
Pain Catastrophizing in Cancer Patients





Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Measurements
2.2. Statistics
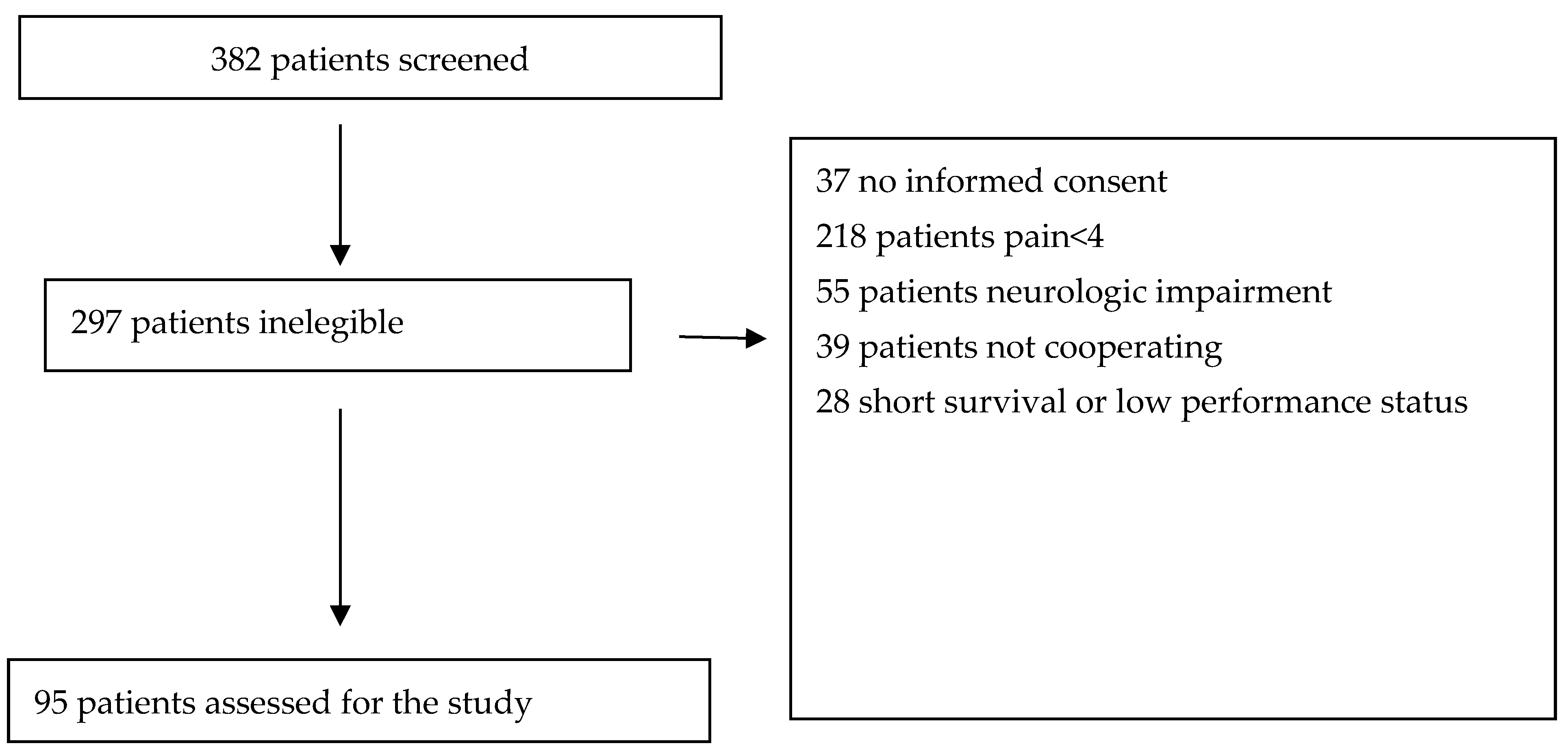
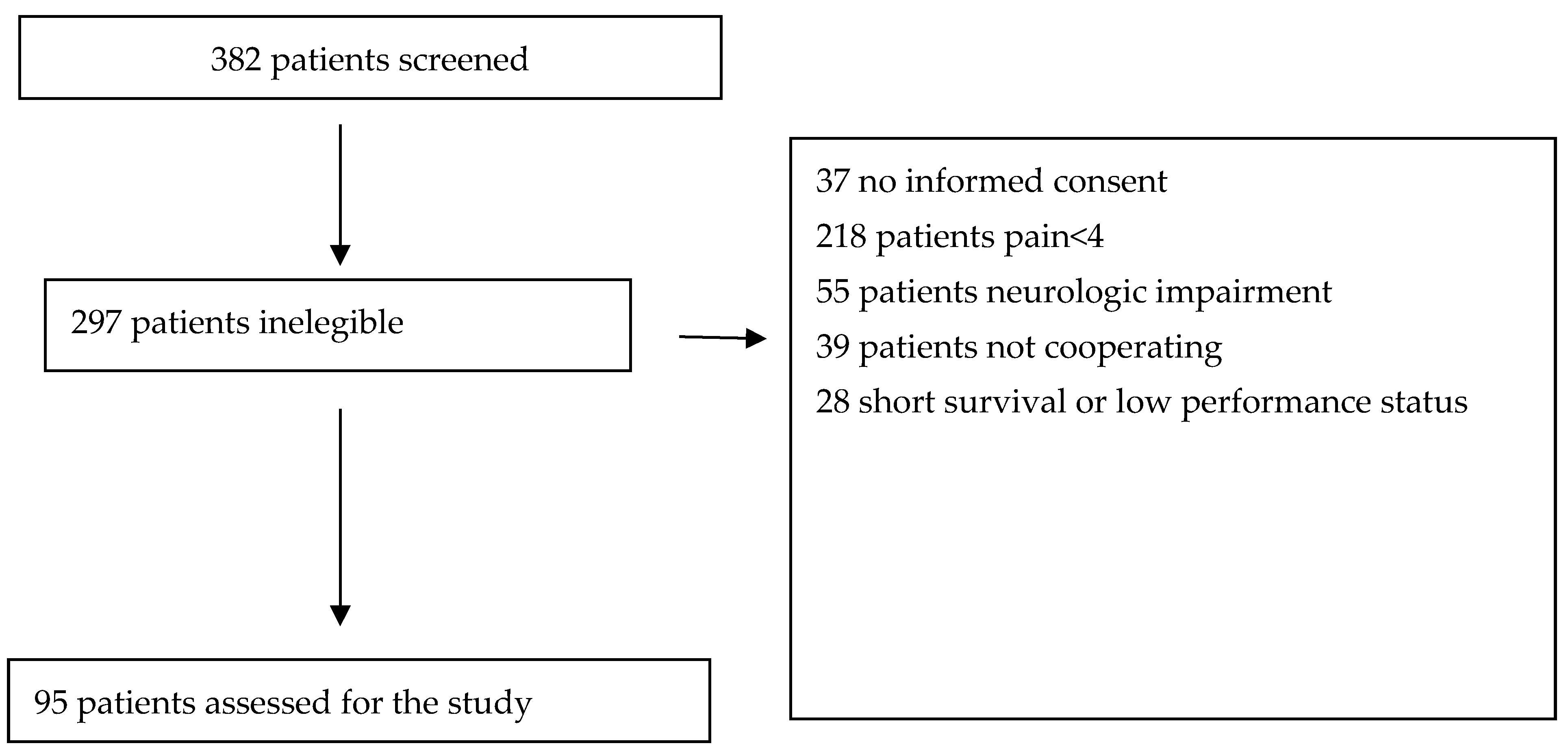
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Snijders, R.A.H.; Brom LTheunissen M van den Beuken-van Everdingen, M.H.J. Update on Prevalence of Pain in Patients with Cancer 2022: A Systematic Literature Review and Meta-Analysis. Cancers 2023, 15, 591. [Google Scholar] [CrossRef] [PubMed]
- Bruera, E. Relieving physical and psychosocial pain in patients with cancer—The search for enlightened academic medical leaders. JAMA Oncol. 2019, 5, 1401–1402. [Google Scholar] [CrossRef]
- Gorin, S.S.; Krebs, P.; Badr, H.; Janke, E.A.; Jim, H.S.; Spring, B.; Mohr, D.C.; Berendsen, M.A.; Jacobsen, P.B. Meta-analysis of psychosocial interventions to reduce pain in patients with cancer. J. Clin. Oncol. 2012, 30, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Syrjala, K.L.; Jensen, M.P.; Mendoza, M.E.; Yi, J.C.; Fisher, H.M.; Keefe, F.J. Psychological and Behavioral Approaches to Cancer Pain Management. J. Clin. Oncol. 2014, 32, 1703–1711. [Google Scholar] [CrossRef] [PubMed]
- Azizoddin, D.R.; Schreiber, K.; Beck, M.R.; Enzinger, A.C.; Hruschak, V.; Darnall, B.D.; Edwards, R.R.; Allsop, M.J.; Tulsky, J.A.; Boyer, E.; et al. Chronic pain severity, impact, and opioid use among patients with cancer: An analysis of biopsychosocial factors using the CHOIR learning health care system. Cancer 2021, 127, 3254–3263. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.J.; Lynch, M.E.; Clark, A.J. Dimensions of catastrophic thinking associated with pain experience and disability in patients with neuropathic pain conditions. Pain 2005, 113, 310–315. [Google Scholar] [CrossRef]
- Wilson, J.M.; Schreiber, K.L.; Mackey, S.; Flowers, K.M.; Darnall, B.D.; Edwards, R.R.; Azizoddin, D.R. Increased pain catastrophizing longitudinally predicts worsened pain severity and interference in patients with chronic pain and cancer: A collaborative health outcomes information registry study (CHOIR). Psychooncology 2022, 31, 1753–1761. [Google Scholar] [CrossRef]
