

Principles and Clinical Application of Free-Style Capillary Perforator-Based Flap for Coverage of Facial Skin Cancer Defects


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Operative Technique
- The presence of sufficient tissue around the defect can be determined with a finger-pinching method.
- For perforator selection, it is not necessary to choose one detectable with a hand-held Doppler.
- The direction of the patient’s wrinkles and areas that can be hidden in the relaxed tissue around the defect should be considered.
- The width of the skin flap should account for the defect shape, changing from round to oval when the PBIF donor site is lifted and set around the defect.
- A slightly smaller width of the skin flap, about 5–10 mm, is enough to fit the defect.
- The length of the skin flap should be longer than the defect by about 1.0–2.0 cm because the defect changes to an oval shape.
- When elevating the skin flap, the proximal part of the flap should remain attached to the muscle about 1 cm in diameter without complete isolation.
- In the proximal part of the elevated flap, the subcutaneous layer can be sufficiently dissected to allow easy rotation of the flap.
- It is advantageous to design the axis of the skin flap to rotate within 90 degrees. However, considering scars or wrinkle lines, the axis of rotation can be increased up to 180 degrees.
3. Results
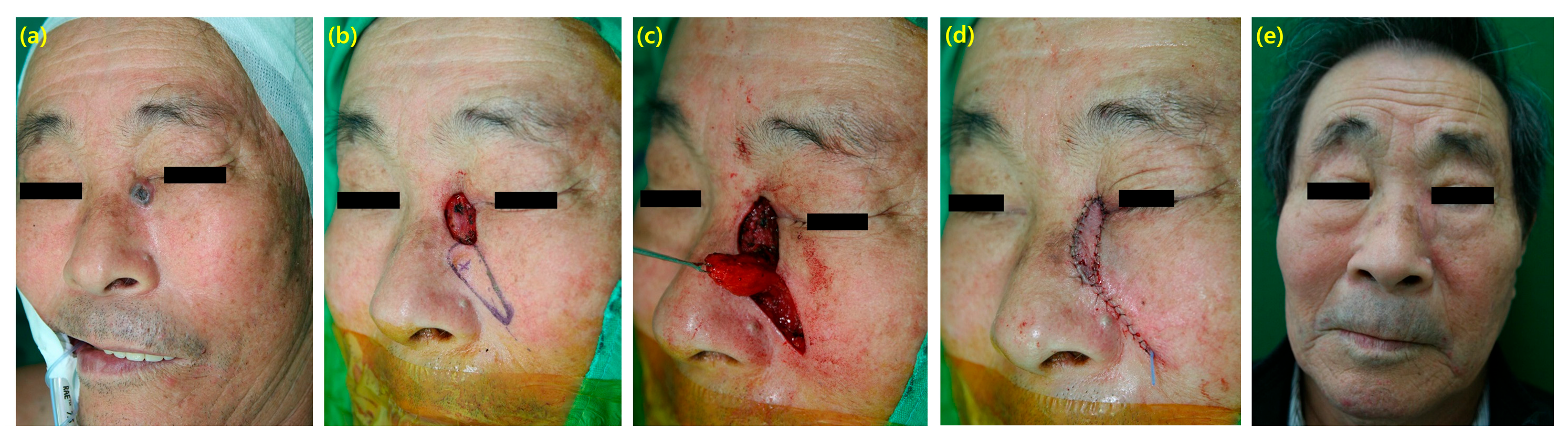
3.1. Case 1
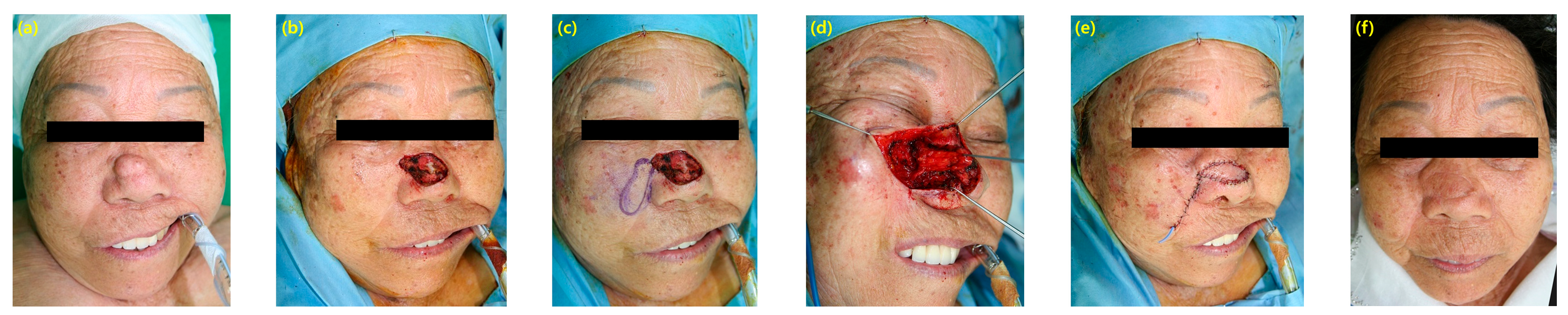
3.2. Case 2
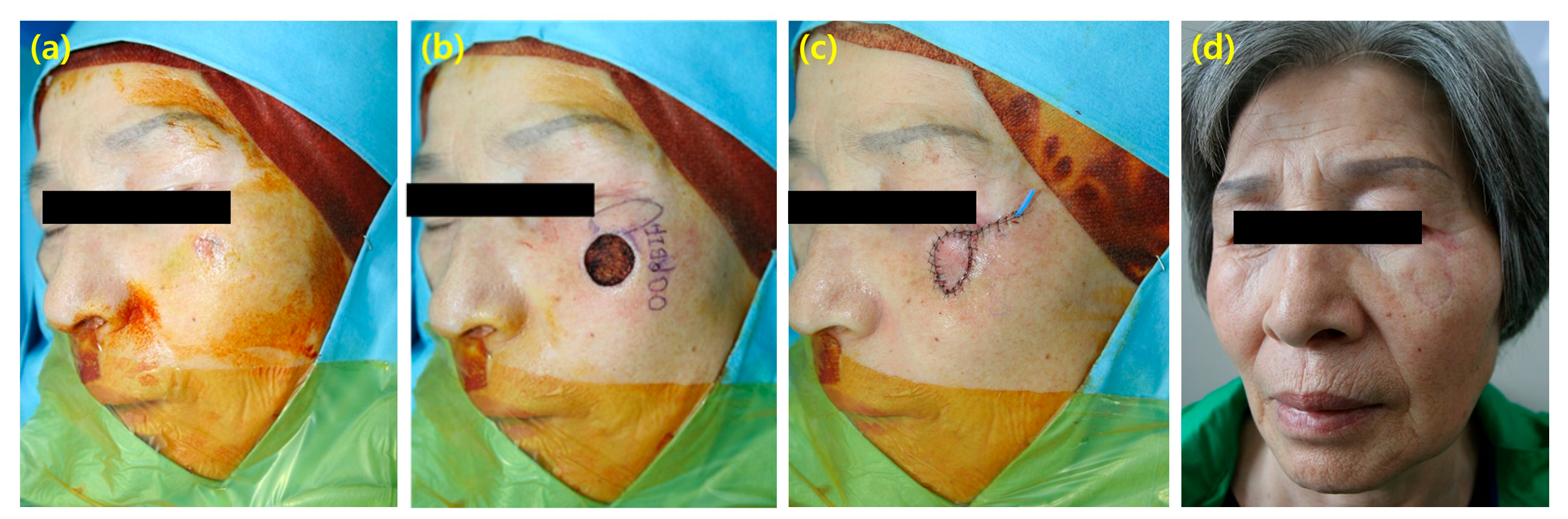
3.3. Case 3
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moon, P.; Mishra, G.S.; Patel, J.V. Reconstruction of Head and Neck Defects Using Medial Sural Artery Perforator Free Flap. Indian J. Otolaryngol. Head. Neck Surg. 2023, 75, 3176–3179. [Google Scholar] [CrossRef] [PubMed]
- Brenner, M.J.; Moyer, J.S. Skin and Composite Grafting Techniques in Facial Reconstruction for Skin Cancer. Facial Plast. Surg. Clin. North Am. 2017, 25, 347–363. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Heo, E.P.; Choi, J.H.; Cho, H.C.; Kim, S.H.; Xu, L.; Lee, Y.; Choi, T.H.; Kim, S. Reconstruction of defects after excision of facial skin cancer using a venous free flap. Ann. Plast. Surg. 2011, 67, 608–611. [Google Scholar] [CrossRef] [PubMed]
- Helmy Ali, Y.; Farahat Mohamed, A.; Nasef, M.A.; Abu-Elsoud, A.; Dahi, A.; Hossni, M.; Ouf, M.O.; Zayed, T.; ELBatawy, A.; Farid, M.; et al. Facial skin cancer reconstructive and cosmetic outcomes: Analysis with algorithm for its management. J. Cosmet. Dermatol. 2020, 19, 1182–1190. [Google Scholar] [CrossRef] [PubMed]
