
Intralesional Vessel Diameter Measured by Optical Coherence Tomography Angiography Could Improve the Differential Diagnosis of Small Melanocytic Choroidal Lesions

 , , , , , and
, , , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shields, C.L.; Furuta, M.; Thangappan, A.; Nagori, S.; Mashayekhi, A.; Lally, D.R.; Kelly, C.C.; Rudich, D.S.; Nagori, A.; Wakade, O.A.; et al. Metastasis of uveal melanoma millimeter-by-millimeter in 8033 consecutive eyes. Arch. Ophthalmol. 2009, 127, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.D.; Raval, V.; Wrenn, J.; Zabor, E.C. Small Choroidal Melanoma: Outcomes After Surveillance Versus Immediate Treatment. Am. J. Ophthalmol. 2022, 241, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Gass, J.D.M. Problems in the differential diagnosis of choroidal nevi and malignant melanomas. Trans. Am. Acad. Ophthalmol. Otolaryngol. 1977, 83, 19–48. [Google Scholar]
- Collaborative Ocular Melanoma Study Group. Factors predictive of growth and treatment of small choroidal melanoma: COMS report no. 5. Arch. Ophthalmol. 1997, 115, 1537–1544. [Google Scholar] [CrossRef] [PubMed]
- Murray, T.G.; Sobrin, L. The case for observational management of suspected small choroidal melanoma. Arch. Ophthalmol. 2006, 124, 1342–1344. [Google Scholar] [CrossRef] [PubMed]
- Collaborative Ocular Melanoma Study Group. Mortality in patients with small choroidal melanoma. COMS report no. 4. The Collaborative Ocular Melanoma Study Group. Arch. Ophthalmol. 1997, 115, 886–893. [Google Scholar] [CrossRef]
- Vigués-Jorba, L.; Morwani, R.; Lorenzo, D.; Baradad-Jurjo, M.C.; Arias, L.; Piulats, J.M.; Gutierrez, C.; Cobos, E.; Garcia-Bru, P.; Caminal, J.M. Survival in small choroidal melanocytic lesions with risk factors managed by initial observation until detection of tumour growth. Clin. Exp. Ophthalmol. 2021, 49, 251–259. [Google Scholar] [CrossRef]
- Shields, J.A. Treating some small melanocytic choroidal lesions without waiting for growth. Arch. Ophthalmol. 2006, 124, 1344–1346. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.L.; Dalvin, L.A.; Yu, M.D.; Ancona-Lezama, D.; Di Nicola, M.; Williams, B.K.; Lucio-Alvarez, J.A.; Mae, S.; Maloney, S.M.; Welch, R.J.; et al. Choroidal Nevus Transformation into Melanoma per Millimeter Increment in Thickness using Multimodal Imaging in 2355 Cases: The 2019 wendell l. hughes lecture. Retina 2019, 39, 1852–1860. [Google Scholar] [CrossRef]
- Damato, B. Ocular treatment of choroidal melanoma in relation to the prevention of metastatic death—A personal view. Prog. Retin. Eye Res. 2018, 66, 187–199. [Google Scholar] [CrossRef]