- Elphinston, R.A.; Sullivan, M.J.; Sterling, M.; Connor, J.P.; Baranoff, J.A.; Tan, D.; Day, M.A. Pain Medication Beliefs Mediate the Relationship Between Pain Catastrophizing and Opioid Prescription Use in Patients with Chronic Non-Cancer Pain. J. Pain 2022, 23, 379–389. [Google Scholar] [CrossRef]
- Hui, D.; Bruera, E. The Edmonton Symptom Assessment System 25 Years Later: Past, Present, and Future Developments. J. Pain Symptom Manag. 2017, 53, 630–643. [Google Scholar] [CrossRef]
- Dalal, S.; Hui, D.; Nguyen, L.; Chacko, R.; Scott, C.; Roberts, L.; Bruera, E. Achievement of personalized pain goal in cancer patients referred to a supportive care clinic at a comprehensive cancer center. Cancer 2012, 118, 3869–3877. [Google Scholar] [CrossRef]
- Hui, D.; Shamieh, O.; Paiva, C.E.; Perez-Cruz, P.E.; Kwon JHMuckaden, M.A.; Park, M.; Yennu, S.; Kang, J.H.; Bruera, E. Minimal clinically important differences in the Edmonton Symptom Assessment Scale in cancer patients: A prospective, multicenter study. Cancer 2015, 121, 3027–3035. [Google Scholar] [CrossRef]
- Hui, D.; Park, M.; Shamieh, O.; Paiva, C.E.; Perez-Cruz, P.E.; Muckaden, M.A.; Bruera, E. Personalized symptom goals and response in patients with advanced cancer. Cancer 2016, 122, 1774–1781. [Google Scholar] [CrossRef]
- Mercadante, S.; Adile, C.; Lanzetta, G.; Mystakidou, K.; Maltoni, M.; Soares, L.G.; De Santis, S.; Ferrera, P.; Valenti, M.; Rosati, M.; et al. Personalized Symptom Goals and Patient Global Impression on Clinical Changes in Advanced Cancer Patients. Oncologist 2019, 24, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, S.; Adile, C.; Aielli, F.; Gaetano, L.; Mistakidou, K.; Maltoni, M.; Soares, L.G.; DeSantis, S.; Ferrera, P.; Rosati, M.; et al. Personalized Pain Goals and Responses in Advanced Cancer Patients. Pain Med. 2020, 21, e215–e221. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, S.; Coluzzi, F. Factors Influencing Pain Expression in Patients with Cancer: An Expert Opinion. Pain Ther. 2021, 10, 765–775. [Google Scholar] [CrossRef] [PubMed]
- Bedard, G.; Zeng, L.; Zhang, L.; Lauzon, N.; Holden, L.; Tsao, M.; Danjoux, C.; Barnes, E.; Sahgal, A.; Poon, M.; et al. Minimal Clinically Important Differences in the Edmonton Symptom Assessment System in Patients with Advanced Cancer. J. Pain Symptom Manag. 2013, 46, 192–200. [Google Scholar] [CrossRef]
