



MRI T2w Radiomics-Based Machine Learning Models in Imaging Simulated Biopsy Add Diagnostic Value to PI-RADS in Predicting Prostate Cancer: A Retrospective Diagnostic Study


Abstract
Simple Summary
Abstract
1. Introduction
2. Method
2.1. Patients and Data Collection
2.2. PI-RADS
2.3. Segmentation and Feature Extraction
2.3.1. ROI Segmentation
2.3.2. Pyradiomics
2.3.3. Feature Extraction
2.4. Model Construction
2.4.1. Data Undersampling
2.4.2. Feature Selection
2.4.3. Predictive Models and Control Models
2.5. Statistical Analysis
3. Results
3.1. Patients
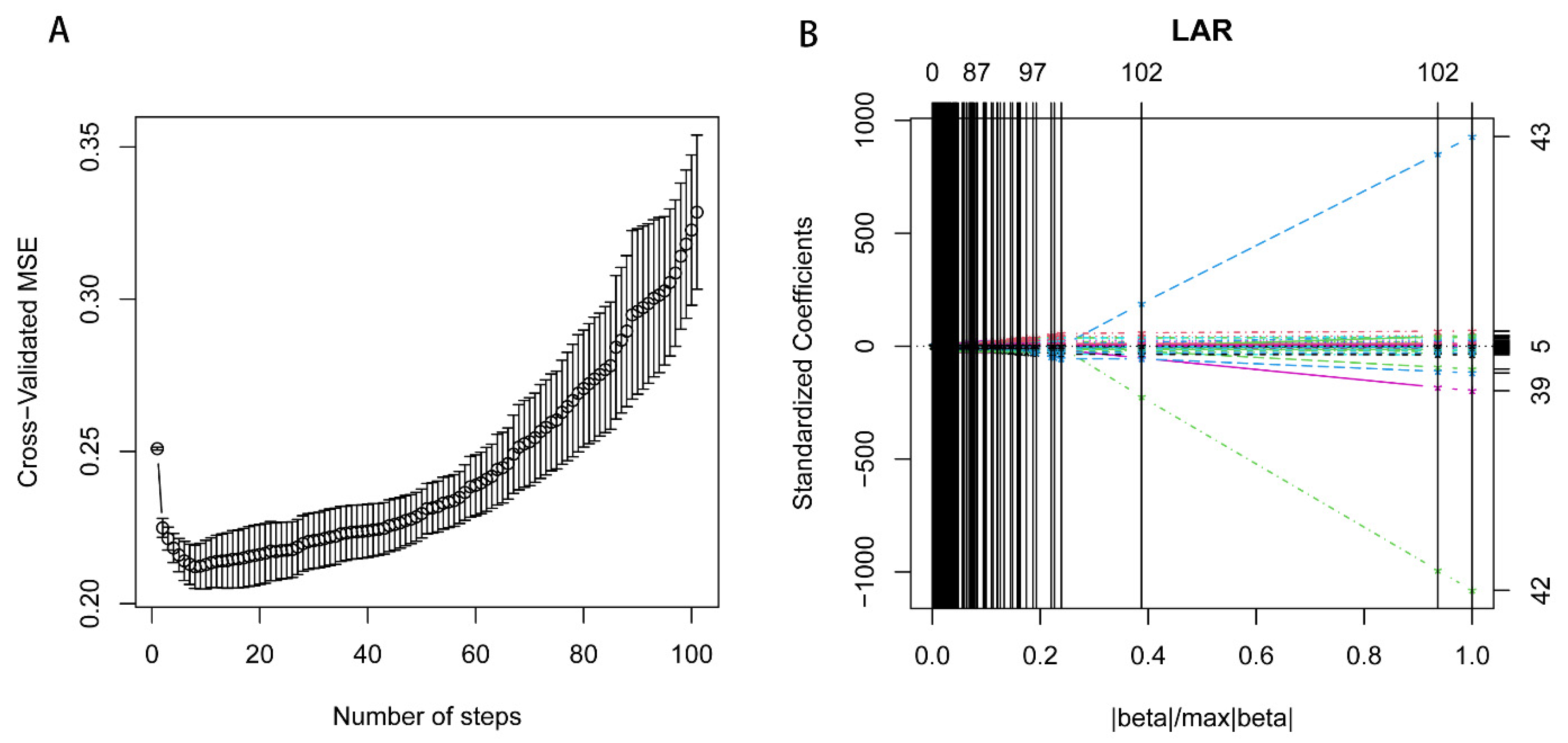
3.2. Feature Screening
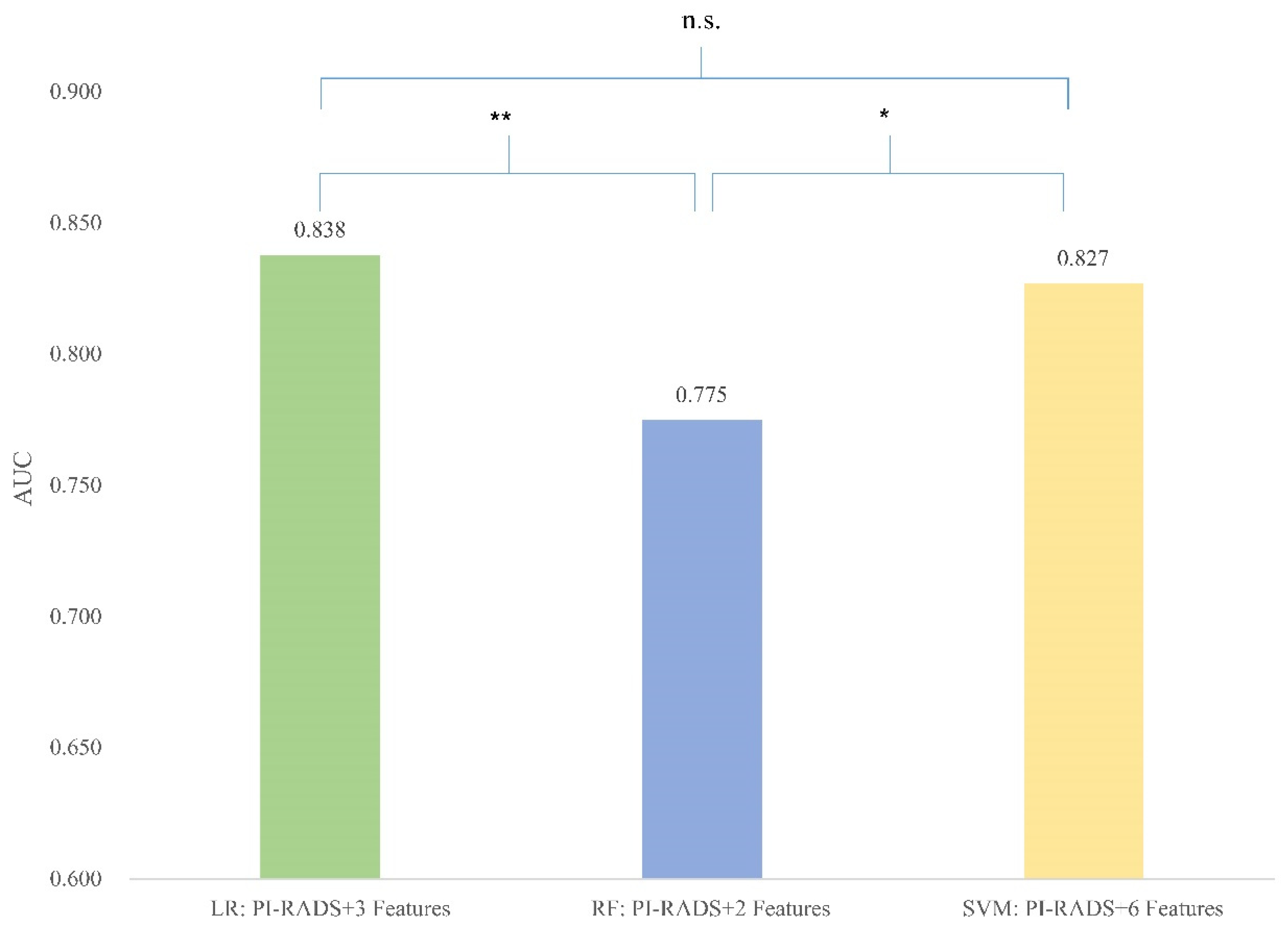
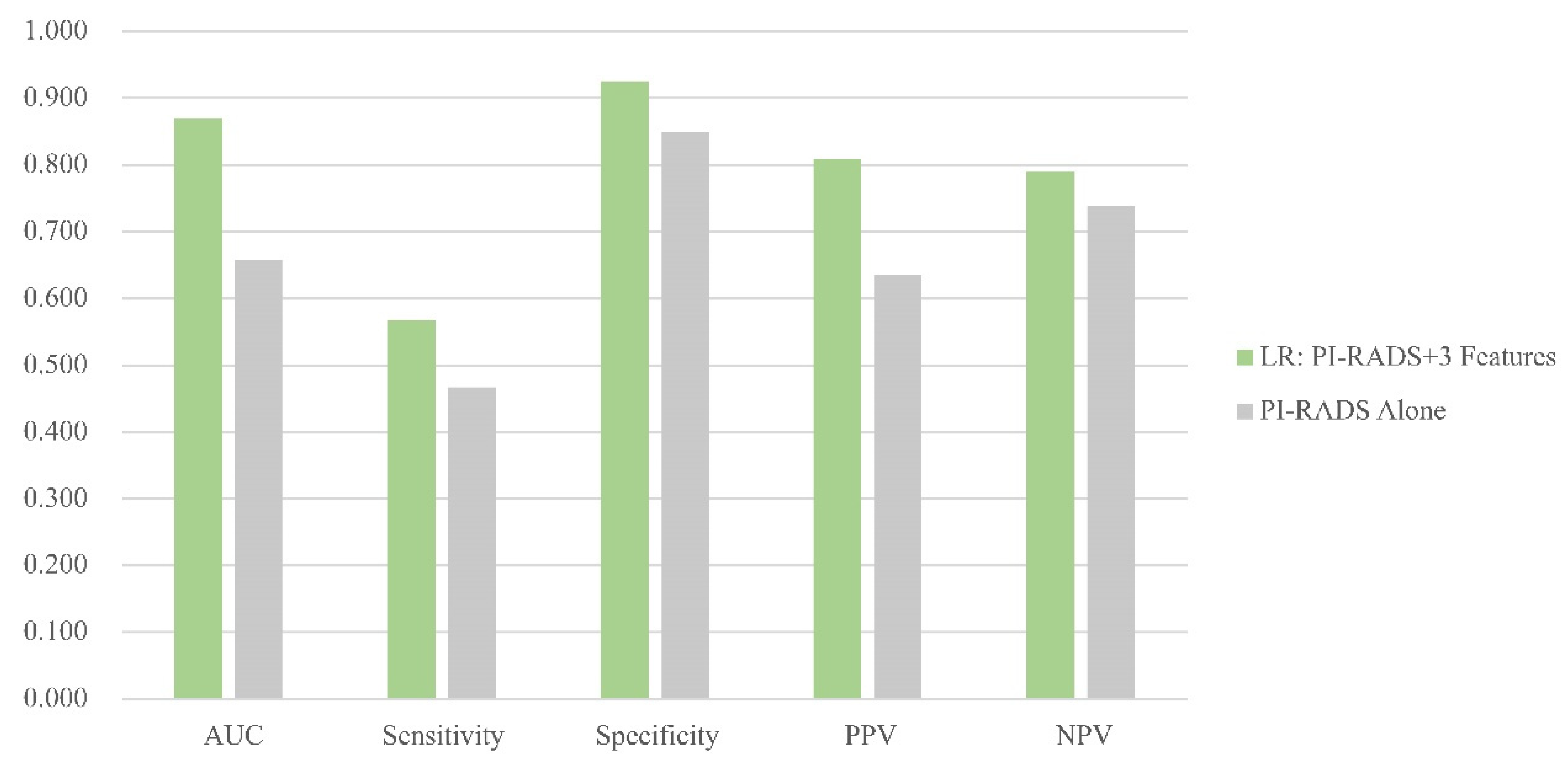
3.3. Model Performance
TCIA Dataset
3.4. HQM Validation Dataset
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F.; Bsc, M.F.B.; Me, J.F.; Soerjomataram, M.I.; et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Chen, W.; Zheng, R.; Baade, P.D.; Zhang, S.; Zeng, H.; Bray, F.; Jemal, A.; Yu, X.Q.; He, J. Cancer statistics in China, 2015. CA Cancer J. Clin. 2016, 66, 115–132. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Chen, H.-D.; Yu, Y.-W.; Li, N.; Chen, W.-Q. Changing profiles of cancer burden worldwide and in China: A secondary anal-ysis of the global cancer statistics 2020. Chin. Med. J. 2021, 134, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Fanti, S.; Minozzi, S.; Antoch, G.; Banks, I.; Briganti, A.; Carrio, I.; Chiti, A.; Clarke, N.; Eiber, M.; De Bono, J.; et al. Consensus on molecular imaging and theranostics in prostate cancer. Lancet Oncol. 2018, 19, e696–e708. [Google Scholar] [CrossRef] [PubMed]
- US Preventive Services Task Force; Grossman, D.C.; Curry, S.J.; Owens, D.K.; Bibbins-Domingo, K.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Ebell, M.; Epling, J.W., Jr.; et al. Screening for Prostate Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 319, 1901–1913. [Google Scholar]
- Schaeffer, E.M.; Srinivas, S.; Adra, N.; An, Y.; Barocas, D.; Bitting, R.; Bryce, A.; Chapin, B.; Cheng, H.H.; D’Amico, A.V.; et al. NCCN Guidelines® Insights: Prostate Cancer, Version 1. 2023. J. Natl. Compr. Canc. Netw. 2022, 20, 1288–1298. [Google Scholar]