- Folberg, R.; Rummelt, V.; Parys-Van Ginderdeuren, R.; Hwang, T.; Woolson, R.F.; Pe’er, J.; Gruman, L.M. The Prognostic Value of Tumor Blood Vessel Morphology in Primary Uveal Melanoma. Ophthalmology 1993, 100, 1389–1398. [Google Scholar] [CrossRef]
- Wang, J.C.; Miller, J.B. Optical Coherence Tomography Angiography: Review of Current Technical Aspects and Applications in Chorioretinal Disease. Semin. Ophthalmol. 2019, 34, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Naseripour, M.; Ghasemi Falavarjani, K.; Mirshahi, R.; Sedaghat, A. Optical coherence tomography angiography (OCTA) applications in ocular oncology. Eye 2020, 34, 1535–1545. [Google Scholar] [CrossRef]
- Maloca, P.; Gyger, C.; Hasler, P.W. A pilot study to image the vascular network of small melanocytic choroidal tumors with speckle noise-free 1050-nm swept source optical coherence tomography (OCT choroidal angiography). Graefe’s Arch. Clin. Exp. Ophthalmol. 2016, 254, 1201–1210. [Google Scholar] [CrossRef]
- Ali, Z.C.; Gray, J.; Balaskas, K. Features of choroidal naevi on swept source optical coherence tomography angiography and structural reverse flow optical coherence tomography. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 1319–1323. [Google Scholar] [CrossRef] [PubMed]
- Cennamo, G.; Romano, M.R.; Breve, M.A.; Velotti, N.; Reibaldi, M.; de Crecchio, G.; Cennamo, G. Evaluation of choroidal tumors with optical coherence tomography: Enhanced depth imaging and OCT-angiography features. Eye 2017, 31, 906–915. [Google Scholar] [CrossRef] [PubMed]
- Ghassemi, F.; Mirshahi, R.; Fadakar, K. Optical coherence tomography angiography in choroidal melanoma and nevus. Clin. Ophthalmol. 2018, 12, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Toledo, J.J.; Asencio, M.; García, J.R.; Morales, L.A.; Tomkinson, C.; Cajigal, C. OCT Angiography: Imaging of Choroidal and Retinal Tumors. Ophthalmol. Retin. 2018, 2, 613–622. [Google Scholar] [CrossRef]
- Lee, M.D.; Kaidonis, G.; Kim, A.Y.; Shields, R.A.; Leng, T. En Face Optical Coherence Tomography Angiography Imaging Versus Fundus Photography in the Measurement of Choroidal Nevi. Ophthalmic Surg. Lasers Imaging Retin. 2017, 48, 741–747. [Google Scholar] [CrossRef]
- Pellegrini, M.; Staurenghi, G.; Preziosa, C. Clinical Applications of Optical Coherence Tomography Angiography in Ocular Oncology: Pearls and Pitfalls. Ocul. Oncol. Pathol. 2022, 8, 79–87. [Google Scholar] [CrossRef]
- Garcia-Arumi Fuste, C.; Peralta Iturburu, F.; Garcia-Arumi, J. Is optical coherence tomography angiography helpful in the differential diagnosis of choroidal nevus versus melanoma? Eur. J. Ophthalmol. 2020, 30, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Gönen, B.; Hepokur, M.; Güleser, Ü.Y.; Yetik, H.; Sarıcı, A.M. Retinal Vascular Patterns and Capillary Plexus Reflectivity of Intraocular Tumors; an Optical Coherence Tomography Angiography Study. Curr. Eye Res. 2022, 47, 1424–1435. [Google Scholar] [CrossRef]
