

Brachytherapy in Brain Metastasis Treatment: A Scoping Review of Advances in Techniques and Clinical Outcomes


 and
and
Abstract
Simple Summary
Abstract
1. Introduction
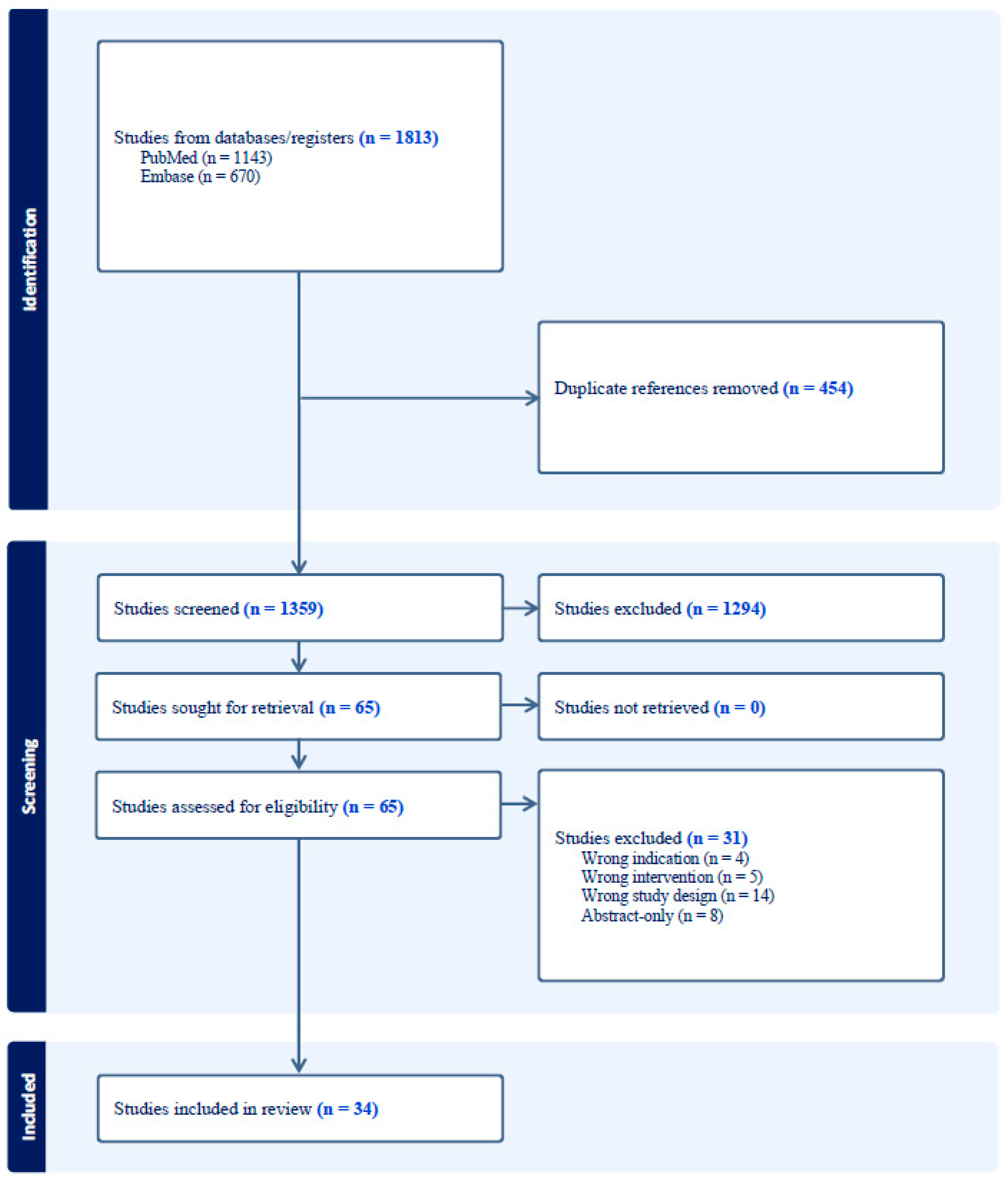
2. Methods
3. Results
- A.
- Radioactive Isotopes: Iodine-125
- B.
- Radioactive Isotopes: Cesium-131
- C.
- Clinical Outcomes and Safety
- D.
- Knowledge Gaps and Future Directions
Limitations
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nayak, L.; Lee, E.Q.; Wen, P.Y. Epidemiology of brain metastases. Curr. Oncol. Rep. 2012, 14, 48–54. [Google Scholar] [CrossRef]
- Chao, J.H.; Phillips, R.; Nickson, J.J. Roentgen-ray therapy of cerebral metastases. Cancer 1954, 7, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.D.; Ballman, K.V.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Whitton, A.C.; Greenspoon, J.; Parney, I.F.; Laack, N.N.I.; Ashman, J.B.; et al. Postoperative stereotactic radiosurgery compared with whole brain radiotherapy for resected metastatic brain disease (NCCTG N107C/CEC·3): A multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1049–1060. [Google Scholar] [CrossRef]
- Gondi, V.; Pugh, S.L.; Tome, W.A.; Caine, C.; Corn, B.; Kanner, A.; Rowley, H.; Kundapur, V.; DeNittis, A.; Greenspoon, J.N.; et al. Preservation of memory with conformal avoidance of the hippocampal neural stem-cell compartment during whole-brain radiotherapy for brain metastases (RTOG 0933): A phase II multi-institutional trial. J. Clin. Oncol. 2014, 32, 3810–3816. [Google Scholar] [CrossRef]
- Vogelbaum, M.A.; Brown, P.D.; Messersmith, H.; Brastianos, P.K.; Burri, S.; Cahill, D.; Dunn, I.F.; Gaspar, L.E.; Gatson, N.T.N.; Gondi, V.; et al. Treatment for Brain Metastases: ASCO-SNO-ASTRO Guideline. J. Clin. Oncol. 2022, 40, 492–516. [Google Scholar] [CrossRef] [PubMed]
- Chitti, B.; Goyal, S.; Sherman, J.H.; Caputy, A.; Sarfaraz, M.; Cifter, G.; Aghdam, H.; Rao, Y.J. The role of brachytherapy in the management of brain metastases: A systematic review. J. Contemp. Brachytherapy 2020, 12, 67–83. [Google Scholar] [CrossRef]
- Schwarz, S.B.; Thon, N.; Nikolajek, K.; Niyazi, M.; Tonn, J.C.; Belka, C.; Kreth, F.W. Iodine-125 brachytherapy for brain tumours—A review. Radiat. Oncol. 2012, 7, 30. [Google Scholar] [CrossRef] [PubMed]
- Bander, E.D.; Kelly, A.; Ma, X.; Christos, P.J.; Wernicke, A.G.; Stieg, P.E.; Trichter, S.; Knisely, J.P.; Ramakrishna, R.; Schwartz, T.H. Safety and efficacy of Cesium-131 brachytherapy for brain tumors. J. Neuro-Oncol. 2023, 163, 355–365. [Google Scholar] [CrossRef]
- Bogart, J.A.; Ungureanu, C.; Shihadeh, E.; Chung, C.T.; King, G.A.; Ryu, S.; Kent, C.; Winfield, J.A. Resection and Permanent I-125 Brachytherapy Without Whole Brain Irradiation for Solitary Brain Metastasis from Non-small Cell Lung Carcinoma. J. Neuro-Oncol. 1999, 44, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Brahimaj, B.; Lamba, M.; Breneman, J.C.; Warnick, R.E. Iodine-125 seed migration within brain parenchyma after brachytherapy for brain metastasis: Case report. J. Neurosurg. 2016, 125, 1167–1170. [Google Scholar] [CrossRef]
- Dagnew, E.; Kanski, J.; McDermott, M.W.; Sneed, P.K.; McPherson, C.; Breneman, J.C.; Warnick, R.E. Management of newly diagnosed single brain metastasis using resection and permanent iodine-125 seeds without initial whole-brain radiotherapy: A two-institution experience. Neurosurg. Focus 2007, 22, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Greenwald, J.; Taube, S.; Yondorf, M.Z.; Smith, A.; Sabbas, A.; Wernicke, A.G. Placement of 131 Cs permanent brachytherapy seeds in a large combined cavity of two resected brain metastases in one setting: Case report and technical note. J. Contemp. Brachytherapy 2019, 11, 356–360. [Google Scholar] [CrossRef]
- Hirschfeld, C.B.; Schwartz, T.H.; Parashar, B.; Wernicke, A.G. Seed migration to the spinal canal after postresection brachytherapy to treat a large brain metastasis. Brachytherapy 2016, 15, 637–641. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Sneed, P.K.; Kunwar, S.; Kragten, A.; Larson, D.A.; Berger, M.S.; Chan, A.; Pouliot, J.; McDermott, M.W. Surgical resection and permanent iodine-125 brachytherapy for brain metastases. J. Neurooncol. 2009, 91, 83–93. [Google Scholar] [CrossRef]
- Julie, D.A.; Lazow, S.P.; Vanderbilt, D.B.; Taube, S.; Yondorf, M.Z.; Sabbas, A.; Pannullo, S.; Schwartz, T.H.; Wernicke, A.G. A matched-pair analysis of clinical outcomes after intracavitary cesium-131 brachytherapy versus stereotactic radiosurgery for resected brain metastases. J. Neurosurg. 2021, 134, 1447–1454. [Google Scholar] [CrossRef] [PubMed]
- Mahase, S.S.; Julie, D.; Pannullo, S.C.; Parashar, B.; Wernicke, A.G. Excellent Outcomes in a Geriatric Patient with Multiple Brain Metastases Undergoing Surgical Resection with Cesium-131 Implantation and Stereotactic Radiosurgery. Cureus 2017, 9, e1970. [Google Scholar] [CrossRef]
