

Does 5-ALA Fluorescence Microscopy Improve Complete Resectability in Cerebral/Cerebellar Metastatic Surgery? A Retrospective Data Analysis from a Cranial Center
 , , , ,
, , , , 
Abstract
Simple Summary
Abstract
1. Introduction
- 5-Aminolevulinic Acid (5-ALA)
- The purpose of the work
2. Materials and Methods
2.1. Ethics Vote
2.2. Inclusion of Patients
2.3. Data Acquisition
2.4. Preoperative Preparation
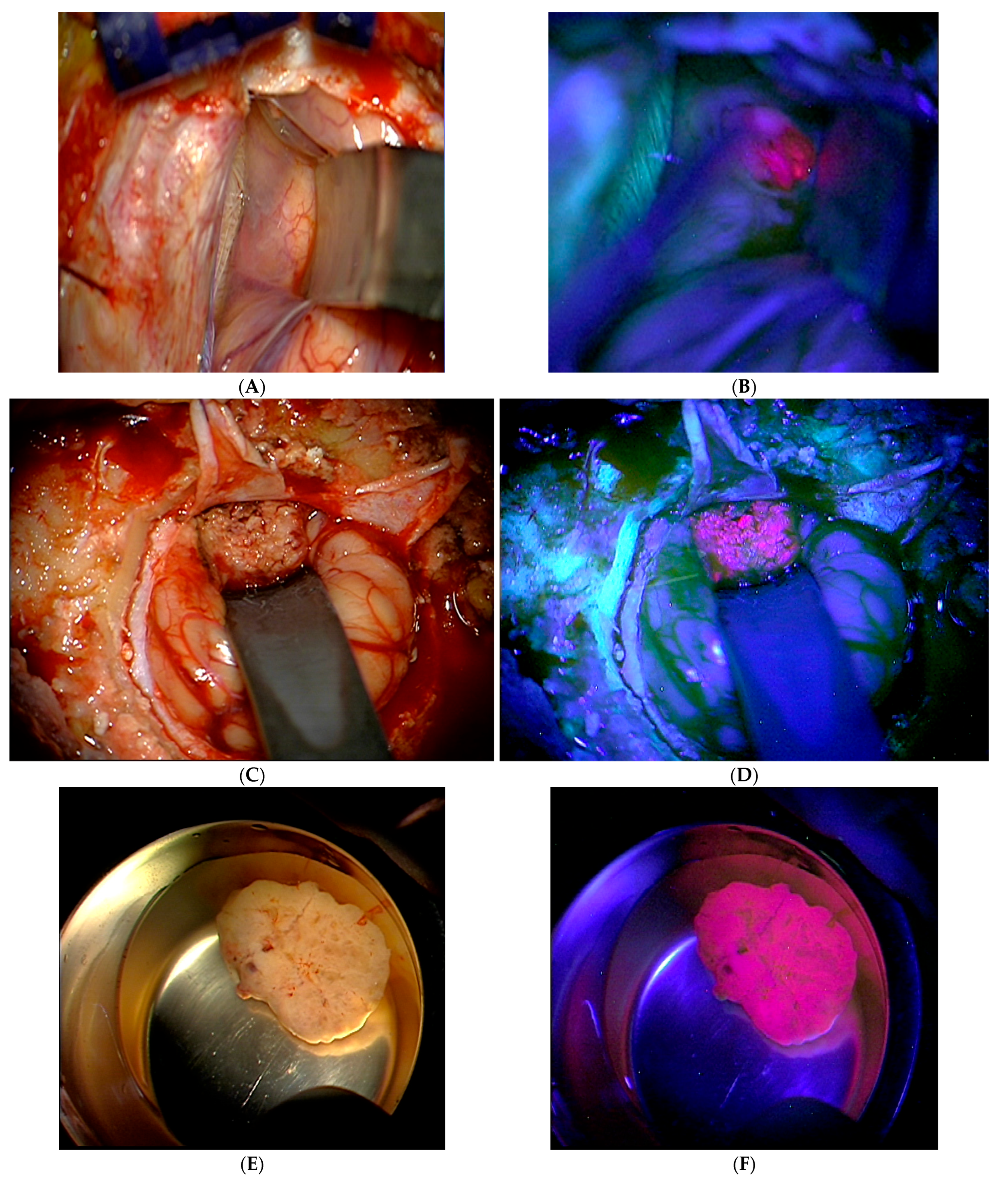
2.5. Intraoperative Procedure
2.6. Processing of the Material
2.7. Postoperative Evaluation and Follow-Up
2.8. Substance and Devices
- Gliolan 30 mg/mL powder for the preparation of a solution with a dosage of 20 mg/kg.
- Microsurgical tumor resection was performed using a surgical microscope with support for intraoperative visualization of fluorescent tumor tissue (OPMI® Pentero® 800 with BLUE® 400 function, Zeiss, Oberkochen, Germany).
- Magnetic resonance imaging was performed with a 1.5 Tesla MRI scanner (MAGNE-TOM®, Siemens, Munich, Germany) to assess the extent of the resection and as a postoperative follow-up.
