
Comprehensive Pulmonary Rehabilitation for Patients with Malignant Pleural Mesothelioma: A Feasibility Pilot Study

 ,
,  ,
, 
 ,
,  ,
,  ,
,  ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
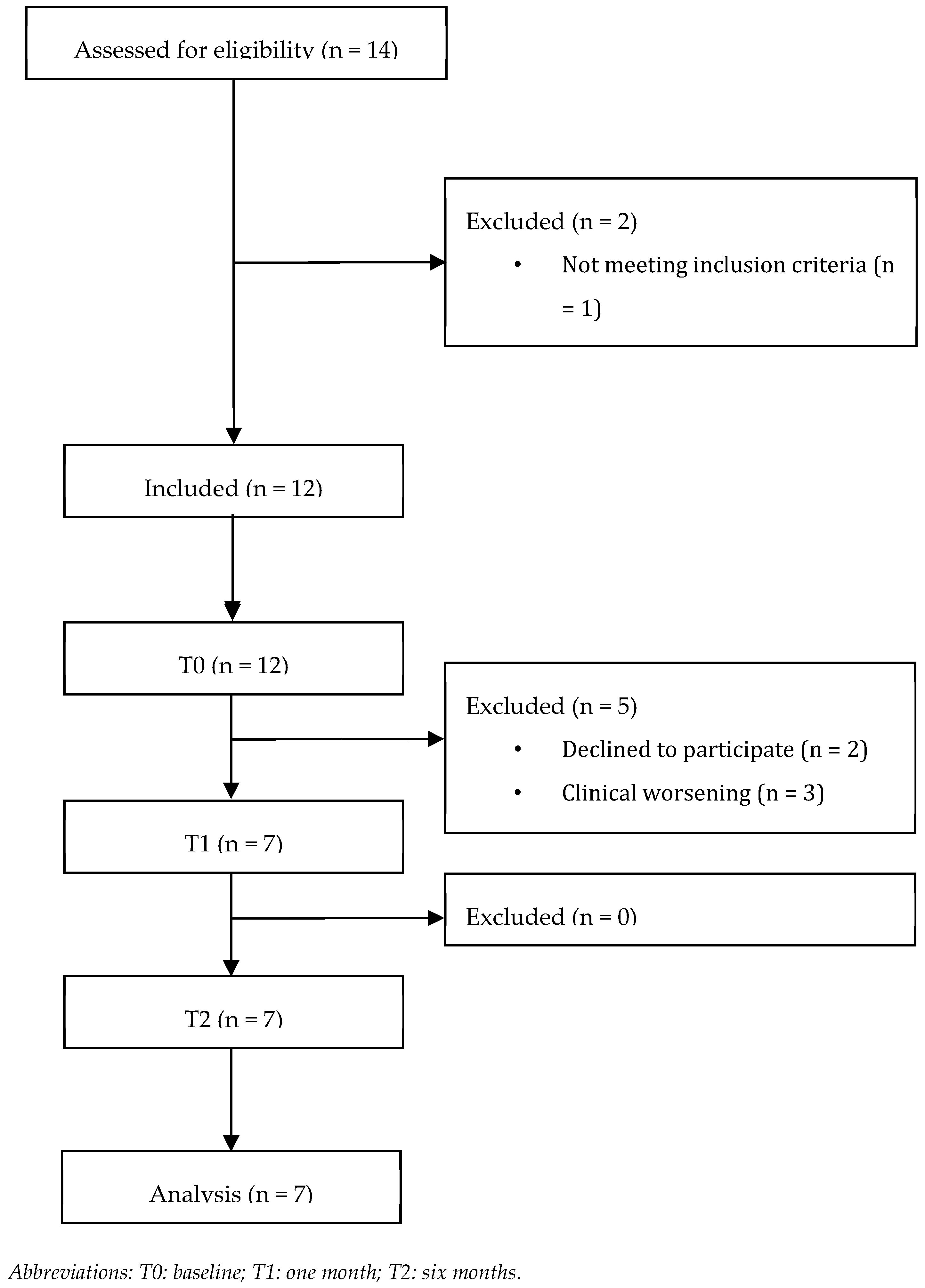
2.1. Study Design and Participants
2.2. Intervention
- Counseling and educational therapy. All patients included underwent a single multidisciplinary educational session conducted by different healthcare operators (physiatrist, physiotherapist, nurse, speech therapist, and dietician), focusing on energy conservation strategies in activities of daily living (ADL), symptom recognition and management, and training for respiratory devices (i.e., oxygen therapy, aerosol therapy, etc.).
