


Prognostic Impact of TERT Promoter Mutations in Adult-Type Diffuse Gliomas Based on WHO2021 Criteria



Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Immunohistochemistry
2.3. DNA and RNA Extraction for Molecular Studies
2.4. Fluorescence In Situ Hybridization for 1p and 19q
2.5. Sanger Sequencing for IDH1/IDH2 Mutation
2.6. TERT Promoter Mutation Analysis
2.7. Methylation-Specific PCR
2.8. Next-Generation Sequencing (NGS)
2.9. Statistical Analysis
3. Results
3.1. Epidemiology and Subgroups of Adult-Type Diffuse Glioma Cohort
3.2. TERTp Mutation Status of the Tumors
3.3. Study for Major Molecular Alterations of Adult-Type Diffuse Gliomas
3.4. Association of TERTp Mutation with Clinicopathological Features and Major Molecular Alterations
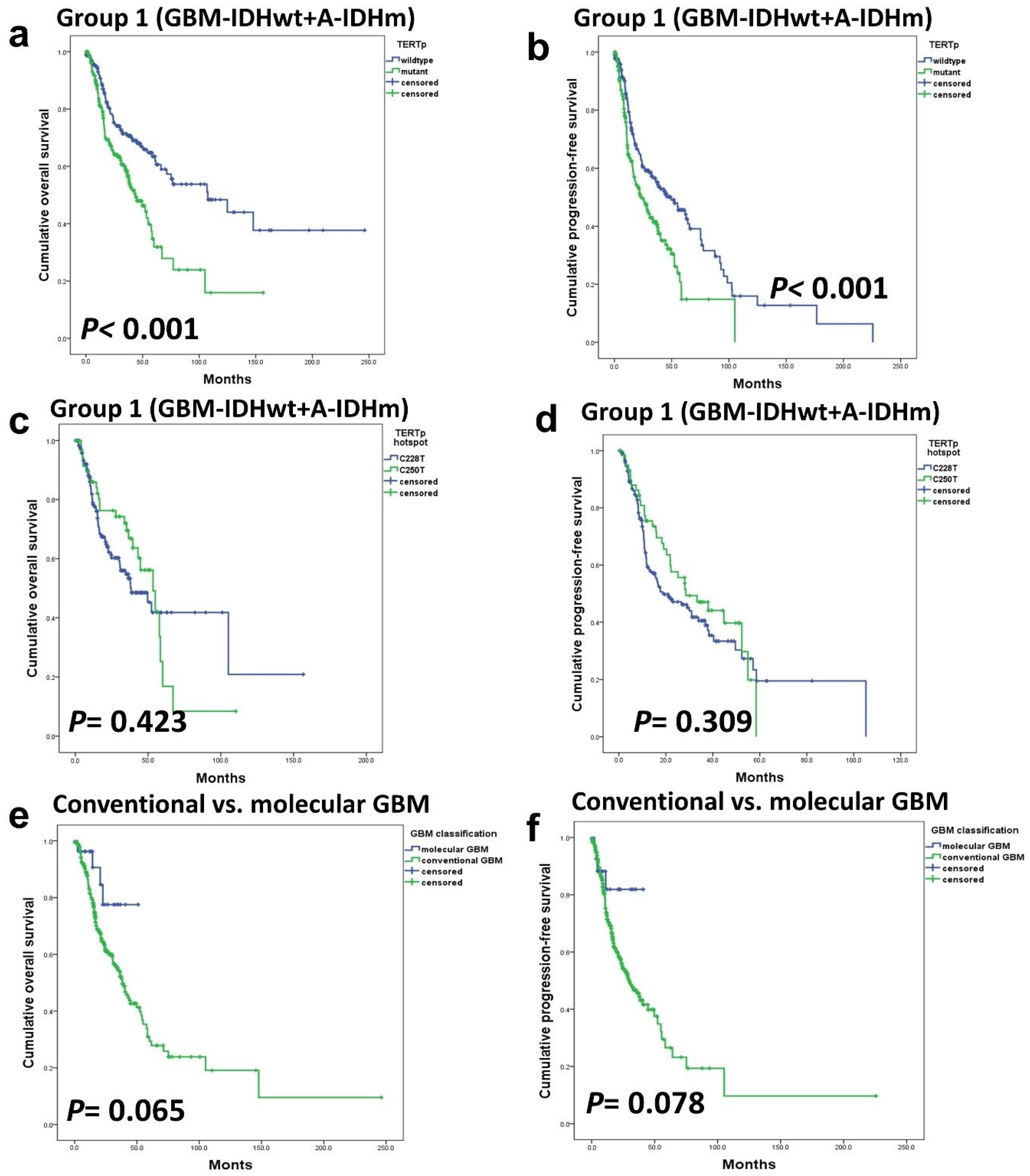
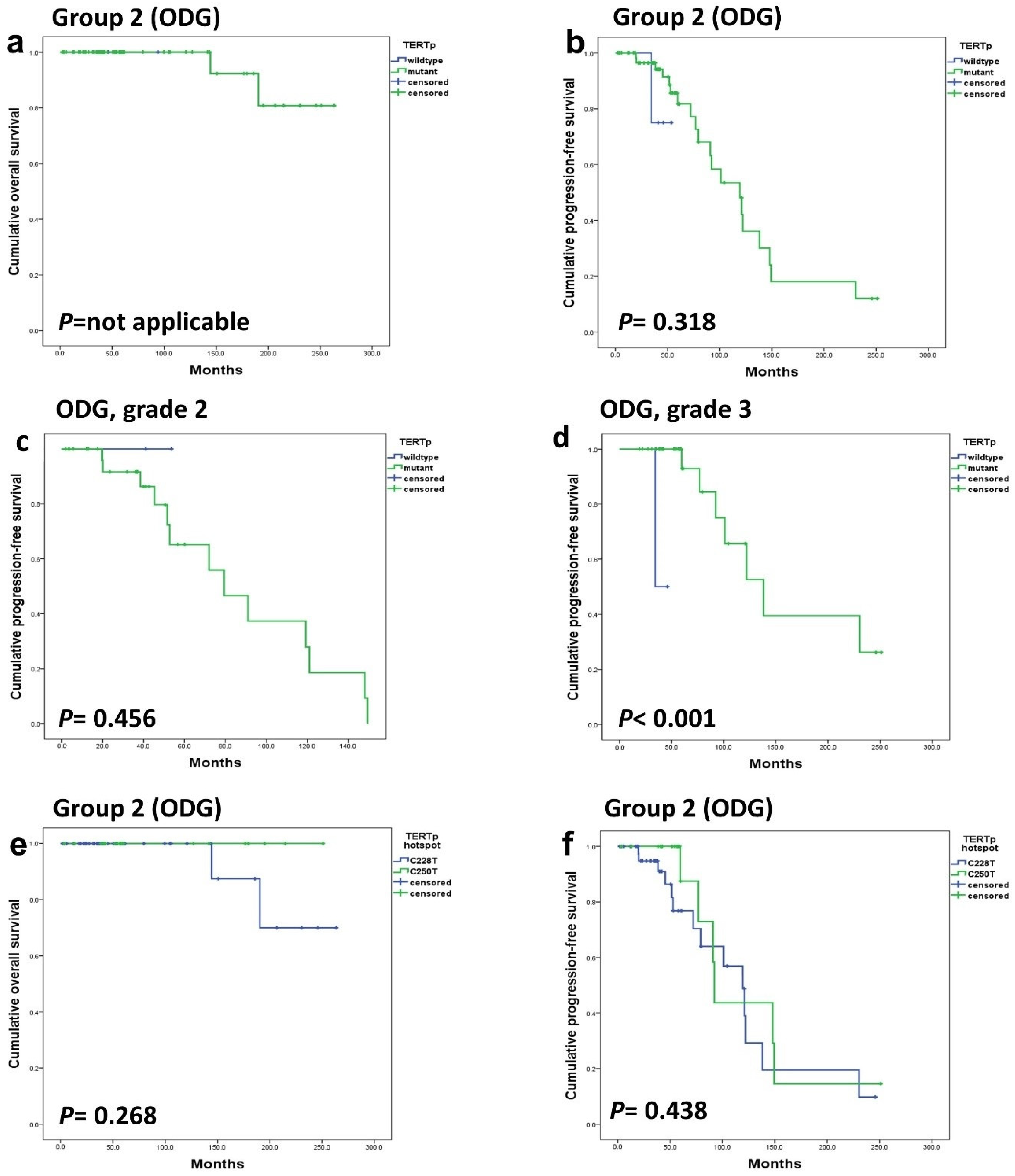
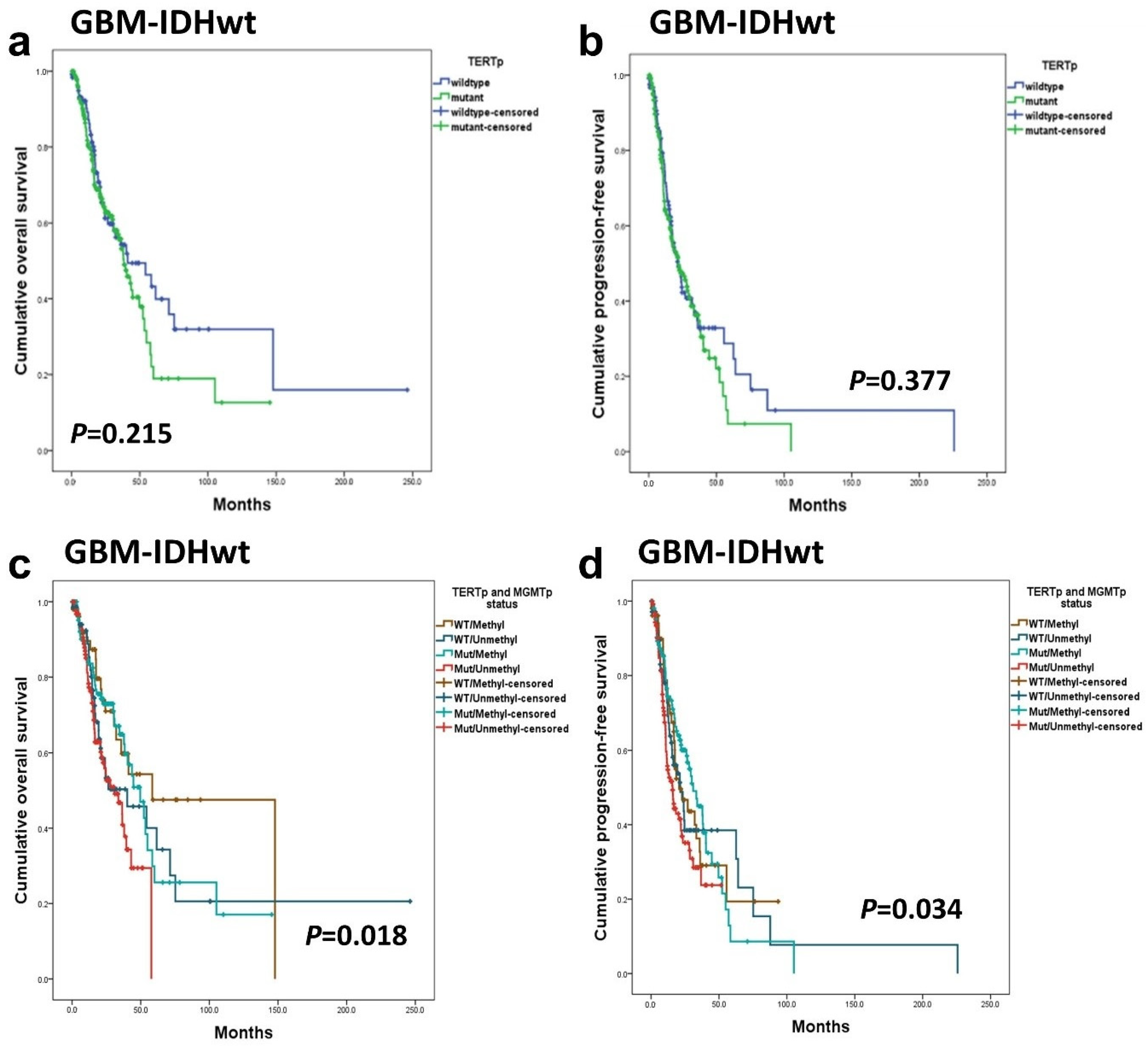
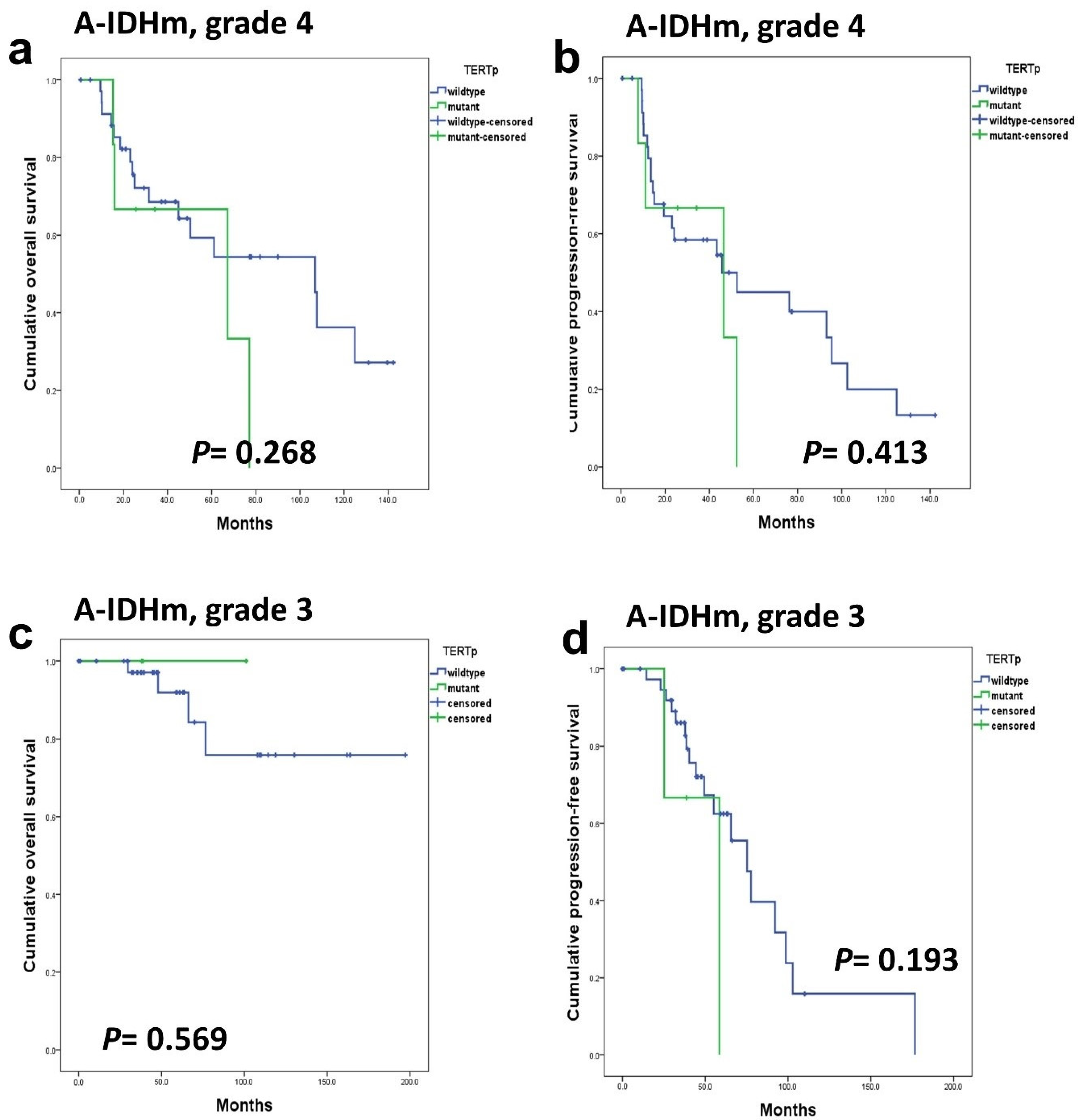
3.5. Overall and Progression-Free Survival Rate
3.6. Prognostic Impact of TERTp Mutations
3.7. Statistical Association between Survival Rate and Clinicopathological Factors in High-Grade Gliomas
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| TERTp | Telomerase reverse transcriptase promoter |
| ALT | alternative lengthening of telomeres |
| ATRX | alpha thalassemia/mental retardation syndrome X-linked |
| DAXX | death-domain associated protein |
| SNP | single nucleotide polymorphisms |
| CNS | central nervous system |
| MVP | microvascular proliferation |
| WHO2021 | 2021 World Health Organization Classification of Tumors of the Central Nervous System, 5th edition |
| cIMPACT-NOW | The Consortium to Inform Molecular and Practical Approaches to CNS Tumor Taxonomy-Not Official WHO |
| GBM-IDHwt | Glioblastoma, IDH-wildtype |
| A-IDHm | Astrocytoma, IDH-mutant |
| ODG | Oligodendroglioma, IDH-mutant, and 1p/19q-codeleted |
| OS | overall survival |
| PFS | progression-free survival |
References
- Blasco, M.A. Telomeres and human disease: Ageing, cancer and beyond. Nat. Rev. Genet. 2005, 6, 611–622. [Google Scholar] [CrossRef]
- Shay, J.W.; Wright, W.E. Telomeres and telomerase: Three decades of progress. Nat. Rev. Genet. 2019, 20, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, T.B.; Sa, A.; Lopes, J.M.; Sobrinho-Simoes, M.; Soares, P.; Vinagre, J. Telomere maintenance mechanisms in cancer. Genes 2018, 9, 241. [Google Scholar] [CrossRef] [PubMed]
- Leao, R.; Apolonio, J.D.; Lee, D.; Figueiredo, A.; Tabori, U.; Castelo-Branco, P. Mechanisms of human telomerase reverse transcriptase (htert) regulation: Clinical impacts in cancer. J. Biomed. Sci. 2018, 25, 22. [Google Scholar] [CrossRef]
- Plyasova, A.A.; Zhdanov, D.D. Alternative splicing of human telomerase reverse transcriptase (htert) and its implications in physiological and pathological processes. Biomedicines 2021, 9, 526. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Snow, B.E.; Hande, M.P.; Yeung, D.; Erdmann, N.J.; Wakeham, A.; Itie, A.; Siderovski, D.P.; Lansdorp, P.M.; Robinson, M.O.; et al. The telomerase reverse transcriptase is limiting and necessary for telomerase function in vivo. Curr. Biol. 2000, 10, 1459–1462. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.W.; Hodis, E.; Xu, M.J.; Kryukov, G.V.; Chin, L.; Garraway, L.A. Highly recurrent tert promoter mutations in human melanoma. Science 2013, 339, 957–959. [Google Scholar] [CrossRef] [PubMed]
- Killela, P.J.; Reitman, Z.J.; Jiao, Y.; Bettegowda, C.; Agrawal, N.; Diaz, L.A., Jr.; Friedman, A.H.; Friedman, H.; Gallia, G.L.; Giovanella, B.C.; et al. Tert promoter mutations occur frequently in gliomas and a subset of tumors derived from cells with low rates of self-renewal. Proc. Natl. Acad. Sci. USA 2013, 110, 6021–6026. [Google Scholar] [CrossRef] [PubMed]