2.9. Software and Program
2.10. Statistical Analysis
3. Results
3.1. Laboratory Values
3.2. The Incidence of the Primary Tumor and Subtypes
3.3. Correlation between the 5-ALA Fluorescence and the Primary Tumor
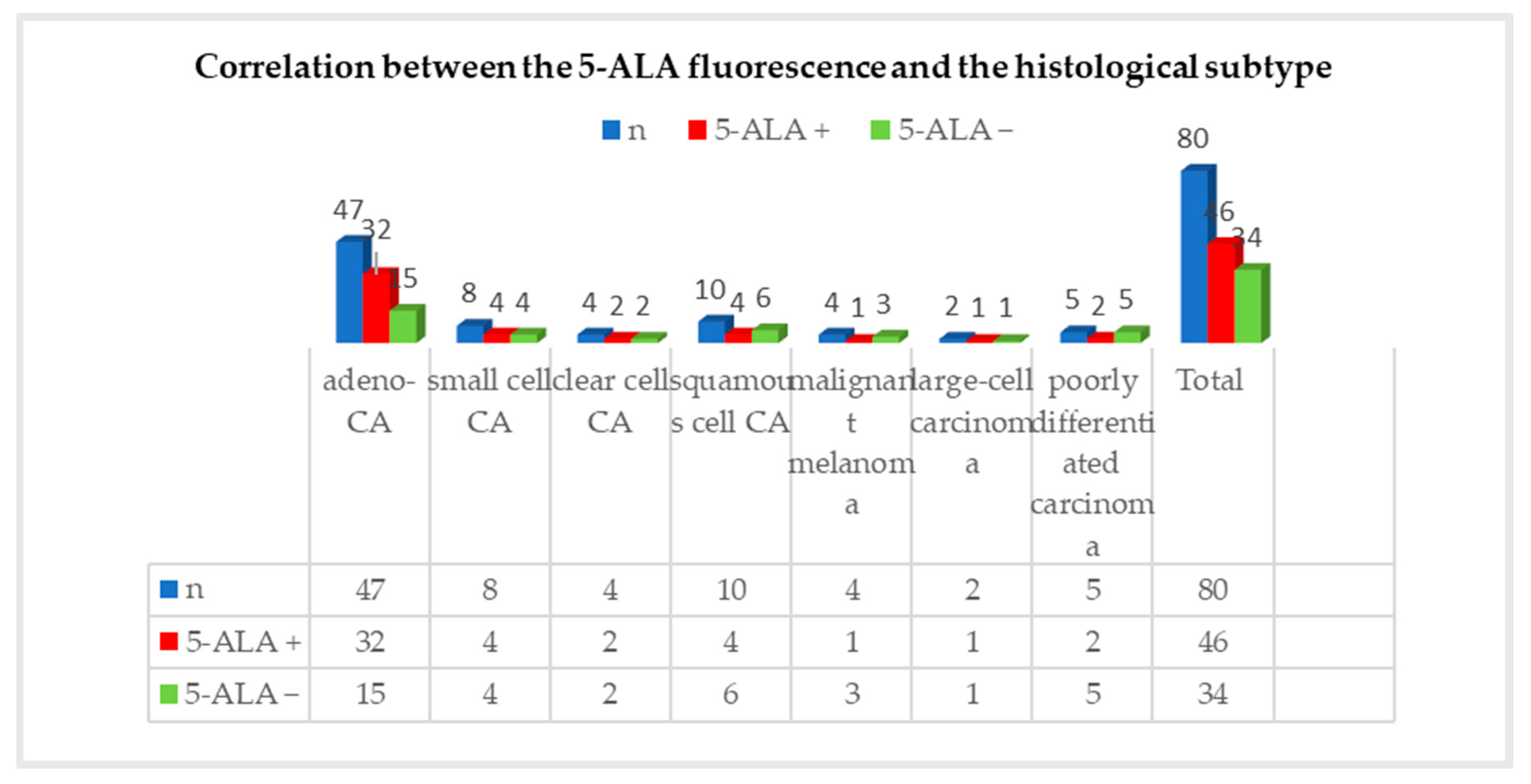
3.4. Correlation between the 5-ALA Fluorescence and the Histological Subtype
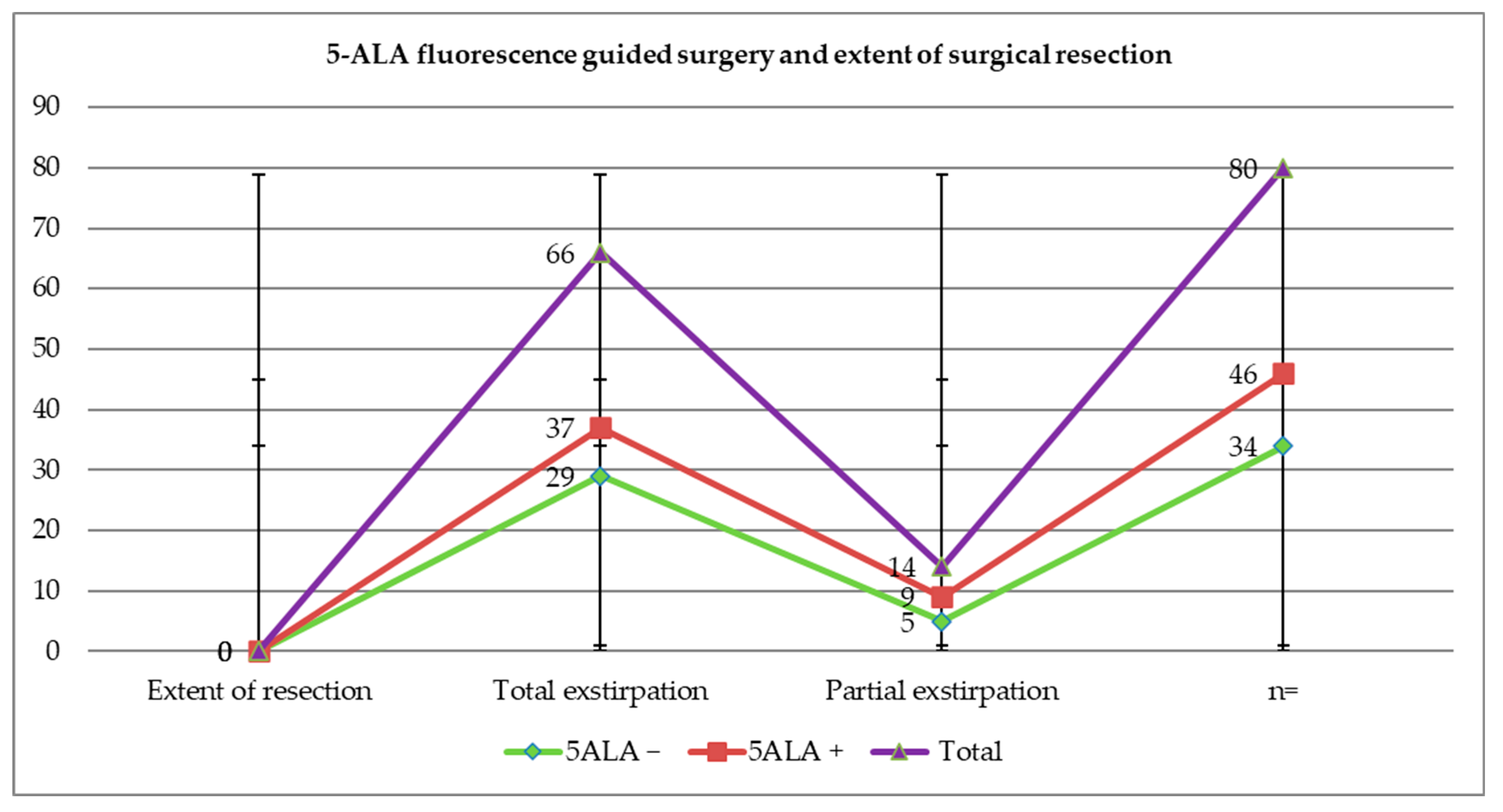
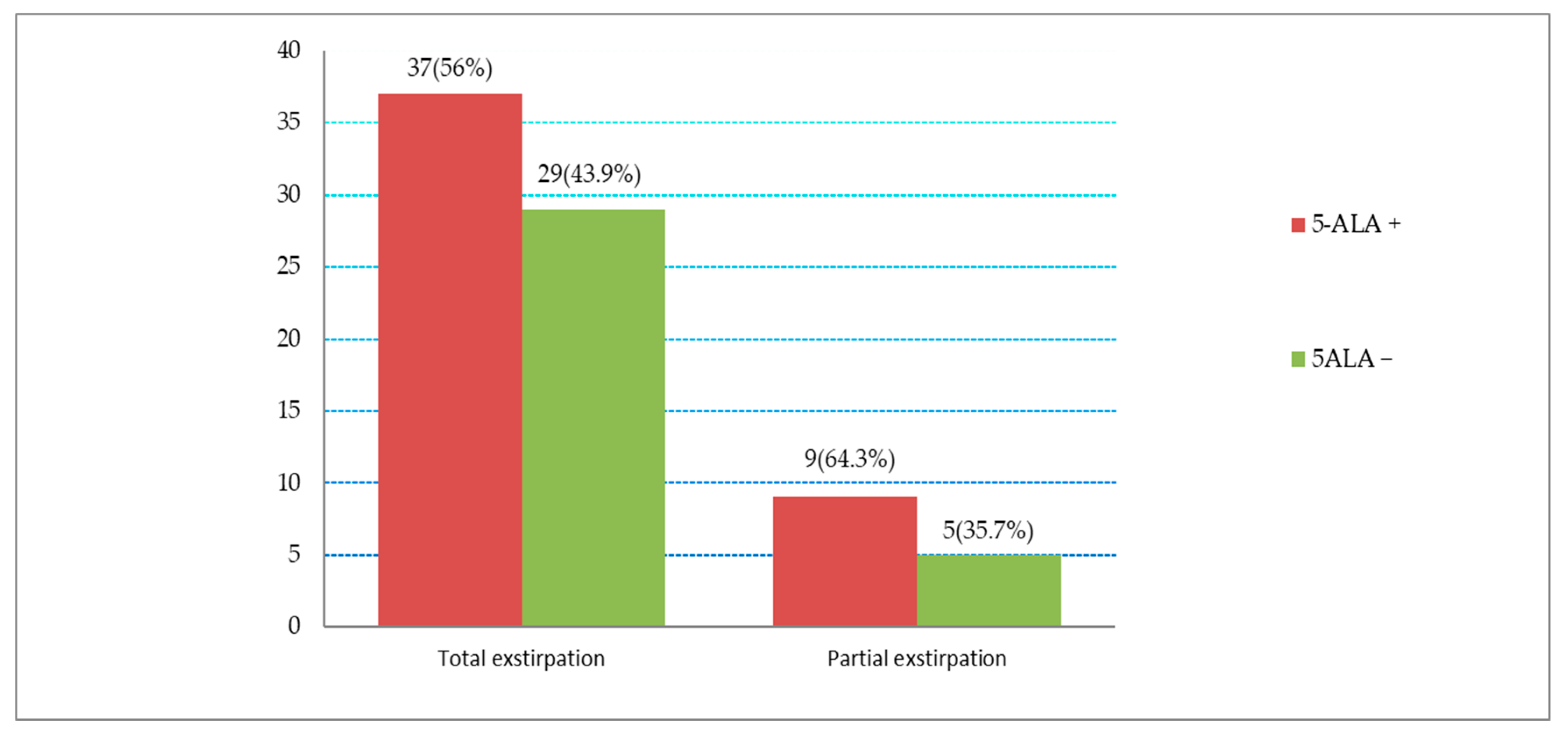
3.5. Correlation between 5-ALA Fluorescence and Extent of Surgical Resection
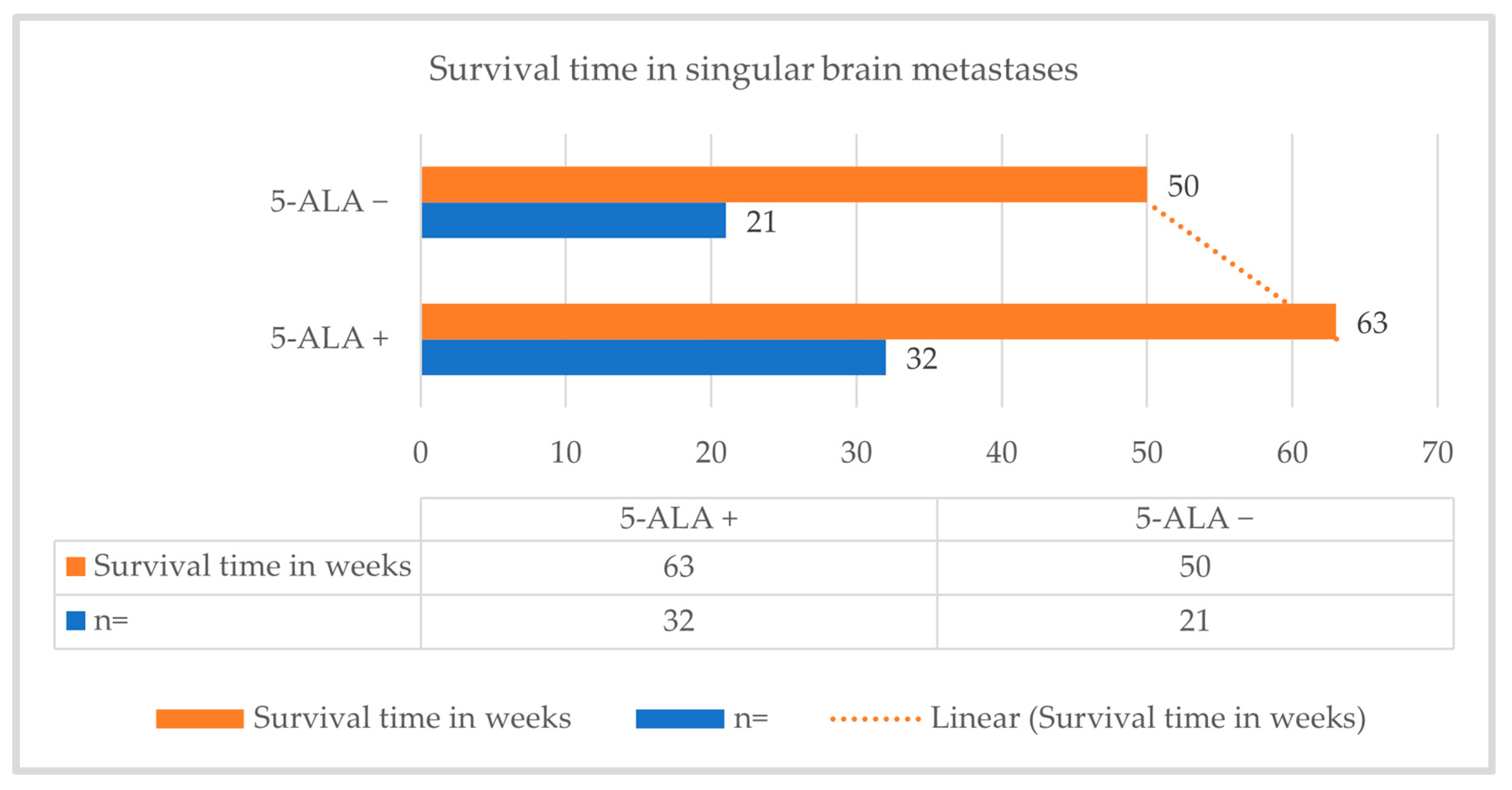
3.6. Progression-Free Survival (PFS) and Survival Rate
4. Discussion
4.1. A Summary of the Results
4.2. Use of 5-Aminolevulinic Acid in Neurosurgery
4.3. Correlation between 5-ALA Fluorescence and Primary Tumor Entity
4.4. Correlation between 5-ALA Fluorescence and Histological Subtype
4.5. Influence on Resectability
4.6. Influence on Median Survival Time
4.7. Biochemical Laboratory Parameters
4.8. Critical Discussion of the Limitations of This Study, Which Was Designed as a Retrospective Study
- One difficulty in the fluorescence diagnosis (absent, weak, or strong) was that its evaluation was very subjective depending on the surgeons. Here, to avoid subjectivity, spectroscopic measurement of PpIX concentration could be useful in the future, which has already been investigated by Kaneko et al. in a 2019 paper. Here, using a hyperspectral camera, they were able to demonstrate that both fluorescence intensity and PpIX concentration were higher centrally than peripherally in high-grade gliomas. They also observed, interestingly, that the marginal weak fluorescence peaked later than the central strong fluorescence (8–9 vs. 7–8 h) [43].
