Simple Summary
Extra-prostatic extension (EPE) is a well-known poor prognostic factor of prostate cancer. As such, accurate radiological diagnosis of EPE is important for urology surgeons due to its surgical implications prior to radical prostatectomy. T2-weighted imaging (T2WI) is a key sequence in prostate MRI for evaluating EPE. Recent technical advancements have allowed for the acquisition of thin-slice T2WI with resultant increased image noise. Deep learning reconstruction (DLR) techniques have been used to decrease the image noise in MRI; however, previous studies have focused mainly on image quality or acquisition times, and the efficacy of DLR regarding the diagnostic performance for EPE has not yet been reported. Our observations reveal that conventional 3 mm T2WI was better than 2 mm thin-slice T2WI with DLR with respect to diagnostic performance for EPE and image quality, thus supporting the minimal technical requirements described in the prostate imaging quality guidelines.
Abstract
The aim of this study was to compare diagnostic performance for extra-prostatic extension (EPE) and image quality among three image datasets: conventional T2-weighted images (T2WIconv, slice thickness, 3 mm) and high-resolution thin-slice T2WI (T2WIHR, 2 mm), with and without deep learning reconstruction (DLR) in patients with prostatic cancer (PCa). A total of 88 consecutive patients (28 EPE-positive and 60 negative) diagnosed with PCa via radical prostatectomy who had undergone 3T-MRI were included. Two independent reviewers performed a crossover review in three sessions, in which each reviewer recorded five-point confidence scores for the presence of EPE and image quality using a five-point Likert scale. Pathologic topographic maps served as the reference standard. For both reviewers, T2WIconv showed better diagnostic performance than T2WIHR with and without DLR (AUCs, in order, for reviewer 1, 0.883, 0.806, and 0.772, p = 0.0006; for reviewer 2, 0.803, 0.762, and 0.745, p = 0.022). The image quality was also the best in T2WIconv, followed by T2WIHR with DLR and T2WIHR without DLR for both reviewers (median, in order, 3, 4, and 5, p < 0.0001). In conclusion, T2WIconv was optimal in regard to image quality and diagnostic performance for the evaluation of EPE in patients with PCa.
1. Introduction
Multi-parametric MRI of the prostate gland is a cornerstone in the diagnosis and evaluation of prostate cancer (PCa). Although technical requirements have been given in the second version of Prostate Imaging-Reporting and Data System (PI-RADS v.2.1), the prostate MRI parameters of acquisition and scan quality vary between different institutions [1,2,3]. However, as the detection of PCa is impaired by poor image quality and artifacts in the acquired images, methods for image optimization have been studied [4,5]. To facilitate the improvement in the image quality of prostate MRI, the Prostate Imaging Quality (PI-QUAL) score has been introduced, including minimal technical requirements described in the PI-RADS, as well as several criteria for visual assessment [3,6].
T2-weighted imaging (T2WI) is a key sequence in multi-parametric MRI, which is important in the evaluation of the zonal anatomy of the prostate gland and neighboring structures, extra-prostatic extension (EPE), seminal vesical and neurovascular bundle invasion, as well as playing a role as the dominant sequence for the evaluation of transitional zone (TZ) malignancies [7]. Of these, EPE is a well-known poor prognostic factor, and so the accurate radiological diagnosis of EPE is important for urology surgeons due to its surgical implications for surgical planning prior to radical prostatectomy [8,9].
The minimal technical requirements of PI-QUAL for T2WI are ≤0.4 mm in the frequency-encoding direction, ≤0.7 mm in the phase-encoding direction for in-plane resolution, and 3 mm for slice thickness (ST) [6]. Recent technical advancements in MRI have allowed for the acquisition of three-dimensional (3D) T2WI with resultant thinner STs. Previous studies have reported the comparable performance of 3D-T2WI to conventional T2WI regarding the diagnosis and characterization of prostate cancer and evaluation of EPE [10,11,12]. A potential drawback of thin-slice T2WI is a decrease in the signal-to-noise ratio (SNR) and an increase in motion-related artifacts in images [7,13]. Deep learning reconstruction (DLR) techniques have been used to decrease image artifacts and noise, and previous studies have applied DLR to cardiac, musculoskeletal, and neuroimaging, revealing promising results in terms of improved image quality [14,15,16,17,18]. Previous studies on DLR in prostate MRI have mainly focused on its effect on image quality or acquisition time, and comparable or improved image quality with DLR has been observed [19,20,21]. However, to the best of our knowledge, the effect of DLR on the diagnostic performance for the evaluation of EPE in PCa has been scarcely reported [22]. Therefore, we aimed to compare the diagnostic performance of three image datasets—conventional T2WI (T2WIconv) and high-resolution thin-slice T2WI (T2WIHR) with and without DLR—in order to find the optimal image set for the evaluation of EPE in patients with PCa.
2. Materials and Methods
The institutional review board approved this retrospective study, and the requirement for informed consent was waived.