- Nault, J.C.; Mallet, M.; Pilati, C.; Calderaro, J.; Bioulac-Sage, P.; Laurent, C.; Laurent, A.; Cherqui, D.; Balabaud, C.; Zucman-Rossi, J. High frequency of telomerase reverse-transcriptase promoter somatic mutations in hepatocellular carcinoma and preneoplastic lesions. Nat. Commun. 2013, 4, 2218. [Google Scholar] [CrossRef]
- Chebly, A.; Ropio, J.; Peloponese, J.M.; Poglio, S.; Prochazkova-Carlotti, M.; Cherrier, F.; Ferrer, J.; Idrissi, Y.; Segal-Bendirdjian, E.; Chouery, E.; et al. Exploring htert promoter methylation in cutaneous t-cell lymphomas. Mol. Oncol. 2022, 16, 1931–1946. [Google Scholar] [CrossRef]
- Lee, D.D.; Leao, R.; Komosa, M.; Gallo, M.; Zhang, C.H.; Lipman, T.; Remke, M.; Heidari, A.; Nunes, N.M.; Apolonio, J.D.; et al. DNA hypermethylation within tert promoter upregulates tert expression in cancer. J. Clin. Invest. 2019, 129, 223–229. [Google Scholar] [CrossRef]
- Waitkus, M.S.; Erman, E.N.; Reitman, Z.J.; Ashley, D.M. Mechanisms of telomere maintenance and associated therapeutic vulnerabilities in malignant gliomas. Neuro Oncol. 2024. [Google Scholar] [CrossRef] [PubMed]
- Arita, H.; Narita, Y.; Fukushima, S.; Tateishi, K.; Matsushita, Y.; Yoshida, A.; Miyakita, Y.; Ohno, M.; Collins, V.P.; Kawahara, N.; et al. Upregulating mutations in the tert promoter commonly occur in adult malignant gliomas and are strongly associated with total 1p19q loss. Acta Neuropathol. 2013, 126, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Koh, J.; Kim, S.I.; Won, J.K.; Park, C.K.; Choi, S.H.; Park, S.H. The frequency and prognostic effect of tert promoter mutation in diffuse gliomas. Acta Neuropathol. Commun. 2017, 5, 62. [Google Scholar] [CrossRef] [PubMed]
- Eckel-Passow, J.E.; Lachance, D.H.; Molinaro, A.M.; Walsh, K.M.; Decker, P.A.; Sicotte, H.; Pekmezci, M.; Rice, T.; Kosel, M.L.; Smirnov, I.V.; et al. Glioma groups based on 1p/19q, idh, and tert promoter mutations in tumors. N. Engl. J. Med. 2015, 372, 2499–2508. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Kim, S.I.; Kim, E.E.; Shim, Y.M.; Won, J.K.; Park, C.K.; Choi, S.H.; Yun, H.; Lee, H.; Park, S.H. Genomic profiles of idh-mutant gliomas: Mycn-amplified idh-mutant astrocytoma had the worst prognosis. Sci. Rep. 2023, 13, 6761. [Google Scholar] [CrossRef] [PubMed]
- Pekmezci, M.; Rice, T.; Molinaro, A.M.; Walsh, K.M.; Decker, P.A.; Hansen, H.; Sicotte, H.; Kollmeyer, T.M.; McCoy, L.S.; Sarkar, G.; et al. Adult infiltrating gliomas with who 2016 integrated diagnosis: Additional prognostic roles of atrx and tert. Acta Neuropathol. 2017, 133, 1001–1016. [Google Scholar] [CrossRef] [PubMed]
- Labussiere, M.; Boisselier, B.; Mokhtari, K.; Di Stefano, A.L.; Rahimian, A.; Rossetto, M.; Ciccarino, P.; Saulnier, O.; Paterra, R.; Marie, Y.; et al. Combined analysis of tert, egfr, and idh status defines distinct prognostic glioblastoma classes. Neurology 2014, 83, 1200–1206. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 who classification of tumors of the central nervous system: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Ceccarelli, M.; Barthel, F.P.; Malta, T.M.; Sabedot, T.S.; Salama, S.R.; Murray, B.A.; Morozova, O.; Newton, Y.; Radenbaugh, A.; Pagnotta, S.M.; et al. Molecular profiling reveals biologically discrete subsets and pathways of progression in diffuse glioma. Cell 2016, 164, 550–563. [Google Scholar] [CrossRef]