- Zhao, L.-T.; Liu, Z.-Y.; Xie, W.-F.; Shao, L.-Z.; Lu, J.; Tian, J.; Liu, J.-G. What benefit can be obtained from magnetic resonance imaging diagnosis with artificial intelligence in prostate cancer compared with clinical assessments? Mil. Med. Res. 2023, 10, 29. [Google Scholar] [CrossRef]
- Ahdoot, M.; Wilbur, A.R.; Reese, S.E.; Lebastchi, A.H.; Mehralivand, S.; Gomella, P.T.; Bloom, J.; Gurram, S.; Siddiqui, M.; Pinsky, P.; et al. MRI-Targeted, Systematic, and Combined Biopsy for Prostate Cancer Diagnosis. N. Engl. J. Med. 2020, 382, 917–928. [Google Scholar] [CrossRef] [PubMed]
- Ahdoot, M.; Lebastchi, A.H.; Long, L.; Wilbur, A.R.; Gomella, P.T.; Mehralivand, S.; Daneshvar, M.A.; Yerram, N.K.; O’connor, L.P.; Wang, A.Z.; et al. Using Prostate Imaging-Reporting and Data System (PI-RADS) Scores to Select an Optimal Prostate Biopsy Method: A Secondary Analysis of the Trio Study. Eur. Urol. Oncol. 2022, 5, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Youn, S.Y.; Choi, M.H.; Kim, D.H.; Lee, Y.J.; Huisman, H.; Johnson, E.; Penzkofer, T.; Shabunin, I.; Winkel, D.J.; Xing, P.; et al. Detection and PI-RADS classification of focal lesions in prostate MRI: Performance comparison between a deep learning-based algorithm (DLA) and radiologists with various levels of experience. Eur. J. Radiol. 2021, 142, 109894. [Google Scholar] [CrossRef]
- Turkbey, B.; Purysko, A.S. PI-RADS: Where Next? Radiology 2023, 307, 223128. [Google Scholar] [CrossRef] [PubMed]
- Bektas, C.T.; Kocak, B.; Yardimci, A.H.; Turkcanoglu, M.H.; Yucetas, U.; Koca, S.B.; Erdim, C.; Kilickesmez, O. Clear Cell Renal Cell Carcinoma: Machine Learning-Based Quantitative Computed Tomography Texture Analysis for Prediction of Fuhrman Nuclear Grade. Eur. Radiol. 2019, 29, 1153–1163. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, M.; Nallabasannagari, A.R.; Reddiboina, M.; Porter, J.R.; Jeong, W.; Mottrie, A.; Dasgupta, P.; Challacombe, B.; Abaza, R.; Rha, K.H.; et al. Predicting intra-operative and postoperative consequential events using machine-learning techniques in patients undergoing robot-assisted partial nephrectomy: A Vattikuti Collective Quality Initiative database study. BJU Int. 2020, 126, 350–358. [Google Scholar] [CrossRef]