- Nakaji, P.; Smith, K.; Youssef, E.; Thomas, T.; Pinnaduwage, D.; Rogers, L.; Wallstrom, G.; Brachman, D. Resection and Surgically Targeted Radiation Therapy for the Treatment of Larger Recurrent or Newly Diagnosed Brain Metastasis: Results from a Prospective Trial. Cureus 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Ostertag, C.B.; Kreth, F.W. Interstitial iodine-125 radiosurgery for cerebral metastases. Br. J. Neurosurg. 1995, 9, 593–603. [Google Scholar] [CrossRef]
- Petr, M.J.; McPherson, C.M.; Breneman, J.C.; Warnick, R.E. Management of newly diagnosed single brain metastasis with surgical resection and permanent I-125 seeds without upfront whole brain radiotherapy. J. Neurooncol. 2009, 92, 393–400. [Google Scholar] [CrossRef]
- Pham, A.; Yondorf, M.Z.; Parashar, B.; Scheff, R.J.; Pannullo, S.C.; Ramakrishna, R.; Stieg, P.E.; Schwartz, T.H.; Wernicke, A.G. Neurocognitive function and quality of life in patients with newly diagnosed brain metastasis after treatment with intra-operative cesium-131 brachytherapy: A prospective trial. J. Neurooncol. 2016, 127, 63–71. [Google Scholar] [CrossRef]
- Raleigh, D.R.; Seymour, Z.A.; Tomlin, B.; Theodosopoulos, P.V.; Berger, M.S.; Aghi, M.K.; Geneser, S.E.; Krishnamurthy, D.; Fogh, S.E.; Sneed, P.K.; et al. Resection and brain brachytherapy with permanent iodine-125 sources for brain metastasis. J. Neurosurg. 2017, 126, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Rogers, L.R.; Rock, J.P.; Sills, A.K.; Vogelbaum, M.A.; Suh, J.H.; Ellis, T.L.; Stieber, V.W.; Asher, A.L.; Fraser, R.W.; Billingsley, J.S.; et al. Results of a phase II trial of the GliaSite Radiation Therapy System for the treatment of newly diagnosed, resected single brain metastases. J. Neurosurg. 2006, 105, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Romagna, A.; Schwartz, C.; Egensperger, R.; Watson, J.; Tonn, J.-C.; Belka, C.; Kreth, F.-W.; Nachbichler, S.B. Iodine-125 brachytherapy as upfront and salvage treatment for brain metastases. Strahlenther. Und Onkol. 2016, 192, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Ruge, M.I.; Kocher, M.; Maarouf, M.; Hamisch, C.; Treuer, H.; Voges, J.; Sturm, V. Comparison of stereotactic brachytherapy (125 iodine seeds) with stereotactic radiosurgery (LINAC) for the treatment of singular cerebral metastases. Strahlenther. Onkol. 2011, 187, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Ruge, M.I.; Suchorska, B.; Maarouf, M.; Runge, M.; Treuer, H.; Voges, J.; Sturm, V. Stereotactic 125iodine brachytherapy for the treatment of singular brain metastases: Closing a gap? Neurosurgery 2011, 68, 1209–1218, discussion 1218–1209. [Google Scholar] [CrossRef] [PubMed]
- Schulder, M.; Black, P.M.; Shrieve, D.C.; Iii, E.A.; Loeffler, J.S. Permanent low-activity iodine-125 implants for cerebral metastases. J. Neuro-Oncol. 1997, 33, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Warren, K.T.; Boucher, A.; Bray, D.P.; Dresser, S.; Zhong, J.; Shu, H.-K.; Olson, J.; Hoang, K. Surgical Outcomes of Novel Collagen Tile Cesium Brachytherapy for Recurrent Intracranial Tumors at a Tertiary Referral Center. Cureus 2021, 13, e19777. [Google Scholar] [CrossRef]
- Wernicke, A.G.; Yondorf, M.Z.; Peng, L.; Trichter, S.; Nedialkova, L.; Sabbas, A.; Kulidzhanov, F.; Parashar, B.; Nori, D.; Clifford Chao, K.S.; et al. Phase I/II study of resection and intraoperative cesium-131 radioisotope brachytherapy in patients with newly diagnosed brain metastases. J. Neurosurg. 2014, 121, 338–348. [Google Scholar] [CrossRef]
- Wernicke, A.G.; Hirschfeld, C.B.; Smith, A.W.; Taube, S.; Yondorf, M.Z.; Parashar, B.; Nedialkova, L.; Kulidzhanov, F.; Trichter, S.; Sabbas, A.; et al. Clinical Outcomes of Large Brain Metastases Treated With Neurosurgical Resection and Intraoperative Cesium-131 Brachytherapy: Results of a Prospective Trial. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 1059–1068. [Google Scholar] [CrossRef]
- Wernicke, A.G.; Lazow, S.P.; Taube, S.; Yondorf, M.Z.; Kovanlikaya, I.; Nori, D.; Christos, P.; Boockvar, J.A.; Pannullo, S.; Stieg, P.E.; et al. Surgical Technique and Clinically Relevant Resection Cavity Dynamics Following Implantation of Cesium-131 (Cs-131) Brachytherapy in Patients With Brain Metastases. Oper. Neurosurg. 2016, 12, 49–60. [Google Scholar] [CrossRef]
- Xia, Y.; A Mashouf, L.; Baker, B.R.; Maxwell, R.; Bettegowda, C.; Redmond, K.J.; Kleinberg, L.R.; Lim, M. Outcomes of Metastatic Brain Lesions Treated with Radioactive Cs-131 Seeds after Surgery: Experience from One Institution. Cureus 2018, 10, e3075. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Wang, C.; Zhang, W.; Liu, S.; Xuan, T.; Jiang, H.; Hu, X.; Hu, M.; Li, H. Iodine-125 brachytherapy treatment for newly diagnosed brain metastasis in non-small cell lung cancer: A biocentric analysis. Front. Oncol. 2022, 12, 1005876. [Google Scholar] [CrossRef]