- Tesileanu, C.M.S.; Dirven, L.; Wijnenga, M.M.J.; Koekkoek, J.A.F.; Vincent, A.; Dubbink, H.J.; Atmodimedjo, P.N.; Kros, J.M.; van Duinen, S.G.; Smits, M.; et al. Survival of diffuse astrocytic glioma, idh1/2-wildtype, with molecular features of glioblastoma, who grade iv: A confirmation of the cimpact-now criteria. Neuro Oncol. 2019, 22, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Wesseling, P.; Aldape, K.; Brat, D.J.; Capper, D.; Cree, I.A.; Eberhart, C.; Figarella-Branger, D.; Fouladi, M.; Fuller, G.N.; et al. Cimpact-now update 6: New entity and diagnostic principle recommendations of the cimpact-utrecht meeting on future cns tumor classification and grading. Brain Pathol. 2020, 30, 844–856. [Google Scholar] [CrossRef] [PubMed]
- Berzero, G.; Di Stefano, A.L.; Ronchi, S.; Bielle, F.; Villa, C.; Guillerm, E.; Capelle, L.; Mathon, B.; Laurenge, A.; Giry, M.; et al. Idh-wildtype lower-grade diffuse gliomas: The importance of histological grade and molecular assessment for prognostic stratification. Neuro Oncol. 2021, 23, 955–966. [Google Scholar] [CrossRef] [PubMed]
- Richardson, T.E.; Hatanpaa, K.J.; Walker, J.M. Molecular characterization of “true” low-grade idh-wildtype astrocytomas. J. Neuropathol. Exp. Neurol. 2021, 80, 431–435. [Google Scholar] [CrossRef]
- Giannini, C.; Giangaspero, F. Tert promoter mutation: Is it enough to call a who grade ii astrocytoma idh wild-type glioblastoma? Neuro Oncol. 2021, 23, 865–866. [Google Scholar] [CrossRef] [PubMed]
- Olympios, N.; Gilard, V.; Marguet, F.; Clatot, F.; Di Fiore, F.; Fontanilles, M. Tert promoter alterations in glioblastoma: A systematic review. Cancers 2021, 13, 1147. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.Y.; Lee, K.; Shim, Y.; Park, J.W.; Kim, H.; Kang, J.; Won, J.K.; Kim, S.K.; Phi, J.H.; Park, C.K.; et al. Molecular subtyping of ependymoma and prognostic impact of ki-67. Brain Tumor Pathol. 2022, 39, 1–13. [Google Scholar] [CrossRef]
- Brat, D.J.; Aldape, K.; Colman, H.; Holland, E.C.; Louis, D.N.; Jenkins, R.B.; Kleinschmidt-DeMasters, B.K.; Perry, A.; Reifenberger, G.; Stupp, R.; et al. Cimpact-now update 3: Recommended diagnostic criteria for “diffuse astrocytic glioma, idh-wildtype, with molecular features of glioblastoma, who grade iv”. Acta Neuropathol. 2018, 136, 805–810. [Google Scholar] [CrossRef]
- Mortensen, D.; Ulhoi, B.P.; Lukacova, S.; Alsner, J.; Stougaard, M.; Nyengaard, J.R. Impact of new molecular criteria on diagnosis and survival of adult glioma patients. IBRO Neurosci. Rep. 2022, 13, 299–305. [Google Scholar] [CrossRef]
- Cimino, P.J.; Zager, M.; McFerrin, L.; Wirsching, H.G.; Bolouri, H.; Hentschel, B.; von Deimling, A.; Jones, D.; Reifenberger, G.; Weller, M.; et al. Multidimensional scaling of diffuse gliomas: Application to the 2016 world health organization classification system with prognostically relevant molecular subtype discovery. Acta Neuropathol. Commun. 2017, 5, 39. [Google Scholar] [CrossRef]
- Aoki, K.; Nakamura, H.; Suzuki, H.; Matsuo, K.; Kataoka, K.; Shimamura, T.; Motomura, K.; Ohka, F.; Shiina, S.; Yamamoto, T.; et al. Prognostic relevance of genetic alterations in diffuse lower-grade gliomas. Neuro Oncol. 2018, 20, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Olar, A.; Wani, K.M.; Alfaro-Munoz, K.D.; Heathcock, L.E.; van Thuijl, H.F.; Gilbert, M.R.; Armstrong, T.S.; Sulman, E.P.; Cahill, D.P.; Vera-Bolanos, E.; et al. Idh mutation status and role of who grade and mitotic index in overall survival in grade ii–iii diffuse gliomas. Acta Neuropathol. 2015, 129, 585–596. [Google Scholar] [CrossRef] [PubMed]