- Physical rehabilitation. Patients were subjected to a home-based physical rehabilitation protocol consisting of 50–60 min sessions three times a week. The sessions were structured as follows: (1) warm-up phase (5–10 min), consisting of stretching and active joint mobilization exercises; (2) resistance-exercises phase with body weight and a TheraBand, targeting all major muscle groups at 60–75% and an estimated one-repetition maximum (1RM) for approximately 20 min; (3) aerobic-exercise phase targeting an exercise intensity between 60 and 85% of maximal heart rate, based on the patient’s tolerance. Activities included walking, swimming, and cycling for at least 20 min; and (4) cool-down phase (5–10 min) with stretching and active joint mobilization exercises. The first three sessions were supervised by an experienced physical therapist, who showed the correct execution of physical exercises. A booklet including pictures and instructions on the physical rehabilitation program was provided to support patients in the home-based rehabilitation program, and progress was recorded in a self-treatment diary to monitor adherence to the rehabilitation program.
- Respiratory physiotherapy. The respiratory physiotherapy program included respiratory muscle training, lung recruitment maneuvers, and bronchial secretion management using a specific device (Temporary Positive Expiratory Pressure—TPEP® ONE, Legnano, Milan, Italy) twice daily for 15 min (as depicted in Figure 1).
2.3. Quantitative Outcome Measures
- -
- Physical functioning: lower-limb physical performance was assessed by the Short Physical Performance Battery (SPPB) [28]; submaximal exercise capacity, measured through a 30 s sit-to-stand (STS) test [29]; a two-minute-walking test (2MWT) [30,31] for the detection of dyspnea (Borg CR10 [32]); and oxygen saturation (SpO2), and muscle strength was assessed by a handgrip strength test (HST) using Jamar® dynamometer [33,34].
- -
- Pulmonary function: assessed by arterial blood gas (ABG) analysis (characterizing partial pressure of oxygen [PaO2], partial pressure of carbon dioxide [PaCO2], and pH) and spirometry, which assessed forced expiratory volume in the first second (FEV1), forced vital capacity (FVC), diffusing capacity for carbon monoxide (DLCO), and peak expiratory flow (PEF).
- -
- Pain intensity: pain was assessed through the Visual Analog Scale (VAS) [35].
- -
- Nutritional assessment: nutritional screening was conducted through the Mini Nutritional Assessment (MNA) [36].
- -
- Health-related quality of life (HR-QoL): evaluated by the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ–C30), a scale composed of a 30-item questionnaire, including a functional scale (physical, role, cognitive, emotional, and social), a symptom scale (fatigue, pain, and nausea and vomiting), and a global QoL scale. Single items assessed further symptoms frequently reported by oncologic patients (such as dyspnea, loss of appetite, insomnia, constipation, and diarrhea) and the perceived financial impact of the disease; there were four possible answers: “Not at all”, “A little”, “Quite a bit” and “Very much” [37]. To better characterize QoL in patients with MPM, the Lung Cancer Symptom Scale-Mesothelioma (LCSS-meso) was used in included patients [38]. This nine-item site-specific QoL measure concentrates on six symptoms (appetite loss, fatigue, cough, dyspnea, hemoptysis, and pain) and three summary items (symptomatic distress, normal activity, and global QoL). All items are measured using 100 mm lines to assess the intensity of patient responses (with 0 as the lowest and 100 mm as the greatest value) in the previous 24 h. The total score is obtained by the average of all nine item scores [38]. Patient perspective on physical, mental, and social well–being was assessed through the Patient-Reported Outcomes Measurement Information System (PROMIS) based on questions in a 7-day recall period, exploring items such as anxiety, anger, depression, fatigue, pain quality, pain interference, pain behavior, satisfaction with participation in discretionary social activities, satisfaction with the involvement in social roles, sleep disturbance, and sleep-related impairment, with five response options (e.g., 1 = Not at all, 2 = A little bit, 3 = Somewhat, 4 = Quite a bit, 5 = Very much) [39].
