
Diagnostic Performance of a Novel Ultra-Thin Endoscopy under Narrow-Band Imaging for Superficial Squamous Cell Carcinoma of the Pharynx and Esophagus
 , , , , , and
, , , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
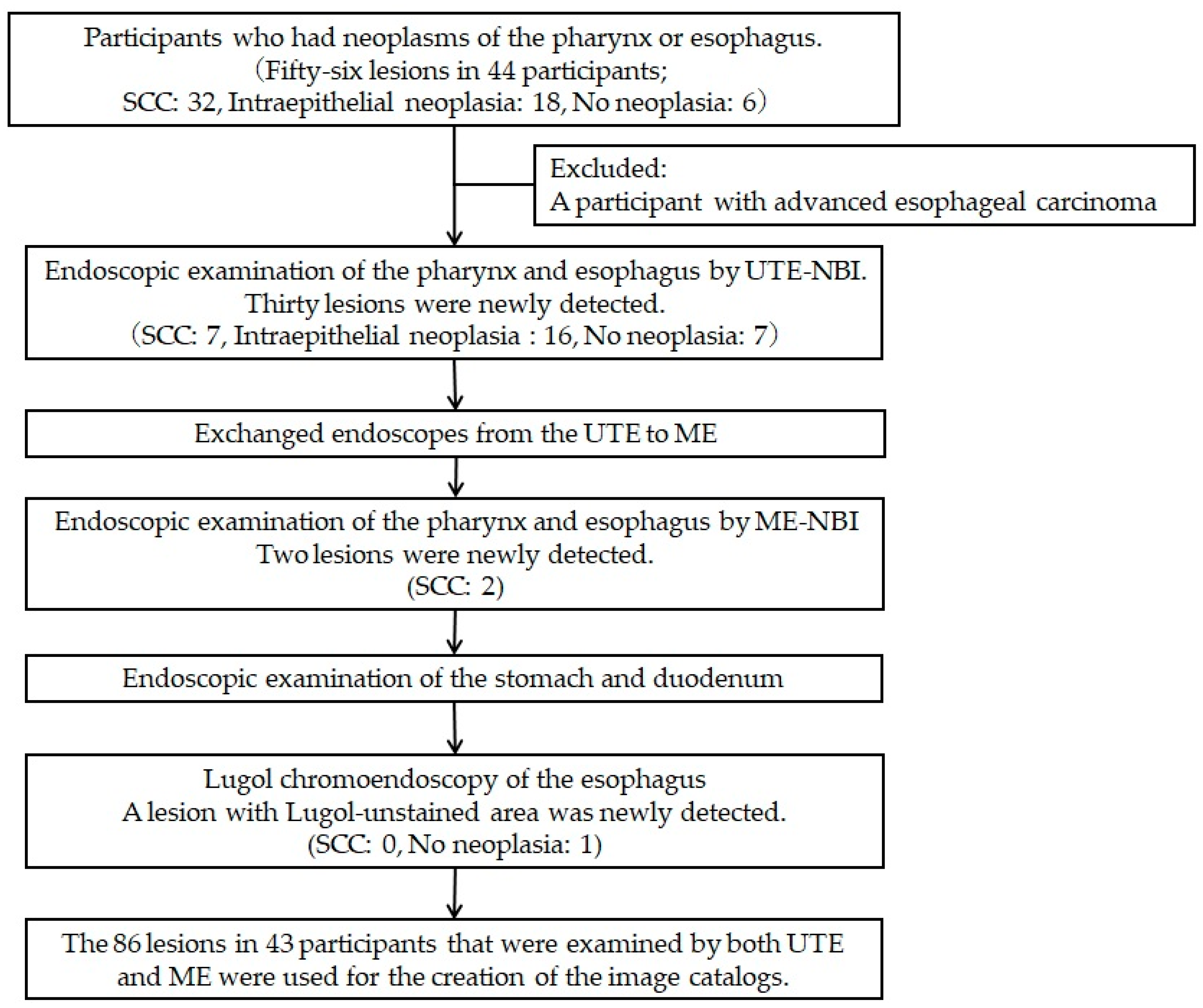
2.1. Trial Design and Study Population
2.2. Participants
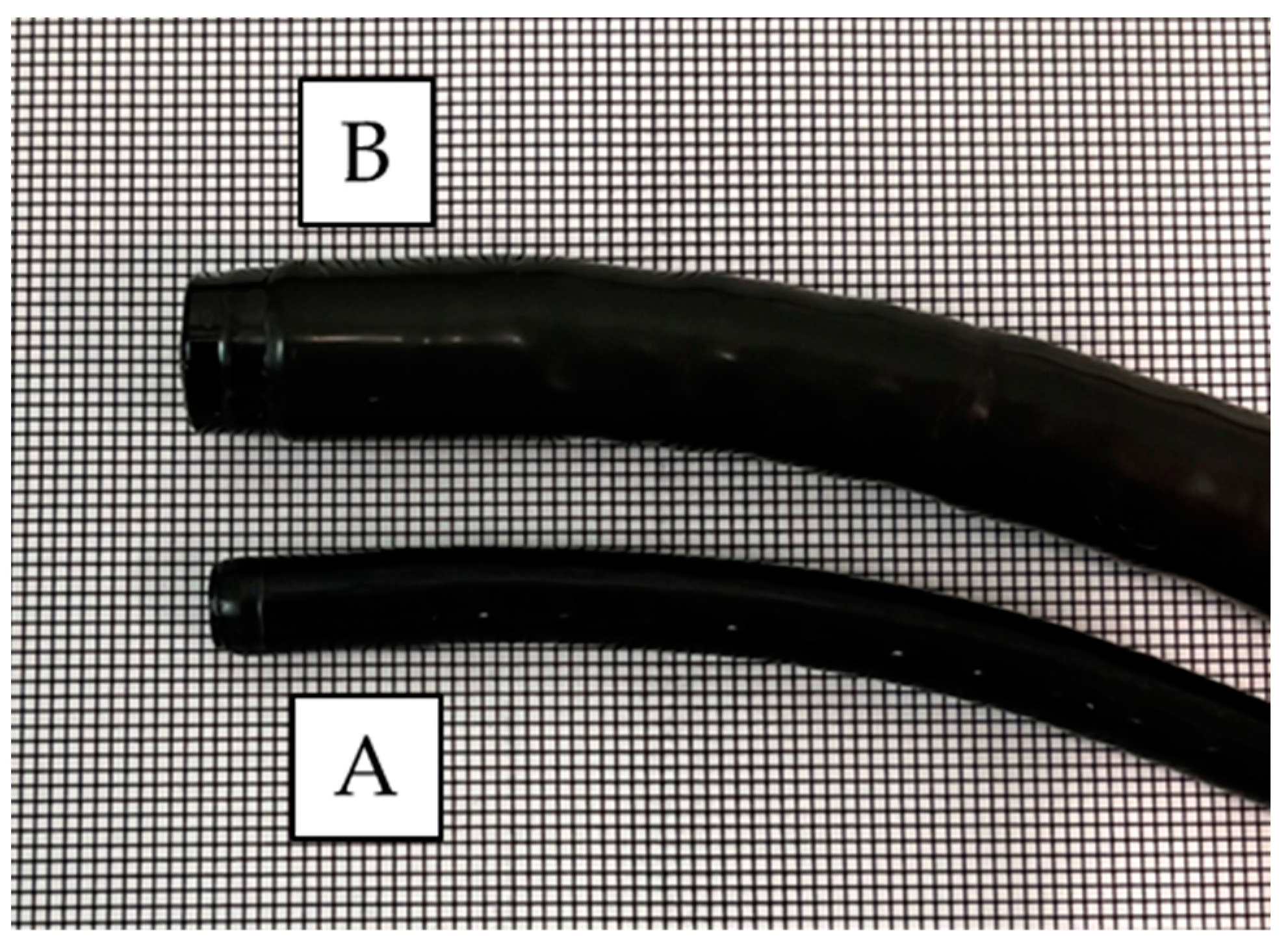
2.3. Endoscopy Equipment and Setting
2.4. Endoscopic Procedure
2.5. Image Assessment Study
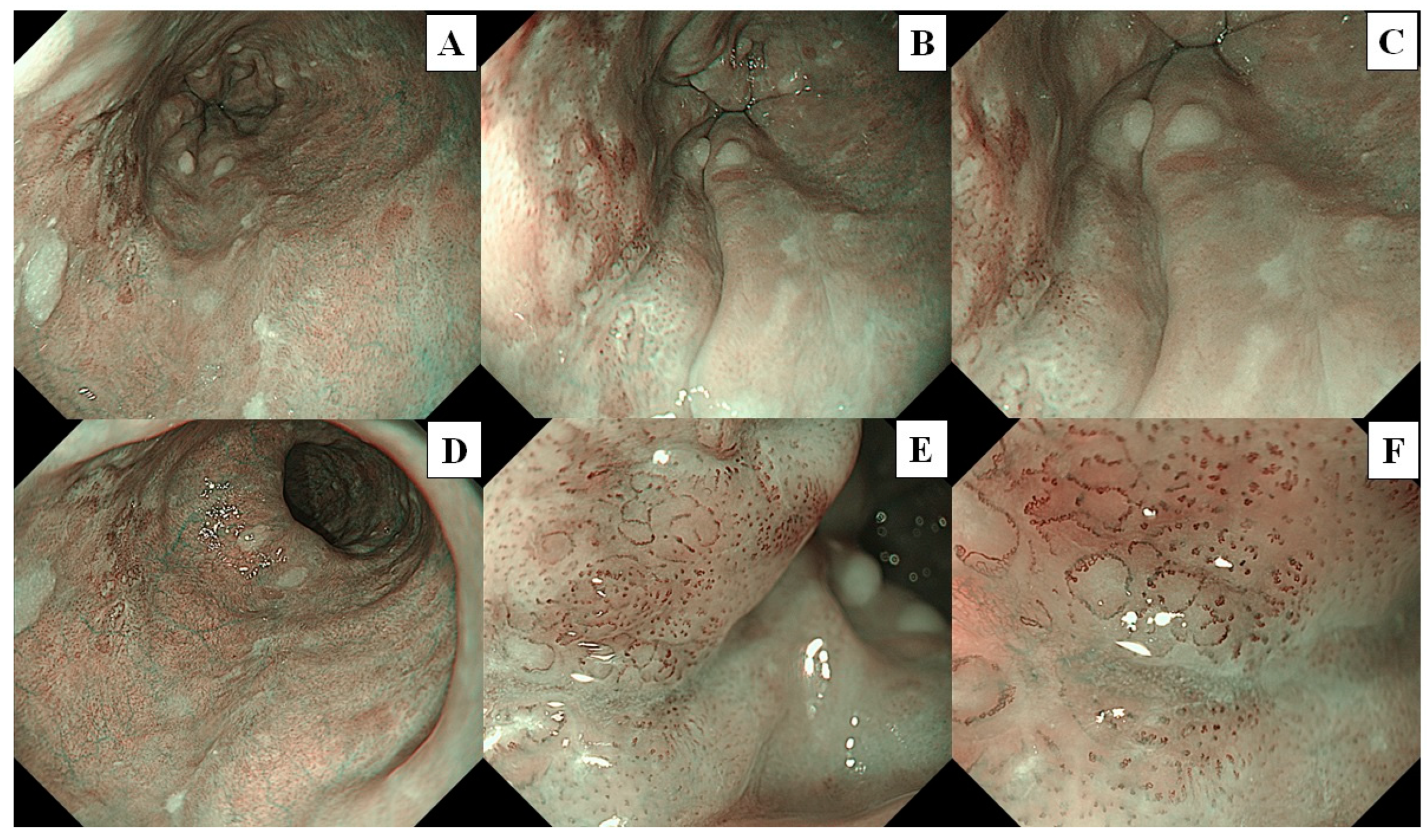
Preparation of Image Catalogs
2.6. Assessment of the Images
2.7. Outcomes
2.8. Sample Size
2.9. Pathological Diagnosis
2.10. Statistical Analysis
3. Results
3.1. Primary Outcome
3.2. Diagnostic Performance of UTE-NBI and ME-NBI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global cancer statistics, 2002. CA Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef] [PubMed]
- Mody, M.D.; Rocco, J.W.; Yom, S.S.; Haddad, R.I.; Saba, N.F. Head and neck cancer. Lancet 2021, 398, 2289–2299. [Google Scholar] [CrossRef] [PubMed]
- Rustgi, A.K.; El-Serag, H.B. Esophageal carcinoma. N. Engl. J. Med. 2014, 371, 2499–2509. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, T.; Suzuki, H. Long-term outcomes of endoscopic submucosal dissection for superficial esophageal squamous cell carcinoma. Cancers 2020, 12, 2849. [Google Scholar] [CrossRef] [PubMed]
- Yoshimizu, S.; Yoshio, T.; Ishiyama, A.; Tsuchida, T.; Horiuchi, Y.; Omae, M.; Hirasawa, T.; Asari, T.; Chin, K.; Fujisaki, J. Long-term outcomes of combined endoscopic resection and chemoradiotherapy for esophageal squamous cell carcinoma with submucosal invasion. Dig. Liver Dis. 2018, 50, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.; Rahmi, G.; Perrod, G.; Pioche, M.; Canard, J.M.; Cesbron-Métivier, E.; Boursier, J.; Samaha, E.; Vienne, A.; Lépilliez, V.; et al. Long-term follow-up after endoscopic resection for superficial esophageal squamous cell carcinoma: A multicenter western study. Endoscopy 2019, 51, 298–306. [Google Scholar] [CrossRef]