2.1. Patient Selection Criteria
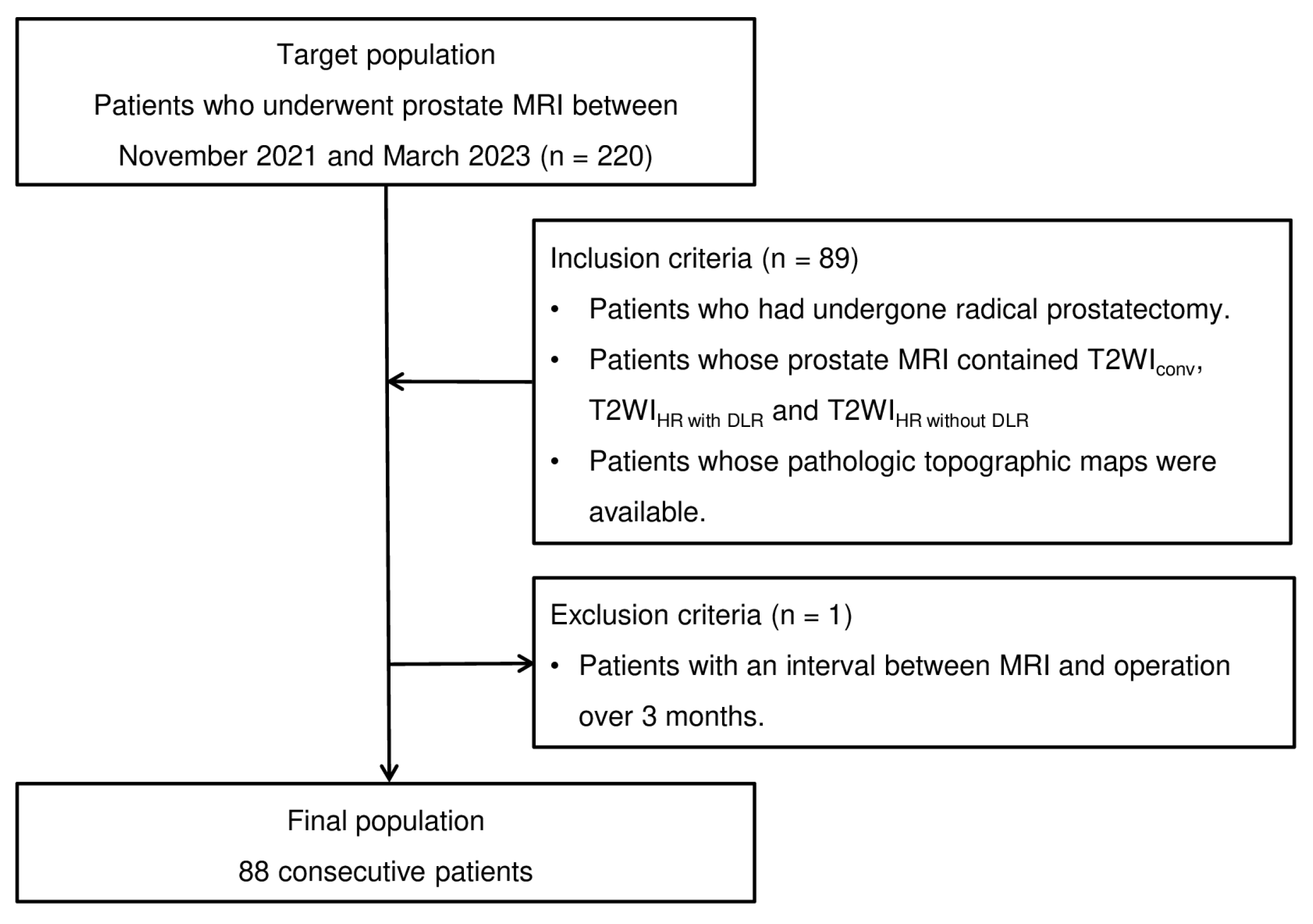
A total of 220 patients who underwent prostate MRI between November 2021 and March 2023 were initially considered eligible for this study. Among them, 88 patients satisfying the following inclusion criteria were finally included in the study. The inclusion criteria were as follows: (1) patients who had undergone radical prostatectomy; (2) patients whose prostate MRI scans contained three image datasets; and (3) patients who had a pathologic topographic map (whole-mount slide) and relevant information such as Gleason scores. The patient enrollment process is summarized in Figure 1.
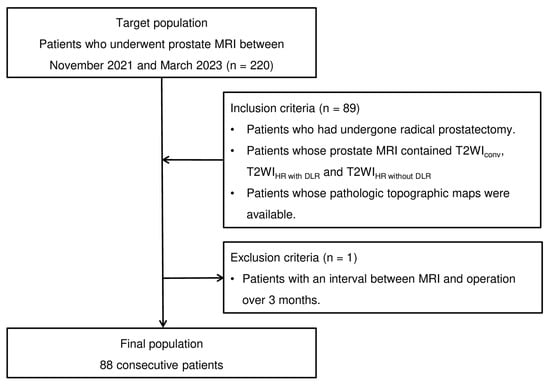
Figure 1.
Flowchart of the case-accrual process.
2.2. Magnetic Resonance Imaging
All MRI examinations were performed using a 3.0-T MR scanner (Signa Architect, GE HealthCare, Chicago, IL, USA) with a body coil (AIRTM Anterior Array, GE HealthCare Coils, Aurora, OH, USA). The scanning protocol consisted of the following sequences: (1) axial, coronal, and sagittal T2WIconv; (2) axial T2WIHR; (3) axial diffusion-weighted imaging (DWI) sequences (b-values of 0 and 1000 s/mm2); and (4) apparent diffusion coefficient (ADC) maps generated from b-values of 0 and 1000 s/mm2. The voxel sizes of T2WIconv and T2WIHR were 0.5 × 0.7 × 3 mm3 and 0.5 × 0.5 × 2 mm3, respectively. The MRI parameters are detailed in Table 1. The DICOM images of all sequences were uploaded and reviewed from a picture archiving and communication system (PACS) workstation (M6; INFINITT Healthcare, Seoul, Republic of Korea).

Table 1.
MRI sequence parameters.