2.4. Qualitative Analysis
2.5. Statistical Analysis
3. Results
3.1. Primary Outcomes
3.2. Secondary Outcomes
3.2.1. Physical Functioning
3.2.2. Blood Gases and Pulmonary Function
3.2.3. Multidimensional Assessment of Patients with MPM
3.3. Qualitative Analysis
3.3.1. Perceived Effectiveness
“Since I started the rehabilitation program, I have had improvements in several settings. I still can do the things I did during the first assessments. […] Two weeks ago, I went for a CT scan. Unfortunately, there was no improvement […], but this is not the fault of the therapy. I enjoyed therapy and enjoyed doing it”.(Patient ID 3)
“I haven’t felt any benefits from rehabilitation therapy, even now I’m doing it. However, I have no perception that it is of any use”.(Patient ID 5)
3.3.2. Barriers to Rehabilitation
“The rehabilitation program was time spending. I still worked several hours a day […] it was a challenge to find time to fit everything together”.(Patient ID 5)
“The program was difficult at the beginning. […] I need a person who follows me and teaches me well. It is important for the elderly when they start to lack memory and desire to do things.”
“The rehabilitation program had no interactions with family. […] We went away for a couple of days; I took the device with me, and I did rehabilitation in the hotel”.(Patient ID 6)
3.3.3. Impact on Quality of Life
“The program had no impact on my free time; I did it when I was free”.(Patient ID 1)
”My social life has reduced a lot, probably also because of the COVID pandemic […] Rehabilitation treatment itself takes up a lot of time”.(Patient ID 1)
3.3.4. Psychological and Social Experiences
“The rehabilitation program was fine, it was simple. […] When I finished the program, I breathed better, and I felt more calm”.(Patient ID 6)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rossini, M.; Rizzo, P.; Bononi, I.; Clementz, A.; Ferrari, R.; Martini, F.; Tognon, M.G. New Perspectives on Diagnosis and Therapy of Malignant Pleural Mesothelioma. Front. Oncol. 2018, 8, 91. [Google Scholar] [CrossRef] [PubMed]
- Opitz, I. Management of malignant pleural mesothelioma-The European experience. J. Thorac. Dis. 2014, 6 (Suppl. S2), S238–S252. [Google Scholar] [PubMed]
- Bille, A.; Okiror, L.; Harling, L.; Pernazza, F.; Muzio, A.; Roveta, A.; Grosso, F. Analysis of survival of patients with metastatic malignant pleural mesothelioma. Tumori 2020, 107, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Solli, P.; Brandolini, J.; Pardolesi, A.; Nardini, M.; Lacava, N.; Parri, S.F.; Kawamukai, K.; Bonfanti, B.; Bertolaccini, L. Diaphragmatic and pericardial reconstruction after surgery for malignant pleural mesothelioma. J. Thorac. Dis. 2018, 10 (Suppl. S2), S298–S303. [Google Scholar] [CrossRef] [PubMed]
- Grosso, F.; D’Ambrosio, L.; Zucchetti, M.; Ibrahim, T.; Tamberi, S.; Matteo, C.; Rulli, E.; Comandini, D.; Palmerini, E.; Baldi, G.G. Pharmacokinetics, safety, and activity of trabectedin as first-line treatment in elderly patients who are affected by advanced sarcoma and are unfit to receive standard chemotherapy: A phase 2 study (TR1US study) from the Italian Sarcoma Group. Cancer 2020, 126, 4726–4734. [Google Scholar] [CrossRef] [PubMed]