- Dobashi, A.; Aizawa, D.; Hara, Y.; Furuhashi, H.; Matsui, H.; Futakuchi, T.; Ono, S.; Toyoizumi, H.; Bazerbachi, F.; Yamauchi, T.; et al. The advantage of immunohistochemical staining for evaluating lymphovascular invasion is limited for patients with esophageal squamous cell carcinoma invading the muscularis mucosa. J. Clin. Med. 2022, 11, 6969. [Google Scholar] [CrossRef]
- Ono, S.; Fujishiro, M.; Niimi, K.; Goto, O.; Kodashima, S.; Yamamichi, N.; Omata, M. Long-term outcomes of endoscopic submucosal dissection for superficial esophageal squamous cell neoplasms. Gastrointest. Endosc. 2009, 70, 860–866. [Google Scholar] [CrossRef]
- Yamashina, T.; Ishihara, R.; Nagai, K.; Matsuura, N.; Matsui, F.; Ito, T.; Fujii, M.; Yamamoto, S.; Hanaoka, N.; Takeuchi, Y.; et al. Long-term outcome and metastatic risk after endoscopic resection of superficial esophageal squamous cell carcinoma. Am. J. Gastroenterol. 2013, 108, 544–551. [Google Scholar] [CrossRef]
- Iizuka, T.; Kikuchi, D.; Suzuki, Y.; Tanaka, M.; Takeda, H. Clinical relevance of endoscopic treatment for superficial pharyngeal cancer: Feasibility of techniques corresponding to each location and long-term outcomes. Gastrointest. Endosc. 2021, 93, 818–827. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, R.; Arima, M.; Iizuka, T.; Oyama, T.; Katada, C.; Kato, M.; Goda, K.; Goto, O.; Tanaka, K.; Yano, T.; et al. Endoscopic submucosal dissection/endoscopic mucosal resection guidelines for esophageal cancer. Dig. Endosc. 2020, 32, 452–493. [Google Scholar] [CrossRef] [PubMed]
- Muto, M.; Minashi, K.; Yano, T.; Saito, Y.; Oda, I.; Nonaka, S.; Omori, T.; Sugiura, H.; Goda, K.; Kaise, M.; et al. Early detection of superficial squamous cell carcinoma in the head and neck region and esophagus by narrow band imaging: A multicenter randomized controlled trial. J. Clin. Oncol. 2010, 28, 1566–1572. [Google Scholar] [CrossRef] [PubMed]