- Appay, R.; Dehais, C.; Maurage, C.A.; Alentorn, A.; Carpentier, C.; Colin, C.; Ducray, F.; Escande, F.; Idbaih, A.; Kamoun, A.; et al. Cdkn2a homozygous deletion is a strong adverse prognosis factor in diffuse malignant idh-mutant gliomas. Neuro Oncol. 2019, 21, 1519–1528. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wu, G.; Shan, Y.; Hartmann, C.; von Deimling, A.; Xing, M. Highly prevalent tert promoter mutations in bladder cancer and glioblastoma. Cell Cycle 2013, 12, 1637–1638. [Google Scholar] [CrossRef]
- Terzi, N.K.; Yilmaz, I.; Oz, A.B. The place and prognostic value of tert promoter mutation in molecular classification in grade ii–iii glial tumors and primary glioblastomas. Turk. Patoloji Derg. 2021, 38, 90. [Google Scholar] [CrossRef] [PubMed]
- Simon, M.; Hosen, I.; Gousias, K.; Rachakonda, S.; Heidenreich, B.; Gessi, M.; Schramm, J.; Hemminki, K.; Waha, A.; Kumar, R. Tert promoter mutations: A novel independent prognostic factor in primary glioblastomas. Neuro Oncol. 2015, 17, 45–52. [Google Scholar] [CrossRef]
- Nonoguchi, N.; Ohta, T.; Oh, J.E.; Kim, Y.H.; Kleihues, P.; Ohgaki, H. Tert promoter mutations in primary and secondary glioblastomas. Acta Neuropathol. 2013, 126, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Reitman, Z.J.; Pirozzi, C.J.; Yan, H. Promoting a new brain tumor mutation: Tert promoter mutations in cns tumors. Acta Neuropathol. 2013, 126, 789–792. [Google Scholar] [CrossRef]
- Yang, P.; Cai, J.; Yan, W.; Zhang, W.; Wang, Y.; Chen, B.; Li, G.; Li, S.; Wu, C.; Yao, K.; et al. Classification based on mutations of tert promoter and idh characterizes subtypes in grade ii/iii gliomas. Neuro Oncol. 2016, 18, 1099–1108. [Google Scholar] [CrossRef]
- Batista, R.; Cruvinel-Carloni, A.; Vinagre, J.; Peixoto, J.; Catarino, T.A.; Campanella, N.C.; Menezes, W.; Becker, A.P.; de Almeida, G.C.; Matsushita, M.M.; et al. The prognostic impact of tert promoter mutations in glioblastomas is modified by the rs2853669 single nucleotide polymorphism. Int. J. Cancer 2016, 139, 414–423. [Google Scholar] [CrossRef]
- Killela, P.J.; Pirozzi, C.J.; Healy, P.; Reitman, Z.J.; Lipp, E.; Rasheed, B.A.; Yang, R.; Diplas, B.H.; Wang, Z.; Greer, P.K.; et al. Mutations in idh1, idh2, and in the tert promoter define clinically distinct subgroups of adult malignant gliomas. Oncotarget 2014, 5, 1515–1525. [Google Scholar] [CrossRef] [PubMed]
- Arita, H.; Ichimura, K. Prognostic significance of tert promoter mutations in adult-type diffuse gliomas. Brain Tumor Pathol. 2022, 39, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Mosrati, M.A.; Malmstrom, A.; Lysiak, M.; Krysztofiak, A.; Hallbeck, M.; Milos, P.; Hallbeck, A.L.; Bratthall, C.; Strandeus, M.; Stenmark-Askmalm, M.; et al. Tert promoter mutations and polymorphisms as prognostic factors in primary glioblastoma. Oncotarget 2015, 6, 16663–16673. [Google Scholar] [CrossRef]
- Kikuchi, Z.; Shibahara, I.; Yamaki, T.; Yoshioka, E.; Shofuda, T.; Ohe, R.; Matsuda, K.I.; Saito, R.; Kanamori, M.; Kanemura, Y.; et al. Tert promoter mutation associated with multifocal phenotype and poor prognosis in patients with idh wild-type glioblastoma. Neurooncol. Adv. 2020, 2, vdaa114. [Google Scholar] [CrossRef] [PubMed]
- Labussiere, M.; Di Stefano, A.L.; Gleize, V.; Boisselier, B.; Giry, M.; Mangesius, S.; Bruno, A.; Paterra, R.; Marie, Y.; Rahimian, A.; et al. Tert promoter mutations in gliomas, genetic associations and clinico-pathological correlations. Br. J. Cancer 2014, 111, 2024–2032. [Google Scholar] [CrossRef] [PubMed]
- Arita, H.; Yamasaki, K.; Matsushita, Y.; Nakamura, T.; Shimokawa, A.; Takami, H.; Tanaka, S.; Mukasa, A.; Shirahata, M.; Shimizu, S.; et al. A combination of tert promoter mutation and mgmt methylation status predicts clinically relevant subgroups of newly diagnosed glioblastomas. Acta Neuropathol. Commun. 2016, 4, 79. [Google Scholar] [CrossRef] [PubMed]