- Lauridsen, H.H.; Hartvigsen, J.; Manniche, C.; Korsholm, L.; Grunnet-Nilsson, N. Responsiveness and minimal clinically important difference for pain and disability instruments in low back pain patients. BMC Musculoskelet. Disord. 2006, 7, 82. [Google Scholar] [CrossRef]
- Mercadante, S.; Ferrera, P.; Villari, P.; Casuccio, A.; Intravaia, G.; Mangione, S. Frequency, Indications, Outcomes, and Predictive Factors of Opioid Switching in an Acute Palliative Care Unit. J. Pain Symptom Manag. 2009, 37, 632–641. [Google Scholar] [CrossRef]
- Bruera, E.; Kuehn, N.; Miller, M.J.; Selmser, P.; Macmillan, K. The Edmonton Symptom Assessment System (ESAS): A Simple Method for the Assessment of Palliative Care Patients. J. Palliat. Care 1991, 7, 6–9. [Google Scholar] [CrossRef]
- Sullivan, M.; Bishop, S.R.; Pivik, J. The pain catastrophizing scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Hayashi, K.; Ikemoto, T.; Shiro, Y.; Arai, Y.-C.; Marcuzzi, A.; Costa, D.; Wrigley, P.J. A Systematic Review of the Variation in Pain Catastrophizing Scale Reference Scores Based on Language Version and Country in Patients with Chronic Primary (Non-specific) Pain. Pain Ther. 2022, 11, 753–769. [Google Scholar] [CrossRef]
- Majumder, M.S.M.; Ahmed, S.; Shazzad, N.; Hasan, A.T.M.T.; Haq, S.A.; Rasker, J.J. Translation, cross-cultural adaptation and validation of the Pain Catastrophizing Scale (PCS) into Bengali in patients with chronic non-malignant musculoskeletal pain. Int. J. Rheum. Dis. 2020, 23, 1481–1487. [Google Scholar] [CrossRef]
- Van Damme, S.; Crombez, G.; Bijttebier, P.; Goubert, L.; Van Houdenhove, B. A confirmatory factor analysis of the pain catastrophizing scale: Invariant factor structure across clinical and non-clinical populations. Pain 2002, 96, 319–324. [Google Scholar] [CrossRef]
- Wheeler, C.H.; Williams, A.C.d.C.; Morley, S.J. Meta-analysis of the psychometric properties of the Pain Catastrophizing Scale and associations with participant characteristics. Pain 2019, 160, 1946–1953. [Google Scholar] [CrossRef]
- Available online: https://www.strobe-statement.org (accessed on 11 December 2023).