- Cosway, B.; Drinnan, M.; Paleri, V. Narrow band imaging for the diagnosis of head and neck squamous cell carcinoma: A systematic review. Head Neck 2016, 38 (Suppl. 1), E2358–E2367. [Google Scholar] [CrossRef]
- Uedo, N.; Fujishiro, M.; Goda, K.; Hirasawa, D.; Kawahara, Y.; Lee, J.H.; Miyahara, R.; Morita, Y.; Singh, R.; Takeuchi, M.; et al. Role of narrow band imaging for diagnosis of early-stage esophagogastric cancer: Current consensus of experienced endoscopists in asia-pacific region. Dig. Endosc. 2011, 23 (Suppl. 1), 58–71. [Google Scholar] [CrossRef]
- Goda, K.; Dobashi, A.; Tajiri, H. Perspectives on narrow-band imaging endoscopy for superficial squamous neoplasms of the orohypopharynx and esophagus. Dig. Endosc. 2014, 26 (Suppl. 1), 1–11. [Google Scholar] [CrossRef]
- Morita, F.H.; Bernardo, W.M.; Ide, E.; Rocha, R.S.; Aquino, J.C.; Minata, M.K.; Yamazaki, K.; Marques, S.B.; Sakai, P.; de Moura, E.G. Narrow band imaging versus lugol chromoendoscopy to diagnose squamous cell carcinoma of the esophagus: A systematic review and meta-analysis. BMC Cancer 2017, 17, 54. [Google Scholar] [CrossRef]
- Oyama, T.; Inoue, H.; Arima, M.; Momma, K.; Omori, T.; Ishihara, R.; Hirasawa, D.; Takeuchi, M.; Tomori, A.; Goda, K. Prediction of the invasion depth of superficial squamous cell carcinoma based on microvessel morphology: Magnifying endoscopic classification of the japan esophageal society. Esophagus 2017, 14, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, K.; Matsui, T.; Mukai, M.; Sugimoto, T. Prediction of the depth of invasion in superficial pharyngeal cancer: Microvessel morphological evaluation with narrowband imaging. Head Neck 2019, 41, 3970–3975. [Google Scholar] [CrossRef] [PubMed]