- Drake, V.E.; Moyer, J.S. The Measure of a Scar: Patient Perceptions and Scar Optimization after Skin Cancer Reconstruction. Facial Plast. Surg. 2023, 39, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Thiem, D.G.E.; Scharr, K.; Pabst, A.M.; Saka, B.; Kammerer, P.W. Facial cutaneous squamous cell carcinoma—Microscopic safety margins and their impact on developing local recurrences. J. Cranio-Maxillofac. Surg. 2020, 48, 49–55. [Google Scholar] [CrossRef]
- Wei, M.Z.; Luo, Q.N.; Huang, J.Y.; Yan, W.J.; Li, X. The clinical features and surgical treatment of facial basal cell carcinoma. J. Clin. Otorhinolaryngol. Head Neck Surg. 2018, 32, 279–281. [Google Scholar] [CrossRef] [PubMed]
- Namgoong, S.; Lee, K.I.; Han, S.K.; Jeong, S.H.; Dhong, E.S. Staged Excision Technique to Reduce Scar Length. J. Plast. Reconstr. Aesthet. Surg. 2022, 75, 2775–2783. [Google Scholar] [CrossRef] [PubMed]
- Schrudde, J.; Beinhoff, U. Reconstruction of the face by means of the angle-rotation flap. Aesthetic Plast. Surg. 1987, 11, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Larrabee, Y.C.; Phillips, D.J.; Sclafani, A.P. Trends in Nasal Subunit Reconstruction by Facial Plastic and Reconstructive Surgeons. Facial Plast. Surg. 2017, 33, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Jang, U.; Baek, S.O.; Lee, J.Y. Full-Thickness Skin Graft according to Surrounding Relaxed Skin Tension Line Improves Scar Quality in Facial Defect Coverage: A Retrospective Comparative Study. Biomed. Res. Int. 2021, 2021, 7398090. [Google Scholar] [CrossRef] [PubMed]
- Salgarelli, A.C.; Cangiano, A.; Sartorelli, F.; Bellini, P.; Collini, M. The bilobed flap in skin cancer of the face: Our experience on 285 cases. J. Cranio-Maxillofac. Surg. 2010, 38, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Kirazoglu, A.; Cengiz, F.P.; Kelahmetoglu, O.; Guneren, E. Revisiting the Limberg flap for central midface reconstruction in elderly patients. Dermatol. Ther. 2020, 33, e13377. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Hong, J.W.; Lee, W.J.; Yun, I.S. Perforating patterns of cutaneous perforator vessels in anterolateral thigh flaps for head and neck reconstruction and clinical outcomes. Arch. Craniofac Surg. 2022, 23, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Zhang, Y.; Chen, L.; Wang, H.; Zhou, Y.; Guo, Y.; Dong, D.; Wang, W.; Liu, T. The Facial Artery Perforator Flap for Reconstruction of Facial Defects: Surgical Pearls and Clinical Series. J. Craniofac Surg. 2024, 35, e227–e230. [Google Scholar] [CrossRef] [PubMed]
