
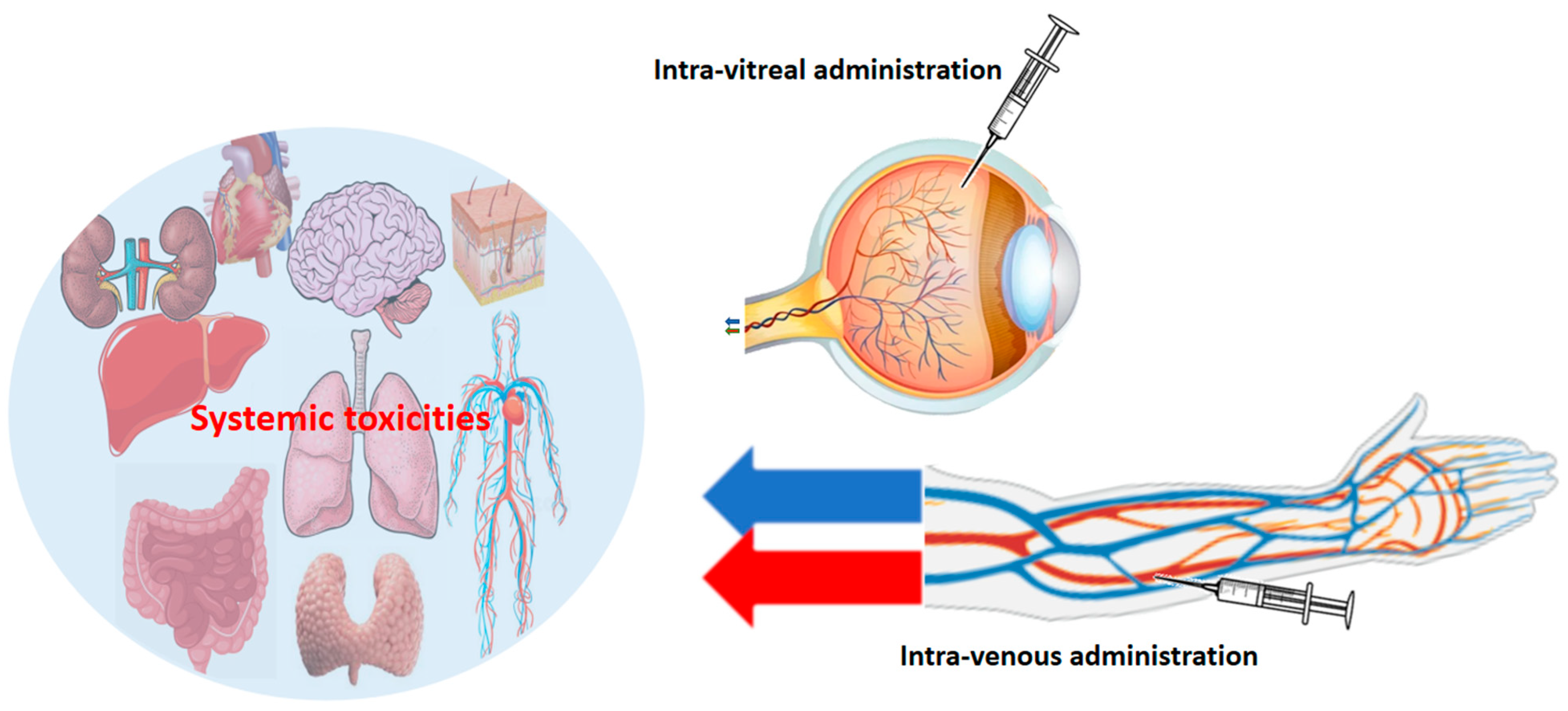
Exploring the Spectrum of VEGF Inhibitors’ Toxicities from Systemic to Intra-Vitreal Usage in Medical Practice

 ,
,  ,
,  , ,
, ,  ,
,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Pharmacokinetics and Pharmacodynamic Aspects of VEGFi
2.1. VEGFi Belonging to the Antibodies/Chimeric Proteins Category
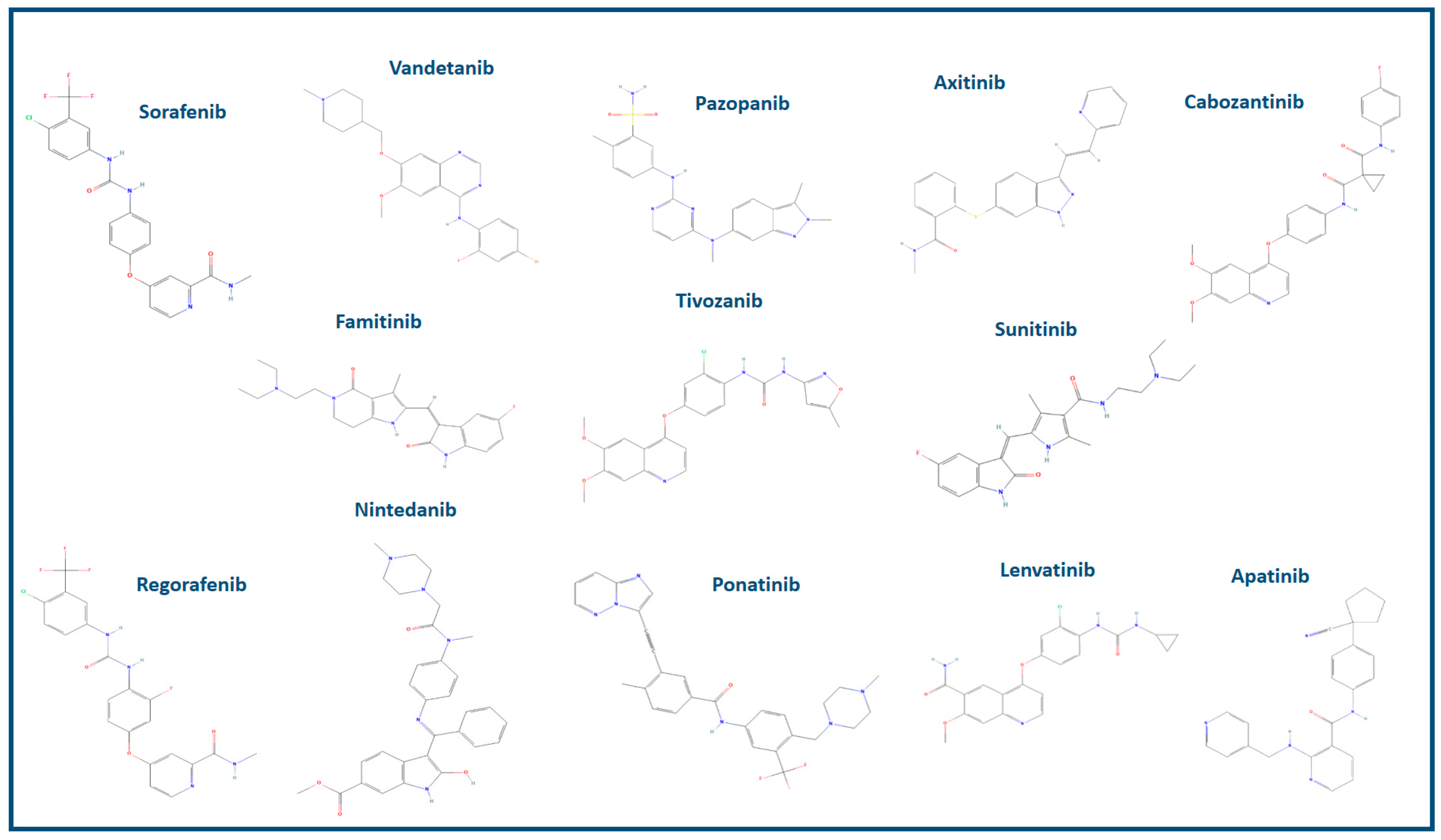
2.2. VEGFi Belonging to the Small Molecules Category
3. Etiology and Epidemiology of VEGFi Toxicity
- Physiological survival and proliferation of endothelial cells make existing blood vessels more fragile and susceptible to damage [64].
- Permeability is controlled by the endothelial cells of glomerular capillaries in the kidneys [67].