2.3. Deep Learning Reconstruction of T2WIHR
A commercially available DLR algorithm (AIRTM Recon DL, GE HealthCare) was applied to T2WIHR to create T2WIHR with DLR. The DLR algorithm employed in this study incorporates a deep convoluted neural network to produce images that are consistent with the original image data while reducing Gibbs ringing artifacts, sharpness of object edges, and image noise, thus improving the SNR ratio [18]. The level of de-noising achieved by the DLR algorithm can be selected from three presets: low, medium, or high strength. A medium strength was chosen for this study. The medium strength achieves a 50% reduction in image noise, compared with the anticipated image noise, whereas the low strength yields a 30% reduction and the high strength yields a 75% reduction [18].
2.4. Image Analysis
The three image sets (axial T2WIconv, T2WIHR with DLR, and T2WIHR without DLR) were reviewed in three separate sessions with a cross-over review design. The images for review in each session comprised approximately one-third of each image set, and the order of images for review was randomized. The images were independently reviewed by two radiologists (with 4 and 3 years of experience in interpreting prostate MRI, respectively). The three review sessions were separated by a 4-week interval, in order to reduce recall bias. Coronal and sagittal T2WIconv, axial DWI, and corresponding ADC maps (b2000) of each patient were also provided in each review session. Reviewers were blinded to the clinical and pathologic data of the patients, except for the fact that all patients had pathologically proven PCa. Reviewers identified the largest tumor (i.e., the index tumor) in the prostate gland and manually drew the tumor in a schematic diagram of the prostate gland with regard to the level and zonal anatomy. The reviewers then assessed the presence of EPE in the index tumor and assigned a confidence score for EPE based on a 5-point scale describing their confidence in the finding (1 = definitely absent, 2 = probably absent, 3 = equivocal, 4 = probably present, and 5 = definitely present). The window width and level values could be adjusted by each reviewer.
2.5. Image Quality
Contemporaneously to confidence scoring for EPE, the two reviewers also subjectively assessed the image quality of each image dataset. A subjective image quality score was assigned to each image set based on a 5-point Likert scale, where the score represented the number of the visual assessment criteria that the images satisfied. For example, if an image set satisfied only four out of five criteria, a subjective image quality score of 4 would be assigned. The visual assessment criteria were partially based on those described in PI-QUAL [6] and were as follows: (a) prostatic capsule is clearly delineated; (b) seminal vesicles are clearly delineated; (c) neurovascular bundles are clearly delineated; (d) absence of noise; and (e) absence of artifacts such as motion artifacts.
For quantitative analysis of image quality, the SNR and contrast-to-noise ratio (CNR) were assessed for the three image datasets by a third radiologist. The SNR for each image dataset was defined as the mean signal intensity (SI) value of the non-cancerous prostate parenchyma divided by the image noise, while the CNR for each image data set was defined as the absolute SI value of the index tumor (defined as the difference between the mean SI value of the index tumor and the mean SI value of the non-cancerous prostate parenchyma) divided by the image noise. Image noise was defined as the standard deviation of the SI value of the skeletal muscle of the pelvic wall.
2.6. Reference Standard
All patients underwent radical prostatectomy. The resected specimens were evaluated with respect to EPE and the Gleason grading system [23] by a dedicated pathologist. Whole-mount histopathology served as the reference standard for the ground truth of the presence of EPE, as well as tumor location and extent. A senior radiologist with 14 years of experience in interpreting prostate MRI determined whether the pathologic index tumor coincided with the index tumor identified by the two reviewers in each review session.
2.7. Statistical Analysis
The MedCalc software for Windows (MedCalc Software version 19.6.1, Mariakerke, Belgium) was used for the statistical analyses. Statistical significance was set at p < 0.05. The detection rate (i.e., sensitivity) with regard to the index tumor was compared using McNemar’s test. Receiver operating characteristic (ROC) curve analyses were performed for the diagnostic performance of each reviewer for a specific dataset. The area under the ROC curve (AUC) was calculated and compared pairwise to compare diagnostic performances between any two image datasets. For each reviewer, the image quality of each dataset was compared using the Wilcoxon signed-rank test. For the assessment of quantitative image quality, SNR and CNR were compared through repeated measures ANOVA.
3. Results
3.1. Patient Demographics
The study population comprised 28 patients with EPE and 60 patients without EPE. The mean interval from pre-operative prostate MRI to radical prostatectomy was 33.5 days (range: 1–88 days), and the mean prostate-specific antigen (PSA) level was 20.37 ng/dL (range: 0.85–154 ng/dL). The number of patients with each Gleason score (GS) was as follows: GS6 (n = 25), GS7 (3 + 4, n = 37; 4 + 3, n = 18), GS8 (n = 3), and GS9 (n = 5). The number of patients with each pathologic T-stage was as follows: T2 (n = 60), T3a (n = 13), and T3b (n = 15). The specific demographic data are presented in Table 2.
Table 2.
Demographic data of the study population.
3.2. Comparison of Detection Rates for the Index Tumor
For reviewer 1, the detection rate of the index tumor was 85% for all three image datasets. For reviewer 2, the detection rate of the index tumor on T2WIconv, T2WIHR with DLR, and T2WIHR without DLR was 87%, 86%, and 86%, respectively. The detection rates did not present significant differences among the three image datasets for both reviewers (p > 0.05).
3.3. Comparison of Diagnostic Performance for EPE
For reviewer 1, T2WIconv (AUC, 0.883; 95% confidence interval (CI), 0.784–0.947) showed a significantly better diagnostic performance compared to T2WIHR with DLR (AUC, 0.806; 95% CI, 0.694–0.891; p = 0.0057) and T2WIHR without DLR (AUC, 0.772; 95% CI, 0.656–0.864; p = 0.0006). For reviewer 2, T2WIconv (AUC, 0.803; 95% CI, 0.691–0.888) also showed a significantly greater AUC compared to T2WIHR with DLR (AUC, 0.762; 95% CI, 0.646–0.855; p = 0.0220) and T2WIHR without DLR (AUC, 0.745; 95% CI, 0.627–0.841; p = 0.0277). For both reviewers, the diagnostic performance between T2WIHR with DLR and T2WIHR without DLR did not present a significant difference (for reviewer 1, p = 0.1610; for reviewer 2, p = 0.3175). Representative images are presented in Figure 2, and the diagnostic performance is summarized in Table 3.