- Ueda, T.; Dohi, O.; Naito, Y.; Yoshida, T.; Azuma, Y.; Ishida, T.; Matsumura, S.; Kitae, H.; Takayama, S.; Mizuno, N.; et al. Diagnostic performance of magnifying blue laser imaging versus magnifying narrow-band imaging for identifying the depth of invasion of superficial esophageal squamous cell carcinoma. Dis. Esophagus 2021, 34, doaa078. [Google Scholar] [CrossRef]
- Goda, K.; Dobashi, A.; Yoshimura, N.; Aihara, H.; Kato, M.; Sumiyama, K.; Toyoizumi, H.; Kato, T.; Saijo, H.; Ikegami, M.; et al. Dual-focus versus conventional magnification endoscopy for the diagnosis of superficial squamous neoplasms in the pharynx and esophagus: A randomized trial. Endoscopy 2016, 48, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Kawai, Y.; Hamada, M.; Iwata, E.; Niikura, R.; Nagata, N.; Yanagisawa, K.; Sugimoto, M.; Fukuzawa, M.; Yamagishi, T.; et al. Present status and the future of ultrathin endoscopy. Dig. Endosc. 2022, 34, 1110–1120. [Google Scholar] [CrossRef] [PubMed]
- Dobashi, A.; Goda, K.; Furuhashi, H.; Matsui, H.; Hara, Y.; Kamba, S.; Kobayashi, M.; Sumiyama, K.; Hirooka, S.; Hamatani, S.; et al. Diagnostic efficacy of dual-focus endoscopy with narrow-band imaging using simplified dyad criteria for superficial esophageal squamous cell carcinoma. J. Gastroenterol. 2019, 54, 501–510. [Google Scholar] [CrossRef]
- Dobashi, A.; Goda, K.; Yoshimura, N.; Ohya, T.R.; Kato, M.; Sumiyama, K.; Matsushima, M.; Hirooka, S.; Ikegami, M.; Tajiri, H. Simplified criteria for diagnosing superficial esophageal squamous neoplasms using narrow band imaging magnifying endoscopy. World J. Gastroenterol. 2016, 22, 9196–9204. [Google Scholar] [CrossRef] [PubMed]
- Inoue, H.; Honda, T.; Yoshida, T.; Nishikage, T.; Nagahama, T.; Yano, K.; Nagai, K.; Kawano, T.; Yoshino, K.; Tani, M.; et al. Ultra-high magnification endoscopy of the normal esophageal mucosa. Dig. Endosc. 1996, 8, 134–138. [Google Scholar] [CrossRef]
- Yoshida, T.; Inoue, H.; Usui, S.; Satodate, H.; Fukami, N.; Kudo, S.E. Narrow-band imaging system with magnifying endoscopy for superficial esophageal lesions. Gastrointest. Endosc. 2004, 59, 288–295. [Google Scholar] [CrossRef]