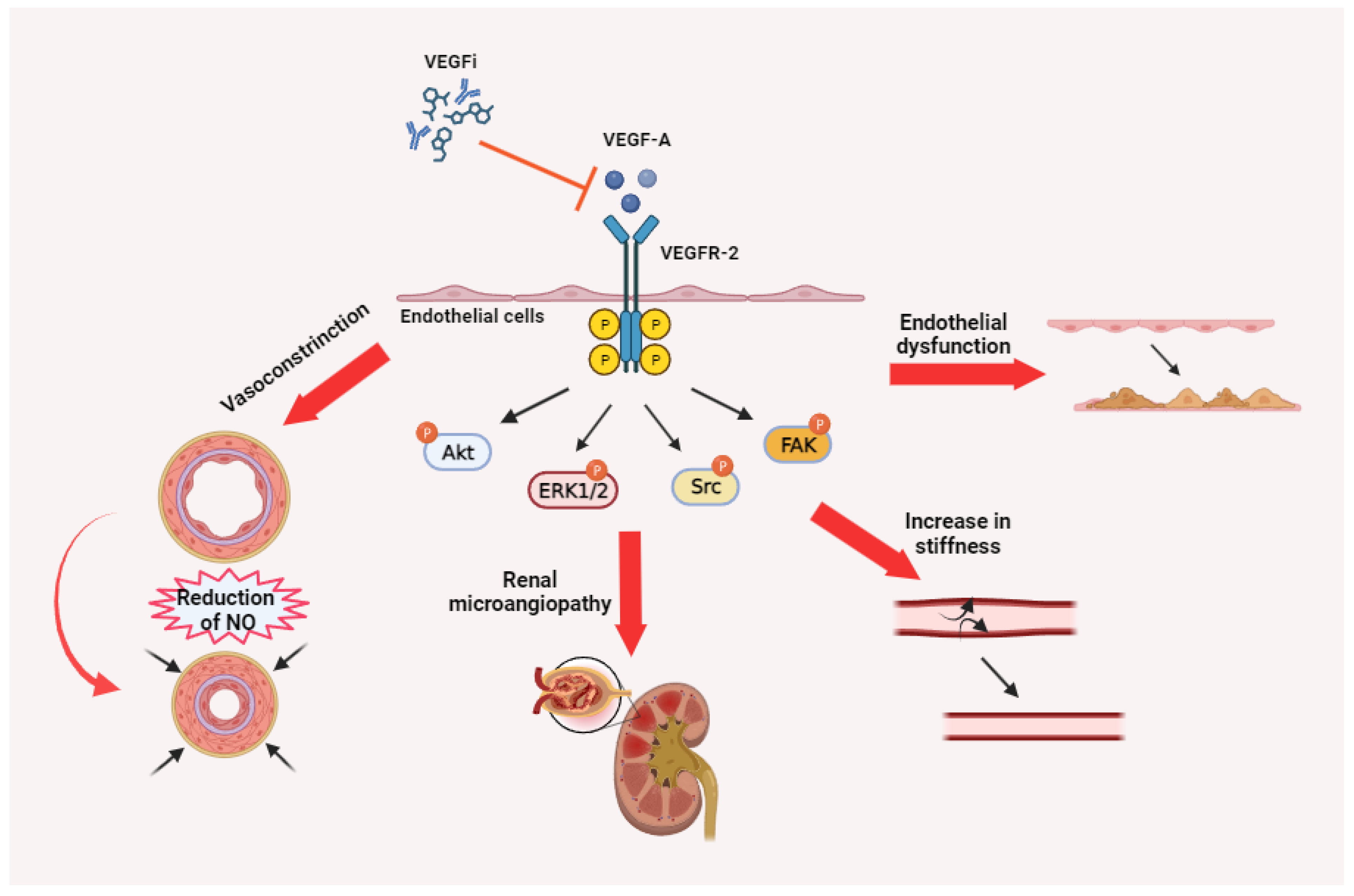
4. Pathophysiology of VEGFi Toxicity
5. Clinical Identification of VEGFi Toxicity
6. Assessment of Toxicities Induced by VEGFi: Pragmatic Approaches for Intervention
7. Management of VEGFi Toxicities
- A decrease in best-corrected visual acuity (BCVA) by ≥30 letters compared to the last visual acuity assessment.
- Intraocular pressure (IOP) attaining or surpassing 30 mm Hg.
- Presence of a retinal tear.
- Incidence of rhegmatogenous retinal detachment.
- Detection of macular holes.
- Extension of retinal hemorrhage to the central fovea, or if the extent of hemorrhage is ≥50% of the total lesion area.
- Performance or planned intraocular surgery within the preceding or subsequent 28 days.
8. Reducing VEGFi-Associated Toxicities through Patient Education and Preventive Interventions
9. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thapa, K.; Khan, H.; Kaur, G.; Kumar, P.; Singh, T.G. Therapeutic targeting of angiopoietins in tumor angiogenesis and cancer development. Biochem. Biophys. Res. Commun. 2023, 687, 149130. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.A.; Nilsson, M.B.; Le, X.; Cascone, T.; Jain, R.K.; Heymach, J.V. Molecular Mechanisms and Future Implications of VEGF/VEGFR in Cancer Therapy. Clin. Cancer Res. 2023, 29, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Apte, R.S.; Chen, D.S.; Ferrara, N. VEGF in Signaling and Disease: Beyond Discovery and Development. Cell 2019, 176, 1248–1264. [Google Scholar] [CrossRef]
- Brouillet, S.; Hoffmann, P.; Feige, J.-J.; Alfaidy, N. EG-VEGF: A key endocrine factor in placental development. Trends Endocrinol. Metab. 2012, 23, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Trifanescu, O.G.; Gales, L.N.; Tanase, B.C.; Marinescu, S.A.; Trifanescu, R.A.; Gruia, I.M.; Paun, M.A.; Rebegea, L.; Mitrica, R.; Serbanescu, L.; et al. Prognostic Role of Vascular Endothelial Growth Factor and Correlation with Oxidative Stress Markers in Locally Advanced and Metastatic Ovarian Cancer Patients. Diagnostics 2023, 13, 166. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Gutiérrez, L.; Ferrara, N. Biology and therapeutic targeting of vascular endothelial growth factor A. Nat. Rev. Mol. Cell Biol. 2023, 24, 816–834. [Google Scholar] [CrossRef]
- Roskoski, R., Jr. VEGF receptor protein–tyrosine kinases: Structure and regulation. Biochem. Biophys. Res. Commun. 2008, 375, 287–291. [Google Scholar] [CrossRef]
- Mabeta, P.; Steenkamp, V. The VEGF/VEGFR Axis Revisited: Implications for Cancer Therapy. Int. J. Mol. Sci. 2022, 23, 15585. [Google Scholar] [CrossRef]
- Rosen, L.S.; Jacobs, I.A.; Burkes, R.L. Bevacizumab in Colorectal Cancer: Current Role in Treatment and the Potential of Biosimilars. Target. Oncol. 2017, 12, 599–610. [Google Scholar] [CrossRef]
- Mukherji, S.K. Bevacizumab (Avastin). Am. J. Neuroradiol. 2010, 31, 235–236. [Google Scholar] [CrossRef]
- Garcia, J.; Hurwitz, H.I.; Sandler, A.B.; Miles, D.; Coleman, R.L.; Deurloo, R.; Chinot, O.L. Bevacizumab (Avastin®) in cancer treatment: A review of 15 years of clinical experience and future outlook. Cancer Treat. Rev. 2020, 86, 102017. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Turner, D.C.; Li, F.; Chen, X.; Liao, M.Z.; Li, C. Pharmacokinetics of biologics in gastric cancer. Clin. Transl. Sci. 2023, 16, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Owen, J.S.; Rackley, R.J.; Hummel, M.A.; Roepcke, S.; Huang, H.; Liu, M.; Idris, T.A.; Murugesan, S.M.N.; Marwah, A.; Loganathan, S.; et al. Population Pharmacokinetics of MYL-1402O, a Proposed Biosimilar to Bevacizumab and Reference Product (Avastin®) in Patients with Non-squamous Non-small Cell Lung Cancer. Eur. J. Drug Metab. Pharmacokinet. 2023, 48, 675–689. [Google Scholar] [CrossRef] [PubMed]
- Estarreja, J.; Mendes, P.; Silva, C.; Camacho, P.; Mateus, V. The Efficacy, Safety, and Efficiency of the Off-Label Use of Bevacizumab in Patients Diagnosed with Age-Related Macular Degeneration: Protocol for a Systematic Review and Meta-Analysis. JMIR Res. Protoc. 2023, 12, e38658. [Google Scholar] [CrossRef] [PubMed]
- Dupuis-Girod, S.; Rivière, S.; Lavigne, C.; Fargeton, A.; Gilbert-Dussardier, B.; Grobost, V.; Leguy-Seguin, V.; Maillard, H.; Mohamed, S.; Decullier, E.; et al. Efficacy and safety of intravenous bevacizumab on severe bleeding associated with hemorrhagic hereditary telangiectasia: A national, randomized multicenter trial. J. Intern. Med. 2023, 294, 761–774. [Google Scholar] [CrossRef] [PubMed]
- Stewart, M.W. Off-Label Drug Use: The Bevacizumab Story. Mayo Clin. Proc. 2013, 88, 305. [Google Scholar] [CrossRef]
- Poole, R.M.; Vaidya, A. Ramucirumab: First Global Approval. Drugs 2014, 74, 1047–1058. [Google Scholar] [CrossRef]
- Greig, S.L.; Keating, G.M. Ramucirumab: A Review in Advanced Gastric Cancer: Clinical immunotherapeutics, biopharmaceuticals and gene therapy. BioDrugs 2015, 29, 341–351. [Google Scholar] [CrossRef]
- Garon, E.B.; Visseren-Grul, C.; Rizzo, M.T.; Puri, T.; Chenji, S.; Reck, M. Clinical outcomes of ramucirumab plus docetaxel in the treatment of patients with non-small cell lung cancer after immunotherapy: A systematic literature review. Front. Oncol. 2023, 13, 1247879. [Google Scholar] [CrossRef]
- Gordan, J.D.; Kennedy, E.B.; Abou-Alfa, G.K.; Beg, M.S.; Brower, S.T.; Gade, T.P.; Goff, L.; Gupta, S.; Guy, J.; Harris, W.P.; et al. Systemic Therapy for Advanced Hepatocellular Carcinoma: ASCO Guideline. J. Clin. Oncol. 2020, 38, 4317–4345. [Google Scholar] [CrossRef]
- Gambardella, V.; Tarazona, N.; Cejalvo, J.M.; Roselló, S.; Cervantes, A. Clinical pharmacokinetics and pharmacodynamics of ramucirumab in the treatment of colorectal cancer. Expert Opin. Drug Metab. Toxicol. 2016, 12, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Patel, A. Ziv-aflibercept in metastatic colorectal cancer. Biol. Targets Ther. 2014, 8, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Ciombor, K.K.; Berlin, J. Aflibercept—A Decoy VEGF Receptor. Curr. Oncol. Rep. 2014, 16, 368. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Garcia, E.; Saurí, T.; Tabernero, J.; Macarulla, T. Pharmacokinetic and pharmacodynamic evaluation of aflibercept for the treatment of colorectal cancer. Expert Opin. Drug Metab. Toxicol. 2015, 11, 995–1004. [Google Scholar] [CrossRef] [PubMed]