- To observe the long-term laboratory chemical change after 5-ALA administration, laboratory controls over time were lacking. The dosage of 5-ALA used in this work referred to the previously recommended 5-ALA dosage in glioblastoma surgery. Due to different tumor cell entities of the metastases, higher 5-ALA doses could be targeted.
- In this retrospective work, the interoperative adjuvant methods (such as neuromonitoring, neuronavigation, or ultrasound) were not regularly used, which could influence the intraoperative assessment of complete resection of the metastasis.
- The adenocarcinomas could be typed and classified more precisely after molecular analyses; here, more targeted investigations should be carried out for a possible correlation between the 5-ALA fluorescence and the adenocarcinoma with different histomorphological and genetic subtypes. In order to improve the study quality, based on the present retrospective design, the study protocols should be expanded accordingly in a future prospective study and the data collections should be performed in a larger patient population, taking into account the histomorphological and genetic subtypes of brain metastases.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fox, B.D.; Cheung, V.J.; Patel, A.J.; Suki, D.; Rao, G. Epidemiology of metastatic brain tumors. Neurosurg. Clin. N. Am. 2011, 22, 1–6. [Google Scholar] [CrossRef]
- Norden, A.D.; Wen, P.Y.; Kesari, S. Brain metastases. Curr. Opin. Neurol. 2005, 18, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Graus, F.; Walker, R.W.; Allen, J.C. Brain metastases in children. J. Pediatr. 1983, 103, 558–561. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.K.; Sinha, M.K. Multiple ring-enhancing lesions of the brain. J. Postgrad. Med. 2010, 56, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.E.; Robins, M.; Weinfeld, F.D. Epidemiology of brain tumors: The national survey of intracranial neoplasms. Neurology 1985, 35, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Nayak, L.; Lee, E.Q.; Wen, P.Y. Epidemiology of brain metastases. Curr. Oncol. Rep. 2012, 14, 48–54. [Google Scholar] [CrossRef]
- Pectasides, D.; Aravantinos, G.; Fountzilas, G.; Kalofonos, C.; Efstathiou, E.; Karina, M.; Pavlidis, N.; Farmakis, D.; Economopoulos, T.; Dimopoulos, M.A. Brain metastases from epithelial ovarian cancer. The Hellenic Cooperative Oncology Group (HeCOG) experience and review of the literature. Anticancer Res. 2005, 25, 3553–3558. [Google Scholar]
- Weller, M. S2k-Leitlinie Hirnmetastasen und Meningeosis Neoplastica der Deutschen Gesellschaft für Neurologie (DGN); AWMF: Frankfurt am Main, Germany, 2024; pp. 6–30. [Google Scholar]
- Hakyemez, B.; Erdogan, C.; Bolca, N.; Yildirim, N.; Gokalp, G.; Parlak, M. Evaluation of different cerebral mass lesions by perfusion-weighted MR imaging. J. Magn. Reson. Imaging 2006, 24, 817–824. [Google Scholar] [CrossRef]
- Potts, D.G.; Abbott, G.F.; Sneidern, J.V. von. National Cancer Institute study: Evaluation of computed tomography in the diagnosis of intracranial neoplasms. III. Metastatic tumors. Radiology 1980, 136, 657–664. [Google Scholar] [CrossRef]
- Eichler, A.F.; Loeffler, J.S. Multidisciplinary management of brain metastases. Oncologist 2007, 12, 884–898. [Google Scholar] [CrossRef]