- Higa, N.; Akahane, T.; Yokoyama, S.; Yonezawa, H.; Uchida, H.; Takajo, T.; Kirishima, M.; Hamada, T.; Matsuo, K.; Fujio, S.; et al. A tailored next-generation sequencing panel identified distinct subtypes of wildtype idh and tert promoter glioblastomas. Cancer Sci. 2020, 111, 3902–3911. [Google Scholar] [CrossRef]
- Brito, C.; Azevedo, A.; Esteves, S.; Marques, A.R.; Martins, C.; Costa, I.; Mafra, M.; Marques, J.M.B.; Roque, L.; Pojo, M. Clinical insights gained by refining the 2016 who classification of diffuse gliomas with: Egfr amplification, tert mutations, pten deletion and mgmt methylation. BMC Cancer 2019, 19, 968. [Google Scholar] [CrossRef]
- Nguyen, H.N.; Lie, A.; Li, T.; Chowdhury, R.; Liu, F.; Ozer, B.; Wei, B.; Green, R.M.; Ellingson, B.M.; Wang, H.J.; et al. Human tert promoter mutation enables survival advantage from mgmt promoter methylation in idh1 wild-type primary glioblastoma treated by standard chemoradiotherapy. Neuro Oncol. 2017, 19, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Kwon, M.J.; Song, J.H.; Kim, E.S.; Kim, H.Y.; Min, K.W. Clinical implications of tert promoter mutation on idh mutation and mgmt promoter methylation in diffuse gliomas. Pathol. Res. Pract. 2018, 214, 881–888. [Google Scholar] [CrossRef]
- Hegi, M.E.; Diserens, A.C.; Gorlia, T.; Hamou, M.F.; de Tribolet, N.; Weller, M.; Kros, J.M.; Hainfellner, J.A.; Mason, W.; Mariani, L.; et al. Mgmt gene silencing and benefit from temozolomide in glioblastoma. N. Engl. J. Med. 2005, 352, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Arita, H.; Matsushita, Y.; Machida, R.; Yamasaki, K.; Hata, N.; Ohno, M.; Yamaguchi, S.; Sasayama, T.; Tanaka, S.; Higuchi, F.; et al. Tert promoter mutation confers favorable prognosis regardless of 1p/19q status in adult diffuse gliomas with idh1/2 mutations. Acta Neuropathol. Commun. 2020, 8, 201. [Google Scholar] [CrossRef] [PubMed]
- Powter, B.; Jeffreys, S.A.; Sareen, H.; Cooper, A.; Brungs, D.; Po, J.; Roberts, T.; Koh, E.S.; Scott, K.F.; Sajinovic, M.; et al. Human tert promoter mutations as a prognostic biomarker in glioma. J. Cancer Res. Clin. Oncol. 2021, 147, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- Aquilanti, E.; Kageler, L.; Wen, P.Y.; Meyerson, M. Telomerase as a therapeutic target in glioblastoma. Neuro Oncol. 2021, 23, 2004–2013. [Google Scholar] [CrossRef]
- Kondo, S.; Kondo, Y.; Li, G.; Silverman, R.H.; Cowell, J.K. Targeted therapy of human malignant glioma in a mouse model by 2-5a antisense directed against telomerase rna. Oncogene 1998, 16, 3323–3330. [Google Scholar] [CrossRef]
- Kondo, Y.; Kondo, S.; Tanaka, Y.; Haqqi, T.; Barna, B.P.; Cowell, J.K. Inhibition of telomerase increases the susceptibility of human malignant glioblastoma cells to cisplatin-induced apoptosis. Oncogene 1998, 16, 2243–2248. [Google Scholar] [CrossRef] [PubMed]
- Aquilanti, E.; Kageler, L.; Watson, J.; Baird, D.M.; Jones, R.E.; Hodges, M.; Szegletes, Z.M.; Doench, J.G.; Strathdee, C.A.; Figueroa, J.; et al. Telomerase inhibition is an effective therapeutic strategy in tert promoter-mutant glioblastoma models with low tumor volume. Neuro Oncol. 2023, 25, 1275–1285. [Google Scholar] [CrossRef]
- Waksal, J.A.; Bruedigam, C.; Komrokji, R.S.; Jamieson, C.H.M.; Mascarenhas, J.O. Telomerase-targeted therapies in myeloid malignancies. Blood Adv. 2023, 7, 4302–4314. [Google Scholar] [CrossRef]