- Tadayoni, R.; Sararols, L.; Weissgerber, G.; Verma, R.; Clemens, A.; Holz, F.G. Brolucizumab: A Newly Developed Anti-VEGF Molecule for the Treatment of Neovascular Age-Related Macular Degeneration. Ophthalmologica 2021, 244, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Abu Serhan, H.; Taha, M.J.J.; Abuawwad, M.T.; Abdelaal, A.; Irshaidat, S.; Abu Serhan, L.; Abu Salim, Q.F.; Awamleh, N.; Abdelazeem, B.; Elnahry, A.G. Safety and Efficacy of Brolucizumab in the Treatment of Diabetic Macular Edema and Diabetic Retinopathy: A Systematic Review and Meta-Analysis. Semin. Ophthalmol. 2023, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jakubiak, P.; Alvarez-Sánchez, R.; Fueth, M.; Broders, O.; Kettenberger, H.; Stubenrauch, K.; Caruso, A. Ocular Pharmacokinetics of Intravitreally Injected Protein Therapeutics: Comparison among Standard-of-Care Formats. Mol. Pharm. 2021, 18, 2208–2217. [Google Scholar] [CrossRef] [PubMed]
- Veritti, D.; Sarao, V.; Gorni, G.; Lanzetta, P. Anti-VEGF Drugs Dynamics: Relevance for Clinical Practice. Pharmaceutics 2022, 14, 265. [Google Scholar] [CrossRef]
- Chatziralli, I. Ranibizumab for the treatment of diabetic retinopathy. Expert Opin. Biol. Ther. 2021, 21, 991–997. [Google Scholar] [CrossRef]
- Dervenis, N.; Mikropoulou, A.M.; Tranos, P.; Dervenis, P. Ranibizumab in the Treatment of Diabetic Macular Edema: A Review of the Current Status, Unmet Needs, and Emerging Challenges. Adv. Ther. 2017, 34, 1270–1282. [Google Scholar] [CrossRef]
- García-Quintanilla, L.; Luaces-Rodríguez, A.; Gil-Martínez, M.; Mondelo-García, C.; Maroñas, O.; Mangas-Sanjuan, V.; González-Barcia, M.; Zarra-Ferro, I.; Aguiar, P.; Otero-Espinar, F.J.; et al. Pharmacokinetics of Intravitreal Anti-VEGF Drugs in Age-Related Macular Degeneration. Pharmaceutics 2019, 11, 365. [Google Scholar] [CrossRef] [PubMed]
- Sharma, K.; Suresh, P.S.; Mullangi, R.; Srinivas, N.R. Quantitation of VEGFR2 (vascular endothelial growth factor receptor) inhibitors—Review of assay methodologies and perspectives. Biomed. Chromatogr. 2015, 29, 803–834. [Google Scholar] [CrossRef] [PubMed]
- Uemura, A.; Fruttiger, M.; D’Amore, P.A.; De Falco, S.; Joussen, A.M.; Sennlaub, F.; Brunck, L.R.; Johnson, K.T.; Lambrou, G.N.; Rittenhouse, K.D.; et al. VEGFR1 signaling in retinal angiogenesis and microinflammation. Prog. Retin. Eye Res. 2021, 84, 100954. [Google Scholar] [CrossRef] [PubMed]
- Șandor, A.; Ionuț, I.; Marc, G.; Oniga, I.; Eniu, D.; Oniga, O. Structure–Activity Relationship Studies Based on Quinazoline Derivatives as EGFR Kinase Inhibitors (2017–Present). Pharmaceuticals 2023, 16, 534. [Google Scholar] [CrossRef]
- Dorff, T.B.; Pal, S.K.; Quinn, D.I. Novel tyrosine kinase inhibitors for renal cell carcinoma. Expert Rev. Clin. Pharmacol. 2014, 7, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.J.; Kulkarni, V.M. Exploration of structural requirements for the inhibition of VEGFR-2 tyrosine kinase: Binding site analysis of type II, ‘DFG-out’ inhibitors. J. Biomol. Struct. Dyn. 2022, 40, 5712–5727. [Google Scholar] [CrossRef]
- Takahashi, S. Vascular endothelial growth factor (VEGF), VEGF receptors and their inhibitors for antiangiogenic tumor therapy. Biol. Pharm. Bull. 2011, 34, 1785–1788. [Google Scholar] [CrossRef]
- Hao, Z.; Sadek, I. Sunitinib: The antiangiogenic effects and beyond. OncoTargets Ther. 2016, 9, 5495–5505. [Google Scholar] [CrossRef]
- Nassif, E.; Thibault, C.; Vano, Y.; Fournier, L.; Mauge, L.; Verkarre, V.; Timsit, M.-O.; Mejean, A.; Tartour, E.; Oudard, S. Sunitinib in kidney cancer: 10 years of experience and development. Expert Rev. Anticancer. Ther. 2017, 17, 129–142. [Google Scholar] [CrossRef]
- Al-Ghusn, A.I.; Bakheit, A.H.; Attwa, M.W.; AlRabiah, H. Vandetanib. In Profiles of Drug Substances, Excipients, and Related Methodology; Academic Press: New York, NY, USA, 2023; Volume 48, pp. 109–134. [Google Scholar] [CrossRef]
- Miyamoto, S.; Kakutani, S.; Sato, Y.; Hanashi, A.; Kinoshita, Y.; Ishikawa, A. Drug review: Pazopanib. Jpn. J. Clin. Oncol. 2018, 48, 503–513. [Google Scholar] [CrossRef]
- Limvorasak, S.; Posadas, E.M. Pazopanib: Therapeutic developments. Expert Opin. Pharmacother. 2009, 10, 3091–3102. [Google Scholar] [CrossRef]
- Chen, Y.; Tortorici, M.A.; Garrett, M.; Hee, B.; Klamerus, K.J.; Pithavala, Y.K. Clinical pharmacology of axitinib. Clin. Pharmacokinet. 2013, 52, 713–725. [Google Scholar] [CrossRef] [PubMed]
- Maroto, P.; Porta, C.; Capdevila, J.; Apolo, A.B.; Viteri, S.; Rodriguez-Antona, C.; Martin, L.; Castellano, D. Cabozantinib for the treatment of solid tumors: A systematic review. Ther. Adv. Med. Oncol. 2022, 14, 17588359221107112. [Google Scholar] [CrossRef] [PubMed]
- Ettrich, T.J.; Seufferlein, T. Regorafenib. Recent results in cancer research. Fortschritte der Krebsforschung. Prog. Dans Les Rech. Sur Le Cancer 2018, 211, 45–56. [Google Scholar] [CrossRef]
- Arai, H.; Battaglin, F.; Wang, J.; Lo, J.H.; Soni, S.; Zhang, W.; Lenz, H.-J. Molecular insight of regorafenib treatment for colorectal cancer. Cancer Treat. Rev. 2019, 81, 101912. [Google Scholar] [CrossRef] [PubMed]
- Strumberg, D.; Schultheis, B. Regorafenib for cancer. Expert Opin. Investig. Drugs 2012, 21, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Lamb, Y.N. Nintedanib: A Review in Fibrotic Interstitial Lung Diseases. Drugs 2021, 81, 575–586. [Google Scholar] [CrossRef]
- Wind, S.; Schmid, U.; Freiwald, M.; Marzin, K.; Lotz, R.; Ebner, T.; Stopfer, P.; Dallinger, C. Clinical Pharmacokinetics and Pharmacodynamics of Nintedanib. Clin. Pharmacokinet. 2019, 58, 1131–1147. [Google Scholar] [CrossRef]
- Gao, Y.; Ding, Y.; Tai, X.-R.; Zhang, C.; Wang, D. Ponatinib: An update on its drug targets, therapeutic potential and safety. Biochim. Biophys. Acta BBA Rev. Cancer 2023, 1878, 188949. [Google Scholar] [CrossRef]
- Motzer, R.J.; Taylor, M.H.; Evans, T.R.J.; Okusaka, T.; Glen, H.; Lubiniecki, G.M.; Dutcus, C.; Smith, A.D.; Okpara, C.E.; Hussein, Z.; et al. Lenvatinib dose, efficacy, and safety in the treatment of multiple malignancies. Expert Rev. Anticancer Ther. 2022, 22, 383–400. [Google Scholar] [CrossRef]
- Hao, Z.; Wang, P. Lenvatinib in Management of Solid Tumors. Oncologist 2020, 25, e302–e310. [Google Scholar] [CrossRef] [PubMed]
