

Impact of Dose-Escalated Chemoradiation on Pathological Complete Response in Patients with Locally Advanced Rectal Cancer

 , ,
, ,
Abstract
Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Sample Population
2.2. Treatment Protocol
2.2.1. Neoadjuvant Chemotherapy
2.2.2. Radiotherapy
2.2.3. Planned Surgery
2.2.4. Adjuvant Chemotherapy
2.2.5. Response
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Patients
3.2. Surgery
3.3. Pathological Response and Downstaging
3.4. Acute and Chronic Toxicity
3.5. Univariable and Multivariate Analyses
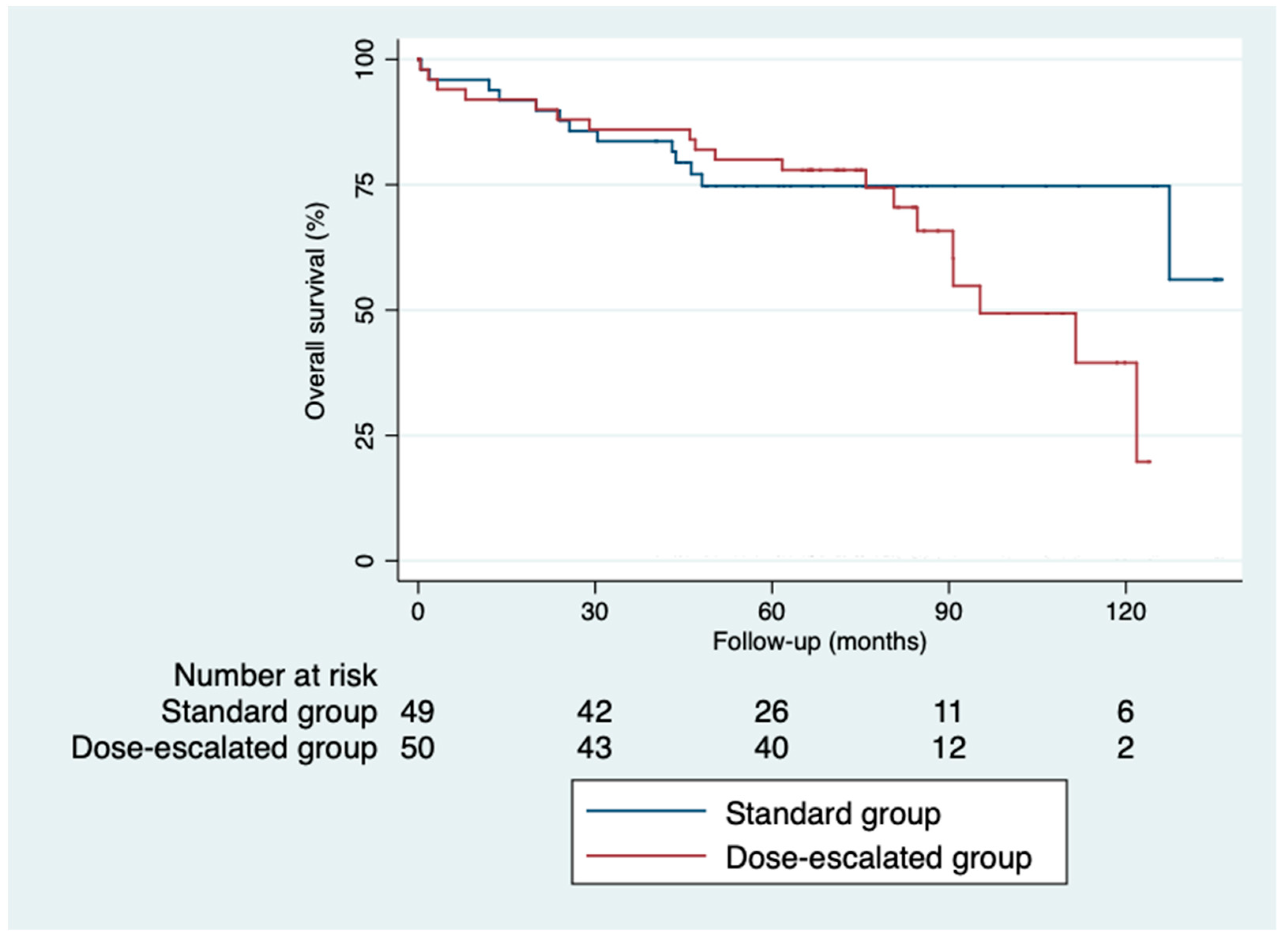
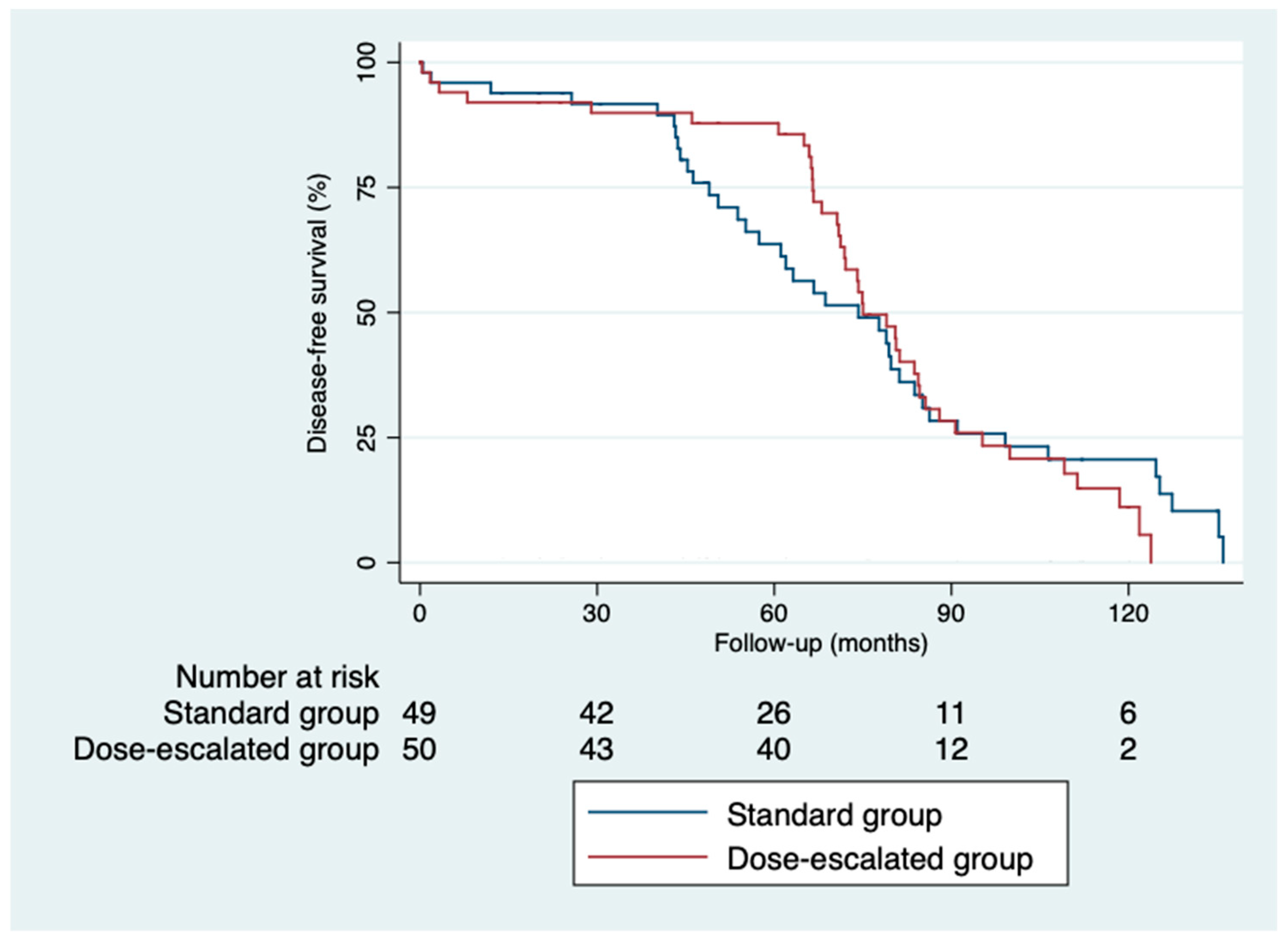
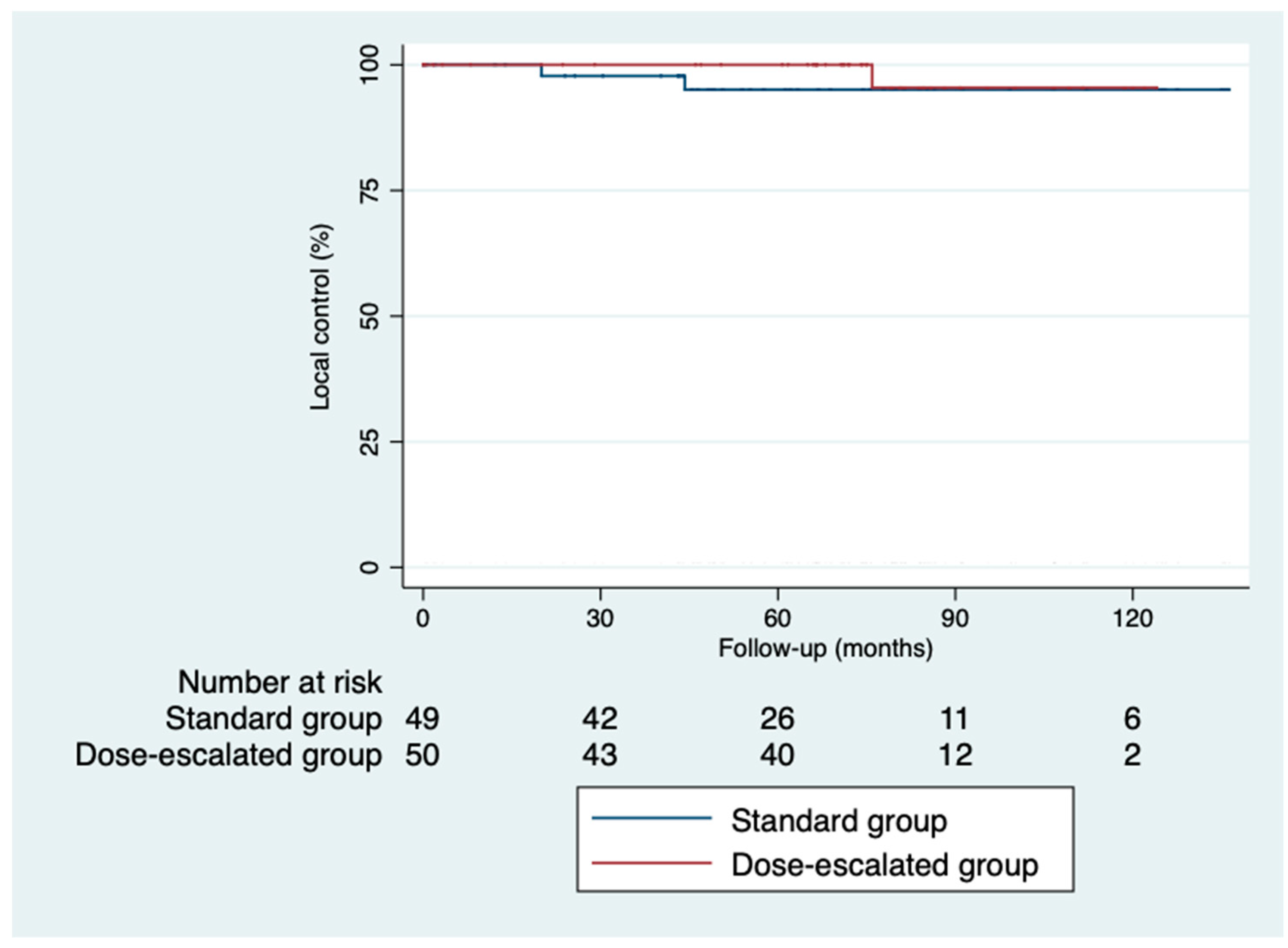
3.6. Control and Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sociedad Española de Oncología Médica. Available online: https://seom.org/images/publicaciones/informes-seom-de-evaluacion-de-farmacos/LAS_CIFRAS_2024.pdf (accessed on 8 April 2024).
