
Methylated Cell-Free Tumor DNA in Sputum as a Tool for Diagnosing Lung Cancer—A Systematic Review and Meta-Analysis

 ,
,  , ,
, ,  , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Protocol and Registration
2.2. Data Sources and Search Strategy
2.3. Reference Screening and Eligibility Criteria
2.4. Data Extraction and Quality Assessment
2.5. Statistical Analysis
3. Results
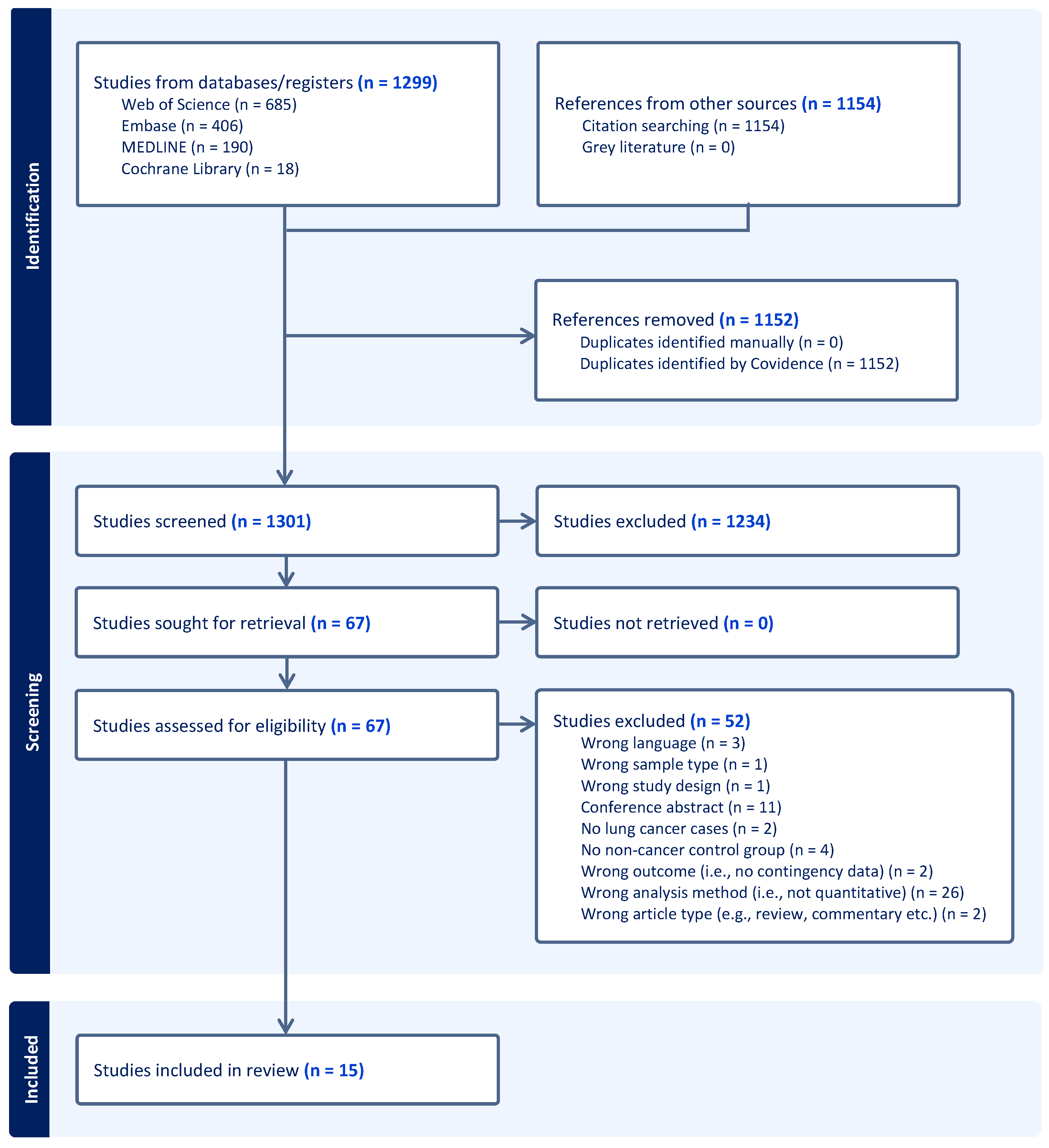
3.1. Search Results and Study Selection
3.2. Study Characteristics
3.3. Biological Sample Types and Collection Method
3.4. The Reporting of Key Domains of the Analysis Methods
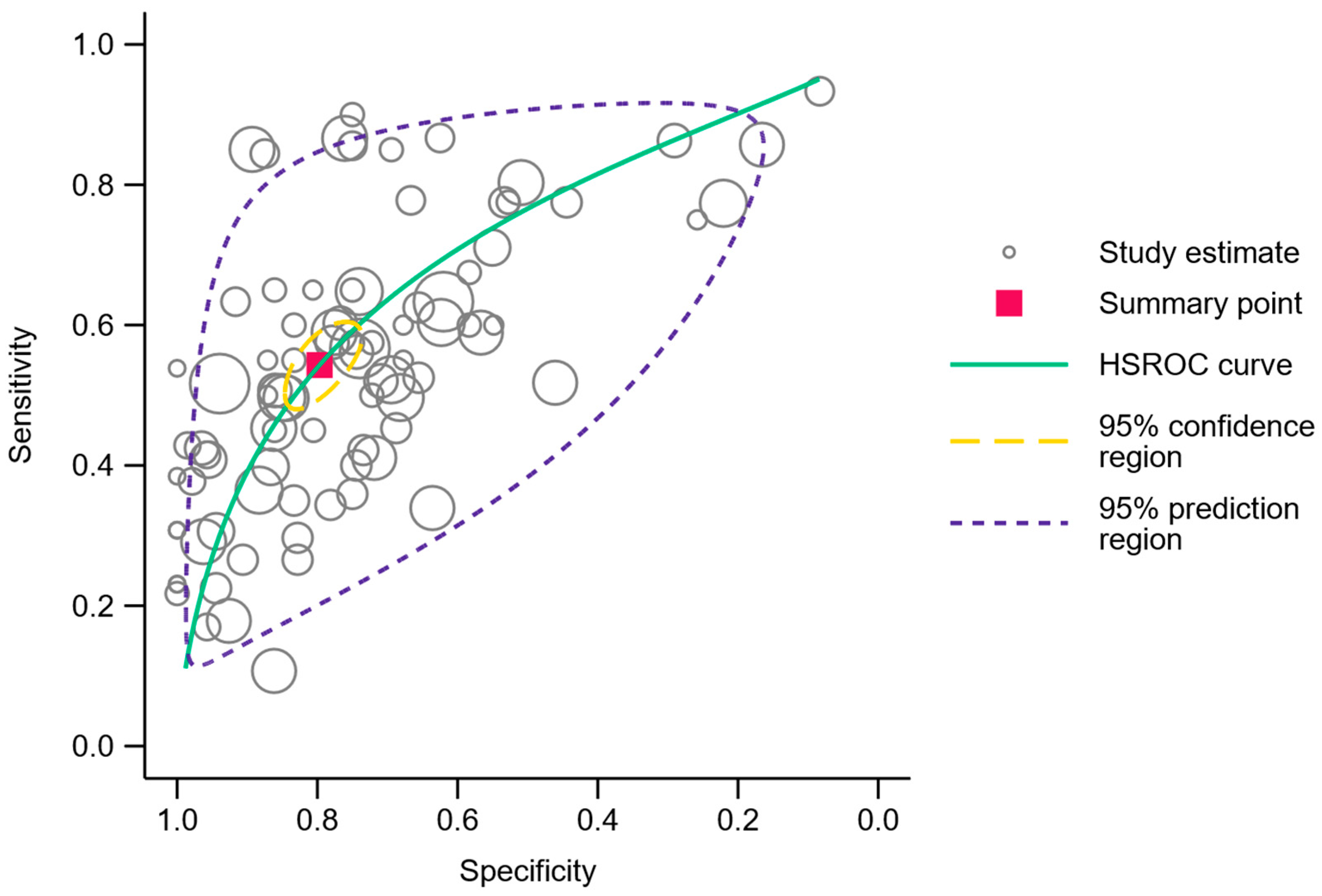
3.5. Methylated DNA Analysis in Sputum for the Diagnosis of Lung Cancer
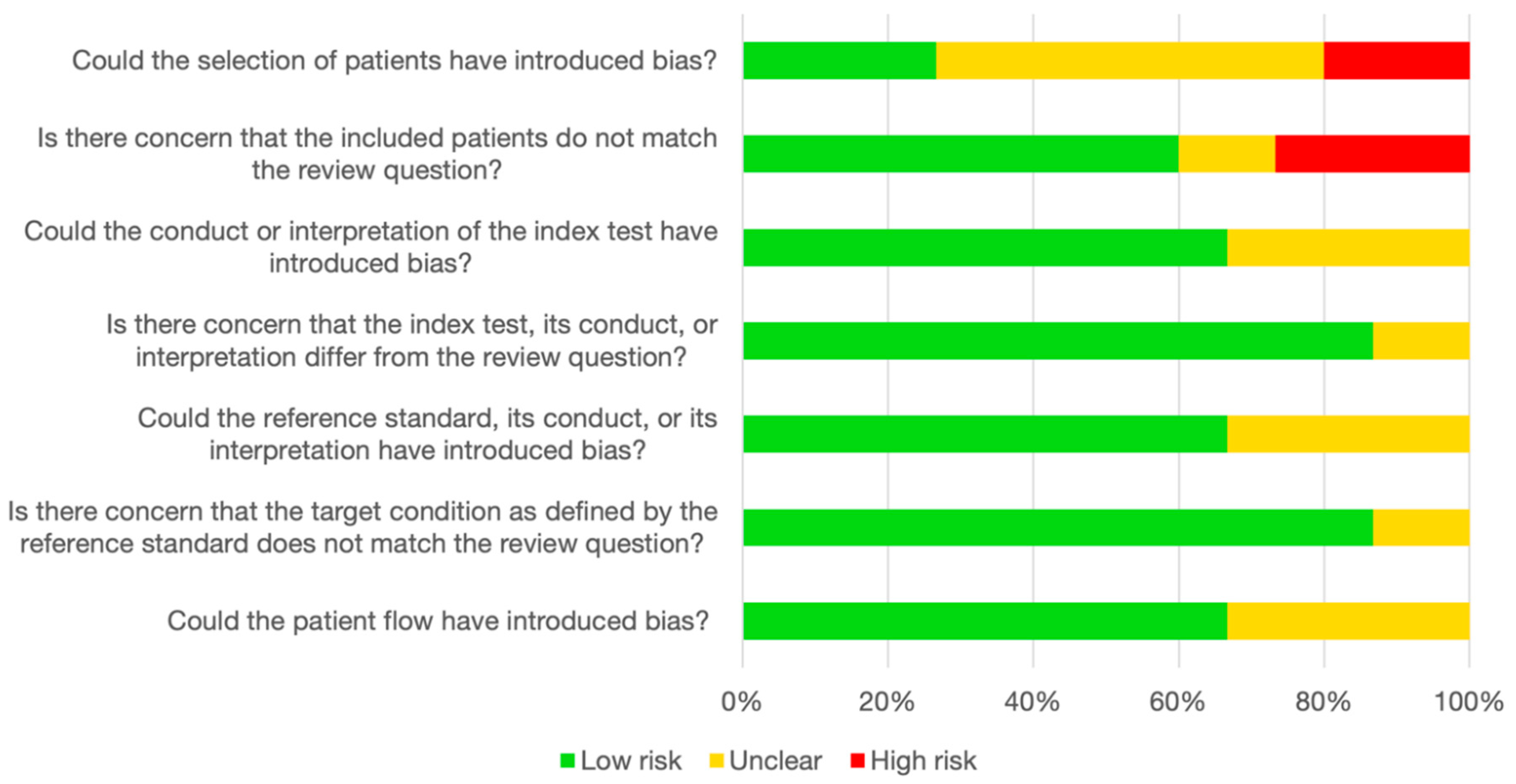
3.6. Quality Assessment and Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mattiuzzi, C.; Lippi, G. Current Cancer Epidemiology. J. Epidemiol. Glob. Health 2019, 9, 217. [Google Scholar] [CrossRef]
- Woodard, G.A.; Jones, K.D.; Jablons, D.M. Lung Cancer Staging and Prognosis. In Lung Cancer; Reckamp, K.L., Ed.; Cancer Treatment and Research; Springer International Publishing: Cham, Switzerland, 2016; Volume 170, pp. 47–75. ISBN 978-3-319-40387-8. [Google Scholar]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global Surveillance of Trends in Cancer Survival 2000–14 (CONCORD-3): Analysis of Individual Records for 37 513 025 Patients Diagnosed with One of 18 Cancers from 322 Population-Based Registries in 71 Countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [PubMed]