- Chawla, P.A.; Passi, I.; Billowria, K.; Kumar, B. Tivozanib: A New Hope for Treating Renal Cell Carcinoma. Anticancer Agents Med. Chem. 2023, 23, 562–570. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.; Zhou, J.; Guo, Z.; Diao, X.; Gao, Z.; Zhong, D.; Jiang, H.; Zhang, L.; Chen, X. Metabolism and bioactivation of famitinib, a novel inhibitor of receptor tyrosine kinase, in cancer patients. Br. J. Pharmacol. 2013, 168, 1687–1706. [Google Scholar] [CrossRef]
- Scott, L.J. Apatinib: A Review in Advanced Gastric Cancer and Other Advanced Cancers. Drugs 2018, 78, 747–758. [Google Scholar] [CrossRef]
- Geng, R.; Li, J. Apatinib for the treatment of gastric cancer. Expert Opin. Pharmacother. 2015, 16, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Schenone, S.; Bondavalli, F.; Botta, M. Antiangiogenic agents: An update on small molecule VEGFR inhibitors. Curr. Med. Chem. 2007, 14, 2495–2516. [Google Scholar] [CrossRef]
- Chaar, M.; Kamta, J.; Ait-Oudhia, S. Mechanisms, monitoring, and management of tyrosine kinase inhibitors-associated cardiovascular toxicities. OncoTargets Ther. 2018, 11, 6227–6237. [Google Scholar] [CrossRef]
- Dembinska-Kiec, A.; Dulak, J.; Partyka, L.; Huk, I.; Mailnski, T. VEGF–nitric oxide reciprocal regulation. Nat. Med. 1997, 3, 1177. [Google Scholar] [CrossRef]
- Feliers, D.; Chen, X.; Akis, N.; Choudhury, G.G.; Madaio, M.; Kasinath, B.S. VEGF regulation of endothelial nitric oxide synthase in glomerular endothelial cells. Kidney Int. 2005, 68, 1648–1659. [Google Scholar] [CrossRef]
- Kroll, J.; Waltenberger, J. A novel function of VEGF receptor-2 (KDR): Rapid release of nitric oxide in response to VEGF-A stimulation in endothelial cells. Biochem. Biophys. Res. Commun. 1999, 265, 636–639. [Google Scholar] [CrossRef]
- Sane, D.C.; Anton, L.; Brosnihan, K.B. Angiogenic growth factors and hypertension. Angiogenesis 2004, 7, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Greene, A.S.; Amaral, S.L. Microvascular angiogenesis and the renin-angiotensin system. Curr. Hypertens. Rep. 2002, 4, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Byrne, A.M.; Bouchier-Hayes, D.; Harmey, J. Angiogenic and cell survival functions of Vascular Endothelial Growth Factor (VEGF). J. Cell. Mol. Med. 2005, 9, 777–794. [Google Scholar] [CrossRef] [PubMed]
- Van Hinsbergh, V.W.M. Endothelium—Role in regulation of coagulation and inflammation. Semin. Immunopathol. 2012, 34, 93–106. [Google Scholar] [CrossRef] [PubMed]
- van Hinsbergh, V.W. The endothelium: Vascular control of haemostasis. European journal of obstetrics, gynecology, and reproductive biology. Eur. J. Obstet. Gynecol. Reprod. Biol. 2001, 95, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Wautier, J.-L.; Wautier, M.-P. Vascular Permeability in Diseases. Int. J. Mol. Sci. 2022, 23, 3645. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.; Olsen, B.R. The roles of vascular endothelial growth factor in bone repair and regeneration. Bone 2016, 91, 30–38. [Google Scholar] [CrossRef]
- DiPietro, L.A. Angiogenesis and wound repair: When enough is enough. J. Leukoc. Biol. 2016, 100, 979–984. [Google Scholar] [CrossRef]
- Parmar, D.; Apte, M. Angiopoietin inhibitors: A review on targeting tumor angiogenesis. Eur. J. Pharmacol. 2021, 899, 174021. [Google Scholar] [CrossRef]
- Cutroneo, P.M.; Giardina, C.; Ientile, V.; Potenza, S.; Sottosanti, L.; Ferrajolo, C.; Trombetta, C.J.; Trifirò, G. Overview of the Safety of Anti-VEGF Drugs: Analysis of the Italian Spontaneous Reporting System. Drug Saf. 2017, 40, 1131–1140. [Google Scholar] [CrossRef]
- Jiang, L.; Ping, L.; Yan, H.; Yang, X.; He, Q.; Xu, Z.; Luo, P. Cardiovascular toxicity induced by anti-VEGF/VEGFR agents: A special focus on definitions, diagnoses, mechanisms and management. Expert Opin. Drug Metab. Toxicol. 2020, 16, 823–835. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, K.; Rolfo, C.; Dewaele, E.; Van De Wiel, M.; Brande, J.V.D.; Altintas, S.; Huizing, M.; Specenier, P.; Peeters, M. Incorporating anti-VEGF pathway therapy as a continuum of care in metastatic colorectal cancer. Curr. Treat. Options Oncol. 2015, 16, 18. [Google Scholar] [CrossRef]
- Riondino, S.; Del Monte, G.; Fratangeli, F.; Guadagni, F.; Roselli, M.; Ferroni, P. Anti-Angiogenic Drugs, Vascular Toxicity and Thromboembolism in Solid Cancer. Cardiovasc. Hematol. Agents Med. Chem. 2017, 15, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Caraglia, M.; Santini, D.; Bronte, G.; Rizzo, S.; Sortino, G.; Rini, G.B.; Di Fede, G.; Russo, A. Predicting Efficacy and Toxicity in the Era of Targeted Therapy: Focus on Anti-EGFR and Anti-VEGF Molecules. Curr. Drug Metab. 2011, 12, 944–955. [Google Scholar] [CrossRef] [PubMed]
- Hayman, S.R.; Leung, N.; Grande, J.P.; Garovic, V.D. VEGF Inhibition, Hypertension, and Renal Toxicity. Curr. Oncol. Rep. 2012, 14, 285–294. [Google Scholar] [CrossRef]
- Chen, H.X.; Cleck, J.N. Adverse effects of anticancer agents that target the VEGF pathway. Nat. Rev. Clin. Oncol. 2009, 6, 465–477. [Google Scholar] [CrossRef]
- Bracha, P.; Moore, N.A.; Ciulla, T.A.; WuDunn, D.; Cantor, L.B. The acute and chronic effects of intravitreal anti-vascular endothelial growth factor injections on intraocular pressure: A review. Surv. Ophthalmol. 2018, 63, 281–295. [Google Scholar] [CrossRef]
- Boyer, D.S.; Hopkins, J.J.; Sorof, J.; Ehrlich, J.S. Anti-vascular endothelial growth factor therapy for diabetic macular edema. Ther. Adv. Endocrinol. Metab. 2013, 4, 151–169. [Google Scholar] [CrossRef]
- Rodrigues, E.B.; Farah, M.E.; Maia, M.; Penha, F.M.; Regatieri, C.; Melo, G.B.; Pinheiro, M.M.; Zanetti, C.R. Therapeutic monoclonal antibodies in ophthalmology. Prog. Retin. Eye Res. 2009, 28, 117–144. [Google Scholar] [CrossRef]
- Hsu, S.T.; Ponugoti, A.; Deaner, J.D.; Vajzovic, L. Update on Retinal Drug Toxicities. Curr. Ophthalmol. Rep. 2021, 9, 168–177. [Google Scholar] [CrossRef]
- Ollero, M.; Sahali, D. Inhibition of the VEGF signalling pathway and glomerular disorders. Nephrol. Dial. Transpl. 2015, 30, 1449–1455. [Google Scholar] [CrossRef] [PubMed]
- Ferroni, P.; Formica, V.; Roselli, M.; Guadagni, F. Thromboembolic events in patients treated with anti-angiogenic drugs. Curr. Vasc. Pharmacol. 2010, 8, 102–113. [Google Scholar] [CrossRef]
- Braile, M.; Marcella, S.; Cristinziano, L.; Galdiero, M.R.; Modestino, L.; Ferrara, A.L.; Varricchi, G.; Marone, G.; Loffredo, S. VEGF-A in Cardiomyocytes and Heart Diseases. Int. J. Mol. Sci. 2020, 21, 5294. [Google Scholar] [CrossRef]