- Kumagai, Y.; Monma, K.; Kawada, K. Magnifying chromoendoscopy of the esophagus: In-vivo pathological diagnosis using an endocytoscopy system. Endoscopy 2004, 36, 590–594. [Google Scholar] [CrossRef]
- Shimizu, Y.; Takahashi, M.; Yoshida, T.; Ono, S.; Mabe, K.; Kato, M.; Asaka, M.; Hatanaka, K.; Sakamoto, N. Endoscopic in vivo cellular imaging of superficial squamous cell carcinoma of the head and neck by using an integrated endocytoscopy system (with video). Gastrointest. Endosc. 2013, 78, 351–358. [Google Scholar] [CrossRef]
- Guo, J.; Li, C.Q.; Li, M.; Zuo, X.L.; Yu, T.; Liu, J.W.; Liu, J.; Kou, G.J.; Li, Y.Q. Diagnostic value of probe-based confocal laser endomicroscopy and high-definition virtual chromoendoscopy in early esophageal squamous neoplasia. Gastrointest. Endosc. 2015, 81, 1346–1354. [Google Scholar] [CrossRef]
- Arens, C.; Betz, C.; Kraft, M.; Voigt-Zimmermann, S. Narrow band imaging for early diagnosis of epithelial dysplasia and microinvasive tumors in the upper aerodigestive tract. HNO 2017, 65, 5–12. [Google Scholar] [CrossRef]
- Muto, M.; Nakane, M.; Katada, C.; Sano, Y.; Ohtsu, A.; Esumi, H.; Ebihara, S.; Yoshida, S. Squamous cell carcinoma in situ at oropharyngeal and hypopharyngeal mucosal sites. Cancer 2004, 101, 1375–1381. [Google Scholar] [CrossRef]
- Watanabe, A.; Taniguchi, M.; Tsujie, H.; Hosokawa, M.; Fujita, M.; Sasaki, S. The value of narrow band imaging endoscope for early head and neck cancers. Otolaryngol. Head Neck Surg. 2008, 138, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Piazza, C.; Cocco, D.; Del Bon, F.; Mangili, S.; Nicolai, P.; Peretti, G. Narrow band imaging and high definition television in the endoscopic evaluation of upper aero-digestive tract cancer. Acta Otorhinolaryngol. Ital. 2011, 31, 70–75. [Google Scholar] [PubMed]