- Greig, E.C.; Laver, N.V.; Mendonca, L.S.M.; Levine, E.S.; Baumal, C.R.; Waheed, N.K.; Duker, J.S. Swept-Source Optical Coherence Tomography Angiography in Small Choroidal Melanomas and Choroidal Nevi. Retina 2021, 41, 1182–1192. [Google Scholar] [CrossRef]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2016. [Google Scholar]
- Shields, C.L.; Furuta, M.; Berman, E.L.; Zahler, J.D.; Hoberman, D.M.; Dinh, D.H.; Mashayekhi, A.; Shields, J.A. Choroidal nevus transformation into melanoma: Analysis of 2514 consecutive cases. Arch. Ophthalmol. 2009, 127, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, E.; Parravano, M.; Sacconi, R.; Costanzo, E.; Querques, L.; Vella, G.; Bandello, F.; Querques, G. Guidelines on Optical Coherence Tomography Angiography Imaging: 2020 Focused Update. Ophthalmol. Ther. 2020, 9, 697. [Google Scholar] [CrossRef] [PubMed]
- Zudaire, E.; Gambardella, L.; Kurcz, C.; Vermeren, S. A computational tool for quantitative analysis of vascular networks. PLoS ONE 2011, 6, e27385. [Google Scholar] [CrossRef] [PubMed]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Cardona, A. Fiji: An open-source platform for biological-image analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Landini, G.; Murray, P.I.; Misson, G.P. Local connected fractal dimensions and lacunarity analyses of 60° fluorescein angiograms. Investig. Ophthalmol. Vis. Sci. 1995, 36, 2749–2755. [Google Scholar]
- Zahid, S.; Dolz-Marco, R.; Freund, K.B.; Balaratnasingam, C.; Dansingani, K.; Gilani, F.; Mehta, N.; Young, E.; Klifto, M.R.; Chae, B.; et al. Fractal dimensional analysis of optical coherence tomography angiography in eyes with diabetic retinopathy. Investig. Ophthalmol. Vis. Sci. 2016, 57, 4940–4947. [Google Scholar] [CrossRef]
- Shields, C.L.; Dalvin, L.A.; Ancona-Lezama, D.; Yu, M.D.; Di Nicola, M.; Williams, B.K.; Lucio-Alvarez, J.A.; Mae, S.; Maloney, S.; Welch, R.J.; et al. Choroidal nevus imaging features in 3806 cases and risk factors for transformation into melanoma in 2355 cases. Retina 2019, 39, 1840–1851. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 86) | Nevi (n = 67) | Melanomas (n = 19) | p Value † | RR for Growth (95% CI) † |
|---|---|---|---|---|---|
| Demographics | |||||
| Age at diagnosis, mean (SD) | 61.01 (13.9) | 60.6 (15.1) | 62.4 (9.1) | 0.633 * | |
| Sex | 0.538 ** | 0.77 (0.3–1.8) | |||
| Female, n (%) | 49 (57.0) | 37 (55.2) | 12 (63.2) | ||
| Male, n (%) | 37 (43.0) | 30 (44.8) | 7 (36.8) | ||