- Kivelä, R.; Hemanthakumar, K.A.; Vaparanta, K.; Robciuc, M.; Izumiya, Y.; Kidoya, H.; Takakura, N.; Peng, X.; Sawyer, D.B.; Elenius, K.; et al. Endothelial Cells Regulate Physiological Cardiomyocyte Growth via VEGFR2-Mediated Paracrine Signaling. Circulation 2019, 139, 2570–2584. [Google Scholar] [CrossRef] [PubMed]
- Bagnes, C.; Panchuk, P.N.; Recondo, G. Antineoplastic chemotherapy induced QTc prolongation. Curr. Drug Saf. 2010, 5, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Witchel, H.J. Drug-induced hERG Block and Long QT Syndrome. Cardiovasc. Ther. 2011, 29, 251–259. [Google Scholar] [CrossRef]
- Thomas, S.H.L.; Behr, E.R. Pharmacological treatment of acquired QT prolongation and torsades de pointes. Br. J. Clin. Pharmacol. 2016, 81, 420–427. [Google Scholar] [CrossRef]
- Tisdale, J.E. Drug-induced QT interval prolongation and torsades de pointes: Role of the pharmacist in risk assessment, prevention and management. Can. Pharm. J. 2016, 149, 139–152. [Google Scholar] [CrossRef]
- Walraven, M.; Witteveen, P.O.; Lolkema, M.P.J.; van Hillegersberg, R.; Voest, E.E.; Verheul, H.M.W. Antiangiogenic tyrosine kinase inhibition related gastrointestinal perforations: A case report and literature review. Angiogenesis 2011, 14, 135–141. [Google Scholar] [CrossRef]
- Maeda, Y.; Shinohara, T.; Minagawa, N.; Kobayashi, T.; Koyama, R.; Shimada, S.; Tsunetoshi, Y.; Murayama, K.; Hasegawa, H. A retrospective analysis of emergency surgery for cases of acute abdomen during cancer chemotherapy. Case series. Ann. Med. Surg. 2020, 57, 143–147. [Google Scholar] [CrossRef]
- Roodhart, J.M.; Langenberg, M.H.; Witteveen, E.; Voest, E.E. The Molecular Basis of Class Side Effects Due to Treatment with Inhibitors of the VEGF/VEGFR Pathway. Curr. Clin. Pharmacol. 2008, 3, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Detmar, M. The role of VEGF and thrombospondins in skin angiogenesis. J. Dermatol. Sci. 2000, 24 (Suppl. 1), S78–S84. [Google Scholar] [CrossRef] [PubMed]
- Tlemsani, C.; Mir, O.; Boudou-Rouquette, P.; Huillard, O.; Maley, K.; Ropert, S.; Coriat, R.; Goldwasser, F. Posterior reversible encephalopathy syndrome induced by anti-VEGF agents. Target. Oncol. 2011, 6, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Shord, S.S.; Bressler, L.R.; Tierney, L.A.; Cuellar, S.; George, A. Understanding and managing the possible adverse effects associated with bevacizumab. Am. J. Health-System Pharm. 2009, 66, 999–1013. [Google Scholar] [CrossRef] [PubMed]
- Schmidinger, M. Understanding and managing toxicities of vascular endothelial growth factor (VEGF) inhibitors. Eur. J. Cancer Suppl. 2013, 11, 172–191. [Google Scholar] [CrossRef] [PubMed]
- Arora, N.; Gupta, A.; Singh, P.P. Biological agents in gastrointestinal cancers: Adverse effects and their management. J. Gastrointest. Oncol. 2017, 8, 485–498. [Google Scholar] [CrossRef]
- Peters, A.; Schweiger, U.; Frühwald-Schultes, B.; Born, J.; Fehm, H.L. The neuroendocrine control of glucose allocation. Exp. Clin. Endocrinol. Diabetes 2002, 110, 199–211. [Google Scholar] [CrossRef]
- Liu, Y.; Olsen, B.R. Distinct VEGF Functions During Bone Development and Homeostasis. Arch. Immunol. Ther. Exp. 2014, 62, 363–368. [Google Scholar] [CrossRef]
- Florentin, J.; O’Neil, S.P.; Ohayon, L.L.; Uddin, A.; Vasamsetti, S.B.; Arunkumar, A.; Ghosh, S.; Boatz, J.C.; Sui, J.; Kliment, C.R.; et al. VEGF Receptor 1 Promotes Hypoxia-Induced Hematopoietic Progenitor Proliferation and Differentiation. Front. Immunol. 2022, 13, 882484. [Google Scholar] [CrossRef]
- Fons, P.; Herault, J.P.; Delesque, N.; Tuyaret, J.; Bono, F.; Herbert, J.M. VEGF-R2 and neuropilin-1 are involved in VEGF-A-induced differentiation of human bone marrow progenitor cells. J. Cell. Physiol. 2004, 200, 351–359. [Google Scholar] [CrossRef]
- Kampougeris, G.; Spyropoulos, D.; Mitropoulou, A. Intraocular Pressure rise after Anti-VEGF Treatment: Prevalence, Possible Mechanisms and Correlations. J. Curr. Glaucoma Pract. 2013, 7, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Good, T.J.; Kimura, A.E.; Mandava, N.; Kahook, M.Y. Sustained elevation of intraocular pressure after intravitreal injections of anti-VEGF agents. Br. J. Ophthalmol. 2010, 95, 1111–1114. [Google Scholar] [CrossRef]
- Cox, J.T.; Eliott, D.; Sobrin, L. Inflammatory Complications of Intravitreal Anti-VEGF Injections. J. Clin. Med. 2021, 10, 981. [Google Scholar] [CrossRef] [PubMed]
- Palestine, A.G.; Pecen, P.E. Infectious Endophthalmitis in the Current Era. Ophthalmol. Retin. 2020, 4, 553–554. [Google Scholar] [CrossRef]
- Brinda, B.J.; Viganego, F.; Vo, T.; Dolan, D.; Fradley, M.G. Anti-VEGF-Induced Hypertension: A Review of Pathophysiology and Treatment Options. Curr. Treat. Options Cardiovasc. Med. 2016, 18, 33. [Google Scholar] [CrossRef] [PubMed]
- Ishak, R.S.; Aad, S.A.; Kyei, A.; Farhat, F.S. Cutaneous manifestations of anti-angiogenic therapy in oncology: Review with focus on VEGF inhibitors. Crit. Rev. Oncol. Hematol. 2014, 90, 152–164. [Google Scholar] [CrossRef]
- Wang, P.; Wang, D.; Meng, A.B.; Zhi, X.; Zhu, P.; Lu, L.; Tang, L.; Pu, Y.; Li, X. Effects of Walking on Fatigue in Cancer Patients: A Systematic Review and Meta-analysis. Cancer Nurs. 2022, 45, E270–E278. [Google Scholar] [CrossRef]
- Baumal, C.R.; Spaide, R.F.; Vajzovic, L.; Freund, K.B.; Walter, S.D.; John, V.; Rich, R.; Chaudhry, N.; Lakhanpal, R.R.; Oellers, P.R.; et al. Retinal Vasculitis and Intraocular Inflammation after Intravitreal Injection of Brolucizumab. Ophthalmology 2020, 127, 1345–1359. [Google Scholar] [CrossRef]
- van Dorst, D.C.; Dobbin, S.J.; Neves, K.B.; Herrmann, J.; Herrmann, S.M.; Versmissen, J.; Mathijssen, R.H.; Danser, A.J.; Lang, N.N. Hypertension and Prohypertensive Antineoplastic Therapies in Cancer Patients. Circ. Res. 2021, 128, 1040–1061. [Google Scholar] [CrossRef]
- Schiffer, M.; Zukovic, L.; Hall, S.; Merl, M.Y. Assessment of extended urine protein monitoring frequency in patients receiving bevacizumab. J. Oncol. Pharm. Pract. 2021, 27, 902–906. [Google Scholar] [CrossRef]
- Raskob, G.E.; Silverstein, R.; Bratzler, D.W.; Heit, J.A.; White, R.H. Surveillance for deep vein thrombosis and pulmonary embolism: Recommendations from a national workshop. Am. J. Prev. Med. 2010, 38, S502–S509. [Google Scholar] [CrossRef] [PubMed]