- Metaxas, Y.; Fruh, M.; Eboulet, E.I.; Grosso, F.; Pless, M.; Zucali, P.A.; Ceresoli, G.L.; Mark, M.; Schneider, M.; Maconi, A.; et al. Lurbinectedin as second- or third-line palliative therapy in malignant pleural mesothelioma: An international, multi-centre, single-arm, phase II trial (SAKK 17/16). Ann. Oncol. 2020, 31, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Grosso, F.; Steele, N.; Novello, S.; Nowak, A.K.; Popat, S.; Greillier, L.; John, T.; Leighl, N.B.; Reck, M.; Taylor, P.; et al. Nintedanib Plus Pemetrexed/Cisplatin in Patients With Malignant Pleural Mesothelioma: Phase II Results From the Randomized, Placebo-Controlled LUME-Meso Trial. J. Clin. Oncol. 2017, 35, 3591–3600. [Google Scholar] [CrossRef] [PubMed]
- Grosso, F.; Roveta, A.; Gallizzi, G.; Belletti, M. Management of recurrent pleural mesothelioma: Successful rechallenge with nintedanib in combination with chemotherapy. Clin. Case Rep. 2018, 6, 2000–2004. [Google Scholar] [CrossRef] [PubMed]
- Scagliotti, G.V.; Nowak, A.K.; Nakano, T.; van Meerbeeck, J.; Popat, S.; Vogelzang, N.J.; Grosso, F.; Aboelhassan, R.; Jakopovic, M.; Ceresoli, G.L.; et al. Nintedanib in combination with pemetrexed and cisplatin for chemotherapy-naive patients with advanced malignant pleural mesothelioma (LUME-Meso): A double-blind, randomised, placebo-controlled phase 3 trial. Lancet Respir. Med. 2019, 7, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Vogelzang, N.J.; Rusthoven, J.J.; Symanowski, J.; Denham, C.; Kaukel, E.; Ruffie, P.; Gatzemeier, U.; Boyer, M.; Emri, S.; Manegold, C.; et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J. Clin. Oncol. 2003, 21, 2636–2644. [Google Scholar] [CrossRef]
- Ceresoli, G.L.; Zucali, P.A.; Favaretto, A.G.; Grossi, F.; Bidoli, P.; Del Conte, G.; Ceribelli, A.; Bearz, A.; Morenghi, E.; Cavina, R.; et al. Phase II study of pemetrexed plus carboplatin in malignant pleural mesothelioma. J. Clin. Oncol. 2006, 24, 1443–1448. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Stahel, R.A.; Nackaerts, K.; Baas, P.; Karthaus, M.; Eberhardt, W.; Paz-Ares, L.; Sundstrom, S.; Liu, Y.; Ripoche, V.; et al. Pemetrexed plus cisplatin or pemetrexed plus carboplatin for chemonaïve patients with malignant pleural mesothelioma: Results of the International Expanded Access Program. J. Thorac. Oncol. 2008, 3, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Yap, T.A.; Aerts, J.G.; Popat, S.; Fennell, D.A. Novel insights into mesothelioma biology and implications for therapy. Nat. Rev. Cancer 2017, 17, 475–488. [Google Scholar] [CrossRef] [PubMed]
- Scherpereel, A.; Astoul, P.; Baas, P.; Berghmans, T.; Clayson, H.; de Vuyst, P.; Dienemann, F.; Galateau-Salle, C.; Hennequin, G.; Hillerdal, C.; et al. Guidelines of the European Respiratory Society and the European Society of Thoracic Surgeons for the management of malignant pleural mesothelioma. Eur. Respir. J. 2010, 35, 479–495. [Google Scholar] [CrossRef] [PubMed]
- Ceruti, P.; Lonni, S.; Baglivo, F.; Marchetti, G. Endoscopic diagnosis and management of pleural effusion in malignant pleural mesothelioma. J. Thorac. Dis. 2018, 10, S269–S275. [Google Scholar] [CrossRef]
- Brims, F.J.; Davies, H.E.; Lee, Y.C. Respiratory chest pain: Diagnosis and treatment. Med. Clin. N. Am. 2010, 94, 217–232. [Google Scholar] [CrossRef]
- Moore, S.; Darlison, L.; Tod, A.M. Living with mesothelioma. A literature review. Eur. J. Cancer Care 2010, 19, 458–468. [Google Scholar] [CrossRef] [PubMed]
- Lippi, L.; D’Abrosca, F.; Folli, A.; Turco, A.; Curci, C.; Ammendolia, A.; de Sire, A.; Invernizzi, M. Rehabilitation interventions for weaning from mechanical ventilation in patients with spinal cord injury: A systematic review. J. Back. Musculoskelet. Rehabil. 2023, 36, 577–593. [Google Scholar] [CrossRef] [PubMed]
