


The Impact of FDA-Approved Novel Agents for Steroid-Refractory Chronic Graft vs. Host Disease on Treatment Patterns and Outcomes—A Single-Center Longitudinal Cohort Analysis
 ,
,
Simple Summary
Abstract
1. Introduction
2. Methods
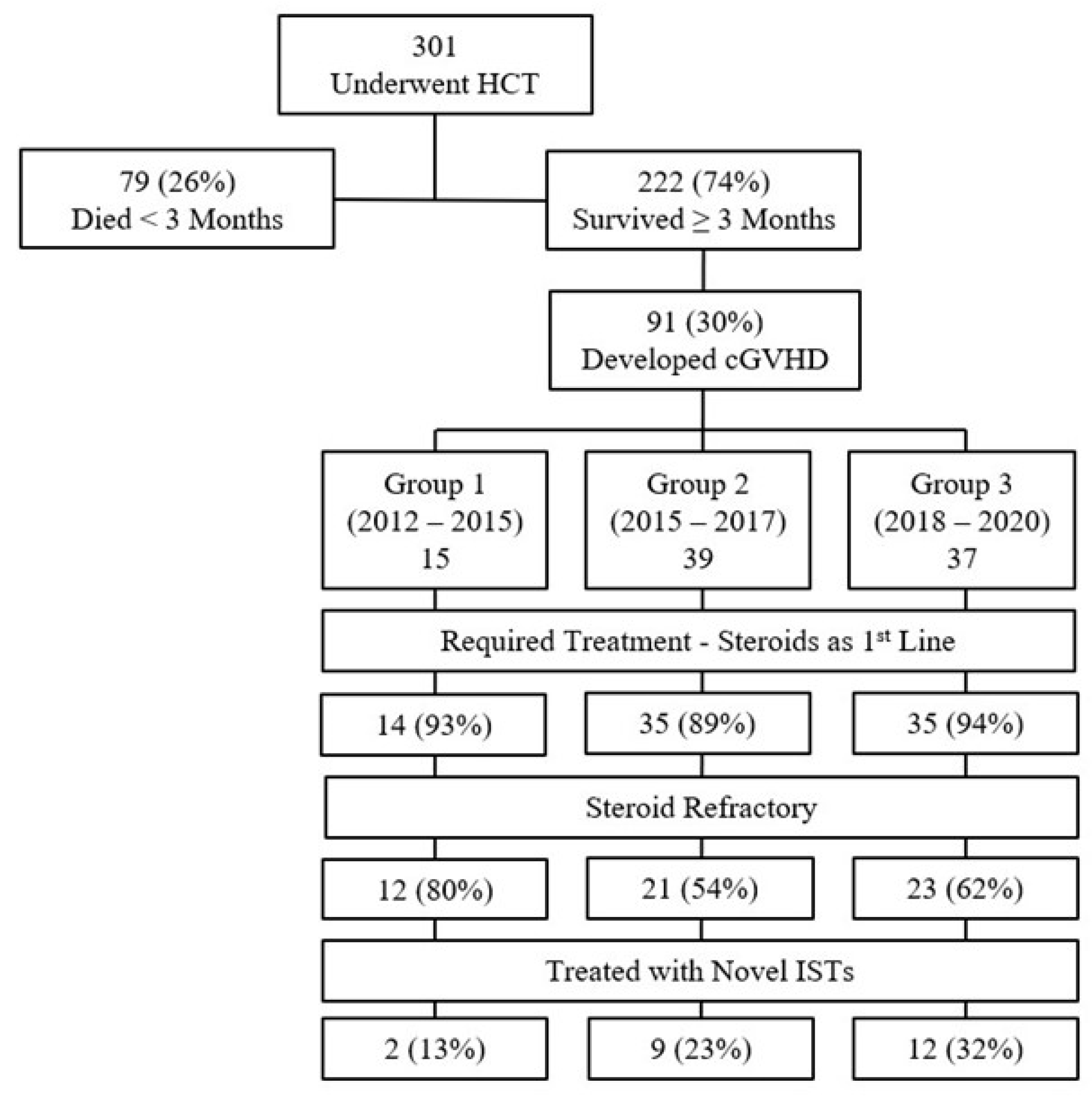
2.1. Patients and Initial Treatment for Chronic GVHD
2.2. Second Line Treatment
2.3. Evaluation and Definition of Outcomes
2.4. Supportive Care
2.5. Statistical Analysis
3. Results
3.1. Patient and Chronic GVHD Characteristics
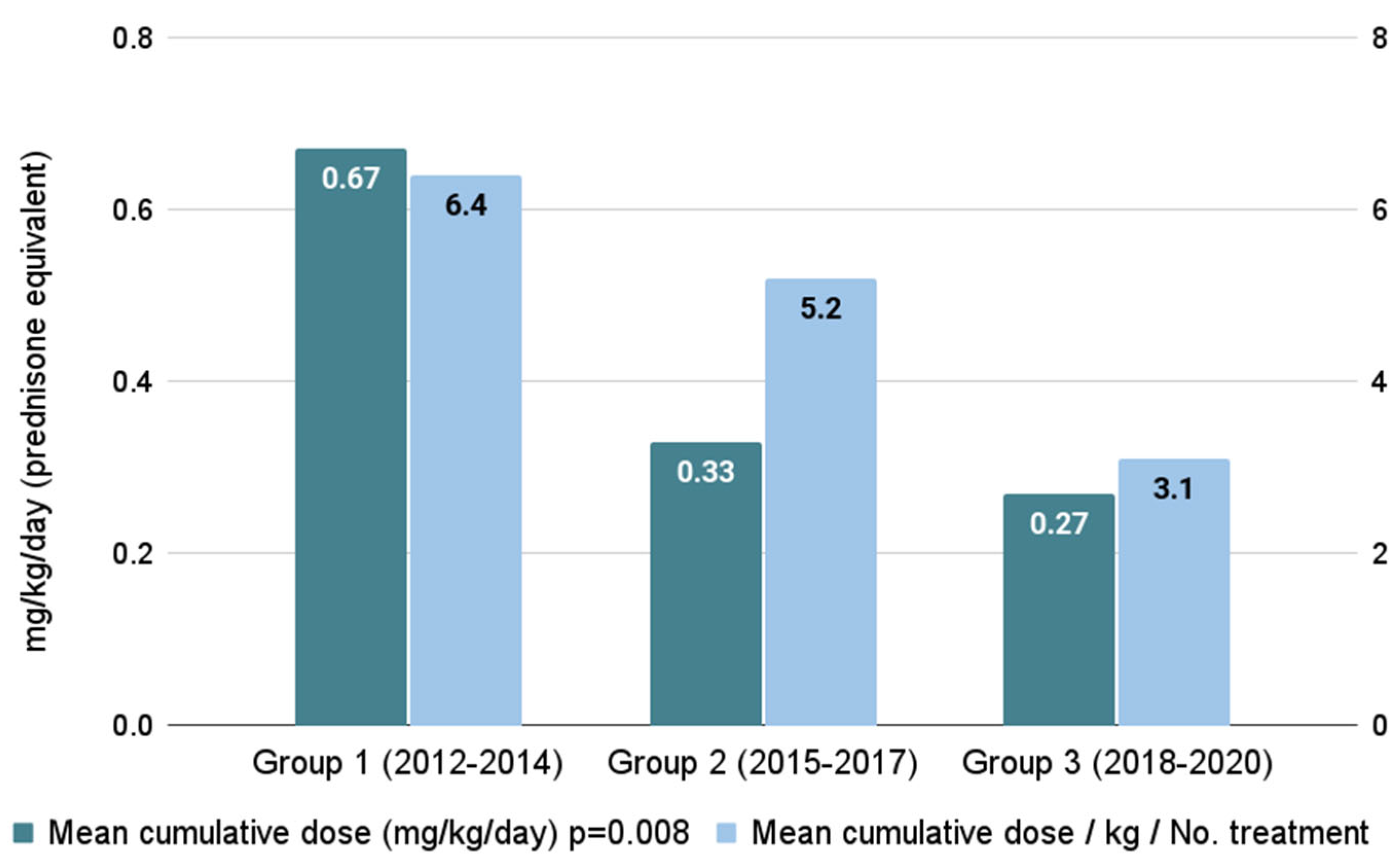
3.2. Steroid Burden and Subsequent Treatment Patterns
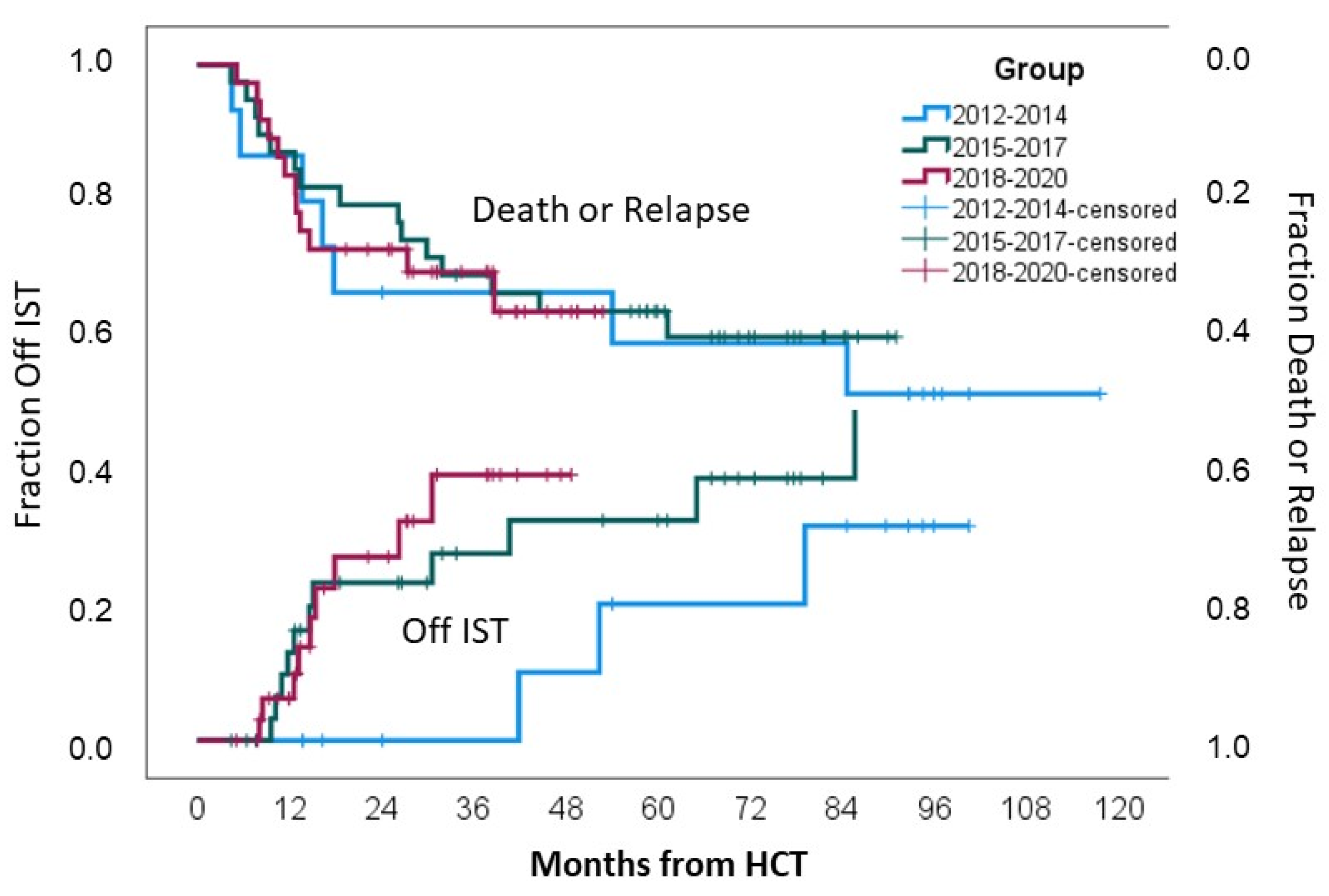
3.3. Long-Term Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zeiser, R.; Blazar, B.R. Pathophysiology of Chronic Graft-versus-Host Disease and Therapeutic Targets. N. Engl. J. Med. 2017, 377, 2565–2579. [Google Scholar] [CrossRef]
- Cooke, K.R.; Luznik, L.; Sarantopoulos, S.; Hakim, F.T.; Jagasia, M.; Fowler, D.H.; Van Den Brink, M.R.; Hansen, J.A.; Parkman, R.; Miklos, D.B.; et al. The Biology of Chronic Graft-versus-Host Disease: A Task Force Report from the National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2017, 23, 211–234. [Google Scholar] [CrossRef]
- Csanadi, M.; Agh, T.; Tordai, A.; Webb, T.; Jeyakumaran, D.; Sengupta, N.; Schain, F.; Mattsson, J. A systematic literature review of incidence, mortality, and relapse of patients diagnosed with chronic graft versus host disease. Expert Rev. Hematol. 2019, 12, 311–323. [Google Scholar] [CrossRef]
- Axt, L.; Naumann, A.; Toennies, J.; Haen, S.P.; Vogel, W.; Schneidawind, D.; Wirths, S.; Moehle, R.; Faul, C.; Kanz, L.; et al. Retrospective single center analysis of outcome, risk factors and therapy in steroid refractory graft-versus-host disease after allogeneic hematopoietic cell transplantation. Bone Marrow Transplant. 2019, 54, 1805–1814. [Google Scholar] [CrossRef]