- Schmieder, K.; Keilholz, U.; Combs, S. The Interdisciplinary Management of Brain Metastases. Dtsch. Arztebl. Int. 2016, 113, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Sperduto, C.M.; Watanabe, Y.; Mullan, J.; Hood, T.; Dyste, G.; Watts, C.; Bender, G.P.; Sperduto, P. A validation study of a new prognostic index for patients with brain metastases: The Graded Prognostic Assessment. J. Neurosurg. 2008, 109, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Sperduto, P.W.; Kased, N.; Roberge, D.; Xu, Z.; Shanley, R.; Luo, X.; Sneed, P.K.; Chao, S.T.; Weil, R.J.; Suh, J.; et al. Summary report on the graded prognostic assessment: An accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J. Clin. Oncol. 2012, 30, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Lin, N.U.; Lee, E.Q.; Aoyama, H.; Barani, I.J.; Barboriak, D.P.; Baumert, B.G.; Bendszus, M.; Brown, P.D.; Camidge, D.R.; Chang, S.M.; et al. Response assessment criteria for brain metastases: Proposal from the RANO group. Lancet Oncol. 2015, 16, e270–e278. [Google Scholar] [CrossRef]
- Hooda, J.; Alam, M.; Zhang, L. Measurement of Heme Synthesis Levels in Mammalian Cells. J. Vis. Exp. 2015, e51579. [Google Scholar] [CrossRef] [PubMed]
- Stummer, W.; Stocker, S.; Wagner, S.; Stepp, H.; Fritsch, C.; Goetz, C.; Goetz, A.E.; Kiefmann, R.; Reulen, H.J. Intraoperative detection of malignant gliomas by 5-aminolevulinic acid-induced porphyrin fluorescence. Neurosurgery 1998, 42, 518–525; discussion 525–526. [Google Scholar] [CrossRef] [PubMed]
- Ennis, S.R.; Novotny, A.; Xiang, J.; Shakui, P.; Masada, T.; Stummer, W.; Smith, D.E.; Keep, R.F. Transport of 5-aminolevulinic acid between blood and brain. Brain Res. 2003, 959, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Navone, N.M.; Polo, C.F.; Frisardi, A.L.; Andrade, N.E.; Battle, A.M. Heme biosynthesis in human breast cancer—Mimetic “in vitro” studies and some heme enzymic activity levels. Int. J. Biochem. 1990, 22, 1407–1411. [Google Scholar] [CrossRef] [PubMed]
- Krieg, R.C.; Messmann, H.; Rauch, J.; Seeger, S.; Knuechel, R. Metabolic Characterization of Tumor Cell–specific Protoporphyrin IX Accumulation After Exposure to 5-Aminolevulinic Acid in Human Colonic Cells. Photochem. Photobiol. 2002, 76, 518. [Google Scholar] [CrossRef]
- Stepp, H.; Stummer, W. 5-ALA in the management of malignant glioma. Lasers Surg. Med. 2018, 50, 399–419. [Google Scholar] [CrossRef]
- Hefti, M. Comment concerning: Intraoperative 5-aminolevulinic-acid-induced fluorescence in meningiomas, Acta Neurochir DOl 1O.1007/s00701-010-0708-4, Intratumoral heterogeneity and fluorescence intensity in meningioma after 5-ALA pretreatment. Acta Neurochir. 2011, 153, 959–960. [Google Scholar] [CrossRef] [PubMed]
- Marbacher, S.; Klinger, E.; Schwyzer, L.; Fischer, I.; Nevzati, E.; Diepers, M.; Roelcke, U.; Fathi, A.-R.; Coluccia, D.; Fandino, J. Use of fluorescence to guide resection or biopsy of primary brain tumors and brain metastases. Neurosurg. Focus 2014, 36, E10. [Google Scholar] [CrossRef]
- Kamp, M.A.; Grosser, P.; Felsberg, J.; Slotty, P.J.; Steiger, H.-J.; Reifenberger, G.; Sabel, M. 5-aminolevulinic acid (5-ALA)-induced fluorescence in intracerebral metastases: A retrospective study. Acta Neurochir. 2012, 154, 223–228; discussion 228. [Google Scholar] [CrossRef] [PubMed]
- Utsuki, S.; Miyoshi, N.; Oka, H.; Miyajima, Y.; Shimizu, S.; Suzuki, S.; Fujii, K. Fluorescence-guided resection of metastatic brain tumors using a 5-aminolevulinic acid-induced protoporphyrin IX: Pathological study. Brain Tumor Pathol. 2007, 24, 53–55. [Google Scholar] [CrossRef]
- Aminolevulinic Acid Hydrochloride, Known as ALA HCl (Gleolan, NX Development Corp.) as an Optical Imaging Agent Indicated in Patients with Gliomas 2017; pp. 4–12. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/aminolevulinic-acid-hydrochloride-known-ala-hcl-gleolan-nx-development-corp-optical-imaging-agent (accessed on 14 June 2024).