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Barzi, A.; Jemal, A. Colorectal cancer statistics. Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Bown, E.J.; Lloyd, G.M.; Boyle, K.M.; Miller, A.S. Rectal cancer: Prognostic indicators of long-term outcome in patients considered for surgery. Int. J. Colorectal Dis. 2014, 29, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Compton, C.C.; Fielding, L.P.; Burgart, L.J.; Conley, B.; Cooper, H.S.; Hamilton, S.R.; Hammond, M.E.H.; Henson, D.E.; Hutter, R.V.P.; Nagle, R.B.; et al. Prognostic factors in colorectal cancer. Arch. Pathol. Lab. Med. 2000, 124, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Betge, J.; Pollheimer, M.J.; Lindtner, R.A.; Kornprat, P.; Schlemmer, A.; Rehak, P.; Vieth, M.; Hoefler, G.; Langner, C. Intramural and extramural vascular invasion in colorectal cancer. Cancer 2012, 118, 628–638. [Google Scholar] [CrossRef] [PubMed]
- Liebig, C.; Ayala, G.; Wilks, J.; Verstovsek, G.; Liu, H.; Agarwal, N.; Berger, D.H.; Albo, D. Perineural invasion is an independent predictor of outcome in colorectal cancer. J. Clin. Oncol. 2009, 27, 5131–5137. [Google Scholar] [CrossRef]
- Dukes, C.E.; Bussey, H.J.R. The spread of rectal cancer and its effect on prognosis. Br. J. Cancer 1958, 12, 309–320. [Google Scholar] [CrossRef]
- Blenkinsopp, W.K.; Stewart-Brown, S.; Blesovsky, L.; Kearney, G.; Fielding, L.P. Histopathology reporting in large bowel cancer. J. Clin. Pathol. 1981, 3, 509–513. [Google Scholar] [CrossRef]
- Revista Ciencia y Salud. Available online: http://revistacienciaysalud.ac.cr/ojs/index.php/cienciaysalud/article/view/25 (accessed on 23th November 2023).