- Zeiser, R.; Polverelli, N.; Ram, R.; Hashmi, S.K.; Chakraverty, R.; Middeke, J.M.; Musso, M.; Giebel, S.; Uzay, A.; Langmuir, P.; et al. Ruxolitinib for Glucocorticoid-Refractory Chronic Graft-versus-Host disease. N. Engl. J. Med. 2021, 385, 228–238. [Google Scholar] [CrossRef]
- Martini, D.J.; Chen, Y.; DeFilipp, Z. Recent FDA approvals in the treatment of Graft-Versus-Host disease. Oncologist 2022, 27, 685–693. [Google Scholar] [CrossRef]
- Waller, E.K.; Miklos, D.; Cutler, C.; Arora, M.; Jagasia, M.H.; Pusic, I.; Flowers, M.E.; Logan, A.C.; Nakamura, R.; Chang, S.; et al. Ibrutinib for chronic Graft-versus-Host disease after failure of prior therapy: 1-Year update of a Phase 1b/2 study. Biol. Blood Marrow Transplant. 2019, 25, 2002–2007. [Google Scholar] [CrossRef]
- Cutler, C.; Lee, S.J.; Arai, S.; Rotta, M.; Zoghi, B.; Ramakrishnan, A.; Lazaryan, A.; Eiznhamer, D.A.; Schueller, O.; Yang, Z.; et al. Belumosudil for Chronic Graft-Versus-Host Disease (cGVHD) after 2 or More Prior Lines of Therapy: The Rockstar Study (KD025-213). Transplant. Cell. Ther. 2021, 27, S7–S8. [Google Scholar] [CrossRef]
- Wang, D.; Liu, Y.; Lai, X.; Chen, J.; Cheng, Q.; Ma, X.; Lin, Z.; Wu, D.; Xu, Y. Efficiency and toxicity of ruxolitinib as a salvage treatment for Steroid-Refractory Chronic Graft-Versus-Host Disease. Front. Immunol. 2021, 12, 673636. [Google Scholar] [CrossRef]
- Elli, E.M.; Baratè, C.; Mendicino, F.; Palandri, F.; Palumbo, G.A. Mechanisms underlying the anti-inflammatory and immunosuppressive activity of ruxolitinib. Front. Oncol. 2019, 9, 1186. [Google Scholar] [CrossRef]
- Dubovsky, J.A.; Flynn, R.; Du, J.; Harrington, B.K.; Zhong, Y.; Kaffenberger, B.; Yang, C.; Towns, W.H.; Lehman, A.; Johnson, A.J.; et al. Ibrutinib treatment ameliorates murine chronic graft-versus-host disease. J. Clin. Investig. 2014, 124, 4867–4876. [Google Scholar] [CrossRef]