- Yondorf, M.Z.; Faraz, S.; Smith, A.W.; Sabbas, A.; Parashar, B.; Schwartz, T.H.; Wernicke, A.G. Dosimetric differences between cesium-131 and iodine-125 brachytherapy for the treatment of resected brain metastases. J. Contemp. Brachytherapy 2020, 12, 311–316. [Google Scholar] [CrossRef]
- Bernstein, M.; Cabantog, A.; Laperriere, N.; Leung, P.; Thomason, C. Brachytherapy for Recurrent Single Brain Metastasis. Can. J. Neurol. Sci. / J. Can. des Sci. Neurol. 1995, 22, 13–16. [Google Scholar] [CrossRef]
- Chen, W.C.; Lafreniere, M.; Phuong, C.; Liu, S.J.; Baal, J.D.; Lometti, M.; Morin, O.; Ziemer, B.; Vasudevan, H.N.; Lucas, C.-H.G.; et al. Resection with intraoperative cesium-131 brachytherapy as salvage therapy for recurrent brain tumors. J. Neurosurg. 2022, 137, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Cummins, D.D.; Morshed, R.A.; Chavez, M.M.; Avalos, L.N.; Sudhakar, V.; Chung, J.E.; Gallagher, A.; Saggi, S.; Daras, M.; Braunstein, S.; et al. Salvage Surgery for Local Control of Brain Metastases After Previous Stereotactic Radiosurgery: A Single-Center Series. World Neurosurg. 2021, 158, E323–E333. [Google Scholar] [CrossRef] [PubMed]
- Dharnipragada, R.; Ferreira, C.; Shah, R.; Reynolds, M.; Dusenbery, K.; Chen, C.C. GammaTile(R) (GT) as a brachytherapy platform for rapidly growing brain metastasis. Neurooncol. Adv. 2023, 5, vdad062. [Google Scholar] [CrossRef] [PubMed]
- Ruge, M.I.; Kickingereder, P.; Grau, S.; Hoevels, M.; Treuer, H.; Sturm, V. Stereotactic biopsy combined with stereotactic 125iodine brachytherapy for diagnosis and treatment of locally recurrent single brain metastases. J. Neuro-Oncol. 2011, 105, 109–118. [Google Scholar] [CrossRef]
- Wernicke, A.G.; Smith, A.W.; Taube, S.; Yondorf, M.Z.; Parashar, B.; Trichter, S.; Nedialkova, L.; Sabbas, A.; Christos, P.; Ramakrishna, R.; et al. Cesium-131 brachytherapy for recurrent brain metastases: Durable salvage treatment for previously irradiated metastatic disease. J. Neurosurg. 2017, 126, 1212–1219. [Google Scholar] [CrossRef]
- Wu, K.C.; Cantalino, J.M.; Dee, E.C.; Hsu, L.; Harris, T.C.; Rawal, B.; Juvekar, P.R.; A Mooney, M.; Dunn, I.F.; A Aizer, A.; et al. Salvage brachytherapy for multiply recurrent metastatic brain tumors: A matched case analysis. Neuro-Oncol. Adv. 2022, 4, vdac039. [Google Scholar] [CrossRef]
- Kim, J.H.; Hilaris, B. Iodine 125 source in interstitial tumor therapy. Clinical and biological considerations. Am. J. Roentgenol. Radium Ther. Nucl. Med. 1975, 123, 163–169. [Google Scholar] [CrossRef]
- Krishnaswamy, V. Dose distribution around an 125I seed source in tissue. Radiology 1978, 126, 489–491. [Google Scholar] [CrossRef]
- Bernstein, M.; Gutin, P.H. Interstitial irradiation of brain tumors: A review. Neurosurgery 1981, 9, 741–750. [Google Scholar] [CrossRef]
- Gutin, P.H.; Phillips, T.L.; Hosobuchi, Y.; Wara, W.M.; MacKay, A.R.; Weaver, K.A.; Lamb, S.; Hurst, S. Permanent and removable implants for the brachytherapy of brain tumors. Int. J. Radiat. Oncol. Biol. Phys. 1981, 7, 1371–1381. [Google Scholar] [CrossRef] [PubMed]
- Prados, M.; Leibel, S.; Barnett, C.M.; Gutin, P. Interstitial brachytherapy for metastatic brain tumors. Cancer 1989, 63, 657–660. [Google Scholar] [CrossRef]
- Shaw, E.; Mikkelson, T.; Kleinberg, L.; Crocker, I.; Herman, T.; Pearlman, J.; Carson, K.; Fisher, J.; deGuzman, A.; Tatter, S. The gliasite radiation therapy system (RTS): A novel approach to brain brachytherapy for recurrent malignant glioma. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 203. [Google Scholar] [CrossRef]
- Tatter, S.B.; Shaw, E.G.; Rosenblum, M.L.; Karvelis, K.C.; Kleinberg, L.; Weingart, J.; Olson, J.J.; Crocker, I.R.; Brem, S.; Pearlman, J.L.; et al. An inflatable balloon catheter and liquid 125I radiation source (GliaSite Radiation Therapy System) for treatment of recurrent malignant glioma: Multicenter safety and feasibility trial. J. Neurosurg. 2003, 99, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Wernicke, A.G.; Sherr, D.L.; Schwartz, T.H.; Pannullo, S.C.; Stieg, P.E.; Boockvar, J.A.; Ivanidze, J.; Moliterno, J.A.; Parashar, B.; Trichter, S.; et al. Feasibility and safety of GliaSite brachytherapy in treatment of CNS tumors following neurosurgical resection. J. Cancer Res. Ther. 2010, 6, 65–74. [Google Scholar] [CrossRef]
- Imber, B.S.; Young, R.J.; Beal, K.; Reiner, A.S.; Giantini-Larsen, A.M.; Krebs, S.; Yang, J.T.; Aramburu-Nunez, D.; Cohen, G.N.; Brennan, C.; et al. Salvage resection plus cesium-131 brachytherapy durably controls post-SRS recurrent brain metastases. J. Neuro-Oncol. 2022, 159, 609–618. [Google Scholar] [CrossRef]