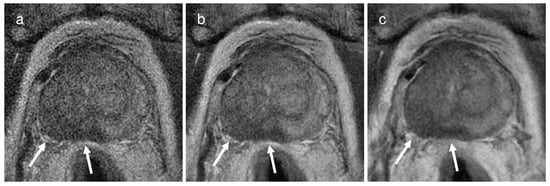
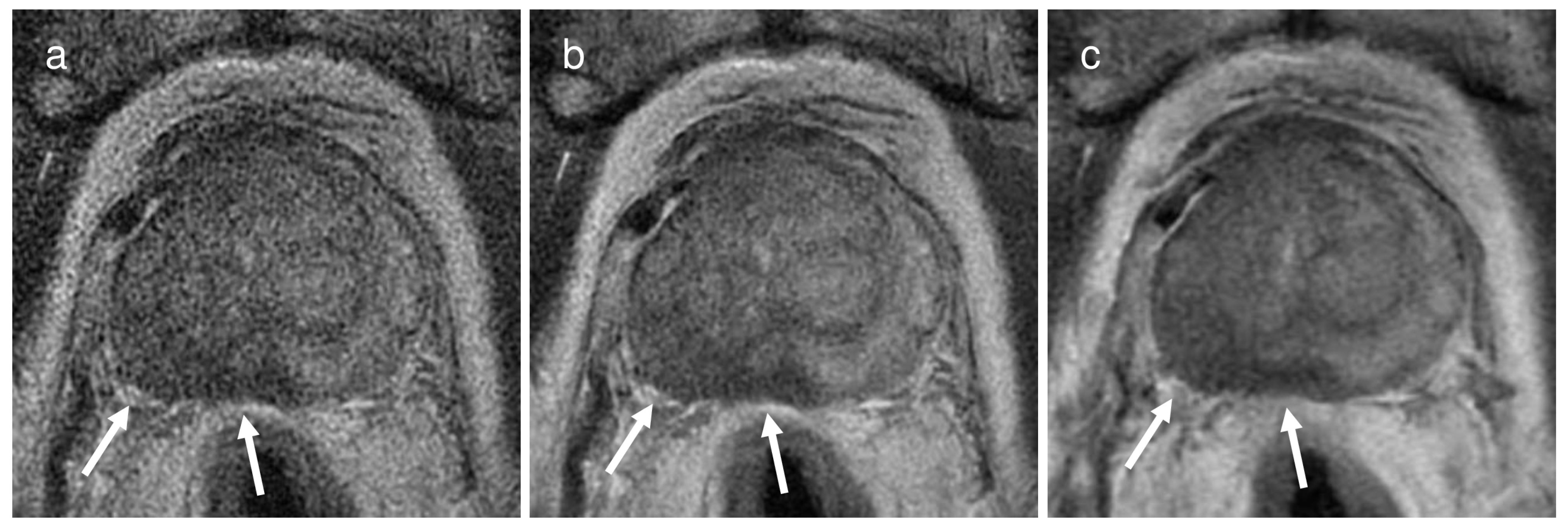
Figure 2.
A representative case of a 74-year-old man with a Gleason score of 9 in the right middle peripheral zone demonstrating extra-prostatic extension through the right posterolateral capsule (arrows) on (a) a 2 mm thin-slice T2WI without deep learning reconstruction (DLR), (b) the same 2 mm T2WI with DLR, and (c) conventional T2WI with 3 mm slice thickness. For both reviewers, the confidence score for presence of extra-prostatic extension increased from 4 (probably present) on the 2 mm thin-slice T2WI with or without DLR to 5 (definitely present) on conventional T2WI.
Table 3.
Comparison of diagnostic performance and predictive values of T2WIconv, T2WIHR with DLR, and T2WIHR without DLR.
3.4. Comparison of Image Quality
3.4.1. Qualitative Analysis
For reviewer 1, the subjective image quality score of T2WIconv (median, 5; interquartile range, 5–5) was greater than T2WIHR with DLR (median, 4; interquartile range, 3–5; p < 0.0001) and T2WIHR without DLR (median, 3; interquartile range, 3–4; p < 0.0001). For reviewer 2, the subjective image quality score of T2WIconv (median, 5; interquartile range, 4–5) was also greater than T2WIHR with DLR (median, 4; interquartile range, 3–4; p < 0.0001) and T2WIHR without DLR (median, 3; interquartile range, 3–4; p < 0.0001). For both reviewers, T2WIHR with DLR had a significantly higher subjective image quality score compared to T2WIHR without DLR (p < 0.0001). Representative images are presented in Figure 3.