- Fritsch, C.; Verwohlt, B.; Bolsen, K.; Ruzicka, T.; Goerz, G. Influence of topical photodynamic therapy with 5-aminolevulinic acid on porphyrin metabolism. Arch. Dermatol. Res. 1996, 288, 517–521. [Google Scholar] [CrossRef]
- Stummer, W.; Pichlmeier, U.; Meinel, T.; Wiestler, O.D.; Zanella, F.; Reulen, H.-J. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: A randomised controlled multicentre phase III trial. Lancet Oncol. 2006, 7, 392–401. [Google Scholar] [CrossRef]
- Berghoff, A.S.; Ilhan-Mutlu, A.; Dinhof, C.; Magerle, M.; Hackl, M.; Widhalm, G.; Hainfellner, J.A.; Dieckmann, K.; Pichler, J.; Hutterer, M.; et al. Differential role of angiogenesis and tumour cell proliferation in brain metastases according to primary tumour type: Analysis of 639 cases. Neuropathol. Appl. Neurobiol. 2015, 41, e41–e55. [Google Scholar] [CrossRef]
- Koizumi, N.; Harada, Y.; Minamikawa, T.; Tanaka, H.; Otsuji, E.; Takamatsu, T. Recent advances in photodynamic diagnosis of gastric cancer using 5-aminolevulinic acid. World J. Gastroenterol. 2016, 22, 1289–1296. [Google Scholar] [CrossRef] [PubMed]
- Frei, K.A.; Bonel, H.M.; Frick, H.; Walt, H.; Steiner, R.A. Photodynamic detection of diseased axillary sentinel lymph node after oral application of aminolevulinic acid in patients with breast cancer. Br. J. Cancer 2004, 90, 805–809. [Google Scholar] [CrossRef]
- Kamp, M.A.; Fischer, I.; Bühner, J.; Turowski, B.; Cornelius, J.F.; Steiger, H.-J.; Rapp, M.; Slotty, P.J.; Sabel, M. 5-ALA fluorescence of cerebral metastases and its impact for the local-in-brain progression. Oncotarget 2016, 7, 66776–66789. [Google Scholar] [CrossRef]
- Shimizu, K.; Tamura, K.; Hara, S.; Inaji, M.; Tanaka, Y.; Kobayashi, D.; Sugawara, T.; Wakimoto, H.; Nariai, T.; Ishii, K.; et al. Correlation of Intraoperative 5-ALA-Induced Fluorescence Intensity and Preoperative 11C-Methionine PET Uptake in Glioma Surgery. Cancers 2022, 14, 1449. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.R.; Yatabe, Y.; Beer, D.G.; Powell, C.A.; Riely, G.J.; van Schil, P.E.; et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J. Thorac. Oncol. 2011, 6, 244–285. [Google Scholar] [CrossRef] [PubMed]
- Stummer, W.; Kamp, M.A. The importance of surgical resection in malignant glioma. Curr. Opin. Neurol. 2009, 22, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.; Kim, Y.Z.; Nam, B.H.; Shin, S.H.; Yang, H.S.; Lee, J.S.; Zo, J.I.; Lee, S.H. Reduced local recurrence of a single brain metastasis through microscopic total resection. J. Neurosurg. 2009, 110, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Ewelt, C.; Nemes, A.; Senner, V.; Wölfer, J.; Brokinkel, B.; Stummer, W.; Holling, M. Fluorescence in neurosurgery: Its diagnostic and therapeutic use. Review of the literature. J. Photochem. Photobiol. B 2015, 148, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Kamp, M.A.; Munoz-Bendix, C.; Mijderwijk, H.-J.; Turowski, B.; Dibué-Adjei, M.; von Saß, C.; Cornelius, J.F.; Steiger, H.-J.; Rapp, M.; Sabel, M. Is 5-ALA fluorescence of cerebral metastases a prognostic factor for local recurrence and overall survival? J. Neurooncol. 2019, 141, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Soffietti, R.; Cornu, P.; Delattre, J.Y.; Grant, R.; Graus, F.; Grisold, W.; Heimans, J.; Hildebrand, J.; Hoskin, P.; Kalljo, M.; et al. EFNS Guidelines on diagnosis and treatment of brain metastases: Report of an EFNS Task Force. Eur. J. Neurol. 2006, 13, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Schwake, M.; Kaneko, S.; Suero Molina, E.; Müther, M.; Schipmann, S.; Köchling, M.; Brentrup, A.; Stummer, W. Spectroscopic measurement of 5-ALA-induced intracellular protoporphyrin IX in pediatric brain tumors. Acta Neurochir. 2019, 161, 2099–2105. [Google Scholar] [CrossRef] [PubMed]
- Gliolan, INN-5-Aminolevulinic Acid Hydrochloride 2007; pp. 3–4. Available online: https://ec.europa.eu/health/documents/community-register/2012/20120830123873/anx_123873_en.pdf (accessed on 14 June 2024).