- Bonekamp, D.; Kohl, S.; Wiesenfarth, M.; Schelb, P.; Radtke, J.P.; Götz, M.; Kickingereder, P.; Yaqubi, K.; Hitthaler, B.; Gählert, N.; et al. Radiomic Machine Learning for Characterization of Prostate Lesions with MRI: Comparison to ADC Values. Radiology 2018, 289, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Anari, P.Y.; Lay, N.; Gopal, N.; Chaurasia, A.; Samimi, S.; Harmon, S.; Firouzabadi, F.D.; Merino, M.J.; Wakim, P.; Turkbey, E.; et al. An MRI-based radiomics model to predict clear cell renal cell carcinoma growth rate classes in patients with von Hippel-Lindau syndrome. Abdom. Imaging 2022, 47, 3554–3562. [Google Scholar] [CrossRef]
- Ogbonnaya, C.N.; Zhang, X.; Alsaedi, B.S.O.; Pratt, N.; Zhang, Y.; Johnston, L.; Nabi, G. Prediction of Clinically Significant Cancer Using Radiomics Features of Pre-Biopsy of Multiparametric MRI in Men Suspected of Prostate Cancer. Cancers 2021, 13, 6199. [Google Scholar] [CrossRef]
- Bleker, J.; Kwee, T.C.; Rouw, D.; Roest, C.; Borstlap, J.; de Jong, I.J.; Dierckx, R.A.J.O.; Huisman, H.; Yakar, D. A deep learning masked segmentation alternative to manual segmentation in biparametric MRI prostate cancer radiomics. Eur. Radiol. 2022, 32, 6526–6535. [Google Scholar] [CrossRef]
- Szczypiński, P.M.; Strzelecki, M.; Materka, A.; Klepaczko, A. MaZda – The Software Package for Textural Analysis of Biomedical Images. In Computers in Medical Activity; Kącki, E., Rudnicki, M., Stempczyńska, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; pp. 73–84. [Google Scholar]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 29 January 2024).
- Moldovan, P.C.; Van den Broeck, T.; Sylvester, R.; Marconi, L.; Bellmunt, J.; van den Bergh, R.C.N.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; Fossati, N.; et al. What Is the Negative Predictive Value of Multiparametric Magnetic Reso-nance Imaging in Excluding Prostate Cancer at Biopsy? A Systematic Review and Meta-analysis from the European Associa-tion of Urology Prostate Cancer Guidelines Panel. Eur. Urol. 2017, 72, 250–266. [Google Scholar] [CrossRef]