- Borg, M.; Hilberg, O.; Andersen, M.B.; Weinreich, U.M.; Rasmussen, T.R. Increased Use of Computed Tomography in Denmark: Stage Shift toward Early Stage Lung Cancer through Incidental Findings. Acta Oncol. 2022, 61, 1256–1262. [Google Scholar] [CrossRef] [PubMed]
- Bredtoft, E.N.; Madsen, H.H.; Rasmussen, T.R. Stage I Lung Cancer Patients with or without Symptoms—Are the Patients Different and Should We Treat Them Differently? Acta Oncol. 2021, 60, 1169–1174. [Google Scholar] [CrossRef] [PubMed]
- Potter, A.L.; Rosenstein, A.L.; Kiang, M.V.; Shah, S.A.; Gaissert, H.A.; Chang, D.C.; Fintelmann, F.J.; Yang, C.-F.J. Association of Computed Tomography Screening with Lung Cancer Stage Shift and Survival in the United States: Quasi-Experimental Study. BMJ 2022, 376, e069008. [Google Scholar] [CrossRef]
- Field, J.K.; Vulkan, D.; Davies, M.P.A.; Baldwin, D.R.; Brain, K.E.; Devaraj, A.; Eisen, T.; Gosney, J.; Green, B.A.; Holemans, J.A.; et al. Lung Cancer Mortality Reduction by LDCT Screening: UKLS Randomised Trial Results and International Meta-Analysis. Lancet Reg. Health Eur. 2021, 10, 100179. [Google Scholar] [CrossRef]
- The National Lung Screening Trial Research Team. Reduced Lung-Cancer Mortality with Low-Dose Computed Tomographic Screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef]