| Laterality | 0.663 ** | ||||
| Right eye, n (%) | 46 (53.5) | 35 (52.2) | 11 (57.9) | ||
| Left eye, n (%) | 40 (46.5) | 32 (47.8) | 8 (42.1) | ||
| Visual acuity, median (IQR) | 0.9 (0.5) | 0.9 (0.4) | 0.8 (0.5) | 0.369 *** | |
| Small Melanocytic Lesions | |||||
| Thickness (mm), mean (SD) | 1.22 (0.72) | 1.04 (0.67) | 1.88 (0.46) | 0.000 *** | |
| Greatest basal diameter (mm), mean (SD) | 5.91 (2.77) | 5.23 (2.55) | 8.34 (2.13) | 0.000 * | |
| Distance to the optic nerve (mm), median (IQR) | 2.75 (4.2) | 2.70 (4.6) | 3.00 (2.3) | 0.766 *** | |
| Distance to fovea (mm), median (IQR) | 1.20 (3.7) | 1.70 (4.2) | 0.00 (2.8) | 0.213 *** | |
| Number of risk factors present at diagnosis, median (IQR) | 4 (3) | 3 (2) | 6 (1.5) | 0.000 * | |
| Thickness > 2 mm, n (%) | 12 (14.0) | 6 (8.96) | 6 (31.6) | 0.021 **** | 2.85 (1.3–6.0) |
| Subretinal fluid in optical coherence tomography, n (%) | 45 (52.3) | 32 (47.8) | 13 (68.4) | 0.112 ** | 1.97 (0.8–4.7) |
| Symptoms, n (%) | 40 (46.5) | 25 (37.3) | 15 (78.9) | 0.001 ** | 4.3 (1.6–11.9) |
| Orange pigment, n (%) | 33 (38.4) | 18 (26.9) | 15 (78.9) | 0.000 ** | 6.02 (2.2–16.6) |
| Margin ≤ 3 mm from optic nerve, n (%) | 48 (55.8) | 37 (55.2) | 11 (57.9) | 0.836 ** | 1.09 (0.5–2.4) |
| Ultrasonographic hollowness (Kappa sign), n (%) | 15 (17.4) | 5 (7.46) | 10 (52.6) | 0.000 **** | 5.26 (3.6–10.7) |
| Halo, n (%) | 2 (2.3) | 2 (2.99) | 0 (0.0) | 1.000 **** | 0.97 (0.9–1.0) |
| Drusen, n (%) | 42 (48.8) | 36 (53.7) | 6 (31.6) | 0.088 ** | 0.48 (0.2–1.2) |
| Changes during Follow-Up | |||||
| Lesion growth, n (%) | 19 (22.1) | 0 (0.00) | 19 (100) | ||
| Local recurrence after Brachytherapy treatment, n (%) | 1 (1.16) | 0 (0.0) | 1 (5.3) | 0.221 **** | |
| Metastasis, n (%) | 0 (0.00) | 0 (0.0) | 0 (0.0) | ||
| Death, n (%) | 3 (3.5) | 2 (3.0) | 1 (5.3) | 0.532 **** | |
| Follow-up (months), median (IQR) | 41.5 (26) | 41 (29) | 44 (20) | 0.337 * |
| Variable | Total (n = 86) | Nevi (n = 67) | Melanomas (n = 19) | p Value † | RR for Growth (95% CI) † |
|---|---|---|---|---|---|
| Largest vessel diameter (µm), median (IQR) | 56.1 (31.1) | 55.1 (28.0) | 62.8 (47.2) | 0.135 *** | |
| Largest vessel diameter ≥ 100 µm, n (%) | 14 (16.3) | 7 (10.4) | 7 (36.8) | 0.012 **** | 3 (1.4–6.3) |
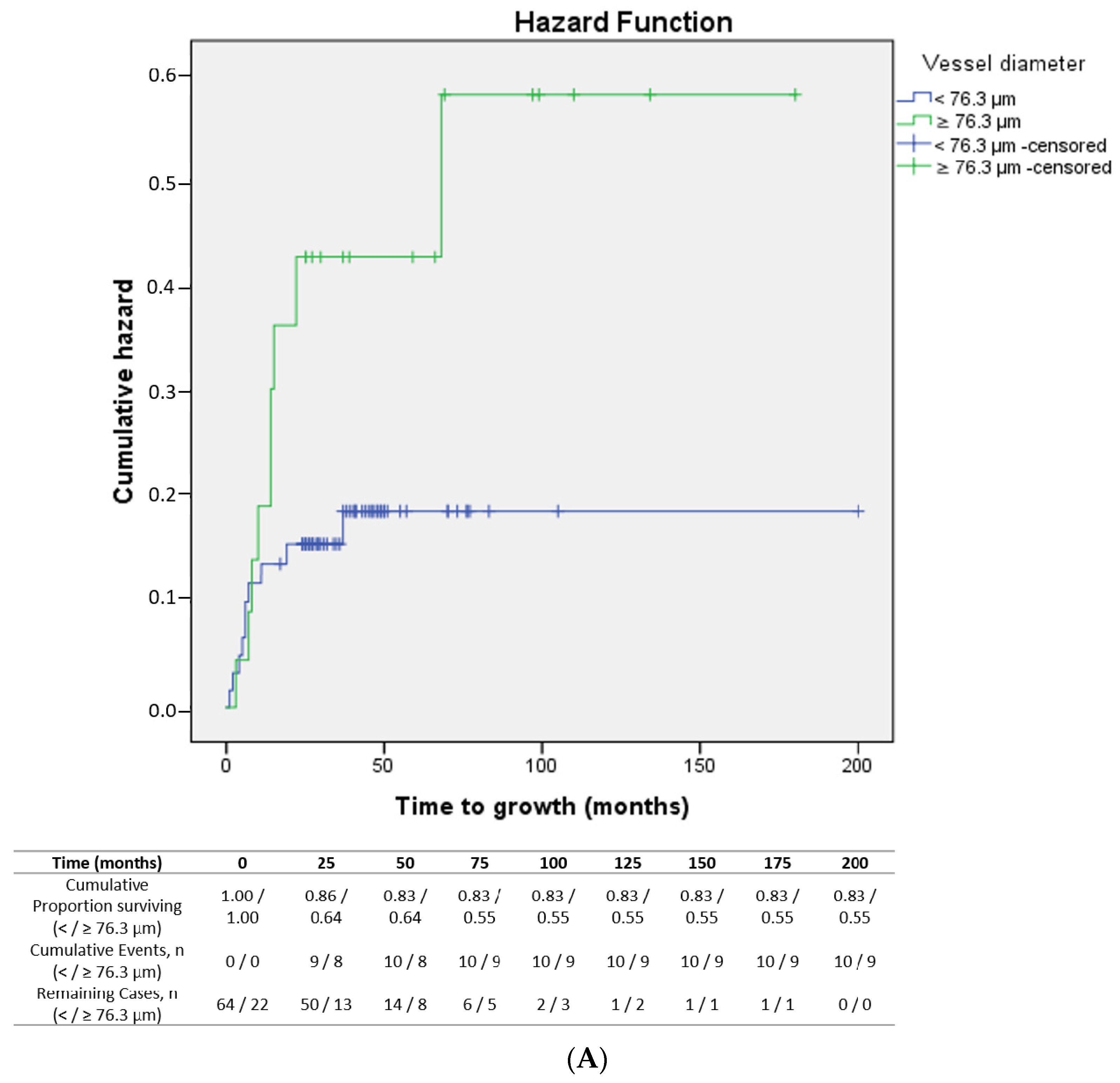
| Largest vessel diameter ≥ 76.3 µm, n (%) | 23 (26.7) | 14 (20.9) | 9 (47.4) | 0.025 **** | 2.46 (1.2–5.3) |
| Well-defined margins, n (%) | 23 (26.74) | 20 (29.9) | 3 (15.8) | 0.222 ** | 0.51 (0.2–1.6) |
| Hyper-reflective ring, n (%) | 28 (32.56) | 23 (34.3) | 5 (26.3) | 0.511 ** | 0.74 (0.3–1.8) |
| Choriocapillaris vascular flow, n (%) | 83 (96.51) | 66 (98.5) | 17 (89.5) | 0.121 **** | 0.31 (0.1–0.8) |