- Ali, M.; Gupta, G.; Silu, M.; Chand, D.; Samor, V. Narrow band imaging in early diagnosis of laryngopharyngeal malignant and premalignant lesions. Auris Nasus Larynx 2022, 49, 676–679. [Google Scholar] [CrossRef] [PubMed]
- Puxeddu, R.; Sionis, S.; Gerosa, C.; Carta, F. Enhanced contact endoscopy for the detection of neoangiogenesis in tumors of the larynx and hypopharynx. Laryngoscope 2015, 125, 1600–1606. [Google Scholar] [CrossRef]
- Ina, H.; Shibuya, H.; Ohashi, I.; Kitagawa, M. The frequency of a concomitant early esophageal cancer in male patients with oral and oropharyngeal cancer. Screening results using lugol dye endoscopy. Cancer 1994, 73, 2038–2041. [Google Scholar] [CrossRef]
- Hori, K.; Okada, H.; Kawahara, Y.; Takenaka, R.; Shimizu, S.; Ohno, Y.; Onoda, T.; Sirakawa, Y.; Naomoto, Y.; Yamamoto, K. Lugol-voiding lesions are an important risk factor for a second primary squamous cell carcinoma in patients with esosphageal cancer or head and neck cancer. Am. J. Gastroenterol. 2011, 106, 858–866. [Google Scholar] [CrossRef]
- Murata, A.; Akahoshi, K.; Sumida, Y.; Yamamoto, H.; Nakamura, K.; Nawata, H. Prospective randomized trial of transnasal versus peroral endoscopy using an ultrathin videoendoscope in unsedated patients. J. Gastroenterol. Hepatol. 2007, 22, 482–485. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Location: oropharynx, hypopharynx/Ce, Ut, Mt, Lt, Ae | 3, 19/12, 19, 23, 10, 0 |
| Diameter (mm), median (range) | 8 (3–54) |
| Macroscopic type: 0-I/0-IIa, 0-Iib, 0-Iic/0-III | 1/10, 45, 30/0 |
| Histopathology: SCC, IN, no neoplasia | 39, 34, 13 |
| UTE (Test-1) vs. ME-1 (Test-2) | ME-1 (Test-2) vs. ME-2 (Test-3) | |
|---|---|---|
| Reviewer A | 0.74 (87.2%) | 0.84 (91.9%) |
| Reviewer B | 0.63 (81.4%) | 0.76 (88.3%) |
| Reviewer C | 0.79 (90.7%) | 0.88 (94.2%) |
| All Lesions (n = 86) | High Confidence Lesions | |||||||
|---|---|---|---|---|---|---|---|---|
| UTE | ME-1 | p-Value | UTE | ME-1 | p-Value | |||
| Reviewer A | Number of lesions | 26 (30.2%) | 24 (27.9%) | 0.74 ** | ||||