- de Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.-W.J.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef]
- Gill, R.R.; Jaklitsch, M.T.; Jacobson, F.L. Controversies in Lung Cancer Screening. J. Am. Coll. Radiol. 2016, 13, R2–R7. [Google Scholar] [CrossRef]
- Seijo, L.M.; Peled, N.; Ajona, D.; Boeri, M.; Field, J.K.; Sozzi, G.; Pio, R.; Zulueta, J.J.; Spira, A.; Massion, P.P.; et al. Biomarkers in Lung Cancer Screening: Achievements, Promises, and Challenges. J. Thorac. Oncol. 2019, 14, 343–357. [Google Scholar] [CrossRef]
- Henriksen, M.B.; Jensen, L.H.; Hilberg, O.; Hansen, T.F.; Brasen, C.L. 1284P Lung Cancer among Patients with Chronic Obstructive Pulmonary Disease: A Danish 10-Year Observational Study of the Overlapping Population. Ann. Oncol. 2023, 34, S741. [Google Scholar] [CrossRef]
- Thunnissen, F.B.J.M. Sputum Examination for Early Detection of Lung Cancer. J. Clin. Pathol. 2003, 56, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Horinouchi, H.; Kusumoto, M.; Yatabe, Y.; Aokage, K.; Watanabe, S.; Ishikura, S. Lung Cancer in Japan. J. Thorac. Oncol. 2022, 17, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Soukiasian, H.J.; Leung, A.; Imai, T.; Bose, S.; Kim, S.; Mosenifar, Z.; Gupta, N.K.; Tajbakhsh, J. Highly Sensitive Noninvasive Early Lung Cancer Detection Using DNA Methylation Topology in Sputum-Derived Epithelial Cells. JTCVS Open 2023, 13, 389–410. [Google Scholar] [CrossRef] [PubMed]