- Qian, Y.; Haider, A.; Lu, Z.; Naqvi, S.; Zhuang, A.; Nguyen, K.; Reddy, A.; Arthur, J.; Tanco, K.; Williams, J.; et al. Factors Associated with Improvement in Uncontrolled Cancer Pain without Increasing the Opioid Daily Dose among Patients Seen by an Inpatient Palliative Care Team. J. Palliat. Med. 2020, 23, 483–488. [Google Scholar] [CrossRef]
- Quartana, P.J.; Campbell, C.M.; Edwards, R.R. Pain catastrophizing: A critical review. Expert Rev. Neurother. 2009, 9, 745–758. [Google Scholar] [CrossRef]
- Martinez-Calderon, J.; Jensen, M.P.; Morales-Asencio, J.M.; Luque-Suarez, A. Pain Catastrophizing and Function in Individuals with Chronic Musculoskeletal Pain. Clin. J. Pain 2019, 35, 279–293. [Google Scholar] [CrossRef]
- Brown, L.F.; Kroenke, K.; Theobald, D.E.; Wu, J.; Tu, W. The association of depression and anxiety with health-related quality of life in cancer patients with depression and/or pain. Psychooncology 2010, 19, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Guay, M.; Parsons, H.A.; Li ZPalmer, J.L.; Bruera, E. Symptom distress in advanced cancer patients with anxiety and depression in the palliative care setting. Support. Care Cancer 2009, 17, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, P.; Lo, C.; Li, M.; Gagliese, L.; Zimmermann, C.; Rodin, G. The relationship between depression and physical symptom burden in advanced cancer. BMJ Support. Palliat. Care 2013, 5, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Grotmol, K.S.; Lie, H.C.; Loge, J.H.; Aass, N.; Haugen, D.F.; Stone, P.C.; Kaasa, S.; Hjermstad, M.J. Patients with advanced cancer and depression report a significantly higher symptom burden than non-depressed patients. Palliat. Support. Care 2018, 17, 143–149. [Google Scholar] [CrossRef]
- Lloyd-Williams, M.; Shiels, C.; Taylor, F.; Dennis, M. Depression—An independent predictor of early death in patients with advanced cancer. J. Affect. Disord. 2009, 113, 127–132. [Google Scholar] [CrossRef]