| Sensitivity (%) | 74.4 | 84.6 | Sensitivity (%) | 95.7 | 100 | 0.32 ** | ||
| Specificity (%) | 97.9 | 87.2 | Specificity (%) | 100 | 0 | 0.046 | ||
| Accuracy (%) | 87.2 | 86.0 | 0.059 * | Accuracy (%) | 96.2 | 95.8 | 0.95 ** | |
| PPV (%) | 96.7 | 84.6 | PPV (%) | 100 | 95.8 | 0.33 ** | ||
| NPV (%) | 82.1 | 87.2 | NPV (%) | 75.0 | − | − | ||
| Reviewer B | Number of lesions | 48 (55.8%) | 54 (62.8%) | 0.35 ** | ||||
| Sensitivity (%) | 79.5 | 82.1 | Sensitivity (%) | 95.2 | 92.9 | 0.73 ** | ||
| Specificity (%) | 76.0 | 66.0 | Specificity (%) | 92.6 | 76.9 | 0.11 ** | ||
| Accuracy (%) | 78.0 | 73.2 | 0.13 * | Accuracy (%) | 93.8 | 85.2 | 0.16 ** | |
| PPV (%) | 73.8 | 66.7 | PPV (%) | 90.9 | 81.3 | 0.33 ** | ||
| NPV (%) | 81.8 | 81.6 | NPV (%) | 96.2 | 90.9 | 0.45 ** | ||
| Reviewer C | Number of lesions | 50 (58.1%) | 48 (55.8%) | 0.76 ** | ||||
| Sensitivity (%) | 59.0 | 69.2 | Sensitivity (%) | 87.5 | 81.5 | 0.33 ** | ||
| Specificity (%) | 89.4 | 93.6 | Specificity (%) | 84.6 | 95.2 | 0.36 ** | ||
| Accuracy (%) | 75.6 | 82.6 | 0.48 * | Accuracy (%) | 86.0 | 87.5 | 0.83 ** | |
| PPV (%) | 82.1 | 90.0 | PPV (%) | 88.0 | 95.7 | 0.34 ** | ||
| NPV (%) | 72.4 | 78.6 | NPV (%) | 84.0 | 80.0 | 0.71 ** | ||
| Pharynx (n = 22) | Esophagus (n = 64) | |||||||
|---|---|---|---|---|---|---|---|---|
| UTE | ME-1 | p-Value | UTE | ME-1 | p-Value | |||
| Reviewer A | Sensitivity (%) | 92.3 | 100 | 1.00 * | Sensitivity (%) | 65.4 | 76.9 | 0.011 * |
| Specificity (%) | 100 | 100 | Specificity (%) | 97.4 | 84.2 | |||
| Accuracy (%) | 95.5 | 100 | Accuracy (%) | 84.3 | 81.3 | |||
| PPV (%) | 100 | 100 | PPV (%) | 94.4 | 76.9 | |||
| NPV (%) | 90.0 | 100 | NPV (%) | 80.4 | 84.2 | |||
| Reviewer B | Sensitivity (%) | 84.6 | 92.3 | 0.317 * | Sensitivity (%) | 76.9 | 76.9 | 0.248 * |
| Specificity (%) | 55.6 | 44.4 | Specificity (%) | 81.6 | 71.1 | |||
| Accuracy (%) | 72.7 | 72.7 | Accuracy (%) | 79.7 | 73.4 | |||