- Redshaw, N.; Huggett, J.F.; Taylor, M.S.; Foy, C.A.; Devonshire, A.S. Quantification of Epigenetic Biomarkers: An Evaluation of Established and Emerging Methods for DNA Methylation Analysis. BMC Genom. 2014, 15, 1174. [Google Scholar] [CrossRef] [PubMed]
- McGinn, S.; Gut, I.G. DNA Sequencing—Spanning the Generations. N. Biotechnol. 2013, 30, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Hubers, A.J.; Heideman, D.A.M.; Burgers, S.A.; Herder, G.J.M.; Sterk, P.J.; Rhodius, R.J.; Smit, H.J.; Krouwels, F.; Welling, A.; Witte, B.I.; et al. DNA Hypermethylation Analysis in Sputum for the Diagnosis of Lung Cancer: Training Validation Set Approach. Br. J. Cancer 2015, 112, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- Leng, S.; Do, K.; Yingling, C.M.; Picchi, M.A.; Wolf, H.J.; Kennedy, T.C.; Feser, W.J.; Baron, A.E.; Franklin, W.A.; Brock, M.V.; et al. Defining a Gene Promoter Methylation Signature in Sputum for Lung Cancer Risk Assessment. Clin. Cancer Res. 2012, 18, 3387–3395. [Google Scholar] [CrossRef]
- Su, Y.; Fang, H.; Jiang, F. Integrating DNA Methylation and microRNA Biomarkers in Sputum for Lung Cancer Detection. Clin. Epigenetics 2016, 8, 109. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Borg, M.; Wen, S.W.C. Methylated Cell Free Tumor DNA in Sputum as a Tool for Diagnosing Lung Cancer. PROSPERO 2023 CRD42023453066. 2023. Available online: https://www.Crd.York.Ac.Uk/Prospero/Display_record.Php?ID=CRD42023453066 (accessed on 1 October 2023).