- Van Cutsem, E.; Nordlinger, B.; Cervantes, A. Advanced colorectal cancer: ESMO Clinical Practice Guidelines for treatment. Ann. Oncol. 2010, 21, v93–v97. [Google Scholar] [CrossRef]
- Schmoll, H.J.; Van Cutsem, E.; Kakegawa, T. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann. Oncol. 2012, 23, 2479–2516. [Google Scholar] [CrossRef]
- Krook, J.E.; Moertel, C.G.; Gunderson, L.L.; Wieand, H.S.; Collins, R.T.; Beart, R.W.; Kubista, T.P.; Poon, M.A.; Meyers, W.C.; Mailliard, J.A. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N. Engl. J. Med. 1991, 324, 709–715. [Google Scholar] [CrossRef]
- Gastrointestinal Tumor Study Group. Radiation therapy and fluorouracil with or without semustine for the treatment of patients with surgical adjuvant adenocarcinoma of the rectum. J. Clin. Oncol. 1992, 10, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Hofheinz, R.; Wenz, F.K.; Post, S.; Matzdorff, A.; Laechelt, S.; Hartmann, J.T.; Müller, L.; Link, H.; Moehler, M.H. Capecitabine (Cape) versus 5-fluorouracil (5-FU)–based (neo)adjuvant chemoradiotherapy (CRT) for locally advanced rectal cancer (LARC): Long-term results of a randomized, phase III trial. J. Clin. Oncol. 2011, 29, 3504. [Google Scholar] [CrossRef]
- Swedish Rectal Cancer Group. Improved survival with preoperative radiotherapy in resectable rectal cancer. N. Engl. J. Med. 1997, 336, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Cammà, C.; Giunta, M.; Fiorica, F.; Pagliaro, L.; Craxì, A.; Cottone, M. Preoperative radiotherapy for resectable rectal cancera meta-analysis. JAMA 2000, 284, 1008–1015. [Google Scholar] [CrossRef]
- Colorectal Cancer Collaborative Group. Adjuvant radiotherapy for rectal cancer: A systematic overview of 8507 patients from 22 randomised trials. Lancet 2001, 358, 1291–1304. [Google Scholar] [CrossRef]
- Bosset, J.F.; Collette, L.; Calais, G.; Mineur, L.; Maingon, P.; Radosevic-Jelic, L.; Daban, A.; Bardet, E.; Beny, A.; Ollier, J.C. Chemotherapy with preoperative radiotherapy in rectal cancer. N. Engl. J. Med. 2006, 355, 1114–1123. [Google Scholar] [CrossRef]
- Saif, M.W.; Hashmi, S.; Zelterman, D.; Almhanna, K.; Kim, R. Capecitabine vs. continuous infusion 5-FU in neoadjuvant treatment of rectal cancer. A retrospective review. Int. J. Colorectal Dis. 2008, 23, 139–145. [Google Scholar] [CrossRef]
- Gérard, J.P.; Azria, D.; Gourgou-Bourgade, S.; Martel-Laffay, I.; Hennequin, C.; Ettienne, P.L.; Vendrely, V.; François, E.; de La Roche, G.; Bouché, O.; et al. Comparison of two neoadjuvant chemoradiotherapy regimens for locally advanced rectal cancer: Results of the Phase III Trial ACCORD 12/0405-prodige 2. J. Clin. Oncol. 2012, 28, 1638–1644. [Google Scholar] [CrossRef]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rödel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. Rectal cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef]
- Hong, Y.S.; Kim, S.Y.; Lee, J.S.; Nam, B.H.; Kim, K.P.; Kim, J.E.; Park, Y.S.; Park, J.O.; Baek, J.Y.; Kim, T.Y.; et al. Oxaliplatin-based adjuvant chemotherapy for rectal cancer after preoperative chemoradiotherapy (ADORE): Long-term results of a randomized controlled trial. J. Clin. Oncol. 2019, 37, 3111–3123. [Google Scholar] [CrossRef] [PubMed]