- Flynn, R.; Paz, K.; Du, J.; Reichenbach, D.K.; Taylor, P.A.; Panoskaltsis-Mortari, A.; Vulic, A.; Luznik, L.; MacDonald KK, P.; Hill, G.R.; et al. Targeted Rho-associated kinase 2 inhibition suppresses murine and human chronic GVHD through a Stat3-dependent mechanism. Blood 2016, 127, 2144–2154. [Google Scholar] [CrossRef]
- Zeiser, R.; Burchert, A.; Lengerke, C.; Verbeek, M.; Maas-Bauer, K.; Metzelder, S.K.; Spoerl, S.; Ditschkowski, M.; Ecsedi, M.; Sockel, K.; et al. Ruxolitinib in corticosteroid-refractory graft-versus-host disease after allogeneic stem cell transplantation: A multicenter survey. Leukemia 2015, 29, 2062–2068. [Google Scholar] [CrossRef]
- Filipovich, A.H.; Weisdorf, D.; Pavletic, S.; Socie, G.; Wingard, J.R.; Lee, S.J.; Martin, P.; Chien, J.; Przepiorka, D.; Couriel, D.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-Versus-Host Disease: I. Diagnosis and Staging Working Group Report. Biol. Blood Marrow Transplant. 2005, 11, 945–956. [Google Scholar] [CrossRef]
- Jagasia, M.H.; Greinix, H.T.; Arora, M.; Williams, K.M.; Wolff, D.; Cowen, E.W.; Palmer, J.; Weisdorf, D.; Treister, N.S.; Cheng, G.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-Versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group Report. Biol. Blood Marrow Transplant. 2015, 21, 389–401.e1. [Google Scholar] [CrossRef]
- DeFilipp, Z.; Couriel, D.R.; Lazaryan, A.; Bhatt, V.R.; Buxbaum, N.P.; Alousi, A.M.; Olivieri, A.; Pulanic, D.; Halter, J.P.; Henderson, L.A.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-Versus-Host Disease: III. The 2020 Treatment of Chronic GVHD Report. Transplant. Cell. Ther. 2021, 27, 729–737. [Google Scholar] [CrossRef]