- O’Connor, M.; Weir, J.; Butcher, I.; Kleiboer, A.; Murray, G.; Sharma, G.; Thekkumpurath, P.; Walker, J.; Fallon, M.; Storey, D.J.; et al. Pain in patients attending a specialist cancer service: Prevalence and association with emotional distress. J. Pain Symptom Manag. 2012, 43, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, S.; Adile, A.; Ferrera, P.; Cortegiani, A.; Casuccio, A. Symptom hyper-expression in advanced cancer patients with anxiety and depression admitted to an acute supportive/palliative care unit. Support. Care Cancer 2019, 27, 3081–3088. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Overall N° 95 | PCS < 30; N° 57 | PCS ≥ 30; N° 38 | p | |
|---|---|---|---|---|
| Age (years, mean, ±SD) | 61.9 (11.5) | 62.2(11.1) | 61.4(12.1) | 0.753 |
| Gender (female/male) | 53/42 | 32/25 | 21/17 | 0.933 |
| Karnofsky (mean SD) | 53.9 (9.0) | 53.9(9.2) | 53.9(8.8) | 0.963 |
| Primary tumor N° | ||||
| Gastrointestinal | 29 | 21 | 8 | |
| Breast | 23 | 12 | 11 | |
| Lung | 23 | 15 | 8 | 0.338 |
| Genitourinary | 14 | 6 | 8 | |
| Others | 6 | 3 | 3 | |
| Education N° | ||||
| No education | 1 | 1 | 0 | |
| Primary | 22 | 14 | 8 | 0.964 |
| Secondary school | 39 | 22 | 17 | |
| High school | 24 | 15 | 9 | |
| Degree | 9 | 5 | 4 | |
| Believer N° | 51 | 33 | 18 | |
| Practicing believer | 41 | 23 | 18 | 0.510 |
| Not believer | 3 | 1 | 2 |
| PCS < 30 | PCS ≥ 30 | |||
|---|---|---|---|---|
| T0 | T7 | T0 | T7 | |
| Pain | 6.1 (1.9) | 2.0 (1.6) ** | 6.8 (1.9) | 2.4 (1.7) ** |
| Dyspnea | 0.7 (2.3) | 0.0 (0.0) * | 0.7 (2.1) | 0.4 (1.2) ° |
| Anxiety | 2.9 (3.1) | 1.1 (1.9) ** | 4.6 (3.5) ° | 2.7 (2.6) **° |
| Depression | 2.5 (3.3) | 0.6 (1.5) ** | 4.4 (3.6) ° | 2.3 (2.7) **° |
| Poor sleep | 3.3 (3.2) | 1.6 (2.6) ** | 4.6 (3.7) | 1.7 (2.0) ** |
| Drowsiness | 2.8 (2.6) | 1.6 (2.0) ** | 4.3 (2.7) ° | 2.6 (2.7) ** |
| Nausea | 1.2 (2.7) | 0.5 (1.5) | 1.2 (2.5) | 0.8 (2.2) |
| Poor appetite | 2.3 (3.4) | 1.3 (2.2) | 4.5 (3.7) ° | 2.6 (2.9) **° |
| Weakness | 4.8 (3.2) | 2.3 (2.5) ** | 6.6 (2.3) ° | 3.5 (3.0) **° |
| Poor well-being | 4.6 (3.2) | 1.5 (2.0) ** | 6.6 (2.6) ° | 3.1 (2.9) **° |
| Total ESAS | 31.9 (14.7) | 13.1 (11.0) ** | 45.5 (16.9) ° | 23.61 (16.8) **° |
| OME | 78.8 (82) | 93.4 (88) | 176.7 (209) ° | 122.1 (98) |
| PCR < 30 | PCR ≥ 30 | PCR < 30 | PCR ≥ 30 | PC < 30 | PC ≥ 30 | |
|---|---|---|---|---|---|---|
| PSG | PSG | PGI | PGI | PSGR | PSGR | |