- Atalar, B.; Choi, C.Y.; Harsh, G.R.T.; Chang, S.D.; Gibbs, I.C.; Adler, J.R.; Soltys, S.G. Cavity volume dynamics after resection of brain metastases and timing of postresection cavity stereotactic radiosurgery. Neurosurgery 2013, 72, 180–185, discussion 185. [Google Scholar] [CrossRef]
- Dale, R.G.; Jones, B.; Coles, I.P. Effect of tumour shrinkage on the biological effectiveness of permanent brachytherapy implants. Br. J. Radiol. 1994, 67, 639–645. [Google Scholar] [CrossRef]
- Wowra, B.; Schmitt, H.P.; Sturm, V. Incidence of late radiation necrosis with transient mass effect after interstitial low dose rate radiotherapy for cerebral gliomas. Acta Neurochir. 1989, 99, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Han, D.Y.; Ma, L.; Braunstein, S.; Raleigh, D.; Sneed, P.K.; McDermott, M. Resection Cavity Contraction Effects in the Use of Radioactive Sources (1-25 versus Cs-131) for Intra-Operative Brain Implants. Cureus 2018, 10, e2079. [Google Scholar] [CrossRef] [PubMed]
- Tom, M.C.; Joshi, N.; Vicini, F.; Chang, A.J.; Hong, T.S.; Showalter, T.N.; Chao, S.T.; Wolden, S.; Wu, A.J.; Martin, D.; et al. The American Brachytherapy Society consensus statement on intraoperative radiation therapy. Brachytherapy 2019, 18, 242–257. [Google Scholar] [CrossRef] [PubMed]
- Budnick, H.C.; Richardson, A.M.; Shiue, K.; Watson, G.; Ng, S.K.; Le, Y.; Shah, M.V. GammaTile for Gliomas: A Single-Center Case Series. Cureus 2021, 13, e19390. [Google Scholar] [CrossRef]
- Gessler, D.J.; Neil, E.C.; Shah, R.; Levine, J.; Shanks, J.; Wilke, C.; Reynolds, M.; Zhang, S.; Ozutemiz, C.; Gencturk, M.; et al. GammaTile(R) brachytherapy in the treatment of recurrent glioblastomas. Neurooncol. Adv. 2022, 4, vdab185. [Google Scholar] [CrossRef] [PubMed]
- Patchell, R.A.; Tibbs, P.A.; Regine, W.F.; Dempsey, R.J.; Mohiuddin, M.; Kryscio, R.J.; Markesbery, W.R.; Foon, K.A.; Young, B. Postoperative radiotherapy in the treatment of single metastases to the brain: A randomized trial. JAMA 1998, 280, 1485–1489. [Google Scholar] [CrossRef] [PubMed]
- Aoyama, H.; Shirato, H.; Tago, M.; Nakagawa, K.; Toyoda, T.; Hatano, K.; Kenjyo, M.; Oya, N.; Hirota, S.; Shioura, H.; et al. Stereotactic Radiosurgery Plus Whole-Brain Radiation Therapy vs Stereotactic Radiosurgery Alone for Treatment of Brain MetastasesA Randomized Controlled Trial. JAMA 2006, 295, 2483–2491. [Google Scholar] [CrossRef] [PubMed]
- Andrews, D.W.; Scott, C.B.; Sperduto, P.W.; Flanders, A.E.; Gaspar, L.E.; Schell, M.C.; Werner-Wasik, M.; Demas, W.; Ryu, J.; Bahary, J.-P.; et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: Phase III results of the RTOG 9508 randomised trial. Lancet 2004, 363, 1665–1672. [Google Scholar] [CrossRef] [PubMed]
- Jagannathan, J.; Yen, C.P.; Ray, D.K.; Schlesinger, D.; Oskouian, R.J.; Pouratian, N.; Shaffrey, M.E.; Larner, J.; Sheehan, J.P. Gamma Knife radiosurgery to the surgical cavity following resection of brain metastases. J. Neurosurg. 2009, 111, 431–438. [Google Scholar] [CrossRef]
- Hartford, A.C.; Paravati, A.J.; Spire, W.J.; Li, Z.; Jarvis, L.A.; Fadul, C.E.; Rhodes, C.H.; Erkmen, K.; Friedman, J.; Gladstone, D.J.; et al. Postoperative Stereotactic Radiosurgery Without Whole-Brain Radiation Therapy for Brain Metastases: Potential Role of Preoperative Tumor Size. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Yondorf, M.Z.; Schwartz, T.H.; Boockvar, J.A.; Pannullo, S.; Stieg, P.; Sabbas, A.; Pavese, A.; Trichter, S.; Nedialkova, L.; Parashar, B.; et al. Radiation Exposure and Safety Precautions Following 131Cs Brachytherapy in Patients with Brain Tumors. Health Phys. 2017, 112, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Ekhator, C.; Nwankwo, I.; Rak, E.; Homayoonfar, A.; Fonkem, E.; Rak, R. GammaTile: Comprehensive Review of a Novel Radioactive Intraoperative Seed-Loading Device for the Treatment of Brain Tumors. Cureus 2022, 14, e29970. [Google Scholar] [CrossRef] [PubMed]
- Pinnaduwage, D.S.; Srivastava, S.P.; Yan, X.; Jani, S.; Brachman, D.G.; Sorensen, S.P. Dosimetric Impacts of Source Migration, Radioisotope Type, and Decay with Permanent Implantable Collagen Tile Brachytherapy for Brain Tumors. Technol. Cancer Res. Treat. 2022, 21, 15330338221106852. [Google Scholar] [CrossRef] [PubMed]
- Moss, N.S.; Imber, B.S.; Cohen, G.; Prasad, K.; Nunez, D.A.; Brennan, C.W.; Tabar, V.; Beal, K.P. TRLS-07. Intracavitary carrier-embedded Cs131 brachytherapy for recurrent brain metastases: A randomized phase II study. Neuro-Oncol. Adv. 2021, 3, iii7. [Google Scholar] [CrossRef]