- Couriel, D.; Carpenter, P.A.; Cutler, C.; Bolaños-Meade, J.; Treister, N.S.; Gea-Banacloche, J.; Shaughnessy, P.; Hymes, S.; Kim, S.; Wayne, A.S.; et al. Ancillary Therapy and Supportive Care of Chronic Graft-versus-Host Disease: National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: V. Ancillary Therapy and Supportive Care Working Group Report. Biol. Blood Marrow Transplant. 2006, 12, 375–396. [Google Scholar] [CrossRef]
- D’Souza, A.; Fretham, C.; Lee, S.J.; Arora, M.; Brunner, J.; Chhabra, S.; Devine, S.; Eapen, M.; Hamadani, M.; Hari, P.; et al. Current use of and trends in hematopoietic cell transplantation in the United States. Biol. Blood Marrow Transplant. 2020, 26, e177–e182. [Google Scholar] [CrossRef]
- Yu, J.; Khera, N.; Turnbull, J.; Stewart, S.K.; Williams, P.; Bhatt, V.; Meyers, O.; Galvin, J.; Lee, S.J. Impact of Chronic Graft-Versus-Host disease on patient employment, income, and informal caregiver burden: Findings from the Living with Chronic GVHD Patient Survey. Transplant. Cell. Ther. 2023, 29, 470.e1–470.e9. [Google Scholar] [CrossRef]
- Yu, J.; Lal, L.S.; Anderson, A.; DuCharme, M.; Parasuraman, S.; Weisdorf, D. Healthcare resource utilization and costs among patients with steroid-resistant chronic graft-versus-host disease in the United States: A retrospective claims database analysis. Curr. Med. Res. Opin. 2021, 37, 755–759. [Google Scholar] [CrossRef]
- Leung GM, K.; Sim JP, Y.; Hwang, Y.; Chan TS, Y.; Lie AK, W.; Tse, E.; Kwong, Y. Ruxolitinib in the management of steroid-resistant/-dependent acute and chronic graft-versus-host disease: Results of routine practice in an academic centre. Ann. Hematol. 2021, 101, 155–163. [Google Scholar] [CrossRef]