- Lyons, A.J. Perforator flaps in head and neck surgery. Int. J. Oral Maxillofac. Surg. 2006, 35, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Ercan, A.; Ercan, L.D.; Demiroz, A. Nasolabial Perforator Flap: A Multi-Tool for Reconstruction of Facial Units. J. Craniofac Surg. 2020, 31, 1042–1045. [Google Scholar] [CrossRef] [PubMed]
- Wallner, J.; Rieder, M.; Schwaiger, M.; Remschmidt, B.; Zemann, W.; Pau, M. Donor Site Morbidity and Quality of Life after Microvascular Head and Neck Reconstruction with a Chimeric, Thoracodorsal, Perforator-Scapular Flap Based on the Angular Artery (TDAP-Scap-aa Flap). J. Clin. Med. 2022, 11, 4876. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.J.; Huang, H.H.; Kim, Y.D.; Wu, Z.Y.; Luo, S.K.; Wei, Y.; Wang, J.X. A new skin flap from the zygomaticotemporal region: Anatomical study and clinical application to eyelid reconstruction. J. Plast. Reconstr. Aesthet. Surg. 2022, 75, 4423–4431. [Google Scholar] [CrossRef] [PubMed]
- Zapata-Ospina, A.; Chen, J.; Tee, R.; Jeng, S.F.; Karki, B.; Shih, H.S. Harvesting the anterolateral thigh flap with non-sizable perforators. J. Plast. Reconstr. Aesthet. Surg. 2021, 74, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- Visconti, G.; Salgarello, M. Free-style Capillary Perforator-Based Island Flaps for Reconstruction of Skin Cancer Defects of the Face, Body, and Extremities. Ann. Plast. Surg. 2018, 81, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Hyakusoku, H.; Ono, S. The History of Propeller Flaps. Semin. Plast. Surg. 2020, 34, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Teo, T.C. The propeller flap concept. Clin. Plast. Surg. 2010, 37, 615–626. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.N.; Tang, Y.X.; Guo, T.; Hu, H.D.; Ma, Q.; Yu, B.F.; Zhao, X.D. Subcutaneous pedicled propeller flap for reconstructing the large eyelid defect due to excision of malignancies or trauma. Sci. Rep. 2022, 12, 4891. [Google Scholar] [CrossRef] [PubMed]