| PPV (%) | 73.3 | 70.6 | PPV (%) | 74.1 | 64.5 | |||
| NPV (%) | 71.4 | 80.0 | NPV (%) | 83.8 | 81.8 | |||
| Reviewer C | Sensitivity (%) | 84.6 | 84.6 | 0.157 * | Sensitivity (%) | 46.2 | 61.5 | 0.103 * |
| Specificity (%) | 66.7 | 88.9 | Specificity (%) | 94.7 | 94.7 | |||
| Accuracy (%) | 77.2 | 86.4 | Accuracy (%) | 75.0 | 81.2 | |||
| PPV (%) | 78.6 | 91.7 | PPV (%) | 85.7 | 88.9 | |||
| NPV (%) | 75.0 | 80.0 | NPV (%) | 72.0 | 78.2 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobashi, A.; Hara, Y.; Furuhashi, H.; Matsui, H.; Tada, N.; Ito, M.; Futakuchi, T.; Kobayashi, M.; Ono, S.; Aizawa, D.; et al. Diagnostic Performance of a Novel Ultra-Thin Endoscopy under Narrow-Band Imaging for Superficial Squamous Cell Carcinoma of the Pharynx and Esophagus. Cancers 2024, 16, 529. https://doi.org/10.3390/cancers16030529
Dobashi A, Hara Y, Furuhashi H, Matsui H, Tada N, Ito M, Futakuchi T, Kobayashi M, Ono S, Aizawa D, et al. Diagnostic Performance of a Novel Ultra-Thin Endoscopy under Narrow-Band Imaging for Superficial Squamous Cell Carcinoma of the Pharynx and Esophagus. Cancers. 2024; 16(3):529. https://doi.org/10.3390/cancers16030529
Chicago/Turabian StyleDobashi, Akira, Yuko Hara, Hiroto Furuhashi, Hiroaki Matsui, Naoya Tada, Mamoru Ito, Toshiki Futakuchi, Masakuni Kobayashi, Shingo Ono, Daisuke Aizawa, and et al. 2024. "Diagnostic Performance of a Novel Ultra-Thin Endoscopy under Narrow-Band Imaging for Superficial Squamous Cell Carcinoma of the Pharynx and Esophagus" Cancers 16, no. 3: 529. https://doi.org/10.3390/cancers16030529
APA StyleDobashi, A., Hara, Y., Furuhashi, H., Matsui, H., Tada, N., Ito, M., Futakuchi, T., Kobayashi, M., Ono, S., Aizawa, D., Yamauchi, T., Suka, M., & Sumiyama, K. (2024). Diagnostic Performance of a Novel Ultra-Thin Endoscopy under Narrow-Band Imaging for Superficial Squamous Cell Carcinoma of the Pharynx and Esophagus. Cancers, 16(3), 529. https://doi.org/10.3390/cancers16030529