- White, J.; Elemary, M.; Linn, S.M.; Novitzky-Basso, I.; Culos, S.; Tan, S.K.; Kelly, K.; Deotare, U.; Xenocostas, A.; Hamad, N.; et al. A multicenter, retrospective study evaluating clinical outcomes of ruxolitinib therapy in heavily pretreated chronic GVHD patients with steroid failure. Transplant. Cell. Ther. 2023, 29, 120.e1–120.e9. [Google Scholar] [CrossRef]
- Defilipp, Z.; Duarte, R.F.; Snowden, J.A.; Majhail, N.S.; Greenfield, D.M.; Miranda, J.L. Metabolic Syndrome and Cardiovascular Disease Following Hematopoietic Cell Transplantation: Screening and Preventive Practice Recommendations from CIBMTR and EBMT. Bone Marrow Transplant. 2017, 52, 173–182. [Google Scholar] [CrossRef]
- Majhail, N.S.; Flowers, M.E.; Ness, K.K.; Jagasia, M.; Carpenter, P.A.; Arora, M.; Arai, S.; Johnston, L.; Martin, P.J.; Baker, K.S.; et al. High prevalence of metabolic syndrome after allogeneic hematopoietic cell transplantation. Bone Marrow Transplant. 2008, 43, 49–54. [Google Scholar] [CrossRef]
- Zhao, A.T.; Pirsl, F.; Steinberg, S.M.; Holtzman, N.G.; Schulz, E.; Mina, A.; Mays, J.W.; Cowen, E.W.; Comis, L.E.; Joe, G.O.; et al. Metabolic syndrome prevalence and impact on outcomes in patients with chronic graft-versus-host disease. Bone Marrow Transplant. 2023, 58, 1377–1383. [Google Scholar] [CrossRef]
- Fatobene, G.; Storer, B.E.; Salit, R.B. Disability Related to Chronic Graft-versus-Host Disease after Alternative Donor Hematopoietic Cell Transplantation. Haematologica 2019, 104, 835–843. [Google Scholar] [CrossRef]
- Hamilton, B.K.; Storer, B.E.; Wood, W.A.; Pidala, J.A.; Cutler, C.S.; Martin, P.J.; Chen, G.; Flowers, M.E.; Lee, S.J. Disability Related to Chronic Graft-versus-Host Disease. Biol. Blood Marrow Transplant. J. Am. Soc. Blood Marrow Transplant. 2020, 26, 772–777. [Google Scholar] [CrossRef]
