.3390/cancers16030610
Chicago/Turabian StyleBhutada, Abhishek S., Srijan Adhikari, Joshua A. Cuoco, Alexander In, Cara M. Rogers, John A. Jane, Jr., and Eric A. Marvin. 2024. "Prognostic Factors and Nomogram for Choroid Plexus Tumors: A Population-Based Retrospective Surveillance, Epidemiology, and End Results Database Analysis" Cancers 16, no. 3: 610. https://doi.org/10.3390/cancers16030610
APA StyleBhutada, A. S., Adhikari, S., Cuoco, J. A., In, A., Rogers, C. M., Jane, J. A., Jr., & Marvin, E. A. (2024). Prognostic Factors and Nomogram for Choroid Plexus Tumors: A Population-Based Retrospective Surveillance, Epidemiology, and End Results Database Analysis. Cancers, 16(3), 610. https://doi.org/10.3390/cancers16030610