- Borofsky, S.; George, A.K.; Gaur, S.; Bernardo, M.; Greer, M.D.; Mertan, F.V.; Taffel, M.; Moreno, V.; Merino, M.J.; Wood, B.J.; et al. What Are We Missing? False-Negative Cancers at Multiparametric MR Imaging of the Prostate. Radiology 2018, 286, 186–195. [Google Scholar] [CrossRef]
- Williams, C.; Ahdoot, M.; Daneshvar, M.A.; Hague, C.; Wilbur, A.R.; Gomella, P.T.; Shih, J.; Khondakar, N.; Yerram, N.; Mehralivand, S.; et al. Why Does Magnetic Resonance Imaging-Targeted Biopsy Miss Clinically Signifi-cant Cancer? J. Urol. 2022, 207, 95–107. [Google Scholar] [CrossRef]
- Ghezzo, S.; Bezzi, C.; Presotto, L.; Mapelli, P.; Bettinardi, V.; Savi, A.; Neri, I.; Preza, E.; Samanes Gajate, A.M.; De Cobelli, F.; et al. State of the art of radiomic analysis in the clinical management of prostate cancer: A sys-tematic review. Crit. Rev. Oncol. Hematol. 2022, 169, 103544. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Ma, S. Robust genetic interaction analysis. Brief. Bioinform. 2019, 20, 624–637. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Bao, M.; Wu, C.; Zhang, J.; Zhang, Y.; Shi, H. A machine learning-assisted decision-support model to better identify patients with prostate cancer requiring an extended pelvic lymph node dissection. BJU Int. 2019, 124, 972–983. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Miao, Q.; Liu, Y.; Raman, S.S.; Scalzo, F.; Sung, K. Integrative Machine Learning Prediction of Prostate Biopsy Results from Negative Multiparametric MRI. J. Magn. Reson. Imaging 2022, 55, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Gibała, S.; Obuchowicz, R.; Lasek, J.; Piórkowski, A.; Nurzynska, K. Textural Analysis Supports Prostate MR Diagnosis in PIRADS Protocol. Appl. Sci. 2023, 13, 9871. [Google Scholar] [CrossRef]
- Wang, J.; Wu, C.-J.; Bao, M.-L.; Zhang, J.; Wang, X.-N.; Zhang, Y.-D. Machine learning-based analysis of MR radiomics can help to improve the diagnostic performance of PI-RADS v2 in clinically relevant prostate cancer. Eur. Radiol. 2017, 27, 4082–4090. [Google Scholar] [CrossRef]