- Salloum, R.; Hummel, T.R.; Kumar, S.S.; Dorris, K.; Li, S.; Lin, T.; Daryani, V.M.; Stewart, C.F.; Miles, L.; Poussaint, T.Y.; et al. A molecular biology and phase ii study of imetelstat (grn163l) in children with recurrent or refractory central nervous system malignancies: A pediatric brain tumor consortium study. J. Neurooncol. 2016, 129, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.A.; Drissi, R.; Muscal, J.A.; Panditharatna, E.; Fouladi, M.; Ingle, A.M.; Ahern, C.H.; Reid, J.M.; Lin, T.; Weigel, B.J.; et al. A phase i trial of imetelstat in children with refractory or recurrent solid tumors: A children’s oncology group phase i consortium study (advl1112). Clin. Cancer Res. 2013, 19, 6578–6584. [Google Scholar] [CrossRef]
- Platzbecker, U.; Santini, V.; Fenaux, P.; Sekeres, M.A.; Savona, M.R.; Madanat, Y.F.; Diez-Campelo, M.; Valcarcel, D.; Illmer, T.; Jonasova, A.; et al. Imetelstat in patients with lower-risk myelodysplastic syndromes who have relapsed or are refractory to erythropoiesis-stimulating agents (imerge): A multinational, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2024, 403, 249–260. [Google Scholar] [CrossRef]
- Li, X.; Qian, X.; Wang, B.; Xia, Y.; Zheng, Y.; Du, L.; Xu, D.; Xing, D.; DePinho, R.A.; Lu, Z. Programmable base editing of mutated tert promoter inhibits brain tumour growth. Nat. Cell Biol. 2020, 22, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Mancini, A.; Xavier-Magalhaes, A.; Woods, W.S.; Nguyen, K.T.; Amen, A.M.; Hayes, J.L.; Fellmann, C.; Gapinske, M.; McKinney, A.M.; Hong, C.; et al. Disruption of the beta1l isoform of gabp reverses glioblastoma replicative immortality in a tert promoter mutation-dependent manner. Cancer Cell 2018, 34, 513–528. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Wei, S.; Savani, M.; Lin, X.; Du, K.; Mender, I.; Siteni, S.; Vasilopoulos, T.; Reitman, Z.J.; Ku, Y.; et al. A modified nucleoside 6-thio-2’-deoxyguanosine exhibits antitumor activity in gliomas. Clin. Cancer Res. 2021, 27, 6800–6814. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, S.; Sobo, M.; Lee, K.; Kumar, S.S.; White, A.R.; Mender, I.; Fuller, C.; Chow, L.M.L.; Fouladi, M.; Shay, J.W.; et al. Induced telomere damage to treat telomerase expressing therapy-resistant pediatric brain tumors. Mol. Cancer Ther. 2018, 17, 1504–1514. [Google Scholar] [CrossRef]
- Lee, D.D.; Komosa, M.; Sudhaman, S.; Leao, R.; Zhang, C.H.; Apolonio, J.D.; Hermanns, T.; Wild, P.J.; Klocker, H.; Nassiri, F.; et al. Dual role of allele-specific DNA hypermethylation within the tert promoter in cancer. J. Clin. Investig. 2021, 131, e146915. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Variables | Classical GBM-IDHwt n = 335 | Molecular GBM-IDHwt n = 27 | Total GBM-IDHwt n = 362 | A-IDHm, G2 n = 13 | A-IDHm, G3 n = 43 | A-IDHm, G4 n = 42 | Total A-IDHm n = 98 | ODG, G2 n = 33 | ODG, G3 n = 35 | Total ODG n = 68 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | Range (median) | 2–86 (60) | 36–78 (56) | 2–86 (60) | 26–55 (47) | 18–66 (36) | 27–70 (39.5) | 18–70 (38) | 22–66 (42) | 31–69 (52) | 22–69 (49) |
| Gender | Male | 181 | 12 | 193 | 9 | 22 | 27 | 58 | 20 | 20 | 40 |
| Female | 154 | 15 | 169 | 4 | 21 | 15 | 40 | 13 | 15 | 28 | |
| OS (months) | Range (median) | 0.3–236.2 (38.3) | 2.2–50.9 (20.9) | 0.2–246.2 (40.2) | 42.8–209.4 (NA/56.0) | 0.8–197.2 (NA/47.5) | 0.6–153.6 (77.0/37.1) | 0.6–209.4 (NA/47.1) | 2.0–214.7 (NA/42.7) | 19.1–263.4 (NA/56.5) | 2.0–263.4 (NA/52.5) |
| PFS (months) | Range (median) | 0.2–225.7 (30.0) | 2.2–40.8 (11.2) | 0.2–225.7 (22.0) | 10.0–61.8 (NA/53.0) | 0.8–176.7 (75.3/44.4) | 0.6–153.6 (46.5/35.0) | 0.6–176.6 (65.5/43.5) | 2.0–149.4 (79.3) | 19.1–251.0 (109.5) | 2.0–251.0 (92.2) |
| Mitosis | Range (mean) | 1–210 (32.4) | 0–72 (15.3) | 0–250 (31.1) | 0–2 (0.9) | 3–60 (11.0) | 0–110 (25.0) | 0–110 (15.7) | 0–12 (3.5) | 1–55 (15.1) | 0–55 (9.5) |