- Lippi, L.; de Sire, A.; D’Abrosca, F.; Polla, B.; Marotta, N.; Castello, L.M.; Ammendolia, A.; Molinari, C.; Invernizzi, M. Efficacy of Physiotherapy Interventions on Weaning in Mechanically Ventilated Critically Ill Patients: A Systematic Review and Meta-Analysis. Front. Med. 2022, 9, 889218. [Google Scholar] [CrossRef]
- Ferrillo, M.; Migliario, M.; Marotta, N.; Lippi, L.; Antonelli, A.; Calafiore, D.; Ammendolia, V.; Fortunato, L.; Renò, F.; Giudice, A.; et al. Oral Health in Breast Cancer Women with Vitamin D Deficiency: A Machine Learning Study. J. Clin. Med. 2022, 11, 4662. [Google Scholar] [CrossRef]
- Invernizzi, M.; de Sire, A.; Lippi, L.; Venetis, K.; Sajjadi, E.; Gimigliano, F.; Gennari, A.; Criscitiello, C.; Cisari, C.; Fusco, N. Impact of Rehabilitation on Breast Cancer Related Fatigue: A Pilot Study. Front. Oncol. 2020, 10, 556718. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 statement: Defining standard protocol items for clinical trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef]
- Tombaugh, T.N.; McIntyre, N.J. The mini-mental state examination: A comprehensive review. J. Am. Geriatr. Soc. 1992, 40, 922–935. [Google Scholar] [CrossRef]
- Mor, V.; Laliberte, L.; Morris, J.N.; Wiemann, M. The Karnofsky Performance Status Scale. An examination of its reliability and validity in a research setting. Cancer 1984, 53, 2002–2007. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194.26. [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (Strobe): Explanation and elaboration. Ann. Intern. Med. 2007, 147, W163–W194. [Google Scholar] [CrossRef]
- Pestelli, M.T.; D’Abrosca, F.; Tognetti, P.; Grecchi, B.; Nicolini, A.; Solidoro, P. Do not forget the lungs: Preliminary feasibility study on I/E mode physiotherapy for people recovering from COVID-19. Panminerva Med. 2022, 64, 208–214. [Google Scholar] [CrossRef]
- de Fátima Ribeiro Silva, C.; Ohara, D.G.; Matos, A.P.; Pinto, A.; Pegorari, M.S. Short Physical Performance Battery as a Measure of Physical Performance and Mortality Predictor in Older Adults: A Comprehensive Literature Review. Int. J. Environ. Res. Public Health 2021, 18, 10612. [Google Scholar] [CrossRef] [PubMed]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef]
- Brooks, D.; Parsons, J.; Tran, D.; Jeng, B.; Gorczyca, B.; Newton, J.; Lo, V.; Dear, C.; Silaj, E.; Hawn, T. The two-minute walk test as a measure of functional capacity in cardiac surgery patients. Arch. Phys. Med. Rehabil. 2004, 85, 1525–1530. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Bubela, D.; Magasi, S.; McCreath, H.; Wang, Y.C.; Reuben, D.; Rymer, W.Z.; Gershon, R. Comparison of walking performance over the first 2 minutes and the full 6 minutes of the Six-Minute Walk Test. BMC Res. Notes 2014, 7, 269. [Google Scholar] [CrossRef] [PubMed]
- Mahler, D.A.; Horowitz, M.B. Perception of breathlessness during exercise in patients with respiratory disease. Med. Sci. Sports Exerc. 1994, 26, 1078–1081. [Google Scholar] [CrossRef] [PubMed]
- NIHR Southampton Biomedical Research Centre. Procedure for measuring gripstrength using the JAMAR dynamometer. In NHR; NIHR Southampton Biomedical Research Centre: Southampton, UK, 2016. [Google Scholar]