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE Guidelines: Minimum Information for Publication of Quantitative Real-Time PCR Experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2 Group QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Harbord, R.M.; Whiting, P. Metandi: Meta-Analysis of Diagnostic Accuracy Using Hierarchical Logistic Regression. Stata J. Promot. Commun. Stat. Stata 2009, 9, 211–229. [Google Scholar] [CrossRef]
- Dwamena, B. MIDAS: Stata Module for Meta-Analytical Integration of Diagnostic Test Accuracy Studies; Boston College Department: Chestnut Hill, MA, USA, 2007. [Google Scholar]
- Hubers, A.J.; Heideman, D.A.M.; Herder, G.J.M.; Burgers, S.A.; Sterk, P.J.; Kunst, P.W.; Smit, H.J.; Postmus, P.E.; Witte, B.I.; Duin, S.; et al. Prolonged Sampling of Spontaneous Sputum Improves Sensitivity of Hypermethylation Analysis for Lung Cancer. J. Clin. Pathol. 2012, 65, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Hulbert, A.; Jusue-Torres, I.; Stark, A.; Chen, C.; Rodgers, K.; Lee, B.; Griffin, C.; Yang, A.; Huang, P.; Wrangle, J.; et al. Early Detection of Lung Cancer Using DNA Promoter Hypermethylation in Plasma and Sputum. Clin. Cancer Res. 2017, 23, 1998–2005. [Google Scholar] [CrossRef] [PubMed]
- Hubers, A.J.; Van Der Drift, M.A.; Prinsen, C.F.M.; Witte, B.I.; Wang, Y.; Shivapurkar, N.; Stastny, V.; Bolijn, A.S.; Hol, B.E.A.; Feng, Z.; et al. Methylation Analysis in Spontaneous Sputum for Lung Cancer Diagnosis. Lung Cancer 2014, 84, 127–133. [Google Scholar] [CrossRef]
- Li, N.; Dhilipkannah, P.; Jiang, F. High-Throughput Detection of Multiple miRNAs and Methylated DNA by Droplet Digital PCR. J. Pers. Med. 2021, 11, 359. [Google Scholar] [CrossRef]
- Shivapurkar, N.; Stastny, V.; Suzuki, M.; Wistuba, I.I.; Li, L.; Zheng, Y.; Feng, Z.; Hol, B.; Prinsen, C.; Thunnissen, F.B.; et al. Application of a Methylation Gene Panel by Quantitative PCR for Lung Cancers. Cancer Lett. 2007, 247, 56–71. [Google Scholar] [CrossRef]
- Shivapurkar, N.; Stastny, V.; Okumura, N.; Girard, L.; Xie, Y.; Prinsen, C.; Thunnissen, F.B.; Wistuba, I.I.; Czerniak, B.; Frenkel, E.; et al. Cytoglobin, the Newest Member of the Globin Family, Functions as a Tumor Suppressor Gene. Cancer Res. 2008, 68, 7448–7456. [Google Scholar] [CrossRef]
- van der Drift, M.A.; Prinsen, C.F.M.; Hol, B.E.A.; Bolijn, A.S.; Jeunink, M.a.F.; Dekhuijzen, P.N.R.; Thunnissen, F.B.J.M. Can Free DNA Be Detected in Sputum of Lung Cancer Patients? Lung Cancer Amst. Neth. 2008, 61, 385–390. [Google Scholar] [CrossRef]
- Shivapurkar, N.; Stastny, V.; Xie, Y.; Prinsen, C.; Frenkel, E.; Czerniak, B.; Thunnissen, F.B.; Minna, J.D.; Gazdar, A.F. Differential Methylation of a Short CpG-Rich Sequence within Exon 1 of TCF21 Gene: A Promising Cancer Biomarker Assay. Cancer Epidemiol. Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2008, 17, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.-H.; Kim, K.U.; Kim, J.-E.; Kim, H.-H.; Lee, M.K.; Lee, C.H.; Lee, S.-Y.; Oh, T.; An, S. Detection of HOXA9 Gene Methylation in Tumor Tissues and Induced Sputum Samples from Primary Lung Cancer Patients. Clin. Chem. Lab. Med. 2011, 49, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Hubers, A.J.; Brinkman, P.; Boksem, R.J.; Rhodius, R.J.; Witte, B.I.; Zwinderman, A.H.; Heideman, D.A.M.; Duin, S.; Koning, R.; Steenbergen, R.D.M.; et al. Combined Sputum Hypermethylation and eNose Analysis for Lung Cancer Diagnosis. J. Clin. Pathol. 2014, 67, 707–711. [Google Scholar] [CrossRef]
- Hubers, A.J.; Heideman, D.A.M.; Duin, S.; Witte, B.I.; De Koning, H.J.; Groen, H.J.M.; Prinsen, C.F.M.; Bolijn, A.S.; Wouters, M.; Van Der Meer, S.E.; et al. DNA Hypermethylation Analysis in Sputum of Asymptomatic Subjects at Risk for Lung Cancer Participating in the NELSON Trial: Argument for Maximum Screening Interval of 2 Years. J. Clin. Pathol. 2017, 70, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Fang, H.B.; Jiang, F. An Epigenetic Classifier for Early Stage Lung Cancer. Clin. Epigenetics 2018, 10, 68. [Google Scholar] [CrossRef] [PubMed]
- Anjuman, N.; Li, N.; Guarnera, M.; Stass, S.A.; Jiang, F. Evaluation of Lung Flute in Sputum Samples for Molecular Analysis of Lung Cancer. Clin. Transl. Med. 2013, 2, e15. [Google Scholar] [CrossRef] [PubMed]