- Santoni, M.; Guerra, F.; Conti, A.; Lucarelli, A.; Rinaldi, S.; Belvederesi, L.; Capucci, A.; Berardi, R. Incidence and risk of cardiotoxicity in cancer patients treated with targeted therapies. Cancer Treat. Rev. 2017, 59, 123–131. [Google Scholar] [CrossRef]
- Machado, M.O.; Kang, N.C.; Tai, F.; Sambhi, R.D.S.; Berk, M.; Carvalho, A.F.; Chada, L.P.; Merola, J.F.; Piguet, V.; Alavi, A. Measuring fatigue: A meta-review. Int. J. Dermatol. 2021, 60, 1053–1069. [Google Scholar] [CrossRef] [PubMed]
- Russell, M.K. Functional Assessment of Nutrition Status. Nutr. Clin. Pract. 2015, 30, 211–218. [Google Scholar] [CrossRef]
- Taberna, D.J.; Navas-Carretero, S.; Martinez, J.A. Current nutritional status assessment tools for metabolic care and clinical nutrition. Curr. Opin. Clin. Nutr. Metab. Care 2019, 22, 323–328. [Google Scholar] [CrossRef]
- Stewart, M.W.; Browning, D.J.; Landers, M.B. Current management of diabetic tractional retinal detachments. Indian J. Ophthalmol. 2018, 66, 1751–1762. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.G.; Maddess, T. The Clinical Interpretation of Changes in Intraocular Pressure Measurements Using Goldmann Applanation Tonometry: A Review. J. Glaucoma 2019, 28, 302–306. [Google Scholar] [CrossRef]
- Baddam, D.O.; Ragi, S.D.; Tsang, S.H.; Ngo, W.K. Ophthalmic Fluorescein Angiography. Methods Mol. Biol. 2023, 2560, 153–160. [Google Scholar] [CrossRef]
- Hamnvik, O.R.; Choueiri, T.K.; Turchin, A.; McKay, R.R.; Goyal, L.; Davis, M.; Kaymakcalan, M.D.; Williams, J.S. Clinical risk factors for the development of hypertension in patients treated with inhibitors of the VEGF signaling pathway. Cancer 2015, 121, 311–319. [Google Scholar] [CrossRef]
- Moriyama, S.; Hieda, M.; Kisanuki, M.; Kawano, S.; Yokoyama, T.; Fukata, M.; Kusaba, H.; Maruyama, T.; Baba, E.; Akashi, K.; et al. Effect of renin–angiotensin system inhibitors in patients with cancer treated with anti-VEGF therapy. Open Heart 2022, 9, e002135. [Google Scholar] [CrossRef]
- Koskina, L.; Andrikou, I.; Thomopoulos, C.; Tsioufis, K. Preexisting hypertension and cancer therapy: Evidence, pathophysiology, and management recommendation. J. Hum. Hypertens. 2023, 37, 331–337. [Google Scholar] [CrossRef]
- Zhu, X.; Wu, S.; Dahut, W.L.; Parikh, C.R. Risks of proteinuria and hypertension with bevacizumab, an antibody against vascular endothelial growth factor: Systematic review and meta-analysis. Am. J. Kidney Dis. 2007, 49, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Faruque, L.I.; Lin, M.; Battistella, M.; Wiebe, N.; Reiman, T.; Hemmelgarn, B.; Thomas, C.; Tonelli, M. Systematic review of the risk of adverse outcomes associated with vascular endothelial growth factor inhibitors for the treatment of cancer. PLoS ONE 2014, 9, e101145. [Google Scholar] [CrossRef]
- Abbas, A.; Mirza, M.M.; Ganti, A.K.; Tendulkar, K. Renal Toxicities of Targeted Therapies. Target. Oncol. 2015, 10, 487–499. [Google Scholar] [CrossRef] [PubMed]
- Tesařová, P.; Tesař, V. Proteinuria and hypertension in patients treated with inhibitors of the VEGF signalling pathway-incidence, mechanisms and management. Folia Biol. 2013, 59, 15–25. [Google Scholar]
- Meilhac, A.; Cautela, J.; Thuny, F. Cancer Therapies and Vascular Toxicities. Curr. Treat. Options Oncol. 2022, 23, 333–347. [Google Scholar] [CrossRef]
- Watson, N.; Al-Samkari, H. Thrombotic and bleeding risk of angiogenesis inhibitors in patients with and without malignancy. J. Thromb. Haemost. 2021, 19, 1852–1863. [Google Scholar] [CrossRef]
- Touyz, R.M.; Herrmann, S.M.; Herrmann, J. Vascular toxicities with VEGF inhibitor therapies–focus on hypertension and arterial thrombotic events. J. Am. Soc. Hypertens. 2018, 12, 409–425. [Google Scholar] [CrossRef]
- Sundararajan, S.; Kumar, A.; Poongkunran, M.; Kannan, A.; Vogelzang, N.J.; Reck, M.; Heigener, D.; Reinmuth, N.; Sullivan, I.; Planchard, D.; et al. Cardiovascular adverse effects of targeted antiangiogenic drugs: Mechanisms and management. Future Oncol. 2016, 12, 1067–1080. [Google Scholar] [CrossRef]
- Mihalcea, D.; Memis, H.; Mihaila, S.; Vinereanu, D. Cardiovascular Toxicity Induced by Vascular Endothelial Growth Factor Inhibitors. Life 2023, 13, 366. [Google Scholar] [CrossRef]
- Dobbin, S.J.; Petrie, M.C.; Myles, R.C.; Touyz, R.M.; Lang, N.N. Cardiotoxic effects of angiogenesis inhibitors. Clin. Sci. 2021, 135, 71–100. [Google Scholar] [CrossRef] [PubMed]
- Sandler, A.; Hirsh, V.; Reck, M.; von Pawel, J.; Akerley, W.; Johnson, D.H. An evidence-based review of the incidence of CNS bleeding with anti-VEGF therapy in non-small cell lung cancer patients with brain metastases. Lung Cancer 2012, 78, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zuo, P.-Y.; Chen, X.-L.; Liu, Y.-W.; Xiao, C.-L.; Liu, C.-Y. Increased risk of cerebrovascular events in patients with cancer treated with bevacizumab: A meta-analysis. PLoS ONE 2014, 9, e102484. [Google Scholar] [CrossRef] [PubMed]
- McLellan, B.; Ciardiello, F.; Lacouture, M.E.; Segaert, S.; Van Cutsem, E. Regorafenib-associated hand–foot skin reaction: Practical advice on diagnosis, prevention, and management. Ann. Oncol. 2015, 26, 2017–2026. [Google Scholar] [CrossRef] [PubMed]
- Manchen, E.; Robert, C.; Porta, C. Management of tyrosine kinase inhibitor-induced hand-foot skin reaction: Viewpoints from the medical oncologist, dermatologist, and oncology nurse. J. Support. Oncol. 2011, 9, 13–23. [Google Scholar] [CrossRef]
- Sugita, K.; Kawakami, K.; Yokokawa, T.; Mae, Y.; Toya, W.; Hagino, A.; Suzuki, K.; Suenaga, M.; Mizunuma, N.; Yamaguchi, T.; et al. Investigation of Regorafenib-induced Hypothyroidism in Patients with Metastatic Colorectal Cancer. Anticancer Res. 2015, 35, 4059–4062. [Google Scholar]
- Fernández, A.A.; Martín, P.; Martínez, M.I.; Bustillo, M.A.; Hernández, F.J.B.; Labrado, J.d.l.C.; Peñas, R.D.-D.; Rivas, E.G.; Delgado, C.P.; Redondo, J.R.; et al. Chronic fatigue syndrome: Aetiology, diagnosis and treatment. BMC Psychiatry 2009, 9, S1. [Google Scholar] [CrossRef]
- Eisen, T.; Sternberg, C.N.; Robert, C.; Mulders, P.; Pyle, L.; Zbinden, S.; Izzedine, H.; Escudier, B. Targeted Therapies for renal cell carcinoma: Review of adverse event management strategies. JNCI J. Natl. Cancer Inst. 2012, 104, 93–113. [Google Scholar] [CrossRef]
- Hartmann, J.T.; Haap, M.; Kopp, H.G.; Lipp, H.P. Tyrosine kinase inhibitors—A review on pharmacology, metabolism and side effects. Curr. Drug Metab. 2009, 10, 470–481. [Google Scholar] [CrossRef]