- Min, X.; Li, M.; Dong, D.; Feng, Z.; Zhang, P.; Ke, Z.; You, H.; Han, F.; Ma, H.; Tian, J.; et al. Multi-parametric MRI-based radiomics signature for discriminating between clinically significant and insignificant prostate cancer: Cross-validation of a machine learning method. Eur. J. Radiol. 2019, 115, 16–21. [Google Scholar] [CrossRef]
- Bleker, J.; Kwee, T.C.; Dierckx, R.A.J.O.; de Jong, I.J.; Huisman, H.; Yakar, D. Multiparametric MRI and auto-fixed volume of inter-est-based radiomics signature for clinically significant peripheral zone prostate cancer. Eur. Radiol. 2020, 30, 1313–1324. [Google Scholar] [CrossRef]
- Rabaan, A.A.; Bakhrebah, M.A.; AlSaihati, H.; Alhumaid, S.; Alsubki, R.A.; Turkistani, S.A.; Al-Abdulhadi, S.; Aldawood, Y.; Alsaleh, A.A.; Alhashem, Y.N.; et al. Artificial Intelligence for Clinical Diagnosis and Treatment of Prostate Cancer. Cancers 2022, 14, 5595. [Google Scholar] [CrossRef] [PubMed]
- Shao, L.; Yan, Y.; Liu, Z.; Ye, X.; Xia, H.; Zhu, X.; Zhang, Y.; Zhang, Z.; Chen, H.; He, W.; et al. Radiologist-like artificial intelligence for grade group prediction of radical prostatectomy for reduc-ing upgrading and downgrading from biopsy. Theranostics 2020, 10, 10200–10212. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Shen, J.; Yuan, Z.; Yu, X.; Jiang, P.; Zhong, B.; Xiang, J.; Ren, G.; Xie, L.; Yan, S. Trends in Treatment for Prostate Cancer in China: Preliminary Patterns of Care Study in a Single Institution. J. Cancer 2018, 9, 1797–1803. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Level Charcteristics | Needle Level before Resample | Needle Level after Resample | Needle Level Training | Needle Level Validation | Needle Level p Value * | |
|---|---|---|---|---|---|---|
| Number | 75 | 820 | 718 | 504 | 214 | / |
| PSA | 6.50 (4.50~9.50) | 6.90 (5.40~11.00) | 6.50 (5.40~12.00) | 6.90 (5.30~11.00) | 6.50 (5.40~12.00) | 0.65 |
| Prostate Cancer | 0.98 | |||||
| Yes | 64 (85.33%) | 363 (44.27%) | 363 (50.56%) | 255 (50.60%) | 108 (50.47%) | / |