- Bahadoer, R.R.; Dijkstra, E.A.; van Etten, B.; Marijnen, C.A.M.; Putter, H.; Kranenbarg, E.M.K.; Roodvoets, A.G.H.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Blomqvist, L.K.; et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Ciseł, B.; Pietrzak, L.; Michalski, W.; Wyrwicz, L.; Rutkowski, A.; Kosakowska, E.; Cencelewicz, A.; Spałek, M.; Polkowski, W.; Jankiewicz, M.; et al. Long-course preoperative chemoradiation versus 5 × 5 Gy and consolidation chemotherapy for clinical T4 and fixed clinical T3 rectal cancer: Long-term results of the randomized Polish II study. Ann. Oncol. 2019, 30, 1298–1303. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Aguilar, J.; Smith, D.D.; Avila, K.; Bergsland, E.K.; Chu, P.; Krieg, R.M. Optimal timing of surgery after chemoradiation for advanced rectal cancer: Preliminary results of a multicenter, nonrandomized phase II prospective trial. Ann. Surg. 2011, 254, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Chi, P.; Lan, P.; Wang, L.; Chen, W.; Cui, L.; Chen, D.; Cao, J.; Wei, H.; Peng, X.; et al. Neoadjuvant modified FOLFOX6 with or without radiation versus fluorouracil plus radiation for locally advanced rectal cancer: Final results of the chinese FOWARC trial. J. Clin. Oncol. 2019, 37, 3223–3233. [Google Scholar] [CrossRef]
- Fernandez-Martos, C.; Garcia-Albeniz, X.; Pericay, C.; Maurel, J.; Aparicio, J.; Montagut, C.; Safont, M.J.; Salud, A.; Vera, R.; Massuti, B.; et al. Chemoradiation, surgery and adjuvant chemotherapy versus induction chemotherapy followed by chemoradiation and surgery: Long-term results of the Spanish GCR-3 phase II randomized trial. Ann. Oncol. 2015, 26, 1722–1728. [Google Scholar] [CrossRef]
- Petrelli, F.; Trevisan, F.; Cabiddu, M.; Sgroi, G.; Bruschieri, L.; Rausa, E.; Ghidini, M.; Turati, L. Total neoadjuvant therapy in rectal cancer: A systematic review and meta-analysis of treatment outcomes. Ann. Surg. 2020, 271, 440–448. [Google Scholar] [CrossRef]
- Vecchio, F.M.; Valentini, V.; Minsky, B.D.; Padula, G.D.A.; Venkatraman, E.S.; Balducci, M.; Miccichè, F.; Ricci, R.; Morganti, A.G.; Gambacorta, M.A.; et al. The relationship of pathologic tumor regression grade (TRG) and outcomes after preoperative therapy in rectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 752–760. [Google Scholar] [CrossRef]
- Habr-Gama, A.; Perez, R.O.; Nadalin, W.; Sabbaga, J.; Ribeiro, U.; Silva e Sousa, A.H.; Campos, F.G.; Kiss, D.R.; Gama-Rodrigues, J. Operative versus nonoperative treatment for stage 0 distal rectal cancer following chemoradiation therapy: Long-term results. Ann. Surg. 2004, 240, 711–718. [Google Scholar] [CrossRef]
- Garcia-Aguilar, J.; Patil, S. Organ preservation in patients with rectal adenocarcinoma treated with total neoadjuvant therapy. J. Clin. Oncol. 2022, 40, 2546–2556. [Google Scholar] [CrossRef]
- Greene, F.L. American Joint Committee on Cancer Staging Manual, 6th ed.; Springer: New York, NY, USA, 2002; p. 421. [Google Scholar]