| Intra-lesional vascular flow, n (%) | 47 (54.65) | 34 (50.7) | 13 (68.4) | 0.172 ** | 1.80 (0.8–4.3) |
| Intra-lesional vascularisation, n (%) | 85 (98.84) | 66 (98.5) | 19 (100) | 1.000 **** | 1 |
| Fine vascularisation pattern, n (%) | 74 (86.05) | 59 (88.1) | 15 (78.9) | 0.452 **** | 0.61 (0.2–1.5) |
| Vessel loops, n (%) | 50 (58.14) | 39 (58.2) | 11 (57.9) | 0.980 ** | 0.99 (0.4–2.2) |
| Variable | Total (n = 86) | Nevi (n = 67) | Melanomas (n = 19) | p Value † |
|---|---|---|---|---|
| Median (IQR) | ||||
| Fractal box count, n | 1.87 (0.04) | 1.88 (0.03) | 1.84 (0.04) | 0.515 |
| Proportion of high flux areas, % | 47.0 (7.2) | 47.0 (7.2) | 47.4 (6.4) | 0.525 |
| Vessel percentage area, % | 51.7 (3.2) | 51.7 (2.5) | 49.9 (4.4) | 0.052 |
| Junction density, junctions/mm2 | 0.0018 (0.001) | 0.0019 (0.001) | 0.0018 (0.002) | 0.336 |
| Mean lacunarity (Λ) | 0.037 (0.02) | 0.037 (0.02) | 0.038 (0.02) | 0.122 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vigués-Jorba, L.; Lorenzo, D.; Pujadas, C.; Morwani, R.; Yamamoto-Rodriguez, L.; Baradad-Jurjo, M.; Arias, L.; Cobos, E.; Garcia-Bru, P.; Santamaria, J.-F.; et al. Intralesional Vessel Diameter Measured by Optical Coherence Tomography Angiography Could Improve the Differential Diagnosis of Small Melanocytic Choroidal Lesions. Cancers 2024, 16, 2167. https://doi.org/10.3390/cancers16122167
Vigués-Jorba L, Lorenzo D, Pujadas C, Morwani R, Yamamoto-Rodriguez L, Baradad-Jurjo M, Arias L, Cobos E, Garcia-Bru P, Santamaria J-F, et al. Intralesional Vessel Diameter Measured by Optical Coherence Tomography Angiography Could Improve the Differential Diagnosis of Small Melanocytic Choroidal Lesions. Cancers. 2024; 16(12):2167. https://doi.org/10.3390/cancers16122167
Chicago/Turabian StyleVigués-Jorba, Laura, Daniel Lorenzo, Cristina Pujadas, Rahul Morwani, Liria Yamamoto-Rodriguez, Maria Baradad-Jurjo, Lluis Arias, Estefania Cobos, Pere Garcia-Bru, Juan-Francisco Santamaria, and et al. 2024. "Intralesional Vessel Diameter Measured by Optical Coherence Tomography Angiography Could Improve the Differential Diagnosis of Small Melanocytic Choroidal Lesions" Cancers 16, no. 12: 2167. https://doi.org/10.3390/cancers16122167
APA StyleVigués-Jorba, L., Lorenzo, D., Pujadas, C., Morwani, R., Yamamoto-Rodriguez, L., Baradad-Jurjo, M., Arias, L., Cobos, E., Garcia-Bru, P., Santamaria, J.-F., Garcia Garcia, O., & Caminal, J.-M. (2024). Intralesional Vessel Diameter Measured by Optical Coherence Tomography Angiography Could Improve the Differential Diagnosis of Small Melanocytic Choroidal Lesions. Cancers, 16(12), 2167. https://doi.org/10.3390/cancers16122167