| Pain | 2.0 (2.0) | 2.3 (2.0) | 2.0 (1.1) | 1.7 (1.1) | 34 (59.6%) | 22 (57.9%) |
| Dyspnea | 0.04 (0.3) | 0.2 (0.6) | 0.4 (0.9) | 0.4 (0.9) | 57 (100%) | 34 (89.5%) * |
| Anxiety | 0.8 (1.5) | 1.2 (1.7) | 0.6 (0.9) | 0.2 (1.1) | 42 (73.7%) | 17 (44.7%) ** |
| Depression | 0.5 (1.3) | 1.2 (1.8) * | 0.6 (0.9) | 0.5 (1.2) | 49 (86.0%) | 25 (65.8%) * |
| Poor sleep | 0.9 (1.7) | 1.0 (1.9) | 0.7 (1.2) | 1.2 (1.3) * | 40 (70.2%) | 24 (63.2%) |
| Drowsiness | 0.9 (1.6) | 1.6 (1.9) | 0.4 (1.0) | 0.2 (1.2) | 34 (59.6%) | 19 (50.0%) |
| Nausea | 0.0 (0.0) | 0.1 (0.5) | 0.4 (0.9) | 0.6 (1.2) | 50 (87.7%) | 32 (84.2%) |
| Poor appetite | 0.7 (1.4) | 1.7 (2.0) ** | 0.7 (1.4) | 0.2 (1.3) | 40 (70.2%) | 26 (68.4%) |
| Weakness | 1.3 (1.7) | 2.1 (2.0) | 1.0 (1.2) | 0.6 (1.5) | 36 (63.2%) | 18 (47.4%) |
| Poor well-being | 1.2 (1.7) | 1.5 (1.8) | 1.2 (1.0) | 1.1 (1.2) | 39 (68.4%) | 18 (47.4%) * |
| Overall | PC < 30; N° 57 | PC ≥ 30; N° 38 | |
|---|---|---|---|
| Pain Catastrophizing Scale | |||
| (mean SD) | 26.9 (10.5) | 20.1 (6.9) | 37.2 (5.3) |
| Median (IQR) | 27(19–34) | 21(15–26) | 36(33–41) |
| Magnification subscale | |||
| (mean SD) | 3.5 (2.3) | 2.7 (2.2) | 4.8 (2.0) |
| Median (IQR) | 3(2–5) | 2(1–4) | 5(4–6) |
| Rumination subscale | |||
| (mean SD) | 12.7 (4.6) | 10.5 (4.4) | 16.1 (2.4) |
| Median (IQR) | 13(10–16) | 11(8–13) | 16(14–18) |
| Helplessness subscale | |||
| (mean SD) | 10.7 (5.7) | 7.4 (3.8) | 15.8 (4.0) |
| Median (IQR) | 11(7–14) | 8(4–10) | 15(13–19) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mercadante, S.; Ferrera, P.; Lo Cascio, A.; Casuccio, A. Pain Catastrophizing in Cancer Patients. Cancers 2024, 16, 568. https://doi.org/10.3390/cancers16030568
Mercadante S, Ferrera P, Lo Cascio A, Casuccio A. Pain Catastrophizing in Cancer Patients. Cancers. 2024; 16(3):568. https://doi.org/10.3390/cancers16030568
Chicago/Turabian StyleMercadante, Sebastiano, Patrizia Ferrera, Alessio Lo Cascio, and Alessandra Casuccio. 2024. "Pain Catastrophizing in Cancer Patients" Cancers 16, no. 3: 568. https://doi.org/10.3390/cancers16030568
APA StyleMercadante, S., Ferrera, P., Lo Cascio, A., & Casuccio, A. (2024). Pain Catastrophizing in Cancer Patients. Cancers, 16(3), 568. https://doi.org/10.3390/cancers16030568