- Weiszhar, Z.; Horvath, I. Induced Sputum Analysis: Step by Step. Breathe 2013, 9, 300–306. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 6.4 (updated August 2023); Cochrane: Calgary, AB, Canada, 2023. [Google Scholar]
- Borg, M.; Wen, S.W.C.; Andersen, R.F.; Timm, S.; Hansen, T.F.; Hilberg, O. Methylated Circulating Tumor DNA in Blood as a Tool for Diagnosing Lung Cancer: A Systematic Review and Meta-Analysis. Cancers 2023, 15, 3959. [Google Scholar] [CrossRef]
- Park, J.A.; Suzuki, K. Novel Screening Tools for Lung Cancer. Thorac. Surg. Clin. 2023, 33, 215–226. [Google Scholar] [CrossRef]
- Usman Ali, M.; Miller, J.; Peirson, L.; Fitzpatrick-Lewis, D.; Kenny, M.; Sherifali, D.; Raina, P. Screening for Lung Cancer: A Systematic Review and Meta-Analysis. Prev. Med. 2016, 89, 301–314. [Google Scholar] [CrossRef]
- Mokhles, S.; Takkenberg, J.J.; Treasure, T. Evidence-Based and Personalized Medicine. It’s [AND] Not [OR]. Ann. Thorac. Surg. 2017, 103, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Salfity, H.V.N.; Tong, B.C.; Kocher, M.R.; Tailor, T.D. Historical Perspective on Lung Cancer Screening. Thorac. Surg. Clin. 2023, 33, 309–321. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.; Ridge, C.A.; Nicholson, A.G.; Mirsadraee, S. The 8th Lung Cancer TNM Classification and Clinical Staging System: Review of the Changes and Clinical Implications. Quant. Imaging Med. Surg. 2018, 8, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Thurlbeck, W.M. Pathophysiology of Chronic Obstructive Pulmonary Disease. Clin. Chest Med. 1990, 11, 389–403. [Google Scholar] [CrossRef]
- Meddeb, R.; Pisareva, E.; Thierry, A.R. Guidelines for the Preanalytical Conditions for Analyzing Circulating Cell-Free DNA. Clin. Chem. 2019, 65, 623–633. [Google Scholar] [CrossRef]
- Sozzi, G.; Roz, L.; Conte, D.; Mariani, L.; Andriani, F.; Verderio, P.; Pastorino, U. Effects of Prolonged Storage of Whole Plasma or Isolated Plasma DNA on the Results of Circulating DNA Quantification Assays. JNCI J. Natl. Cancer Inst. 2005, 97, 1848–1850. [Google Scholar] [CrossRef]
- Thierry, A.R.; El Messaoudi, S.; Gahan, P.B.; Anker, P.; Stroun, M. Origins, Structures, and Functions of Circulating DNA in Oncology. Cancer Metastasis Rev. 2016, 35, 347–376. [Google Scholar] [CrossRef]
- Taylor, S.C.; Nadeau, K.; Abbasi, M.; Lachance, C.; Nguyen, M.; Fenrich, J. The Ultimate qPCR Experiment: Producing Publication Quality, Reproducible Data the First Time. Trends Biotechnol. 2019, 37, 761–774. [Google Scholar] [CrossRef]
- Yu, M.; Carter, K.T.; Makar, K.W.; Vickers, K.; Ulrich, C.M.; Schoen, R.E.; Brenner, D.; Markowitz, S.D.; Grady, W.M. MethyLight Droplet Digital PCR for Detection and Absolute Quantification of Infrequently Methylated Alleles. Epigenetics 2015, 10, 803–809. [Google Scholar] [CrossRef]
- Whale, A.S.; Devonshire, A.S.; Karlin-Neumann, G.; Regan, J.; Javier, L.; Cowen, S.; Fernandez-Gonzalez, A.; Jones, G.M.; Redshaw, N.; Beck, J.; et al. International Interlaboratory Digital PCR Study Demonstrating High Reproducibility for the Measurement of a Rare Sequence Variant. Anal. Chem. 2017, 89, 1724–1733. [Google Scholar] [CrossRef]
- Fahrmann, J.F.; Marsh, T.; Irajizad, E.; Patel, N.; Murage, E.; Vykoukal, J.; Dennison, J.B.; Do, K.-A.; Ostrin, E.; Spitz, M.R.; et al. Blood-Based Biomarker Panel for Personalized Lung Cancer Risk Assessment. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2022, 40, 876–883. [Google Scholar] [CrossRef] [PubMed]
- Leenen, F.A.D.; Muller, C.P.; Turner, J.D. DNA Methylation: Conducting the Orchestra from Exposure to Phenotype? Clin. Epigenetics 2016, 8, 92. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Region | Study Design | Cases | Histology | Stage | Controls | Cases (n) | Controls (n) | Reference Standard |
|---|---|---|---|---|---|---|---|---|---|
| Shivapurkar, 2007 [31] | Europe | Case–control study | Retrospectively selected patients with lung cancer | LUSC 8/13 (62%), LUAD 5/13 (38%) | I 2/13 (15%), II 2/13 (15%), III 4/13 (31%), IV 4/13 (31%), unknown 1/13 (8%) | Unmatched controls with benign diseases; other: four patients with prior lung cancer. | 13 | 25 | Histology or cytology not specified |