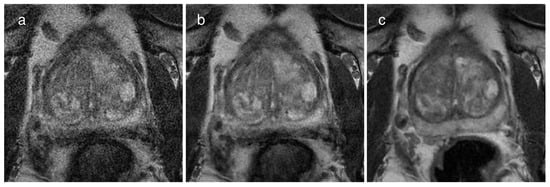
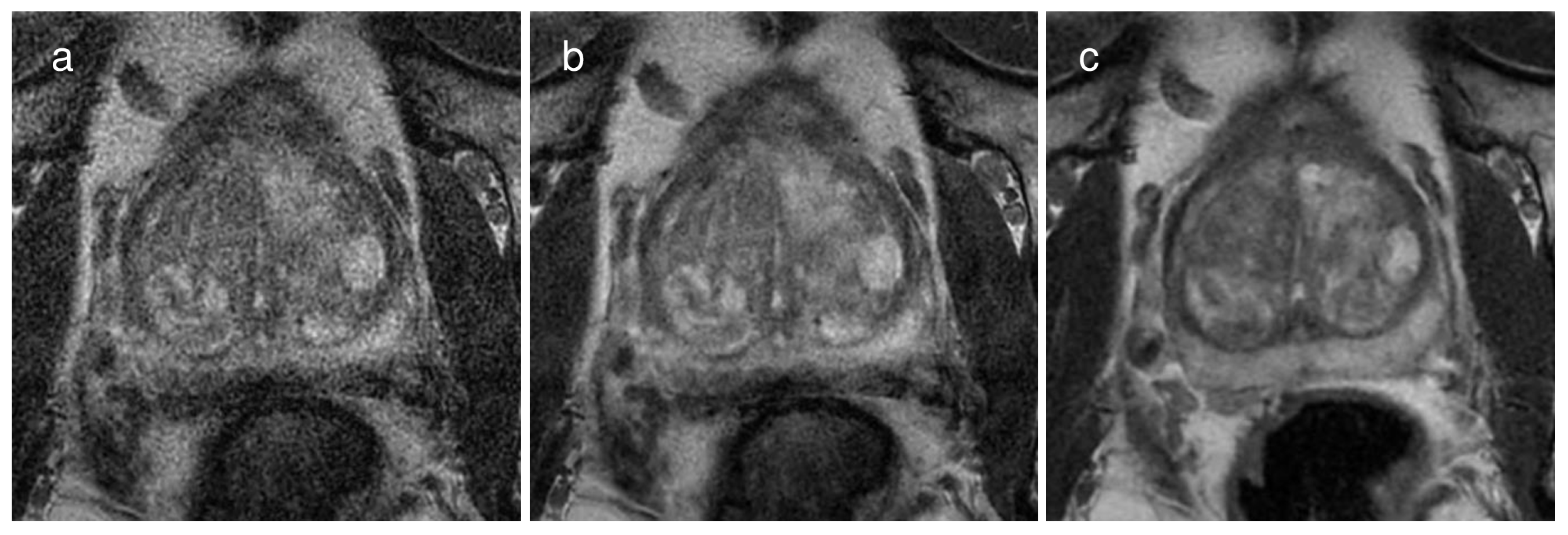
Figure 3.
A representative case of a 67-year-old man with a Gleason score of 6 demonstrating the image quality of each image dataset on (a) a 2 mm thin-slice T2WI without deep learning reconstruction (DLR), (b) the same T2WI with DLR, and (c) conventional T2WI with 3 mm slice thickness. The subjective image quality score was the best on conventional T2WI, followed by the thin-slice T2WI with DLR and the same T2WI without DLR. Specifically, the scores were 5, 4, and 3, respectively, for reviewer 1 and 4, 3, and 2, respectively, for reviewer 2.
3.4.2. Quantitative Analysis
The SNR of T2WIconv (mean ± SD, 22.17 ± 7.02) was the highest, followed by T2WIHR with DLR (15.81 ± 4.80) and T2WIHR without DLR (8.71 ± 2.24) (p < 0.001). Similarly, the CNR of T2WIconv (6.05 ± 4.16) was the highest, followed by T2WIHR with DLR (4.41 ± 3.16) and T2WIHR without DLR (2.33 ± 1.57) (p < 0.001). The measurement results are summarized in Table 4.
Table 4.
Quantitative image quality analysis of T2WIconv, T2WIHR with DLR, and T2WIHR without DLR.
4. Discussion
The results of our study revealed that the diagnostic performance for EPE in PCa was greater in T2WIconv compared to T2WIHR, while DLR did not significantly improve the diagnostic performance in T2WIHR. In terms of image quality, T2WIconv demonstrated a higher image quality than T2WIHR both subjectively and quantitatively, while DLR significantly improved the image quality of T2WIHR.
As PI-RADS v.2.1 recommends the T2WI as the key sequence for the detection of TZ cancer [1] and DWI for peripheral zone (PZ) cancer, we believe that the benefits of DLR in T2WIHR could be expected in cases of TZ cancer. Our observation that DLR did not enhance the diagnostic performance in evaluating EPE can be explained by several factors. First, the proportion of EPE in TZ cancer should be considered. The proportion was approximately 20% (6/28), whereas that of PZ cancer was 32% (17/53). Second, the detection of TZ cancer using T2WI alone is very challenging; thus, supplementary reading of DWI might affect the diagnostic decision on EPE. The better performance of T2WIconv could be attributable to the better SNR and CNR compared to T2WIHR combined (i.e., whether DLR or not). Out of the 28 patients with EPE in this study, 17 patients had PZ cancer (60%) and the EPE was predominant when the PZ cancer invaded the posterolateral capsule. Therefore, this posterolateral area was the main site for the radiologists to confidently evaluate EPE using the three image datasets. Consequently, in our opinion, T2WIconv benefited from the better conspicuity in anatomical structures resulting from the improved SNR and CNR of T2WIconv, compared to the other image datasets. Our observations support the PI-QUAL requirement for image acquisition parameters. A 2 mm ST, even with the aid of DLR, did not outperform the conventional 3 mm on T2WI, which is the PI-QUAL guideline requirement for image acquisition.