- Nijkamp, J.; de Jong, R.; Sonke, J.J.; van Vliet, C.; Marijnen, C. Target volume shape variation during irradiation of rectal cancer patients in supine position: Comparison with prone position. Radiother. Oncol. 2009, 93, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.D.; Nijkamp, J.; Duppen, J.C.; Rasch, C.R.N.; Thomas, C.R.; Wang, S.J.; Okunieff, P.; Jones, W.E.; Baseman, D.; Patel, S.; et al. Prospective randomized double-blind pilot study of site-specific consensus atlas implementation for rectal cancer target volume delineation in the cooperative group setting. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.; Gibbons, D.; Hyland, J.M.P.; Treanor, D.; White, A.; Mulcahy, H.E.; O’Donoghue, D.P.; Moriarty, M.; Fennelly, D.; Sheahan, K. Pathological response following long-course neoadjuvant chemoradiotherapy for locally advanced rectal cancer. Histopathology 2005, 47, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Burbach, J.P.M.; den Harder, A.M.; Intven, M.; van Vulpen, M.; Verkooijen, H.M.; Reerink, O. Impact of radiotherapy boost on pathological complete response in patients with locally advanced rectal cancer: A systematic review and meta-analysis. Radiother. Oncol. 2014, 113, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hearn, N.; Atwell, D.; Intven, M.; van Vulpen, M.; Verkooijen, H.M.; Reerink, O. Neoadjuvant radiotherapy dose escalation in locally advanced rectal cancer: A systematic review and meta-analysis of modern treatment approaches and outcomes. Clin. Oncol. 2021, 33, e1–e14. [Google Scholar] [CrossRef]
- Garcia-Aguilar, J.; Hernandez De Anda, E.; Sirivongs, P.; Lee, S.H.; Madoff, R.D.; Rothenberger, D.A. A pathologic complete response to preoperative chemoradiation is associated with lower local recurrence and improved survival in rectal cancer patients treated by mesorectal excision. Dis. Colon. Rectum 2003, 46, 298–304. [Google Scholar] [CrossRef]
- Capirci, C.; Valentini, V.; Cionini, L.; De Paoli, A.; Rodel, C.; Glynne-Jones, R.; Coco, C.; Romano, M.; Mantello, G.; Palazzi, S.; et al. Prognostic value of pathologic complete response after neoadjuvant therapy in locally advanced rectal cancer: Long-term analysis of 566 ypCR patients. Int. J. Radiat. Oncol. 2008, 72, 99–107. [Google Scholar] [CrossRef]
- Valentini, V.; Minsky, B.D. Tumor regression grading in rectal cancer: Is it time to move forward? JCO 2014, 15, 1534–1536. [Google Scholar] [CrossRef]
- Martin, S.T.; Heneghan, H.M.; Winter, D.C. Systematic review and meta-analysis of outcomes following pathological complete response to neoadjuvant chemoradiotherapy for rectal cancer. Br. J. Surg. 2012, 99, 918–928. [Google Scholar] [CrossRef]
- Valentini, V.; Gambacorta, M.A.; Cellini, F.; Aristei, C.; Coco, C.; Barbaro, B.; Alfieri, S.; D’Ugo, D.; Persiani, R.; Deodato, F.; et al. The INTERACT Trial: Long-term results of a randomised trial on preoperative capecitabine-based radiochemotherapy intensified by concomitant boost or oxaliplatin, for cT2 (distal)–cT3 rectal cancer. Radiother. Oncol. 2019, 134, 110–118. [Google Scholar] [CrossRef]
- Janjan, N.A.; Crane, C.N.; Feig, B.W.; Cleary, K.; Dubrow, R.; Curley, S.A.; Ellis, L.M.; Vautney, J.N.; Lenzi, R.; Lynch, P.; et al. Prospective trial of preoperative concomitant boost radiotherapy with continuous infusion 5-fluorouracil for locally advanced rectal cancer. Int. J. Radiat. Oncol. 2000, 47, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Hernando-Requejo, O.; López, M.; Cubillo, A.; Rodriguez, A.; Ciervide, R.; Valero, J.; Sánchez, E.; Garcia-Aranda, M.; Rodriguez, J.; Potdevin, G.; et al. Complete pathological responses in locally advanced rectal cancer after preoperative IMRT and integrated-boost chemoradiation. Strahlenther. Onkol. 