| No | 11 (14.67%) | 457 (55.73%) | 355 (49.44%) | 249 (49.40%) | 106 (49.53%) | / |
| Gleason Grade Group | 0.88 | |||||
| Not PCa | 11 (14.67%) | 457 (55.73%) | 355 (49.44%) | 249 (49.40%) | 106 (49.53%) | / |
| GG1 | 16 (21.33%) | 184 (22.44%) | 184 (25.63%) | 129 (25.6%) | 55 (25.70%) | / |
| GG2 | 22 (29.33%) | 98 (11.95%) | 98 (13.65%) | 67 (13.29%) | 31 (14.49%) | / |
| GG3 | 14 (18.67%) | 35 (4.27%) | 35 (4.87%) | 24 (4.76%) | 11 (5.14%) | / |
| GG4 | 3 (4.00%) | 23 (2.80%) | 23 (3.20%) | 17 (3.37%) | 6 (2.80%) | / |
| GG5 | 9 (12.00%) | 23 (2.80%) | 23 (3.20%) | 18 (3.57%) | 5 (2.34%) | / |
| Variables | AUC | Sensitivity | Specificity | PPV | NPV | p Value (vs. PI-RADS Control) * | p Value (vs. Shape Control) * | |
|---|---|---|---|---|---|---|---|---|
| LR | Shape Control | 0.659 (0.596–0.723) | 61.11% | 70.75% | 68.04% | 64.10% | / | / |
| PI-RADS Alone | 0.701 (0.640–0.763) | 67.59% | 72.64% | 71.57% | 68.75% | / | / | |
| PI-RADS+2 Features | 0.835 (0.779–0.89) | 74.07% | 77.36% | 76.92% | 74.55% | <0.001 | <0.001 | |
| PI-RADS+3 Features | 0.838 (0.783–0.894) | 76.85% | 77.36% | 77.57% | 76.64% | <0.001 | <0.001 | |
| PI-RADS+4 Features | 0.835 (0.780–0.891) | 76.85% | 76.42% | 76.85% | 76.42% | <0.001 | <0.001 | |
| PI-RADS+5 Features | 0.833 (0.777–0.889) | 79.63% | 78.30% | 78.90% | 79.05% | <0.001 | <0.001 | |
| PI-RADS+6 Features | 0.840 (0.784–0.896) | 81.48% | 78.30% | 79.28% | 80.58% | <0.001 | <0.001 | |
| PI-RADS+7 Features | 0.841 (0.785–0.896) | 81.48% | 79.25% | 80.00% | 80.77% | <0.001 | <0.001 | |
| RF | Shape Control | 0.617 (0.552–0.682) | 58.33% | 65.09% | 63.00% | 60.53% | / | / |
| PI-RADS Alone | 0.701 (0.640–0.763) | 67.59% | 72.64% | 71.57% | 68.75% | / | / | |
| PI-RADS+2 Features | 0.776 (0.720–0.831) | 84.26% | 70.75% | 74.59% | 81.52% | 0.005 | <0.001 | |
| PI-RADS+3 Features | 0.743 (0.684–0.801) | 77.78% | 70.75% | 73.04% | 75.76% | 0.220 | <0.001 | |
| PI-RADS+4 Features | 0.766 (0.709–0.822) | 82.41% | 70.75% | 74.17% | 79.79% | 0.042 | <0.001 | |
| PI-RADS+5 Features | 0.766 (0.709–0.823) | 80.56% | 72.64% | 75.00% | 78.57% | 0.042 | <0.001 | |