- Rajak, S.N.; Huilgol, S.C.; Murakami, M.; Selva, D. Propeller flaps in eyelid reconstruction. Eye 2018, 32, 1259–1264. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.T.; Kim, Y.H.; Naidu, S. Perfecting the design of the gluteus maximus perforator-based island flap for coverage of buttock defects. Plast. Reconstr. Surg. 2010, 125, 1744–1751. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Lee, W.M.; Kim, J.T.; Kim, Y.H. Vulvar and vaginal reconstruction using the "angel wing" perforator-based island flap. Gynecol. Oncol. 2015, 137, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Kim, Y.H.; Kim, J.T. Angular artery perforator-based transposition flap for the reconstruction of midface defect. Int. J. Dermatol. 2012, 51, 1366–1370. [Google Scholar] [CrossRef] [PubMed]
- Brunetti, B.; Tenna, S.; Aveta, A.; Segreto, F.; Persichetti, P. Angular artery perforator flap for reconstruction of nasal sidewall and medial canthal defects. Plast. Reconstr. Surg. 2012, 130, 627e–628e. [Google Scholar] [CrossRef] [PubMed]
- Bordianu, A.; Bobirca, F. Facial skin cancer surgery under local anesthesia. J. Med. Life 2018, 11, 231–237. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| N = 32 | (%) | |
|---|---|---|
| Gender | ||
| Male | 12 | 37.5 |
| Female | 20 | 62.5 |
| Age (years) | ||
| Median | 63.6 | |
| Range | 29–94 | |
| Anesthesia | ||
| General | 20 | 62.5 |
| Local | 12 | 37.5 |
| Diagnosis | ||
| Basal cell carcinoma | 20 | 62.5 |
| Squamous cell carcinoma | 10 | 31.25 |
| Follicular lymphoma | 1 | 3.125 |
| Sebaceous carcinoma | 1 | 3.125 |
| Flap size (cm2) | ||
| Median | 7.63 | |
| Range | 3 × 1.5–7 × 3 | |
| Complication | ||
| Wound disruption | 1 | |
| Hypertrophic scar | 1 | |
| Follow-up months (median) | 31 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shim, H.-S.; Ryoo, H.-J.; Choi, J.-S.; Park, J.-A.; Kim, Y.-H. Principles and Clinical Application of Free-Style Capillary Perforator-Based Flap for Coverage of Facial Skin Cancer Defects. Cancers 2024, 16, 2206. https://doi.org/10.3390/cancers16122206
Shim H-S, Ryoo H-J, Choi J-S, Park J-A, Kim Y-H. Principles and Clinical Application of Free-Style Capillary Perforator-Based Flap for Coverage of Facial Skin Cancer Defects. Cancers. 2024; 16(12):2206. https://doi.org/10.3390/cancers16122206
Chicago/Turabian StyleShim, Hyung-Sup, Hyun-Jung Ryoo, Jae-Seon Choi, Ji-Ah Park, and Youn-Hwan Kim. 2024. "Principles and Clinical Application of Free-Style Capillary Perforator-Based Flap for Coverage of Facial Skin Cancer Defects" Cancers 16, no. 12: 2206. https://doi.org/10.3390/cancers16122206
APA StyleShim, H.-S., Ryoo, H.-J., Choi, J.-S., Park, J.-A., & Kim, Y.-H. (2024). Principles and Clinical Application of Free-Style Capillary Perforator-Based Flap for Coverage of Facial Skin Cancer Defects. Cancers, 16(12), 2206. https://doi.org/10.3390/cancers16122206