2014, 190, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Li, J.L.; Ji, J.F.; Cai, Y.; Li, X.F.; Li, Y.H.; Wu, H.; Xu, B.; Dou, F.; Li, Z.; Bu, Z.; et al. Preoperative concomitant boost intensity-modulated radiotherapy with oral capecitabine in locally advanced mid-low rectal cancer: A phase II trial. Radiother. Oncol. 2012, 102, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Lupattelli, M.; Palazzari, E.; Polesel, J.; Chiloiro, G.; Angelicone, I.; Panni, V.; Caravatta, L.; Di Biase, S.; Macchia, G.; Niespolo, R.M.; et al. Preoperative Intensified Chemoradiation with Intensity-Modulated Radiotherapy and Simultaneous Integrated Boost Combined with Capecitabine in Locally Advanced Rectal Cancer: Long-Term Outcomes of a Real-Life Multicenter Study. Cancers 2023, 15, 5702. [Google Scholar] [CrossRef]
- Zhang, Q.; Liang, J.; Chen, J.; Mei, S.; Wang, Z. Predictive Factors for Pathologic Complete Response Following Neoadjuvant Chemoradiotherapy for Rectal Cancer. Asian Pac. J. Cancer Prev. 2021, 22, 1607–1611. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Standard Arm N = 49 | Dose-Escalated Arm N = 50 | p-Value | |
|---|---|---|---|
| Age (years) ≥65 y <65 y | Median = 66.7 (41.1–89.6) 29 (40.82%) 20 (59.18%) | Median = 66.2 (40.9–86.7) 26 (48%) 24 (52%) | 0.36 0.47 |
| Gender (female/male) | F = 20 (40.82%) M = 29 (59.18%) | F = 16 (32%) M = 34 (68%) | 0.36 |
| Tumor distance from internal anal margin (mm) | Mean = 53.88 0–50 = 13 (26.53%) 51–100 = 24 (48.98%) ≥ 101 = 12 (24.49%) | Mean = 58.6 0–50 = 12 (24%) 51–100 = 25 (50%) ≥ 101 = 13 (26%) | 0.53 0.96 |
| cTNM stage | IIA = 6 (12.77%) IIB = 2 (4.26%) IIIA = 4 (8.51%) IIIB = 14 (29.79%) IIIC = 21 (44.68%) | IIA = 5 (10%) IIB = 3 (6%) IIIA = 10 (20%) IIIB = 7 (14%) IIIC = 25 (50%) | 0.24 |
| Histological grade Grade 1 Grade 2 Grade 3 | 39 (81.25%) 7 (14.58%) 2 (4.17%) | 37 (75.51%) 10 (20.41%) 2 (4.08%) | 0.84 |
| Pretreatment CEA 1 ≥ 5 ng/mL (yes/no) | Yes = 23 (52.27%) No = 21 (47.73%) | Yes = 21 (42%) No = 29 (58%) | 0.32 |
| Pretreatment mesorectal fascia invasion (yes/no) | Yes = 34 (69.39%) No = 15 (30.61%) | Yes = 30 (61.22%) No = 19 (38.78%) | 0.40 |
| Complications | Standard Arm N = 49 | Dose-Escalated Arm N = 50 | p-Value |
|---|---|---|---|
| None | 26 (53.06%) | 23 (46%) | 0.48 |
| Wound | 1 (2.04%) | 3 (6%) | 0.62 |
| Abdominal | 7 (14.29%) | 9 (18%) | 0.62 |
| Urinary tract | 3 (6.12%) | 1 (2%) | 0.36 |
| Anastomosis: Leak Fistula Ischemia | 4 (8.16%) 1 (2.04%) - | 10 (20%) - 1 (2%) | 0.09 |
| Stoma | 1 (2.04%) | 2 (2%) | 1.00 |
| Cardiovascular | 4 (8.16%) | 1 (2%) | 0.20 |
| Others | 3 (6.12%) | - | - |
| Clavien–Dindo classification Grade I Grade II Grade IIIa Grade IIIb Grade IVa Grade IVb Grade V | 7 (30.43%) 4 (17.39%) 4 (17.39%) 5 (21.74%) 1 (4.35%) - 2 (8.70%) | 7 (25.93%) 1 (3.70%) 9 (33.33%) 8 (29.63%) - 1 (3.70%) 1 (3.70%) | 0.39 |
| Standard Arm N = 49 | Dose-Escalated Arm N = 50 | p-Value | |
|---|---|---|---|
| Completion of treatment Radiotherapy Chemotherapy | 45 Gy: 24 (48.98%) 50 Gy: 10 (20.41%) 50.4 Gy: 13 (26.53%) Interruptions: (43.2 Gy): 2 (4.08%) Interruptions: 4 (8.16%) | 53.5 Gy: 6 (12%) 54.25 Gy: 41 (82%) 60.76 Gy: 1 (2%) Interruptions: (43.4 Gy): 2 (4%) Interruptions: 5 (10%) | 0.51 |