To the best of our knowledge, the effect of DLR on the detection of EPE has not been previously reported with regard to enhanced spatial resolution. Beyond the spatial resolution, Park et al. [22] compared conventional T2WI (ST, 3 mm) and T2WI with a shorter acquisition time (i.e., fast T2WI) with and without DLR in terms of diagnostic performance for the diagnosis of EPE in terms of enhanced temporal resolution. They achieved an enhanced temporal resolution from 4 min to 2 min 30 s by adopting a reduced repetition time (from 4000 to 2800 ms) and number of excitations (from 1.5 to 1.0), and they employed the same commercially available DLR algorithm (AIRTM Recon DL). Their results revealed that T2WIconv showed a comparable diagnostic performance to fast T2WI with DLR for all three reviewers and a mixed response to applying DLR to fast T2WI. Specifically, an improved performance was observed for two reviewers (AUCs, for reviewer 1, T2WIconv, fast T2WI with DLR, fast T2WI without DLR in order, 0.85, 0.86, 0.75; for reviewer 2, 0.82, 0.82, 0.73, respectively), whereas stationary performance was revealed in one reviewer (AUCs, 0.79, 0.81, 0.74, respectively). Our results partially correspond with the above study, in that T2WIconv presented the best performance and DLR did not improve the diagnostic performance for diagnosis of EPE.
The effect of DLR on the image quality of prostate MRI has been more frequently studied. Wang et al. [19] compared four image datasets—T2WI (ST, 3 mm) with the endo-rectal coil signal turned on and off, both with and without DLR—in terms of image quality and visualization of various anatomic structures and the tumor. They also employed the same commercial DLR software (AIRTM Recon DL). The image quality of T2WI with DLR when the endo-rectal coil signal was turned off was significantly higher than the other three image sets (p < 0.01). This sequence was also most frequently chosen as the best one for the visualization of major anatomical landmarks and the tumor. Park et al. [22] also reported a significant improvement in the SNR (fast T2WI with DLR vs. fast T2WI without DLR, 14.7 vs. 8.8, p < 0.001), CNR (6.5 vs. 3.4, p < 0.001), and lesion delineation quality by subjective assessment and subjective image quality scores (from 1 = non-diagnostic to 5 = excellent; all readers, 4.0 vs. 3.0; all p < 0.001) when DLR was applied to fast MRI. Our study corresponds well with the above studies, in that the subjective image quality as well as quantitative SNR and CNR could be improved with DLR [19,22].
Beyond the two-dimensional (2D) acquisition of T2WI, the benefits of 3D-T2WI in prostate MRI include reduced acquisition time and post-processing in multiple planes. However, the effect on the diagnostic performance for evaluating EPE is a subject with more conflicting data [13]. Choi et al. [10] reported no significant difference between conventional T2WI (ST, 3 mm) and 3D-T2WI (0.6 mm) in terms of the sensitivity (for reader 1, 28% vs. 48%, p = 0.375; for reader 2, 64% vs. 60%, p = 1.000) and specificity (for reader 1, all 91%; for reader 2, all 76%) for detecting EPE. Caglic et al. [24] found that 3D-T2WI (1 mm) had a similar diagnostic performance to conventional 2D-T2WI (3 mm) (AUC, 0.877 vs. 0.835, p = 0.17; sensitivity, 75% vs. 65%, p = 0.058; and specificity, 84% vs. 86%, p = 0.705) in the detection of EPE. Rosenkrantz et al. [11] also compared 3D- (ST, 1 mm) and 2D-T2WI (ST, 3 mm) for the diagnosis of EPE and reported a similar accuracy (3D T2WI vs. 2D T2WI, 68% vs. 74%, p = 0.6250). At present, PI-RADS v.2.1 recommends an ST of 3 mm and, while 3D axial acquisitions may be used as a supplementary sequence, the altered tissue contrast should be treated with caution, and the possibility that in-plane resolution may be lower in 3D acquisitions also should be considered [1,3]. As the added value of 3D-T2WI in the diagnosis of EPE is a subject of debate, we believe that the current guidelines are sufficient for the diagnosis of EPE, and the acquisition of 3D-T2WI could be conducted in prudence when more robust evidence suggests it concordantly.
Emphasizing the pros and cons of DLR is worthy of notice because DLR has been increasingly applied to radiological imaging with the benefits of reducing acquisition times while preserving image quality, as well as improving image quality while maintaining acquisition times. In regard to shortening acquisition time, DLR has been applied to fast-spin echo imaging in prostate MRI, and in particular, a reduction in acquisition time of up to 65% has been shown in T2-weighted fast-spin echo imaging [25]. DLR has also been implemented for the purpose of improving image quality [19,22,26]. Although the application of DLR itself may be harmless to patients, potential cons may include the additional cost of DLR software and the observations that the improved image quality may not always lead to improved diagnostic performance for specific diagnostic tasks like ours. In our opinion, although diagnostic performance based on radiologists’ perceptions of minute anatomical structures or lesions may benefit from the improved image quality after the application of DLR to images with noise [27], diagnostic tasks based on the integration of various image findings may not enhance radiologists’ diagnostic performance in spite of improved image quality after applying DLR [22,28,29,30].
There were several limitations to our study. First, only patients who had undergone radical prostatectomy were included in our study. As advanced, recurrent, or metastatic PCa may undergo systemic therapy, rather than surgical therapy [31], a selection bias against more advanced cases might have been introduced; therefore, it is possible that advanced metastatic cases with EPE were excluded. However, such a criterion was necessary in order to obtain topographic maps with whole-mount pathology, thus providing a ground truth for the MRI findings to be compared with. Second, acquisition parameters other than the ST were slightly different for T2WIHR; thus, the in-plane resolution differed slightly due to different field-of-view and matrix sizes. Further studies are needed to elucidate the isolated effect of thinner STs in the evaluation of EPE. Third, DWI and ADC maps were provided to the reviewers. As DWI and ADC maps are crucial sequences for the detection of PCa, especially for PZ cancers [1,3], the detection rate may not represent the isolated effect of T2WI sequences. However, DWI and ADC sequences are a mainstay in multi-parametric MRI, with a well-established role in the diagnosis of PCa. Therefore, our study adopted daily clinical practice, in that T2WI was reviewed alongside DWI and ADC maps.