- Wang, Y.C.; Bohannon, R.W.; Li, X.; Sindhu, B.; Kapellusch, J. Hand-Grip Strength: Normative Reference Values and Equations for Individuals 18 to 85 Years of Age Residing in the United States. J. Orthop. Sports Phys. Ther. 2018, 48, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Hjermstad, M.J.; Fayers, P.M.; Haugen, D.F.; Caraceni, A.; Hanks, G.W.; Loge, J.H.; Fainsinger, R.; Aass, N.; European Palliative Care Research Collaborative (EPCRC). Studies comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for assessment of pain intensity in adults: A systematic literature review. J. Pain. Symptom Manag. 2011, 41, 1073–1093. [Google Scholar] [CrossRef] [PubMed]
- Valentini, A.; Federici, M.; Cianfarani, M.A.; Tarantino, U.; Bertoli, A. Frailty and nutritional status in older people: The Mini Nutritional Assessment as a screening tool for the identification of frail subjects. Clin. Interv. Aging 2018, 13, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Fayers, P.; Aaronson, N.K.; Bjordal, K.; Sullivan, M. EORTC QLQ–C30 Scoring Manual; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 1995. [Google Scholar]
- Hollen, P.J.; Gralla, R.J.; Liepa, A.M.; Symanowski, J.T.; Rusthoven, J.J. Measuring quality of life in patients with pleural mesothelioma using a modified version of the Lung Cancer Symptom Scale (LCSS): Psychometric properties of the LCSS-Meso. Support. Care Cancer 2006, 14, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.; Riley, W.; Stone, A.; Rothrock, N.; Reeve, B.; Yount, S.; Amtmann, D.; Bode, R.; Buysse, D.; Choi, S.; et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. J. Clin. Epidemiol. 2010, 63, 1179–1194. [Google Scholar] [CrossRef] [PubMed]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Hassani, S.; Mohammadi Shahboulagi, F.; Foroughan, M.; Nadji, S.A.; Tabarsi, P.; Ghaedamini Harouni, G. Factors Associated with Medication Adherence in Elderly Individuals with Tuberculosis: A Qualitative Study. Can. J. Infect. Dis. Med. Microbiol. 2023, 2023, 4056548. [Google Scholar] [CrossRef]
- Invernizzi, M.; Corti, C.; Lopez, G.; Michelotti, A.; Despini, L.; Gambini, D.; Lorenzini, D.; Guerini-Rocco, E.; Maggi, S.; Noale, M.; et al. Lymphovascular invasion and extranodal tumour extension are risk indicators of breast cancer related lymphoedema: An observational retrospective study with long-term follow-up. BMC Cancer 2018, 18, 935. [Google Scholar] [CrossRef]
- Zanini, A.; Crisafulli, E.; D’Andria, M.; Gregorini, C.; Cherubino, F.; Zampogna, E.; Azzola, A.; Spanevello, A.; Schiavone, N.; Chetta, A. Minimum Clinically Important Difference in 30-s Sit-to-Stand Test After Pulmonary Rehabilitation in Subjects With COPD. Respir. Care 2019, 64, 1261–1269. [Google Scholar] [CrossRef]
- Johnston, K.N.; Potter, A.J.; Phillips, A.C. Minimal important difference and responsiveness of 2-minute walk test performance in people with COPD undergoing pulmonary rehabilitation. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 2849–2857. [Google Scholar] [CrossRef]
- Terwee, C.B.; Peipert, J.D.; Chapman, R.; Lai, J.S.; Terluin, B.; Cella, D.; Griffiths, P.; Mokkink, L.B. Minimal important change (MIC): A conceptual clarification and systematic review of MIC estimates of PROMIS measures. Qual. Life Res. 2021, 30, 2729–2754. [Google Scholar] [CrossRef]
- Baas, P.; Daumont, M.J.; Lacoin, L.; Penrod, J.R.; Carroll, R.; Venkatesan, S.; Ubhi, U.; Calleja, A.; Snee, M. Treatment patterns and outcomes for patients with malignant pleural mesothelioma in England in 2013-2017: A nationwide CAS registry analysis from the I-O Optimise initiative. Lung Cancer 2021, 162, 185–193. [Google Scholar] [CrossRef]
- Ho, S.; Culligan, M.; Friedberg, J.; Goloubeva, O.; Marchese, V. Examining the impact of physical function performance in predicting patient outcomes after lung-sparing surgery for malignant pleural mesothelioma. Disabil. Rehabil. 2022, 44, 6676–6683. [Google Scholar] [CrossRef]