| Ki-67 index (%) | Range (mean) | 1.0–96.9 (40.8) | 1.0–92.4 (20.0) | 1.0–96. 9 (39.2) | 0.2–4.3 (2.6) | 1.0–46.0 (9.7) | 1.7–90.2 (31.6) | 0.2–90.2 (18.2) | 0.9–26.6 (7.0) | 7.6–74.3 (29.6) | 0.9–74.3 (18.6) |
| TERTp | GBM-IDHwt n = 362 | A-IDHm, G2 n = 13 | A-IDHm, G3 n = 43 | A-IDHm, G4 n = 42 | A-IDHm n = 98 | ODG, G2 n = 33 | ODG, G3 n = 35 | ODG n = 68 |
|---|---|---|---|---|---|---|---|---|
| Mutant (%) | 240/362 (66.3) | 0/13 (0) | 3/43 (7.0) | 6/42 (14.3) | 9/98 (9.2) | 31/33 (93.9) | 33/35 (94.3) | 64/68 (94.1) |
| C228T | 177/240 (73.8) | 0/0 (0) | 2/3 (66.7) | 4/6 (66.7) | 6/9 (66.6) | 23/31 (74.2) | 22/33 (66.7) | 45/64 (70.3) |
| C250T | 63/240 (26.2) | 0/0 (0) | 1/3 (33.3) | 2/6 (33.3) | 3/9 (33.3) | 8/31 (25.8) | 11/33 (33.3) | 19/64 (29.7) |
| Genes | Changes | Conventional GBM | Molecular GBM | GBM-IDHwt n = 364 (%) | A-IDHm, G2 n = 13 (%) | A-IDHm, G3 n = 43 (%) | A-IDHm, G4 n = 42 (%) | Total A-IDHm n = 98 (%) | ODG, G2 n = 33 (%) | ODG, G3 n = 35 (%) | Total ODG n = 68 (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| MGMTp | Methylated | 159/335 (47.5) | 5/27 (18.5) | 164/364 (45.3) | 8/13 (61.5) | 30/43 (69.8) | 34/42 (81.0) | 72/98 (73.5) | 32/33 (97.0) | 33/35 (94.3) | 65/68 (95.6) |
| Unmethylated | 176/335 (52.5) | 22/27 (81.5) | 198/362 (54.7) | 5/13 (38.5) | 13/43 (30.2) | 8/42 (19.0) | 26/98 (26.5) | 1/33 (3.0) | 2/35 (5.7) | 3/68 (4.4) | |
| ATRX | Mutant | 14/316 (4.4) | 1/27 (3.7) | 15/343 (4.4) | 9/13 (69.2) | 33/42 (78.6) | 26/37 (70.3) | 68/92 (73.9) | 0/33 (0) | 0/35 (0) | 0/68 (0) |
| Wildtype | 302/316 (95.6) | 26/27 (96.3) | 328/343 (95.6) | 4/13 (30.8) | 9/42 (21.4) | 11/37 (29.7) | 24/92 (26.1) | 33/33 (100) | 35/35 (100) | 68/68 (100) | |
| 1p/19q | Co-deletion | 0/330 (0) | 0/26 (0) | 0/356 (0) | 0/13 (0) | 0/43 (0) | 0/41 (0) | 0/98 (0) | 33/33 (100) | 35/35 (100) | 68/68 (100) |
| No co-deletion | 330/330 (100) | 26/26 (100) | 356/356 (100) | 13/13 (100) | 43/43 (100) | 42/42 (100) | 98/98 (100) | 0/33 (0) | 0/35 (0) | 0/68 (0) | |
| EGFR | Amplification | 90/334 (26.9) | 9/27 (33.3) | 99/361 (27.4) | 0/13 (0) | 0/43 (0) | 2/42 (4.8) | 2/98 (2.0) | 0/33 (0) | 0/35 (0) | 0/68 (0) |
| No amplification | 244/334 (73.1) | 18/27(66.7) | 262/361 (72.6) | 13/13 (100) | 43/43 (0) | 40/42 (95.2) | 96/98 (98.0) | 33/33 (100) | 35/35 (100) | 68/68 (100) | |
| CDKN2A/B | Deletion | 165/319 (51.7) | 9/27 (33.3) | 174/346 (10.3) | 0/13 (0) | 0/41 (0) | 20/42 (47.6) | 20/96 (20.8) | 1/33 (3.0) | 7/35 (20.0) | 5/68 (7.4) |
| No deletion | 154/319 (48.3) | 18/27 (66.7) | 172/346 (49.7) | 13/13 (100) | 41/41 (100) | 22/42 (52.4) | 76/96 (79.2) | 32/33 (97.0) | 28/35 (80.0) | 63/68 (92.6) | |
| PTEN | Deletion | 57/334 (17.1) | 2/27 (7.4) | 59/361 (16.3) | 0/13 (0) | 2/43 (4.7) | 6/42 (14.3) | 8/98 (8.2) | 0/33 (0) | 0/35 (11.4) | 0/68 (0) |
| No deletion | 277/334 (82.9) | 25/27 (92.6) | 302/361 (83.7) | 13/13 (100) | 41/43 (95.3) | 36/42 (85.7) | 90/98 (91.8) | 33/33 (100) | 35/35 (88.6) | 68/68 (100) |
| Variables | Comparison | Univariate | ||
|---|---|---|---|---|
| p | HR | 95%CI | ||
| TERTp | Wildtype vs. Mutant | 0.211 | 0.799 | 0.561–1.140 |
| Age | Age ≥ 55 vs. <55 | 0.018 | 1.530 | 1.074–2.178 |
| Gender | Male vs. Female | 0.770 | 0.952 | 0.685–1.323 |
| MVP/necrosis | Absent vs. Present | 0.074 | 0.636 | 0.386–1.046 |
| Mitosis | Mitosis ≥ 11 vs. <11 | 0.021 | 1.607 | 1.073–2.406 |
| Ki-67 (cutoff > 11.19%) | High vs. Low | 0.195 | 1.463 | 0.195–1.463 |
| MGMTp | Methylated vs. Unmethylated | 0.006 | 1.166 | 1.069–1.498 |
| ATRX | Wildtype vs. Mutant | 0.546 | 1.125 | 0.768–1.648 |
| EGFR amplification | Absent vs. Present | 0.919 | 0.991 | 0.826–1.188 |