5. Conclusions
In conclusion, T2WIconv with a 3 mm ST was optimal with respect to diagnostic performance as well as image quality for the evaluation of EPE in patients with PCa. Thin-slice T2WI with a 2 mm ST did not outperform T2WIconv, even with the aid of DLR. Our results support the minimal technical requirements described in the PI-QUAL guidelines, which recommend an ST of 3 mm in the acquisition of axial T2WI.
Author Contributions
Conceptualization, S.H.K.; Methodology, S.H.K.; Software, S.H.K.; Validation, all authors; Formal analysis, all authors; Investigation, all authors; Resources, S.H.K.; Data curation, S.H.K.; Writing—original draft preparation, S.H.K. and M.K.; Writing—review and editing, all authors; Visualization, S.H.K. and M.K.; Supervision, S.H.K.; Project administration, S.H.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (no. 2023-12-005, date of approval 12 December 2023).
Informed Consent Statement
Patient consent was waived due to the extremely low risk to patients associated with this retrospective study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to patients’ privacy.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef]
- Esses, S.J.; Taneja, S.S.; Rosenkrantz, A.B. Imaging Facilities’ Adherence to PI-RADS v2 Minimum Technical Standards for the Performance of Prostate MRI. Acad. Radiol. 2018, 25, 188–195. [Google Scholar] [CrossRef]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging—Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef]
- Caglic, I.; Barrett, T. Optimising prostate mpMRI: Prepare for success. Clin. Radiol. 2019, 74, 831–840. [Google Scholar] [CrossRef]
- Jambor, I. Optimization of prostate MRI acquisition and post-processing protocol: A pictorial review with access to acquisition protocols. Acta Radiol. Open 2017, 6, 2058460117745574. [Google Scholar] [CrossRef]
- Giganti, F.; Kirkham, A.; Kasivisvanathan, V.; Papoutsaki, M.V.; Punwani, S.; Emberton, M.; Moore, C.M.; Allen, C. Understanding PI-QUAL for prostate MRI quality: A practical primer for radiologists. Insights Imaging 2021, 12, 59. [Google Scholar] [CrossRef]
- Gupta, R.T.; Spilseth, B.; Patel, N.; Brown, A.F.; Yu, J. Multiparametric prostate MRI: Focus on T2-weighted imaging and role in staging of prostate cancer. Abdom. Radiol. 2016, 41, 831–843. [Google Scholar] [CrossRef]
- Magi-Galluzzi, C.; Evans, A.J.; Delahunt, B.; Epstein, J.I.; Griffiths, D.F.; van der Kwast, T.H.; Montironi, R.; Wheeler, T.M.; Srigley, J.R.; Egevad, L.L.; et al. International Society of Urological Pathology (ISUP) Consensus Conference on Handling and Staging of Radical Prostatectomy Specimens. Working group 3: Extraprostatic extension, lymphovascular invasion and locally advanced disease. Mod. Pathol. 2011, 24, 26–38. [Google Scholar] [CrossRef]
- McClure, T.D.; Margolis, D.J.; Reiter, R.E.; Sayre, J.W.; Thomas, M.A.; Nagarajan, R.; Gulati, M.; Raman, S.S. Use of MR imaging to determine preservation of the neurovascular bundles at robotic-assisted laparoscopic prostatectomy. Radiology 2012, 262, 874–883. [Google Scholar] [CrossRef]
- Choi, M.H.; Lee, Y.J.; Jung, S.E.; Han, D. High-resolution 3D T2-weighted SPACE sequence with compressed sensing for the prostate gland: Diagnostic performance in comparison with conventional T2-weighted images. Abdom. Radiol. 2023, 48, 1090–1099. [Google Scholar] [CrossRef]
- Rosenkrantz, A.B.; Neil, J.; Kong, X.; Melamed, J.; Babb, J.S.; Taneja, S.S.; Taouli, B. Prostate cancer: Comparison of 3D T2-weighted with conventional 2D T2-weighted imaging for image quality and tumor detection. AJR Am. J. Roentgenol. 2010, 194, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Polanec, S.H.; Lazar, M.; Wengert, G.J.; Bickel, H.; Spick, C.; Susani, M.; Shariat, S.; Clauser, P.; Baltzer, P.A.T. 3D T2-weighted imaging to shorten multiparametric prostate MRI protocols. Eur. Radiol. 2018, 28, 1634–1641. [Google Scholar] [CrossRef]
- Lim, K.K.; Noe, G.; Hornsey, E.; Lim, R.P. Clinical applications of 3D T2-weighted MRI in pelvic imaging. Abdom. Imaging 2014, 39, 1052–1062. [Google Scholar] [CrossRef] [PubMed]
- van der Velde, N.; Hassing, H.C.; Bakker, B.J.; Wielopolski, P.A.; Lebel, R.M.; Janich, M.A.; Kardys, I.; Budde, R.P.J.; Hirsch, A. Improvement of late gadolinium enhancement image quality using a deep learning-based reconstruction algorithm and its influence on myocardial scar quantification. Eur. Radiol. 2021, 31, 3846–3855. [Google Scholar] [CrossRef] [PubMed]