| Shivapurkar, 2008 A [32] | Europe | Case–control study | Retrospectively selected patients with lung cancer | Unknown 13/13 (100%) | Unknown 13/13 (100%) | Unmatched controls with benign diseases | 13 | 25 | Not described |
| van der Drift, 2008 [33] | Europe | Case–control study | Retrospectively selected patients with lung cancer | LUSC 13/28 (46%), LUAD 9/28 (32%), SCLC 4/28 (14%), other 2/28 (7%%) | I 4/28 (14%), II 5/28 (18%), III 4/28 (14%), IV 6/28 (21%), unknown 9/28 (32%) | Unmatched controls with benign diseases | 28 | 68 | Histology or cytology not specified |
| Shivapurkar, 2008 B [34] | Europe | Case–control study | Retrospectively selected patients with lung cancer | Unknown 13/13 (100%) | Unknown 13/13 (100%) | Unmatched controls with benign diseases | 13 | 25 | Not described |
| Hwang, 2011 [35] | Asia | Case–control study | Retrospectively selected patients with lung cancer | LUSC 34/76 (45%), LUAD 42/76 (55%) | I 14/76 (18%), II 5/76 (7%), III 28/76 (37%), IV 29/76 (38%) | Unmatched, healthy controls; unmatched controls with benign diseases | 76 | 109 | Histology or cytology not specified |
| Hubers, 2012 [27] | Europe | Cohort study | Lung cancer cases from a cohort study | Unknown 53/53 (100%) | Unknown 53/53 (100%) | Non-cancer participants from a cohort study | 53 | 47 | Not described |
| Leng, 2012 [19] | North America | Case–control study | Retrospectively selected patients with lung cancer | Cohort 1: unknown 64/64 (100%). | Cohort 1: unknown 64/64 (100%). | Matched on certain characteristics | Cohort 1: 64. | Cohort 1: 64. | Not described |
| Cohort 2: unknown 40/40 (100%) | Cohort 2: Stage I 40/40 (100%) | Cohort 2: 40 | Cohort 2: 90. | Histopathology of surgery specimen | |||||
| Hubers, 2014 A [36] | Europe | Case–control study | Retrospectively selected patients with lung cancer | LUSC 6/20 (30%), LUAD 7/20 (35%), SCLC 1/20 (5%), other 6/20 (30%) | I 1/20 (5%), II 3/20 (15%), III 9/20 (45%), IV 7/20 (35%) | Unmatched controls with benign diseases | 20 | 31 | Histology or cytology not specified |
| Hubers, 2014 B [29] | Europe | Case–control study | Retrospectively selected patients with lung cancer | Cohort 1: unknown 98/98 (100%). | Cohort 1: unknown 98/98 (100%). | Matched on certain characteristics | Cohort 1: 98. | Cohort 1: 90. | Not described |
| Cohort 2: Unknown 60/60 (100%) | Cohort 2: 60/60 (100%) | Cohort 2: 60 | Cohort 2: 445. | Not described | |||||
| Hubers, 2015 [18] | Europe | Case–control study | Lung cancer patients at diagnosis but also at progression on treatment | Cohort 1: LUSC 31/73 (42%), LUAD 26/73 (36%), SCLC 1/73 (1%), other 15/73 (21%). | Cohort 1: I 14/73 (19%), II 9/73 (12%), III 24/73 (33%), IV 25/73 (34%), unknown 1/73 (1%). | Unmatched controls with benign diseases; patients with benign diseases; patients who had surgery for lung cancer and remained cancer-free for 3 years. | Cohort 1: 73. | Cohort 1: 86. | Histology or cytology not specified |
| Cohort 2: LUSC 50/159 (31%), LUAD 66/159 (42%), SCLC 6/159 (1%), other 37/159 (23%) | Cohort 2: I 29/159 (18%), II 17/159 (11%), III 47/159 (30%), IV 66/159 (42%) | Cohort 2: 159 | Cohort 2: 154. | Histology or cytology not specified | |||||
| Su, 2016 [20] | Asia | Case–control study | Retrospectively selected patients with lung cancer | LUSC 54/117 (46%), LUAD 63/117 (54%) | I 117/117 (100%) | Matched on certain characteristics | 117 | 174 | Histopathology of tissue biopsy or surgery specimen |
| Hubers, 2017 [37] | Europe | Case–control study | Lung cancer cohort from another study | LUSC 7/56 (13%), LUAD 34/56 (61%), SCLC 2/56 (4%), other 8/56 (14%), unknown 5/56 (9%) | I 36/56 (64%), II 4/56 (7%), III 6/56 (11%), IV 10/56 (18%) | Non-cancer participants from a cohort study | 56 | 217 | Histopathology of tissue biopsy; cytology |
| Hulbert, 2017 [28] | North America | Cohort study | Lung cancer cases from a cohort study | Unknown 90/90 (100%) | Unknown 90/90 (100%) | Non-cancer participants from a cohort study | 90 | 24 | Histopathology of surgery specimen |