- Fachi, M.M.; Tonin, F.S.; Leonart, L.P.; Rotta, I.; Fernandez-Llimos, F.; Pontarolo, R. Haematological adverse events associated with tyrosine kinase inhibitors in chronic myeloid leukaemia: A network meta-analysis. Br. J. Clin. Pharmacol. 2019, 85, 2280–2291. [Google Scholar] [CrossRef]
- Falavarjani, K.G.; Nguyen, Q.D. Adverse events and complications associated with intravitreal injection of anti-VEGF agents: A review of literature. Eye 2013, 27, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Van der Reis, M.I.; La Heij, E.C.; De Jong-Hesse, Y.; Ringens, P.J.; Hendrikse, F.; Schouten, J.S.A.G. A systematic review of the adverse events of intravitreal anti-vascular endothelial growth factor injections. Retina 2011, 31, 1449–1469. [Google Scholar] [CrossRef] [PubMed]
- Tolentino, M. Systemic and ocular safety of intravitreal anti-vegf therapies for ocular neovascular disease. Surv. Ophthalmol. 2011, 56, 95–113. [Google Scholar] [CrossRef] [PubMed]
- Day, S.; Acquah, K.; Mruthyunjaya, P.; Grossman, D.S.; Lee, P.P.; Sloan, F.A. Ocular complications after anti–vascular endothelial growth factor therapy in medicare patients with age-related macular degeneration. Arch. Ophthalmol. 2011, 152, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Daka, Q.; Špegel, N.; Velkovska, M.A.; Steblovnik, T.; Kolko, M.; Neziri, B.; Cvenkel, B. Exploring the Relationship between Anti-VEGF Therapy and Glaucoma: Implications for Management Strategies. J. Clin. Med. 2023, 12, 4674. [Google Scholar] [CrossRef]
- Singh, R.S.J.; Kim, J.E. Ocular hypertension following intravitreal anti-vascular endothelial growth factor agents. Drugs Aging 2012, 29, 949–956. [Google Scholar] [CrossRef]
- Baumal, C.R.; Bodaghi, B.; Singer, M.; Tanzer, D.J.; Seres, A.; Joshi, M.R.; Feltgen, N.; Gale, R. Expert Opinion on Management of Intraocular Inflammation, Retinal Vasculitis, and Vascular Occlusion after Brolucizumab Treatment. Ophthalmol. Retina. 2021, 5, 519–527. [Google Scholar] [CrossRef]
- Shao, E.H.; Yates, W.B.; Ho, I.-V.; Chang, A.A.; Simunovic, M.P. Endophthalmitis: Changes in Presentation, Management and the Role of Early Vitrectomy. Ophthalmol. Ther. 2021, 10, 877–890. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Toxicity | Incidence (%) | |
|---|---|---|
| Intra-Venous | Intra-Vitreal | |
| Anaemia | 8 | NS |
| Anorexia | 13–58 | NS |
| Asthenia and fatigue | 50 | NS |
| Bowel and nasal septum perforation | <0.5 | NS |
| Brolucizumab-Associated Retinal Vasculitis | NS | 0.8 |
| Cardiac toxicity | <0.5 | NS |
| Conjunctival hemorrhage | NS | 20–40 |
| Diarrhea | 13–74 | NS |
| Hemorrhage | <0.5 | NS |
| Hypertension | 25 | NS |
| Hypothyroidism | 10 | NS |
| Infectious Endophthalmitis | NS | <0.001 |
| Infusion-related hypersensitivity reactions | <0.5 | NS |
| Intraocular inflammation | NS | <0.37 |
| Lymphopenia | 18 | NS |
| Mucositis | 4–42 | NS |
| Nausea/vomiting | 10–39 | NS |
| Neutropenia | 18 | NS |
| Ocular Hypertension | NS | 2.1–3.6 |
| Proteinuria | 8 | NS |
| Retinal hemorrhage | NS | 1–10 |
| Reversible Posterior Leukoencephalopathy Syndrome | <0.05 | NS |
| Rhegmatogenous retinal detachments | NS | 0.013 |
| Skin toxicity | 50 | NS |
| Thrombocytopenia | 9 | NS |
| Thromboembolic events | 0.6–5.6 | NS |
| Vitreous floaters | NS | 5–15 |
| Toxicity | Mechanism |
|---|---|
| Hypertension | Disruption of VEGF/VEGFR pathway leads to endothelial dysfunction and vasoconstriction. |
| Proteinuria | Inhibition of VEGF-A alters glomerular permeability, resulting in proteinuria and peripheral edema. |
| Thromboembolic events | Disruption of VEGF/VEGFR pathway causes endothelial cell damage. |
| Cardiac toxicity | VEGF-A inhibition may produce cardiomyocytes damage. Direct effects on hERG channels may cause arrhythmias. |
| Hemorrhage | VEGF/VEGFR pathway alteration compromises blood vessel integrity, leading to abnormal permeability and bleeding. |
| Bowel and nasal septum perforation | Arise from VEGFi-induced tumor necrosis or mucosal injury associated with the disruption of micro-circulation. This disruption weakens the mucosal wall, ultimately leading to arteriolar thrombosis. |
| Skin toxicity | Exact mechanism is unclear, hypothesized to stem from VEGF signaling disruption, affecting blood flow and vascular permeability in the skin. |
| Reversible Posterior Leukoencephalopathy | Mechanism likely related to VEGF pathway disruption, increasing vascular permeability at the blood-brain barrier level. |
| Infusion-related hypersensitivity | Exact mechanism unclear. |
| Hypothyroidism | Direct cytotoxic effects on thyroid follicular cells and vascular alterations in the thyroid gland. |
| Asthenia and fatigue | Potential causes include hypothyroidism, myocardial changes, VEGF-inhibitor-induced anorexia, and dehydration. |
| Gastrointestinal toxicity | VEGF inhibition diminishes blood flow to mucosal tissues, causing inflammation and damage. |
| Anorexia | Hypothesized to involve central nervous system interactions, potentially linked to changes in neuroendocrine signaling and appetite regulation. |
| Myelotoxicity | VEGFi impacts bone marrow by disrupting vascular networks and directly affecting hematopoietic stem cells, leading to diminished blood cell production. |
| Ocular hypertension | Anti-VEGF injections lead to transient intraocular pressure elevation, with repetitive injections linked to persistent ocular hypertension. |
| Intraocular inflammation | Pathogenesis unclear, may be linked to patient-specific immune responses, manufacturing impurities, and errors in provider preparation. |
| Brolucizumab-Associated Retinal Vasculitis | Hypotheses include severely reduced vascular perfusion and local production of anti-brolucizumab antibodies. Vasculitis affects retinal arteries. |
| Infectious endophthalmitis | Infection affects internal eye structures, causing inflammation and tissue destruction. |
| Toxicity | Clinical Manifestation |
|---|---|
| Hypertension | Headaches, dizziness, visual disturbances, epistaxis, fatigue, shortness of breath. |
| Proteinuria | Peripheral edema, foamy or frothy urine, hypertension. |
| Thromboembolic events | Leg swelling and pain, shortness of breath, chest discomfort, coughing up blood. |