- Weinberg, J.; Beckham, T.; McAleer, M.F.; Johnson, J.M.; Yuan, Y.; Lin, H.; Kudchadker, R.; Schwartz, T.; Knisely, J.; Dunbar, E.; et al. Rtid-01. Phase Iii Multicenter Rct of Post-Surgical Stereotactic Radiotherapy Versus Surgically Targeted Radiation Therapy for the Treatment of Large Newly Diagnosed Brain Metastases—Trial in Progress. Neuro-Oncol. 2021, 23, vi193. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Title | Journal | Country | Study Design | Cohort Size | Number of Patients with BM Treated with Brachytherapy | Primary Tumor | De-Novo or Recurrent BM | Single or Multiple BM | Isotope and Formulation | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bander, 2023 [8] | Safety and efficacy of Cesium-131 brachytherapy for brain tumors | Journal of Neuro-Oncology | USA | Retrospective | 119 | 79 | NSCLC, melanoma, breast, renal, GI, cervical, endometrial | De-Novo | Single | Cs-131 seeds | 1-year survival rates were 53.3% (95%CI 41.9–64.6%) and 1-year local control rates were 84.7% for BM. Local control was superior in NSCLC relative to other BM pathologies (90.8% versus 76.5%). RN: 0 |
| Bogart, 1999 [9] | Resection and permanent I-125 brachytherapy without whole brain irradiation for solitary brain metastasis from non-small cell lung carcinoma | Journal of Neuro-Oncology | USA | Retrospective | 15 | 15 | NSCLC | De-Novo | Single | I-125 seeds | Median survival: 14 months for all patients, 26 months for patients with single BM. No failures were seen with single BM < 2.5 cm. Recurrence rates both adjacent and outside the area of the initial brain lesion are similar to studies with resection + WBRT. |
| Brahimaj, 2016 [10] | Iodine-125 seed migration within brain parenchyma after brachytherapy for brain metastasis: case report | Journal of Neurosurgery | USA | Case report | 1 | 1 | Ovarian | De-Novo | Single | I-125 seeds | Seed migration along white matter tracts with neurological decline and death. |
| Dagnew, 2007 [11] | Management of newly diagnosed single brain metastasis using resection and permanent iodine-125 seeds without initial whole-brain radiotherapy: a two institution experience | Journal of Neurosurgery | USA | Retrospective | 26 | 26 | Lung, melanoma, colon, breast, renal, cervix, prostate, ovarian | De-Novo | Single | I-125 seeds | All patients treated with resection + I-125 seeds showed stable or improved KPS score. Median actuarial survival rate: 17.8 months. |
| Greenwald, 2019 [12] | Placement of 131Cs permanent brachytherapy seeds in a large combined cavity of two resected brain metastases in one setting: case report and technical note | Journal of Contemporary Brachytherapy | USA | Case report | 1 | 1 | Hypopharyngeal | De-Novo | Multiple | Cs-131 seeds | No recurrence; OS 20 months; no RN |
| Hirschfeld, 2016 [13] | Seed migration to the spinal canal after postresection brachytherapy to treat a large brain metastasis | Brachytherapy | USA | Case report | 1 | 1 | Esophageal | De-Novo | Single | Cs-131 seeds | Seed migration to the spinal canal with no new symptoms and no RN |
| Huang, 2009 [14] | Surgical resection and permanent iodine-125 brachytherapy for brain metastases | Journal of Neuro-Oncology | USA | Retrospective | 40 | 40 | Lung, breast, renal, melanoma | De-Novo | Both | I-125 seeds | Median OS: 11.3 months; 12.0 months in patients with de-novo BMs and 7.3 months in patients with recurrent BMs. 1-year local FFP rates for de-novo, recurrent, and all patients, respectively: 92%, 86%, and 88%; 1-year distant FFP rates: 29%, 43%, and 37%. |
| Julie, 2021 [15] | A matched-pair analysis of clinical outcomes after intracavitary cesium-131 brachytherapy versus stereotactic radiosurgery for resected brain metastases | Journal of Neurosurgery | USA | Retrospective | 30 | 30 | NSCLC, breast, CRC, GI, endometrial, melanoma, oropharynx, renal | De-Novo | Single | Cs-131 seeds | SD in LR: 10% for the resection + Cs-131 cohort and 28.3% for resection + SRS cohort (OR 0.281, 95% CI 0.082‚ 0.949; p = 0.049). NSD in RR, DR, and OS. Kaplan–Meier analysis showed a significantly higher likelihood of freedom from LR (p = 0.027) and DR (p = 0.018) after Cs-131 compared to SRS treatment (p = 0.027). NSD in likelihood of OS (p = 0.093). RN: 10% in SRS group and 3.3% in Cs-131 group (p = 0.417). |
| Mahase, 2017 [16] | Excellent Outcomes in a Geriatric Patient with Multiple Brain Metastases Undergoing Surgical Resection with Cesium-131 Implantation and Stereotactic Radiosurgery | Cureus | USA | Case report | 1 | 1 | Unknown | De-Novo | Multiple | Cs-131 seeds | No recurrence; OS 72 months; no RN |
| Nakaji, 2020 [17] | Resection and Surgically Targeted Radiation Therapy for the Treatment of Larger Recurrent or Newly Diagnosed Brain Metastasis: Results From a Prospective Trial | Cureus | USA | Prospective | 11 | 11 | Lung, breast | De-Novo and Recurrent | Both | Cs-131 GammaTile | 1-year local FFP 91%; median OS 9.5 months (range, 1.4–28); RN 0% |