| Su, 2018 [38] | Asia | Case–control study | Retrospectively selected patients with lung cancer | LUSC 57/127 (45%), LUAD 63/127 (50%), other 7/127 (6%) | I 33/127 (26%), II 32/127 (25%), III 29/127 (23%), IV 33/127 (26%) | Matched on certain characteristics | 127 | 159 | Histopathology of tissue biopsy or surgery specimen |
| Li, 2021 [30] | North America | Cohort study | Lung cancer cases from a cohort study | Cohort 1: LUSC 18/40 (45%), LUAD 22/40 (55%). | Cohort 1: I 13/40 (33%), II 13/40 (33%), III–IV 14/40 (35%). | Non-cancer participants from a cohort study | Cohort 1: 40. | Cohort 1: 36. | Histology or cytology not specified |
| Cohort 2: LUSC 16/36 (44%), LUAD 20/36 (56%) | Cohort 2: I 13/36 (36%), II 12/36 (33%), III–IV 11/36 (31%). | Cohort 2: 36. | Cohort 2: 39. | Histology or cytology not specified |
| Study ID | Was the DNA Extraction Kit Name Reported? | Analysis Method | Were the Primer Sequences Reported? | Were the Probe Sequences Reported? | Were the Reaction Volume and Amount of DNA Reported? | Were the Complete Thermocycling Parameters Reported? | Assay Type | Were the Calibration Curves or Serial Dilutions Reported? | How Was the Cutoff Determined? |
|---|---|---|---|---|---|---|---|---|---|
| Shivapurkar, 2007 [31] | Yes | QMSP | Yes | Yes | Yes | Yes | Singleplex | Yes | Defined by a training cohort (unvalidated) |
| Shivapurkar, 2008 A [32] | Yes | QMSP | Yes | Yes | Yes | Yes | Singleplex | No | Defined in a previous study |
| van der Drift, 2008 [33] | Yes | QMSP | Yes | Yes | Yes | Yes | Singleplex | No | Not described |
| Shivapurkar, 2008 B [34] | Yes | QMSP | Yes | Yes | Yes | Yes | Singleplex | No | Defined in a previous study |
| Hwang, 2011 [35] | No | Sequencing | Yes | N/A | Yes | Yes | Singleplex | N/A | Not described |
| Hubers, 2012 [27] | Yes | QMSP | Yes | Yes | Yes | Yes | Multiplex | Yes | Arbitrarily set at a specific level of sensitivity or specificity |
| Leng, 2012 [19] | Yes | QMSP | Yes | No | No | No | Not described | No | Defined by a training cohort (unvalidated) |
| Hubers, 2014 A [36] | No | QMSP | No | No | No | No | Not described | No | Defined in a previous study |
| Hubers, 2014 B [29] | Yes | QMSP | Yes | Yes | No | Yes | Singleplex | Yes | Defined in a previous study |
| Hubers, 2015 [18] | Yes | QMSP | Yes | Yes | Yes | Yes | Singleplex Multiplex | No | Defined by a training cohort and validated in an independent cohort |
| Su, 2016 [20] | Yes | QMSP | Yes | Yes | No | No | Not described | No | Not described |
| Hubers, 2017 [37] | Yes | QMSP | Yes | Yes | Yes | Yes | Multiplex | Yes | Defined in a previous study |
| Hulbert, 2017 [28] | Yes | QMSP | Yes | Yes | Yes | Yes | Not described | No | Sensitivity and specificity values were obtained from the presence or absence of detectable methylation as a cutoff. |
| Su, 2018 [38] | Yes | Digital PCR | Yes | Yes | Yes | Yes | Not described | Yes | Defined by a training cohort and validated in an independent cohort |
| Li, 2021 [30] | Yes | Digital PCR | Yes | N/A | No | Yes | Not described | Yes | Defined in a previous study |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wen, S.W.C.; Borg, M.; Timm, S.; Hansen, T.F.; Hilberg, O.; Andersen, R.F. Methylated Cell-Free Tumor DNA in Sputum as a Tool for Diagnosing Lung Cancer—A Systematic Review and Meta-Analysis. Cancers 2024, 16, 506. https://doi.org/10.3390/cancers16030506
Wen SWC, Borg M, Timm S, Hansen TF, Hilberg O, Andersen RF. Methylated Cell-Free Tumor DNA in Sputum as a Tool for Diagnosing Lung Cancer—A Systematic Review and Meta-Analysis. Cancers. 2024; 16(3):506. https://doi.org/10.3390/cancers16030506
Chicago/Turabian StyleWen, Sara Witting Christensen, Morten Borg, Signe Timm, Torben Frøstrup Hansen, Ole Hilberg, and Rikke Fredslund Andersen. 2024. "Methylated Cell-Free Tumor DNA in Sputum as a Tool for Diagnosing Lung Cancer—A Systematic Review and Meta-Analysis" Cancers 16, no. 3: 506. https://doi.org/10.3390/cancers16030506
APA StyleWen, S. W. C., Borg, M., Timm, S., Hansen, T. F., Hilberg, O., & Andersen, R. F. (2024). Methylated Cell-Free Tumor DNA in Sputum as a Tool for Diagnosing Lung Cancer—A Systematic Review and Meta-Analysis. Cancers, 16(3), 506. https://doi.org/10.3390/cancers16030506