| Surgery Time interval (weeks) from chemoradiation to surgery | Saving-sphincter: 33 (67.35%) Definitive stoma: 15 (30.61%) Hartmann: 1 (2.04%) <8 weeks: 11 (22.45%) ≥8 to <9 weeks: 7 (14.29%) ≥9 to <10 weeks: 14 (28.57%) ≥10 weeks: 17 (34.69%) | Saving-sphincter: 33 (67.35%) Definitive stoma: 15 (30.61%) Hartmann: 1 (2.04%) Hemicolectomy: 1 (2%) <8 weeks: 8 (16%) ≥8 to <9 weeks: 9 (18%) ≥9 to <10 weeks: 15 (30%) ≥10 weeks: 18 (36%) | 1.00 0.85 |
| CAP 1 | ypCR = CAP 0: 5 (10.64%) CAP 1: 16 (34.04%) CAP 2: 13 (27.66%) CAP 3: 13 (27.66%) Unknown: 2 | ypCR = CAP 0: 11 (25%) CAP 1: 16 (36.36%) CAP 2: 13 (29.55%) CAP 3: 4 (9.09%) Unknown: 6 | 0.07 |
| CAP 1-grouped (responders vs. non-responders) | CAP 0 + 1: 21 (44.68%) CAP 2 + 3: 26 (55.32%) | CAP 0 + 1: 27 (61.36%) CAP 2 + 3: 17 (38.64%) | 0.11 |
| Downstaging | Yes: 40 (81.63%) No: 9 (18.37%) | Yes: 44 (88%) No: 6 (12%) | 0.38 |
| p-Value | Odds Ratio | IC 95% Inferior | IC 95% Superior | |
|---|---|---|---|---|
| Age (years) | 0.79 | 1.00 | 0.96 | 1.06 |
| Gender (male vs. female) | 0.64 | 1.27 | 0.40 | 4.00 |
| Tumor location: | 0.82 | |||
| Middle vs. inferior | 0.87 | 0.90 | 0.24 | 3.41 |
| Superior vs. inferior | 0.71 | 1.31 | 0.31 | 5.60 |
| cT3 vs. cT2 | 0.01 | |||
| cT3 vs. cT2 | 0.01 | 0.16 | 0.04 | 0.66 |
| cT4 vs. cT2 | 0.78 | 0.83 | 0.23 | 3.07 |
| cN stage: | 0.46 | |||
| cN1 vs. cN0 | 0.39 | 2.07 | 0.39 | 11.11 |
| cN2 vs. cN0 | 0.96 | 1.05 | 0.19 | 5.82 |
| cTNM (reference: stage 0) | 0.67 | |||
| IIB | 0.55 | 2.5 | 0.12 | 50.44 |
| IIIA | 0.25 | 4 | 0.38 | 42.37 |
| IIIB | 0.47 | 2.35 | 0.23 | 24.09 |
| IIIC | 0.72 | 1.5 | 0.16 | 13.92 |
| Histologic grade: | ||||
| Grade 2 vs. grade 1 | 0.96 | 1.04 | 0.26 | 4.14 |
| Pretreatment CEA 1 ≥ 5 ng/mL (yes vs. no) | ||||
| 0.25 | 0.51 | 0.16 | 1.64 | |
| Pretreatment mesorectal fascia invasion (yes vs. no) | ||||
| 0.36 | 1.73 | 0.51 | 5.85 | |
| Weeks from chemoradiation to surgery (reference: <8) | 0.78 | |||
| ≥8 to <9 | 0.86 | 1.21 | 0.15 | 9.76 |
| ≥9 to <10 | 0.34 | 2.32 | 0.41 | 12.96 |
| ≥10 | 0.52 | 1.76 | 0.32 | 9.71 |
| Dose of RT: | ||||
| >50.4 Gy | 0.11 | 2.48 | 0.79 | 7.77 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domingo-Boluda, C.; Dualde, D.; Taberner-Bonastre, T.; Soler, M.; López-Campos, F. Impact of Dose-Escalated Chemoradiation on Pathological Complete Response in Patients with Locally Advanced Rectal Cancer. Cancers 2024, 16, 3170. https://doi.org/10.3390/cancers16183170
Domingo-Boluda C, Dualde D, Taberner-Bonastre T, Soler M, López-Campos F. Impact of Dose-Escalated Chemoradiation on Pathological Complete Response in Patients with Locally Advanced Rectal Cancer. Cancers. 2024; 16(18):3170. https://doi.org/10.3390/cancers16183170
Chicago/Turabian StyleDomingo-Boluda, Carolina, Diego Dualde, Teresa Taberner-Bonastre, Miguel Soler, and Fernando López-Campos. 2024. "Impact of Dose-Escalated Chemoradiation on Pathological Complete Response in Patients with Locally Advanced Rectal Cancer" Cancers 16, no. 18: 3170. https://doi.org/10.3390/cancers16183170
APA StyleDomingo-Boluda, C., Dualde, D., Taberner-Bonastre, T., Soler, M., & López-Campos, F. (2024). Impact of Dose-Escalated Chemoradiation on Pathological Complete Response in Patients with Locally Advanced Rectal Cancer. Cancers, 16(18), 3170. https://doi.org/10.3390/cancers16183170