- Hamilton, B.K.; Williams, P.; Galvin, J.; Turnbull, J.; Yu, J. Disability Associated with Chronic Graft-versus-Host Disease after Allogeneic Hematopoietic Stem Cell Transplantation: Analysis of a Cross-Sectional US Patient Survey. Oncol. Ther. 2024, 12, 451–464. [Google Scholar] [CrossRef]
- DeFilipp, Z.; Alousi, A.M.; Pidala, J.A.; Carpenter, P.A.; Onstad, L.E.; Arai, S.; Arora, M.; Cutler, C.S.; Flowers ME, D.; Kitko, C.L.; et al. Nonrelapse mortality among patients diagnosed with chronic GVHD: An updated analysis from the Chronic GVHD Consortium. Blood Adv. 2021, 5, 4278–4284. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Domain | All Cohort 2012–2020 (n = 91) | Group 1 2012–2014 (n = 15) | Group 2 2015–2017 (n = 39) | Group 3 2018–2020 (n = 37) | |
|---|---|---|---|---|---|
| Age (mean, ±SD) | 50 ± 15.5 | 43 ± 15.6 | 45 ± 14.2 | 57 ± 14.1 | |
| Sex (Female, %) | 39, 43% | 8, 53% | 18, 46% | 13, 35% | |
| Disease (N, %) | AML | 48, 53% | 6, 40% | 22, 56% | 20, 54% |
| ALL | 16, 18% | 5, 33% | 8, 21% | 3, 8% | |
| Lymphoma | 10, 10% | 0, 0% | 5, 13% | 5, 14% | |
| MDS | 8, 9% | 2, 13% | 2, 5% | 4, 11% | |
| Other | 9, 10% | 2, 13% | 2, 5% | 5, 14% | |
| Conditioning, myeloablative (N, %) | 52, 57% | 13, 87% | 24, 62% | 15, 41% | |
| Donor (N, %) | URD, 10/10 | 53, 58% | 5, 33% | 22, 56% | 25, 68% |
| URD, 9/10 | 3, 3% | 3, 20% | 1, 3% | 0 | |
| Matched sibling | 33, 37% | 7, 47% | 15, 39% | 11, 30% | |
| Haploidentical | 1, 1% | 0 | 0 | 1, 1% | |
| Cord blood | 1, 1% | 0 | 1, 3% | 0 | |
| Female to male | 19, 21% | 3, 20% | 11, 28% | 8, 22% | |
| cGVHD characteristics (N, %) | De novo | 59, 65% | 12, 80% | 27, 69% | 20, 54% |
| Quiescent | 12, 13% | 1, 7% | 4, 10% | 7, 19% | |
| Progressive | 20, 22% | 2, 13% | 8, 20% | 10, 27% | |
| cGVHD Grading (N, %) | Mild | 14, 15% | 1, 7% | 8, 20% | 5, 13% |
| Moderate | 32, 35% | 4, 27% | 11, 28% | 17, 46% | |
| Severe | 45, 49% | 10, 67% | 20, 51% | 15, 40% | |