- de Sire, A.; Losco, L.; Cigna, E.; Lippi, L.; Gimigliano, F.; Gennari, A.; Cisari, C.; Chen, H.C.; Fusco, N.; Invernizzi, M. Three-dimensional laser scanning as a reliable and reproducible diagnostic tool in breast cancer related lymphedema rehabilitation: A proof-of-principle study. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 4476–4485. [Google Scholar]
- Invernizzi, M.; Runza, L.; de Sire, A.; Lippi, L.; Blundo, C.; Gambini, D.; Boldorini, R.; Ferrero, S.; Fusco, N. Integrating Augmented Reality Tools in Breast Cancer Related Lymphedema Prognostication and Diagnosis. J. Vis. Exp. 2020, 6, 156. [Google Scholar]
- Nakano, J.; Fukushima, T.; Tanaka, T.; Fu, J.B.; Morishita, S. Physical function predicts mortality in patients with cancer: A systematic review and meta-analysis of observational studies. Support. Care Cancer 2021, 29, 5623–5634. [Google Scholar] [CrossRef]
- Granger, C.L.; McDonald, C.F.; Irving, L.; Clark, R.A.; Gough, K.; Murnane, A.; Gough, K.; Murnane, A.; Mileshkin, L.; Krishnasamy, M.; et al. Low physical activity levels and functional decline in individuals with lung cancer. Lung Cancer 2014, 83, 292–299. [Google Scholar] [CrossRef]
- Mujovic, N.; Mujovic, N.; Subotic, D.; Ercegovac, M.; Milovanovic, A.; Nikcevic, L.; Zugic, V.; Nikolic, D. Influence of Pulmonary Rehabilitation on Lung Function Changes After the Lung Resection for Primary Lung Cancer in Patients with Chronic Obstructive Pulmonary Disease. Aging Dis. 2015, 6, 466–477. [Google Scholar] [CrossRef]
- Ilonen, I.K.; Rasanen, J.V.; Sihvo, E.I.; Knuuttila, A.; Sovijarvi, A.R.; Sintonen, H.; Salo, J.A. Pneumonectomy: Post-operative quality of life and lung function. Lung Cancer 2007, 58, 397–402. [Google Scholar] [CrossRef]
- Lima, L.N.; da Silva, R.A.; Gross, J.L.; Deheinzelin, D.; Negri, E.M. Assessment of pulmonary function and quality of life in patients submitted to pulmonary resection for cancer. J. Bras. Pneumol. 2009, 35, 521–528. [Google Scholar] [CrossRef]
- Bredin, M.; Corner, J.; Krishnasamy, M.; Plant, H.; Bailey, C.; A’Hern, R. Multicentre randomised controlled trial of nursing intervention for breathlessness in patients with lung cancer. BMJ 1999, 318, 901–904. [Google Scholar] [CrossRef] [PubMed]
- Hately, J.; Laurence, V.; Scott, A.; Baker, R.; Thomas, P. Breathlessness clinics within specialist palliative care settings can improve the quality of life and functional capacity of patients with lung cancer. Palliat. Med. 2003, 17, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Barton, R.; English, A.; Nabb, S.; Rigby, A.S.; Johnson, M.J. A randomised trial of high vs low intensity training in breathing techniques for breathless patients with malignant lung disease: A feasibility study. Lung Cancer 2010, 70, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.J.; Kanaan, M.; Richardson, G.; Nabb, S.; Torgerson, D.; English, A. A randomised controlled trial of three or one breathing technique training sessions for breathlessness in people with malignant lung disease. BMC Med. 2015, 13, 213. [Google Scholar] [CrossRef]
- Molassiotis, A.; Charalambous, A.; Taylor, P.; Stamataki, Z.; Summers, Y. The effect of resistance inspiratory muscle training in the management of breathlessness in patients with thoracic malignancies: A feasibility randomised trial. Support. Care Cancer 2014, 23, 1637–1645. [Google Scholar] [CrossRef]