- Teixidor, P.; Arráez, M.Á.; Villalba, G.; Garcia, R.; Tardáguila, M.; González, J.J.; Rimbau, J.; Vidal, X.; Montané, E. Safety and Efficacy of 5-Aminolevulinic Acid for High Grade Glioma in Usual Clinical Practice: A Prospective Cohort Study. PLoS ONE 2016, 11, e0149244. [Google Scholar] [CrossRef]
- Kaneko, S.; Suero Molina, E.; Ewelt, C.; Warneke, N.; Stummer, W. Fluorescence-Based Measurement of Real-Time Kinetics of Protoporphyrin IX After 5-Aminolevulinic Acid Administration in Human In Situ Malignant Gliomas. Neurosurgery 2019, 85, E739–E746. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Score = 0 | Score = 0.5 | Score = 1 |
|---|---|---|---|
| age (yrs) | >60 | 50–59 | <50 |
| KPS score | <70 | 70–80 | 90–100 |
| number of CNS metastases | >3 | 2–3 | 1 |
| extracranial metastases | yes | no |
| Parameter | Source of Selectivity | Effect |
|---|---|---|
| 1 | Blood brain barrier leakage in glioma | Normal brain fairly protected from 5-ALA |
| 2 | Increased activity of GABA, pepT1, pepT2 transporters | Uptake of 5-ALA in glioma cells increased |
| 3 | Increased activity of ALA-D | More of PpIX-precursor PBG synthesized |
| 4 | Increased activity of PBG-D | More of PpIX-precursor HMB synthesized |
| 5 | Reduced ferrochelatase activity | Accumulation of PpIX as one of the substrates of this step |
| 6 | Reduced availability of Fe2+ | Accumulation of PpIX as the other substrate of this step |
| 7 | ABCB6-transporter | Transport of CPgen III into mitochondria |
| 8 | ABCG2-transporter | Transport of PpIX from mitochondria into the cytosol, but also loss of PpIX through the plasma membrane |
| Parameter | n (%) |
|---|---|
| number of patients | 73 |
| number of cases | 80 |
| age: | |
| Mean | 63 years |
| age range | 33–83 years |
| gender: | |
| Female | 35 (47.9%) |
| Male | 38 (52.1%) |
| primary tumor: | |
| bronchial carcinoma | 46 (57.5%) |
| breast carcinoma | 15 (18.8%) |
| gastrointestinal carcinoma | 9 (11.3%) |
| renal cell carcinoma | 5 (6.3%) |
| malignant melanoma | 4 (5.0%) |
| gynecological carcinoma | 1 (1.3%) |
| Histology: | |
| Adenocarcinoma | 47 (58.7%) |
| squamous cell carcinoma | 10 (12.5%) |
| small cell carcinoma | 8 (10.0%) |
| malignant melanoma | 4 (5.0%) |
| clear cell carcinoma | 4 (5.0%) |
| giant cell carcinoma | 2 (2.5%) |
| poorly differentiated brain metastases from carcinoma | 5 (6.3%) |
| localization of the metastasis: | |
| Supratentorial | 60 (75.0%) |
| Infratentorial | 17 (21.2%) |
| supra/infratentorial | 3 (3.8%) |
| eloquent area | 39 (49.0%) |
| non-eloquent area | 41 (51.0%) |
| number of metastases: | |
| singular | 58 (72.6%) |
| multiple | 22 (27.4%) |
| 5-ALA fluorescence: | |
| positive | 46 (57.5%) |
| negative | 34 (42.5%) |
| degree of surgical resection: | |
| total | 66 (82.5%) |
| partial | 14 (17.5%) |
| incidence of complete resection of the metastasis: | |
| total extirpation | 66 (82.5%) |
| 5-ALA positive | 37 (56.1%) |
| 5-ALA negative | 29 (43.9%) |
| eloquent area | 31 (46.9%) |
| non-eloquent area | 35 (53.1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarkis, H.M.; Zawy Alsofy, S.; Stroop, R.; Lewitz, M.; Schipmann, S.; Unnewehr, M.; Paulus, W.; Nakamura, M.; Ewelt, C. Does 5-ALA Fluorescence Microscopy Improve Complete Resectability in Cerebral/Cerebellar Metastatic Surgery? A Retrospective Data Analysis from a Cranial Center. Cancers 2024, 16, 2242. https://doi.org/10.3390/cancers16122242
Sarkis HM, Zawy Alsofy S, Stroop R, Lewitz M, Schipmann S, Unnewehr M, Paulus W, Nakamura M, Ewelt C. Does 5-ALA Fluorescence Microscopy Improve Complete Resectability in Cerebral/Cerebellar Metastatic Surgery? A Retrospective Data Analysis from a Cranial Center. Cancers. 2024; 16(12):2242. https://doi.org/10.3390/cancers16122242
Chicago/Turabian StyleSarkis, Hraq Mourad, Samer Zawy Alsofy, Ralf Stroop, Marc Lewitz, Stephanie Schipmann, Markus Unnewehr, Werner Paulus, Makoto Nakamura, and Christian Ewelt. 2024. "Does 5-ALA Fluorescence Microscopy Improve Complete Resectability in Cerebral/Cerebellar Metastatic Surgery? A Retrospective Data Analysis from a Cranial Center" Cancers 16, no. 12: 2242. https://doi.org/10.3390/cancers16122242
APA StyleSarkis, H. M., Zawy Alsofy, S., Stroop, R., Lewitz, M., Schipmann, S., Unnewehr, M., Paulus, W., Nakamura, M., & Ewelt, C. (2024). Does 5-ALA Fluorescence Microscopy Improve Complete Resectability in Cerebral/Cerebellar Metastatic Surgery? A Retrospective Data Analysis from a Cranial Center. Cancers, 16(12), 2242. https://doi.org/10.3390/cancers16122242