| ECOG 0-1 (N, %) | 74, 81% | 9, 60% | 29, 74% | 36, 97% | |
| Organ Involvement (N, %) | Skin | 76, 84% | 15, 100% | 33, 85% | 28, 76% |
| Mouth | 78, 86% | 13, 87% | 37, 94% | 28, 76% | |
| Eyes | 64, 70% | 13, 87% | 30, 77% | 21, 57% | |
| Gastrointestinal | 38, 42% | 9, 60% | 12, 31% | 17, 46% | |
| Liver | 41, 45% | 7, 47% | 17, 44% | 17, 46% | |
| Lungs | 26, 29% | 7, 47% | 11, 28% | 8, 22% | |
| Joints/Fascia | 39, 43% | 9, 60% | 16, 41% | 14, 38% | |
| Genital (female) | 20, 22% | 5, 33% | 11, 28% | 4, 11% | |
| Other | 3, 3% | 0 | 2, 5% | 1, 3% | |
| Eosinophilia | 9, 10% | 1, 7% | 3, 8% | 5, 14% | |
| Thrombocytopenia | 29, 32% | 6, 40% | 7, 18% | 16, 43% | |
| Domain | Group 1 2012–2014 (n = 15) | Group 2 2015–2017 (n = 39) | Group 3 2018–2020 (n = 37) | p-Value |
|---|---|---|---|---|
| Steroid-refractory | 12, 80% | 21, 54% | 23, 62% | 0.21 |
| Novel agent | ||||
| Second line | 0 | 4, 10% | 9, 24% | 0.14 |
| Second/third line | 2, 13% | 9, 23% | 12, 32% | 0.31 |
| Median months to second line ◊ (IQR) | 4.3 (1.7–11.2) | 8.2 (2.9–20.1) | 3.3 (1.3–16.5) | 0.07 |
| Discontinuation of IST at 36 months (CI) | 20% (0–45%) | 34% (21–47%) | 47% (25–54%) | 0.11 |
| Maximal HbA1C (mg/dL) | 6.5 ± 0.83 | 5.9 ± 0.69 | 5.7 ± 0.85 | <0.01 |
| CVA—n, % | 1, 7% | 1, 3% | 1, 3% | 0.73 |
| MI/onset of IHD—n, % | 4, 26% | 4, 10% | 3, 8% | 0.16 |
| Bone density ¶—n, % | 0.06 | |||
| Osteopenia | 4, 31% | 14, 39% | 12, 38% | |
| Osteoporosis | 8, 62% | 12, 33% | 5, 16% | |
| Number of admissions\year | 0.7 | 0.24 | 0.36 | <0.001 |
| Return to work | ||||
| N patients, % | 3, 20% | 22, 56% | 16, 43% | 0.05 |
| Months from HCT (mean) | 29 ± 9.8 | 11.9 ± 4.3 | 9.5 ± 3.8 | 0.01 |
| Depression/anxiety—n, % | 6, 53% | 14, 40% | 10, 27% | 0.58 |
| 3-year relapse incidence (CI) ◊ | 14% (5–19%) | 12% (6–18%) | 25% (8–42%) | 0.54 |