| Ostertag, 1995 [18] | Interstitial iodine-125 radiosurgery for cerebral metastases | British Journal of Neurosurgery | Germany | Retrospective | 93 | 93 | Lung, renal, melanoma, GI, GYN, breast, thyroid | De-Novo | Both | I-125 seeds | Median survival: 17 months in group IRT + percutaneous RT, 15 months in group IRT, 6 months in group IRT + prior RT. Favorable prognostic factors were a KPS > or = 70, single BM, absence of disseminated disease, and a time interval > 1 year between primary tumor and BM diagnosis. |
| Petr, 2009 [19] | Management of newly diagnosed single brain metastasis with surgical resection and permanent I-125 seeds without upfront whole brain radiotherapy | Journal of Neuro-Oncology | USA | Retrospective | 72 | 72 | Lung, breast, CRC, melanoma, ovarian, renal, prostate, thyroid, cervical, bladder | De-Novo | Single | I-125 seeds | Local control rate 93% at median 16 months. Distant brain failures occurred in 32%. RN: 5.6%. All patients had stable or improved KPS at 1 month. Median actuarial survival rate: 14 months; 2-year survival rate: 27%. |
| Pham, 2016 [20] | Neurocognitive function and quality of life in patients with newly diagnosed brain metastasis after treatment with intra-operative cesium-131 brachytherapy: a prospective trial | Journal of Neuro-Oncology | USA | Phase I/II Clinical Trial | 24 | 24 | Lung | De-Novo | Single | Cs-131 seeds | SD in MMSE and FACT-BR from baseline at 4 months (p = 0.001) and 6 months (p = 0.001) post-Cs131. |
| Raleigh, 2017 [21] | Resection and brain brachytherapy with permanent iodine-125 sources for brain metastasis | Journal of Neurosurgery | USA | Retrospective | 95 | 95 | Lung, melanoma, breast | De-Novo | Both | I-125 seeds | Crude local control: 90% at median 14.4-month follow-up. Median OS extended from 2.1 months in the shortest quartile to 62.3 months in the longest quartile (p < 0.0001). RN: 15%. |
| Rogers, 2006 [22] | Results of a phase II trial of the GliaSite radiation therapy system for the treatment of newly diagnosed, resected single brain metastases | Journal of Neurosurgery | USA | Prospective | 71 | 71 | NSCLC | De-Novo | Single | I-125 GliaSite | Local control rate: 82–87%. Median survival time and median duration of functional independence: 40 weeks. Results similar to resection + WBRT. |
| Romagna, 2016 [23] | Iodine-125 brachytherapy as upfront and salvage treatment for brain metastases: A comparative analysis | Strahlentherapie und Onkologie | Germany | Prospective | 43 | 43 | Lung, breast, GI, skin, prostate, renal, uterine, ovarian, MSK | De-Novo and Recurrent | Both | I-125 seeds | NSD in 1-year local/distant control rates after upfront and salvage SBT (94%/65% vs. 87%/57%, p = 0.45, respectively). Grade I/II toxicity seen in 2 patients after salvage SBT. |
| Ruge, Kocher, 2011 [24] | Comparison of stereotactic brachytherapy (125 iodine seeds) with stereotactic radiosurgery (LINAC) for the treatment of singular cerebral metastases | Strahlentherapie und Onkologie | Germany | Retrospective | 219 | 77 | NSCLC, breast, melanoma, renal, CRC | De-Novo | Single | I-125 seeds | NSD in median OS or actuarial local/distant control at 1 year. No permanent grade III/IV CNS toxicity. |
| Ruge, Suchorska, 2011 [25] | Stereotactic 125iodine brachytherapy for the treatment of singular brain metastases: closing a gap? | Neurosurgery | Germany | Retrospective | 90 | 90 | NSCLC, breast, renal, melanoma, CRC | De-Novo | Single | I-125 seeds | Median OS: 8.5 months. 1-year actuarial local and distant recurrence: 5.4% and 46.4%, respectively. KPS ≥ 70 (p < 0.002), stable systemic disease (p < 0.02), and a prolonged (>12 month) interval between diagnosis and brachytherapy (p < 0.05) significantly improved survival. |
| Schulder, 1997 [26] | Permanent low-activity iodine-125 implants for cerebral metastases | Journal of Neuro-Oncology | USA | Retrospective | 13 | 13 | Lung, germ cell, breast, melanoma, renal | De-Novo | Single | I-125 seeds | All patients received WBRT. Implant dose ranged from 43 Gy–132 Gy, mean 83 Gy. Survival after implantation ranged from 2 weeks–9 years, median 9 months. |
| Warren, 2021 [27] | Surgical Outcomes of Novel Collagen Tile Cesium Brachytherapy for Recurrent Intracranial Tumors at a Tertiary Referral Center | Cureus | USA | Retrospective | 12 | 2 | Lung, breast | De-Novo | Single | Cs-131 GammaTile | Loco-regional FFP 58.3%; median OS 7 months (IQR, 3–10); RN 8.3% |
| Wernicke, 2014 [28] | Phase I/II study of resection and intraoperative cesium-131 radioisotope brachytherapy in patients with newly diagnosed brain metastases | Journal of Neurosurgery | USA | Phase I/II Clinical Trial | 24 | 24 | Lung, breast, renal, melanoma, colon, cervix | De-Novo | Single | Cs-131 seeds | 1-year FFP: local 100%, regional 93.8%, distant 48.4%; 1-year OS 50%; RN 0% |