| PI-RADS+6 Features | 0.790 (0.735–0.844) | 81.48% | 76.42% | 77.88% | 80.20% | 0.008 | <0.001 | |
| PI-RADS+7 Features | 0.794 (0.740–0.849) | 81.48% | 77.36% | 78.57% | 80.39% | 0.005 | <0.001 | |
| SVM | Shape Control | 0.655 (0.593–0.728) | 55.56% | 75.47% | 69.77% | 62.50% | / | / |
| PI-RADS Alone | 0.701 (0.640–0.763) | 67.59% | 72.64% | 71.57% | 68.75% | / | / | |
| PI-RADS+2 Features | 0.771 (0.714–0.827) | 81.48% | 72.64% | 75.21% | 79.38% | <0.001 | 0.004 | |
| PI-RADS+3 Features | 0.780 (0.725–0.835) | 84.26% | 71.70% | 75.21% | 81.72% | <0.001 | 0.002 | |
| PI-RADS+4 Features | 0.799 (0.745–0.853) | 83.33% | 76.42% | 78.26% | 81.82% | <0.001 | <0.001 | |
| PI-RADS+5 Features | 0.794 (0.74–0.848) | 82.41% | 76.42% | 78.07% | 81.00% | <0.001 | <0.001 | |
| PI-RADS+6 Features | 0.827 (0.776–0.878) | 85.19% | 80.19% | 81.42% | 84.16% | <0.001 | <0.001 | |
| PI-RADS+7 Features | 0.818 (0.766–0.870) | 83.33% | 80.19% | 81.08% | 82.52% | <0.001 | <0.001 |
| LR | Models | Shape Control | PI-RADS Alone | +2 Features | +3 Features | +4 Features | +5 Features | +6 Features | +7 Features |
| Shape Control | |||||||||
| PI-RADS Alone | |||||||||
| PI-RADS+2 Features | <0.001 | <0.001 | |||||||
| PI-RADS+3 Features | <0.001 | <0.001 | 0.051 | ||||||
| PI-RADS+4 Features | <0.001 | <0.001 | 0.935 | 0.531 | |||||
| PI-RADS+5 Features | <0.001 | <0.001 | 0.776 | 0.339 | 0.317 | ||||
| PI-RADS+6 Features | <0.001 | <0.001 | 0.598 | 0.879 | 0.528 | 0.369 | |||
| PI-RADS+7 Features | <0.001 | <0.001 | 0.539 | 0.806 | 0.472 | 0.329 | 0.613 | ||
| RF | Models | Shape Control | PI-RADS Alone | +2 Features | +3 Features | +4 Features | +5 Features | +6 Features | +7 Features |
| Shape Control | |||||||||
| PI-RADS Alone | |||||||||
| PI-RADS+2 Features | <0.001 | 0.005 | |||||||
| PI-RADS+3 Features | <0.001 | 0.220 | 0.164 | ||||||
| PI-RADS+4 Features | <0.001 | 0.042 | 0.688 | 0.280 | |||||
| PI-RADS+5 Features | <0.001 | 0.042 | 0.704 | 0.337 | 0.993 | ||||
| PI-RADS+6 Features | <0.001 | 0.008 | 0.553 | 0.076 | 0.364 | 0.317 | |||
| PI-RADS+7 Features | <0.001 | 0.005 | 0.401 | 0.050 | 0.266 | 0.350 | 0.563 | ||