| 3-year NRM (95%CI) ◊ | 14% (3–25%) | 17% (4–30%) | 26% (8–42%) | 0.69 |
| 3-year OS (95%CI) * | 66% (56–76%) | 74% (60–88%) | 63% (41–85%) | 0.68 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fridberg, G.; Amit, O.; Karni, C.; Tshernichovsky, D.; Shasha, D.; Rouach, V.; Varssano, D.; Bar-Shai, A.; Goldberg, I.; Wasserman, G.; et al. The Impact of FDA-Approved Novel Agents for Steroid-Refractory Chronic Graft vs. Host Disease on Treatment Patterns and Outcomes—A Single-Center Longitudinal Cohort Analysis. Cancers 2024, 16, 3521. https://doi.org/10.3390/cancers16203521
Fridberg G, Amit O, Karni C, Tshernichovsky D, Shasha D, Rouach V, Varssano D, Bar-Shai A, Goldberg I, Wasserman G, et al. The Impact of FDA-Approved Novel Agents for Steroid-Refractory Chronic Graft vs. Host Disease on Treatment Patterns and Outcomes—A Single-Center Longitudinal Cohort Analysis. Cancers. 2024; 16(20):3521. https://doi.org/10.3390/cancers16203521
Chicago/Turabian StyleFridberg, Gil, Odelia Amit, Chen Karni, Dina Tshernichovsky, David Shasha, Vanessa Rouach, David Varssano, Amir Bar-Shai, Ilan Goldberg, Gilad Wasserman, and et al. 2024. "The Impact of FDA-Approved Novel Agents for Steroid-Refractory Chronic Graft vs. Host Disease on Treatment Patterns and Outcomes—A Single-Center Longitudinal Cohort Analysis" Cancers 16, no. 20: 3521. https://doi.org/10.3390/cancers16203521
APA StyleFridberg, G., Amit, O., Karni, C., Tshernichovsky, D., Shasha, D., Rouach, V., Varssano, D., Bar-Shai, A., Goldberg, I., Wasserman, G., Avivi, I., & Ram, R. (2024). The Impact of FDA-Approved Novel Agents for Steroid-Refractory Chronic Graft vs. Host Disease on Treatment Patterns and Outcomes—A Single-Center Longitudinal Cohort Analysis. Cancers, 16(20), 3521. https://doi.org/10.3390/cancers16203521