| Wernicke, Hirschfeld, 2017 [29] | Clinical Outcomes of Large Brain Metastases Treated With Neurosurgical Resection and Intraoperative Cesium-131 Brachytherapy: Results of a Prospective Trial | International Journal of Radiation Oncology Biology Physics | USA | Prospective | 46 | 46 | Lung, colon, breast, melanoma, uterine, esophageal, renal, hepatobiliary, tonsillar | De-Novo | Both | Cs-131 seeds | 1-year FFP: local 100%, regional 89%, distant 52%; 1-year OS 58%; RN 0% |
| Wernicke, Lazow, 2016 [30] | Surgical Technique and Clinically Relevant Resection Cavity Dynamics Following Implantation of Cesium-131 (Cs-131) Brachytherapy in Patients With Brain Metastases | Operative Neurosurgery | USA | Phase I/II Clinical Trial | 24 | 24 | Lung, breast, melanoma, uterine, renal, CRC, esophageal | De-Novo | Single | Cs-131 seeds | SD in post-implantation cavity shrinkage resection + Cs-131 56.5% vs. resection + SRS 84.8% (p = 0.008) |
| Wernicke, Yondorf, 2016 [28] | The cost-effectiveness of surgical resection and cesium-131 intraoperative brachytherapy versus surgical resection and stereotactic radiosurgery in the treatment of metastatic brain tumors | Journal of Neuro-Oncology | USA | Phase I/II Clinical Trial | 24 | 24 | Lung, breast, colon | De-Novo | Single | Cs-131 seeds | Direct costs per patient: resection + Cs-131 USD 19,271 vs. resection + SRS USD 44,219; 1-year OS: resection + SRS 61% vs. resection + Cs-131 50% (p = 0.137); QALY compared (p < 0.0001); ICER resection + SRS significantly inferior (p < 0.0001); resection + Cs-131 significantly more cost-effective. |
| Xia, 2018 [31] | Outcomes of Metastatic Brain Lesions Treated with Radioactive Cs-131 Seeds after Surgery: Experience from One Institution | Cureus | USA | Retrospective | 9 | 9 | Breast, lung, melanoma, uterine, thyroid, CRC | De-Novo | Both | Cs-131 seeds | 1-year FFP: local 100%, distant 66.7%; median OS 9.4 months (range, 1.3–42.2); RN 0% |
| Yang, 2022 [32] | Iodine-125 brachytherapy treatment for newly diagnosed brain metastasis in non-small cell lung cancer: A biocentric analysis | Frontiers of Oncology | China | Retrospective | 99 | 59 | NSCLC | De-Novo | Single | I-125 seeds | SD in 6-month PFS rate in I-125 group vs. EBRT group (p = 0.002). NSD in 12-month PFS rate (p = 0.184). NSD in 12- (p = 0.839) and 24-month (p = 0.284) OS. NSD in median OS (p = 0.525) or PFS (p = 0.425). |
| Yondorf, 2020 [33] | Dosimetric differences between cesium-131 and iodine-125 brachytherapy for the treatment of resected brain metastases | Journal of Contemporary Brachytherapy | USA | Phase I/II Clinical Trial | 24 | 24 | Lung, breast, renal, melanoma, colon, cervix | De-Novo | Single | Cs-131 seeds | Dosimetric characteristics of Cs-131 compared to I-125 implants: Cs-131 exposes lower volumes of brain tissue to radiation, provides more uniform dosing, and targets the desired CTV volume more accurately. |
| Study | Title | Journal | Country | Study Design | Cohort Size | Number of Patients with BM Treated with Brachytherapy | Primary Tumor | De-Novo or Recurrent BM | Single or Multiple BM | Isotope and Formulation | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bernstein, 1995 [34] | Brachytherapy for recurrent single brain metastasis | Canadian Journal of Neurological Sciences | Canada | Retrospective | 10 | 10 | Lung, breast | Recurrent | Single | I-125 seeds | 1-year FFP: local 100%, regional 93.8%, distant 48.4%. 1-year OS 50%. RN 0% |
| Chen, 2022 [35] | Resection with intraoperative cesium-131 brachytherapy as salvage therapy for recurrent brain tumors | Journal of Neurosurgery | USA | Retrospective | 36 | 20 | Lung, breast, GI | Recurrent | Both | Cs-131 GammaTile | Local FFP 90.5%; regional FFP 90.5%; distant FFP 47.6%; median OS 26.7 months (range, 15.6–36.7); RN 11.9% |
| Cummins, 2022 [36] | Salvage Surgery for Local Control of Brain Metastases After Previous Stereotactic Radiosurgery: A Single-Center Series | World Neurosurgery | USA | Retrospective | 43 | 43 | Melanoma, NSCLC, breast, GI, renal | Recurrent | Both | Cs-131 seeds and I-125 seeds | Brachytherapy was associated with improved local control (HR, 0.15; 95% CI, 0.04–0.6; p = 0.008). For patients treated with SRS before salvage surgery, both brachytherapy (HR, 0.07; 95% CI, 0.01–0.39; p = 0.002) and postoperative adjuvant SRS (HR, 0.14; 95% CI, 0.02–1.00; p = 0.05) were associated with improved local control compared with no adjuvant radiation therapy. |
| Dharnipragada, 2023 [37] | GammaTile (GT) as a brachytherapy platform for rapidly growing brain metastasis | Neuro-Oncology Advances | USA | Retrospective | 10 | 10 | Lung, breast, melanoma, uterine | Recurrent | Single | Cs-131 GammaTile | 40% of patients showed symptomatic improvement. Remaining 60% showed stable neurologic conditions. |
| Nakaji, 2020 [17] | Resection and Surgically Targeted Radiation Therapy for the Treatment of Larger Recurrent or Newly Diagnosed Brain Metastasis: Results From a Prospective Trial | Cureus | USA | Prospective | 11 | 11 | Lung, breast | De-Novo and Recurrent | Both | Cs-131 GammaTile | 1-year local FFP 91%; median OS 9.5 months (range, 1.4–28); RN 0% |