- Hahn, S.; Yi, J.; Lee, H.J.; Lee, Y.; Lim, Y.J.; Bang, J.Y.; Kim, H.; Lee, J. Image Quality and Diagnostic Performance of Accelerated Shoulder MRI With Deep Learning-Based Reconstruction. AJR Am. J. Roentgenol. 2022, 218, 506–516. [Google Scholar] [CrossRef]
- Lee, D.H.; Park, J.E.; Nam, Y.K.; Lee, J.; Kim, S.; Kim, Y.H.; Kim, H.S. Deep learning-based thin-section MRI reconstruction improves tumour detection and delineation in pre- and post-treatment pituitary adenoma. Sci. Rep. 2021, 11, 21302. [Google Scholar] [CrossRef]
- Sun, S.; Tan, E.T.; Mintz, D.N.; Sahr, M.; Endo, Y.; Nguyen, J.; Lebel, R.M.; Carrino, J.A.; Sneag, D.B. Evaluation of deep learning reconstructed high-resolution 3D lumbar spine MRI. Eur. Radiol. 2022, 32, 6167–6177. [Google Scholar] [CrossRef]
- Lebel, R.M. Performance characterization of a novel deep learning-based MR image reconstruction pipeline. arXiv 2020, arXiv:2008.06559. [Google Scholar]
- Wang, X.; Ma, J.; Bhosale, P.; Ibarra Rovira, J.J.; Qayyum, A.; Sun, J.; Bayram, E.; Szklaruk, J. Novel deep learning-based noise reduction technique for prostate magnetic resonance imaging. Abdom. Radiol. 2021, 46, 3378–3386. [Google Scholar] [CrossRef]
- Kim, E.H.; Choi, M.H.; Lee, Y.J.; Han, D.; Mostapha, M.; Nickel, D. Deep learning-accelerated T2-weighted imaging of the prostate: Impact of further acceleration with lower spatial resolution on image quality. Eur. J. Radiol. 2021, 145, 110012. [Google Scholar] [CrossRef]
- Gassenmaier, S.; Warm, V.; Nickel, D.; Weiland, E.; Herrmann, J.; Almansour, H.; Wessling, D.; Afat, S. Thin-Slice Prostate MRI Enabled by Deep Learning Image Reconstruction. Cancers 2023, 15, 578. [Google Scholar] [CrossRef] [PubMed]
- Park, J.C.; Park, K.J.; Park, M.Y.; Kim, M.H.; Kim, J.K. Fast T2-Weighted Imaging With Deep Learning-Based Reconstruction: Evaluation of Image Quality and Diagnostic Performance in Patients Undergoing Radical Prostatectomy. J. Magn. Reson. Imaging 2022, 55, 1735–1744. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Caglic, I.; Povalej Brzan, P.; Warren, A.Y.; Bratt, O.; Shah, N.; Barrett, T. Defining the incremental value of 3D T2-weighted imaging in the assessment of prostate cancer extracapsular extension. Eur. Radiol. 2019, 29, 5488–5497. [Google Scholar] [CrossRef]
- Gassenmaier, S.; Afat, S.; Nickel, D.; Mostapha, M.; Herrmann, J.; Othman, A.E. Deep learning-accelerated T2-weighted imaging of the prostate: Reduction of acquisition time and improvement of image quality. Eur. J. Radiol. 2021, 137, 109600. [Google Scholar] [CrossRef] [PubMed]
- Gassenmaier, S.; Küstner, T.; Nickel, D.; Herrmann, J.; Hoffmann, R.; Almansour, H.; Afat, S.; Nikolaou, K.; Othman, A.E. Deep Learning Applications in Magnetic Resonance Imaging: Has the Future Become Present? Diagnostics 2021, 11, 2181. [Google Scholar] [CrossRef]
- Kaniewska, M.; Deininger-Czermak, E.; Lohezic, M.; Ensle, F.; Guggenberger, R. Deep Learning Convolutional Neural Network Reconstruction and Radial k-Space Acquisition MR Technique for Enhanced Detection of Retropatellar Cartilage Lesions of the Knee Joint. Diagnostics 2023, 13, 2438. [Google Scholar] [CrossRef]
- Johnson, P.M.; Lin, D.J.; Zbontar, J.; Zitnick, C.L.; Sriram, A.; Muckley, M.; Babb, J.S.; Kline, M.; Ciavarra, G.; Alaia, E.; et al. Deep Learning Reconstruction Enables Prospectively Accelerated Clinical Knee MRI. Radiology 2023, 307, e220425. [Google Scholar] [CrossRef]
- Hahn, S.; Yi, J.; Lee, H.J.; Lee, Y.; Lee, J.; Wang, X.; Fung, M. Comparison of deep learning-based reconstruction of PROPELLER Shoulder MRI with conventional reconstruction. Skelet. Radiol. 2023, 52, 1545–1555. [Google Scholar] [CrossRef]
- Feuerriegel, G.C.; Weiss, K.; Kronthaler, S.; Leonhardt, Y.; Neumann, J.; Wurm, M.; Lenhart, N.S.; Makowski, M.R.; Schwaiger, B.J.; Woertler, K.; et al. Evaluation of a deep learning-based reconstruction method for denoising and image enhancement of shoulder MRI in patients with shoulder pain. Eur. Radiol. 2023, 33, 4875–4884. [Google Scholar] [CrossRef]
- Virgo, K.S.; Rumble, R.B.; de Wit, R.; Mendelson, D.S.; Smith, T.J.; Taplin, M.E.; Wade, J.L., 3rd; Bennett, C.L.; Scher, H.I.; Nguyen, P.L.; et al. Initial Management of Noncastrate Advanced, Recurrent, or Metastatic Prostate Cancer: ASCO Guideline Update. J. Clin. Oncol. 2021, 39, 1274–1305. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).