| SVM | Models | Shape Control | PI-RADS Alone | +2 Features | +3 Features | +4 Features | +5 Features | +6 Features | +7 Features |
| Shape Control | |||||||||
| PI-RADS Alone | |||||||||
| PI-RADS+2 Features | 0.004 | <0.001 | |||||||
| PI-RADS+3 Features | 0.002 | <0.001 | 0.422 | ||||||
| PI-RADS+4 Features | <0.001 | <0.001 | 0.055 | 0.148 | |||||
| PI-RADS+5 Features | <0.001 | <0.001 | 0.055 | 0.302 | 0.317 | ||||
| PI-RADS+6 Features | <0.001 | <0.001 | 0.004 | 0.016 | 0.106 | 0.051 | |||
| PI-RADS+7 Features | <0.001 | <0.001 | 0.016 | 0.066 | 0.312 | 0.193 | 0.155 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.-C.; Ruan, X.-H.; Chun, T.-T.; Yao, C.; Huang, D.; Wong, H.-L.; Lai, C.-T.; Tsang, C.-F.; Ho, S.-H.; Ng, T.-L.; et al. MRI T2w Radiomics-Based Machine Learning Models in Imaging Simulated Biopsy Add Diagnostic Value to PI-RADS in Predicting Prostate Cancer: A Retrospective Diagnostic Study. Cancers 2024, 16, 2944. https://doi.org/10.3390/cancers16172944
Liu J-C, Ruan X-H, Chun T-T, Yao C, Huang D, Wong H-L, Lai C-T, Tsang C-F, Ho S-H, Ng T-L, et al. MRI T2w Radiomics-Based Machine Learning Models in Imaging Simulated Biopsy Add Diagnostic Value to PI-RADS in Predicting Prostate Cancer: A Retrospective Diagnostic Study. Cancers. 2024; 16(17):2944. https://doi.org/10.3390/cancers16172944
Chicago/Turabian StyleLiu, Jia-Cheng, Xiao-Hao Ruan, Tsun-Tsun Chun, Chi Yao, Da Huang, Hoi-Lung Wong, Chun-Ting Lai, Chiu-Fung Tsang, Sze-Ho Ho, Tsui-Lin Ng, and et al. 2024. "MRI T2w Radiomics-Based Machine Learning Models in Imaging Simulated Biopsy Add Diagnostic Value to PI-RADS in Predicting Prostate Cancer: A Retrospective Diagnostic Study" Cancers 16, no. 17: 2944. https://doi.org/10.3390/cancers16172944
APA StyleLiu, J.-C., Ruan, X.-H., Chun, T.-T., Yao, C., Huang, D., Wong, H.-L., Lai, C.-T., Tsang, C.-F., Ho, S.-H., Ng, T.-L., Xu, D.-F., & Na, R. (2024). MRI T2w Radiomics-Based Machine Learning Models in Imaging Simulated Biopsy Add Diagnostic Value to PI-RADS in Predicting Prostate Cancer: A Retrospective Diagnostic Study. Cancers, 16(17), 2944. https://doi.org/10.3390/cancers16172944