| Romagna, 2016 [23] | Iodine-125 brachytherapy as upfront and salvage treatment for brain metastases: A comparative analysis | Strahlentherapie und Onkologie | Germany | Prospective | 43 | 43 | Lung, breast, GI, skin, prostate, renal, uterine, ovarian, MSK | De-Novo and Recurrent | Both | I-125 seeds | NSD in 1-year local/distant control rates after upfront and salvage SBT (94%/65% vs. 87%/57%, p = 0.45, respectively). Grade I/II toxicity seen in 2 patients after salvage SBT. |
| Ruge, Kickingereder, 2011 [38] | Stereotactic biopsy combined with stereotactic (125) iodine brachytherapy for diagnosis and treatment of locally recurrent single brain metastases | Journal of Neuro-Oncology | Germany | Retrospective | 30 | 30 | Breast, NSCLC, melanoma, CRC, renal, esophageal | Recurrent | Single | I-125 seeds | 27 treated with SBT for recurrent BM. Median survival: 14.8 months. 1-year actuarial local and distant relapse: 6.7% and 45.5%, respectively. No grade III/IV CNS toxicity, even among tumors > 30 mm. |
| Wernicke, Smith, 2017 [39] | Cesium-131 brachytherapy for recurrent brain metastases: durable salvage treatment for previously irradiated metastatic disease | Journal of Neurosurgery | USA | Retrospective | 13 | 13 | Lung, breast, melanoma, pancreatic, gastric | Recurrent | Both | Cs-131 seeds | 1-year FFP: local 83.3%, regional 55.6%, distant 46.7%; 1-year OS 24.7%; RN 6.7% |
| Wu, 2022 [40] | Salvage brachytherapy for multiply recurrent metastatic brain tumors: A matched case analysis | Neuro-Oncology Advances | USA | Retrospective | 14 | 14 | Lung, breast, melanoma | Recurrent | Both | Cs-131 seeds and I-125 seeds | SD in FFLR compared to prior treatments (median 7.39 vs. 5.51 months, p = 0.011) for multiply recurrent BMs. Compared to an independent matched cohort, brachytherapy demonstrated superior FFLR (median 8.49 vs. 1.61 months, p = 0.004) and longer median OS (11.07 vs. 5.93 months, p = 0.055). |
| NCT Number | Study Title | Study Sponsor | Study Design | Conditions | Summary | Interventions | Primary Outcomes |
|---|---|---|---|---|---|---|---|
| 04690348 | Intracavitary Carrier-Embedded Cs-131 Brachytherapy for Recurrent Brain Metastases: A Randomized Phase II Study | Memorial Sloan Kettering Cancer Center | RCT | Recurrent BM | Resection + Cs-131 vs. resection only | PROCEDURE: Craniotomy RADIATION: Cs-131 brachytherapy | FFLP |
| 04427384 | A Multicenter Observational Study of GammaTile Surgically Targeted Radiation Therapy (STaRT) in Intracranial Brain Neoplasms | GT Medical Technologies, Inc. | Prospective Cohort | Primary and Secondary Brain Tumors | Evaluate real-world clinical outcomes and patient-reported outcomes that measure the effectiveness and safety of STaRT post-resection. | DEVICE: Gamma Tile-Surgically Targeted Radiation Therapy (STaRT) | Surgical bed recurrence-free survival |
| 04365374 | Post-Surgical Stereotactic Radiotherapy Versus GammaTile-ROADS (Radiation One and Done Study) | GT Medical Technologies, Inc. | RCT | BM | This trial will be a randomized controlled study comparing the efficacy and safety of intraoperative radiation therapy using GammaTile versus SRS 3–4 weeks following metastatic tumor resection, which is the current standard of care. | DEVICE: Gamma Tile-Surgically Targeted Radiation Therapy (STaRT) RADIATION: Stereotactic Radiation Therapy | Surgical bed recurrence-free survival from the time of randomization up to 2 years post-radiation. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leskinen, S.; Ben-Shalom, N.; Ellis, J.; Langer, D.; Boockvar, J.A.; D’Amico, R.S.; Wernicke, A.G. Brachytherapy in Brain Metastasis Treatment: A Scoping Review of Advances in Techniques and Clinical Outcomes. Cancers 2024, 16, 2723. https://doi.org/10.3390/cancers16152723
Leskinen S, Ben-Shalom N, Ellis J, Langer D, Boockvar JA, D’Amico RS, Wernicke AG. Brachytherapy in Brain Metastasis Treatment: A Scoping Review of Advances in Techniques and Clinical Outcomes. Cancers. 2024; 16(15):2723. https://doi.org/10.3390/cancers16152723
Chicago/Turabian StyleLeskinen, Sandra, Netanel Ben-Shalom, Jason Ellis, David Langer, John A. Boockvar, Randy S. D’Amico, and A. Gabriella Wernicke. 2024. "Brachytherapy in Brain Metastasis Treatment: A Scoping Review of Advances in Techniques and Clinical Outcomes" Cancers 16, no. 15: 2723. https://doi.org/10.3390/cancers16152723
APA StyleLeskinen, S., Ben-Shalom, N., Ellis, J., Langer, D., Boockvar, J. A., D’Amico, R. S., & Wernicke, A. G. (2024). Brachytherapy in Brain Metastasis Treatment: A Scoping Review of Advances in Techniques and Clinical Outcomes. Cancers, 16(15), 2723. https://doi.org/10.3390/cancers16152723