| CDKN2A/B homozygous deletion | Absent vs. Present | <0.001 | 0.679 | 0.566–0.816 |
| PTEN loss | Absent vs. Present | 0.013 | 0.781 | 0.642–0.949 |
| Variables | Comparison | Multivariate | ||
| p | HR | 95%CI | ||
| TERTp | Wildtype vs. Mutant | 0.156 | 1.394 | 0.881–2.207 |
| Age | Age ≥ 55 vs. <55 | 0.002 | 1.023 | 1.009–1.038 |
| Gender | Male vs. Female | 0.733 | 0.935 | 0.634–1.377 |
| MVP/necrosis | Absent vs. Present | 0.147 | 0.440 | 0.145–1.334 |
| Mitosis | Mitosis ≥ 11 vs. <11 | 0.170 | 1.463 | 0.849–2.519 |
| Ki-67 (cutoff > 11.19%) | High vs. Low | 0.585 | 0.798 | 0.354–1.797 |
| MGMTp | Methylated vs. Unmethylated | 0.003 | 1.851 | 1.237–2.769 |
| ATRX | Wildtype vs. Mutant | 0.378 | 1.466 | 0.626–3.436 |
| EGFR amplification | Absent vs. Present | 0.129 | 1.434 | 0.900–2.284 |
| CDKN2A/B homozygous deletion | Absent vs. Present | 0.001 | 0.501 | 0.328–0.765 |
| PTEN loss | Absent vs. Present | 0.219 | 0.754 | 0.480–1.183 |
| Variables | Comparison | Univariate | ||
|---|---|---|---|---|
| p | HR | 95%CI | ||
| TERTp mutation | Wildtype vs. Mutant | 0.275 | 1.869 | 0.308–5.750 |
| Age | Age ≥ 55 vs. <55 | 0.896 | 0.929 | 0.309–2.796 |
| Gender | Male vs. Female | 0.376 | 0.663 | 0.267–1.646 |
| MVP/necrosis | Absent vs. Present | 0.649 | 1.348 | 0.373–4.862 |
| Mitosis | Mitosis ≥ 32 vs. <32 | 0.130 | 2.001 | 0.815–4.913 |
| Ki-67 (cutoff > 25.3%) | High vs. Low | 0.003 | 4.578 | 1.653–12.673 |
| MGMTp | Methylated vs. Unmethylated | 0.174 | 2.045 | 0.730–5.726 |
| ATRX | Wildtype vs. Mutant | 0.217 | 0.544 | 0.207–1.429 |
| EGFR amplification | Absent vs. Present | 0.607 | 1.704 | 0.226–12.981 |
| CDKN2A/B homozygous deletion | Absent vs. Present | 0.345 | 0.648 | 0.264–1.594 |
| PTEN deletion | Absent vs. Present | 0.501 | 1.479 | 0.473–4.627 |
| MYCN amplification | Absent vs. Present | 0.031 | 0.137 | 0.023–0.832 |
| Variables | Comparison | Multivariate | ||
| p | HR | 95%CI | ||
| TERTp mutation | Wildtype vs. Mutant | 0.106 | 4.376 | 0.729–26.267 |
| Age | Age ≥ 55 vs. <55 | 0.073 | 3.594 | 0.886–14.580 |
| Gender | Male vs. Female | 0.359 | 0.488 | 0.105–2.262 |
| MVP/necrosis | Absent vs. Present | 0.538 | 1.635 | 0.342–7.813 |
| Mitosis | Mitosis ≥ 32 vs. <32 | 0.038 | 0.168 | 0.031–0.906 |
| Ki-67 (cutoff > 25.3%) | High vs. Low | 0.002 | 16.567 | 2.872–95.576 |
| MGMTp | Methylated vs. Unmethylated | 0.024 | 6.587 | 1.275–34.038 |
| ATRX | Wildtype vs. Mutant | 0.604 | 0.694 | 0.174–2.767 |
| EGFR amplification | Absent vs. Present | 0.976 | 0.965 | 0.094–10.227 |
| CDKN2A/B homozygous deletion | Absent vs. Present | 0.950 | 0.954 | 0.220–4.130 |
| PTEN deletion | Absent vs. Present | 0.746 | 1.376 | 0.199–9.538 |
| MYCN amplification | Absent vs. Present | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.; Park, C.-K.; Park, S.-H. Prognostic Impact of TERT Promoter Mutations in Adult-Type Diffuse Gliomas Based on WHO2021 Criteria. Cancers 2024, 16, 2032. https://doi.org/10.3390/cancers16112032
Lee Y, Park C-K, Park S-H. Prognostic Impact of TERT Promoter Mutations in Adult-Type Diffuse Gliomas Based on WHO2021 Criteria. Cancers. 2024; 16(11):2032. https://doi.org/10.3390/cancers16112032
Chicago/Turabian StyleLee, Yujin, Chul-Kee Park, and Sung-Hye Park. 2024. "Prognostic Impact of TERT Promoter Mutations in Adult-Type Diffuse Gliomas Based on WHO2021 Criteria" Cancers 16, no. 11: 2032. https://doi.org/10.3390/cancers16112032
APA StyleLee, Y., Park, C.-K., & Park, S.-H. (2024). Prognostic Impact of TERT Promoter Mutations in Adult-Type Diffuse Gliomas Based on WHO2021 Criteria. Cancers, 16(11), 2032. https://doi.org/10.3390/cancers16112032