| Cardiac toxicity | Asthenia, fatigue, shortness of breath, fluid retention, peripheral edema, hepatomegaly, QT prolongation. |
| Hemorrhage | Diverse clinical presentation ranging from epistaxis to severe gastrointestinal bleeding. Intracranial hemorrhage is more severe. |
| Bowel/Nasal perforation | Acute abdominal pain, peritonitis, fever, nausea, vomiting, constipation or diarrhea. Nasal symptoms like epistaxis and difficulty breathing. |
| Skin toxicity | Hand–foot syndrome, rash, mucositis, pruritus, alopecia, subungual hemorrhage. |
| Reversible Posterior Leukoencephalo-pathy | Severe headache, nausea, confusion, cortical blindness, seizures. |
| Infusion-related reactions | Allergic symptoms to anaphylactoid reactions, flushing, itching, hypertension, wheezing, chest pain. |
| Hypothyroidism | Nonspecific symptoms like fatigue, unexplained weight gain, sensitivity to cold, dry skin and hair, muscle aches, depression. |
| Asthenia and fatigue | Reduced energy levels, physical or mental weariness. |
| Gastrointestinal toxicity | Nausea, vomiting, heightened salivation, pallor, mucositis, diarrhea, anorexia. |
| Myelotoxicity | Anemia, neutropenia, lymphopenia, thrombocytopenia with respective symptoms. |
| Conjunctival hemorrhage | Visible red discoloration in the conjunctiva, irritation, sensation of a foreign body in the eye. |
| Vitreous floaters | Perceived specks, dots, or cobweb-like shapes in the visual field, can cause visual disturbances. |
| Rhegmatogenous retinal detachments | Sudden onset marked by flashes of light, appearance of new or increased floaters, visual impairment. |
| Retinal hemorrhage | Blood within the retina, sudden changes in vision, pain or discomfort. |
| Ocular hypertension | Endures without discernible discomfort, routine eye examinations are imperative. |
| Intraocular inflammation | Pseudoendophthalmitis, acute-onset inflammation without infection, blurred vision, floaters, pain, photophobia. |
| Brolucizumab-Associated Retinal Vasculitis | Clinical evidence of inflammation without infectious endophthalmitis, worse visual acuity than baseline. |
| Infectious endophthalmitis | Decreased vision, severe pain, conjunctival injection, anterior chamber cell with hypopyon, vitritis. |
| Toxicity | Assessment and Monitoring Methods |
|---|---|
| Hypertension | Regular blood pressure assessments before and after VEGFi treatment. Patient education on self-monitoring at home. |
| Proteinuria | Comprehensive urinalysis test with eventual 24 h urine collection for protein evaluation. |
| Thromboembolic events | Patient education on recognizing signs and symptoms. Imaging techniques (ultrasound, CT) for diagnosis. |
| Cardiac toxicity | Periodic monitoring of QT interval. Echocardiography and routine ECG for cardiac function assessment. |
| Hemorrhage | Regular clinical assessments for bleeding signs. Hematological tests for platelet counts and coagulation parameters. |
| Bowel/Nasal septum perforation | Vigilant clinical monitoring for early detection of signs and symptoms. |
| Skin toxicity | Periodic clinical inspection for early signs of cutaneous toxicity. |
| Reversible Posterior Leu-koencephalo-pathy | Diagnostic tests include brain imaging (MRI) and blood pressure monitoring. |
| Infusion-related hypersensitivity reactions | Close clinical observation during and after drug infusion. |
| Hypothyroidism | Regular monitoring of blood biochemistry, including thyroid function. |
| Asthenia and fatigue | Systematic clinical examinations and specific questionnaires. Blood tests to rule out physiological causes. |
| Gastrointestinal toxicity | Diagnosis through clinical examination and anamnestic collection. Electrolyte tests for assessing vomiting and diarrhea. |
| Anorexia | Clinical assessment, BMI measurement, and blood tests for nutritional parameters. Consideration of psychological criteria. |
| Myelotoxicity | Combination of clinical evaluation and laboratory tests. |
| Conjunctival hemorrhage | Diagnosis based on clinical presentation with subconjunctival bleeding. |
| Vitreous floaters | Visualization techniques (fundus examination, OCT, ultrasound) for assessment. |
| Rhegmatogenous retinal detachments | Imaging modalities (ultrasound, OCT) for diagnosis of retinal detachments. |
| Retinal hemorrhage | Fundus examination, OCT, or fluorescein angiography for visualization. |
| Ocular hypertension | Tonometry (GAT, non-contact, rebound) for IOP evaluation. Visual field evaluation with Goldmann or automated perimetry. |
| Intraocular inflammation | Laboratory tests (CBC, ESR, CRP) for systemic inflammation. Instrumental tests (slit-lamp, fundus photography, OCT). |
| Brolucizumab-Associated Retinal Vasculitis | Fundus examination and obtaining serum and vitreous cultures. Rule out infectious endophthalmitis. |
| Infectious endophthalmitis | Needle-based vitreous sampling for microbiologic analysis. Inflammatory markers (ESR, CRP) and ocular imaging. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santorsola, M.; Capuozzo, M.; Nasti, G.; Sabbatino, F.; Di Mauro, A.; Di Mauro, G.; Vanni, G.; Maiolino, P.; Correra, M.; Granata, V.; et al. Exploring the Spectrum of VEGF Inhibitors’ Toxicities from Systemic to Intra-Vitreal Usage in Medical Practice. Cancers 2024, 16, 350. https://doi.org/10.3390/cancers16020350
Santorsola M, Capuozzo M, Nasti G, Sabbatino F, Di Mauro A, Di Mauro G, Vanni G, Maiolino P, Correra M, Granata V, et al. Exploring the Spectrum of VEGF Inhibitors’ Toxicities from Systemic to Intra-Vitreal Usage in Medical Practice. Cancers. 2024; 16(2):350. https://doi.org/10.3390/cancers16020350
Chicago/Turabian StyleSantorsola, Mariachiara, Maurizio Capuozzo, Guglielmo Nasti, Francesco Sabbatino, Annabella Di Mauro, Giordana Di Mauro, Gianluca Vanni, Piera Maiolino, Marco Correra, Vincenza Granata, and et al. 2024. "Exploring the Spectrum of VEGF Inhibitors’ Toxicities from Systemic to Intra-Vitreal Usage in Medical Practice" Cancers 16, no. 2: 350. https://doi.org/10.3390/cancers16020350
APA StyleSantorsola, M., Capuozzo, M., Nasti, G., Sabbatino, F., Di Mauro, A., Di Mauro, G., Vanni, G., Maiolino, P., Correra, M., Granata, V., Gualillo, O., Berretta, M., & Ottaiano, A. (2024). Exploring the Spectrum of VEGF Inhibitors’ Toxicities from Systemic to Intra-Vitreal Usage in Medical Practice. Cancers, 16(2), 350. https://doi.org/10.3390/cancers16020350