- Jeffery, E.; Lee, Y.C.G.; Newton, R.U.; Lyons-Wall, P.; McVeigh, J.; Nowak, A.K.; Cheah, H.M.; Nguyen, B.; Fitzgerald, D.B.; Creaney, J.; et al. Body composition and nutritional status in malignant pleural mesothelioma: Implications for activity levels and quality of life. Eur. J. Clin. Nutr. 2019, 73, 1412–1421. [Google Scholar] [CrossRef]
- Tanaka, T.; Morishita, S.; Hashimoto, M.; Nakamichi, T.; Uchiyama, Y.; Hasegawa, S.; Hasegawa, S.; Domen, K. Physical function and health-related quality of life in the convalescent phase in surgically treated patients with malignant pleural mesothelioma. Support. Care Cancer 2019, 27, 4107–4113. [Google Scholar] [CrossRef]
- Tanaka, T.; Morishita, S.; Hashimoto, M.; Itani, Y.; Mabuchi, S.; Kodama, N.; Hasegawa, S.; Domen, K. Physical function and health-related quality of life in patients undergoing surgical treatment for malignant pleural mesothelioma. Support. Care Cancer 2017, 25, 2569–2575. [Google Scholar] [CrossRef]
- de Sire, A.; Lippi, L.; Aprile, V.; Calafiore, D.; Folli, A.; D’Abrosca, F.; Moalli, S.; Lucchi, M.; Ammendolia, A.; Invernizzi, M. Pharmacological, Nutritional, and Rehabilitative Interventions to Improve the Complex Management of Osteoporosis in Patients with Chronic Obstructive Pulmonary Disease: A Narrative Review. J. Pers. Med. 2022, 12, 1626. [Google Scholar] [CrossRef] [PubMed]
- Lippi, L.; Folli, A.; Curci, C.; D’Abrosca, F.; Moalli, S.; Mezian, K.; de Sire, A.; Invernizzi, M. Osteosarcopenia in Patients with Chronic Obstructive Pulmonary Diseases: Which Pathophysiologic Implications for Rehabilitation? Int. J. Environ. Res. Public Health 2022, 19, 14314. [Google Scholar] [CrossRef] [PubMed]
- Lippi, L.; Turco, A.; Folli, A.; D’Abrosca, F.; Curci, C.; Mezian, K.; de Sire, A.; Invernizzi, M. Technological advances and digital solutions to improve quality of life in older adults with chronic obstructive pulmonary disease: A systematic review. Aging Clin. Exp. Res. 2023, 35, 953–968. [Google Scholar] [CrossRef] [PubMed]
- Lippi, L.; D’Abrosca, F.; Folli, A.; Dal Molin, A.; Moalli, S.; Maconi, A.; Ammendolia, A.; de Sire, A.; Invernizzi, M. Closing the Gap between Inpatient and Outpatient Settings: Integrating Pulmonary Rehabilitation and Technological Advances in the Comprehensive Management of Frail Patients. Int. J. Environ. Res. Public Health 2022, 19, 9150. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | Value |
|---|---|
| Patients (n = 7) | |
| Age (years) | 67 ± 6 |
| Female | 1 (14.3%) |
| Male | 6 (85.7%) |
| Weight (kg) | 76.71 ± 12.89 |
| Height (cm) | 172 ± 6.71 |
| BMI (kg/m2) | 26.05 ± 5.04 |
| Smokers | 2 (28.6%) |
| Comorbidities | |
| Diabetes Mellitus | 3 (42.9%) |
| Myocardial Infarction | 1 (14.3%) |
| Chronic Obstructive Pulmonary Disease | 1 (14.3%) |
| Arterial Hypertension | 3 (42.9%) |
| Benign Prostatic Hypertrophy | 1 (14.3%) |
| Dyslipidemia | 2 (28.6%) |
| Level of physical activity * | |
| None | 4 (57.1%) |
| Low | 1 (14.3%) |
| Medium | 2 (28.6%) |
| High | 0 (0.0%) |
| Histology | |
| Epithelioid | 7 (100%) |
| Sarcomatoid | 0 (0%) |
| Biphasic/mixed | 0 (0%) |
| Right-side tumor | 6 (85.7%) |
| Left-side tumor | 1 (14.3%) |
| Stage | |
| IA | 2 (28.6%) |
| IB | 2 (28.6%) |
| II | 0 (0%) |
| IIIA | 2 (28.6%) |
| IIIB | 1 (14.3%) |
| IV | 0 (0%) |
| Grade | |
| Low | 2 (28.6%) |
| High | 5 (71.4%) |
| Pleural Surgery | |
| Pleurodesis with talc | 4 (57.1%) |
| Pleurectomy/decortication | 2 (28.6%) |
| No surgery | 1 (14.3%) |
| Radiotherapy | 0 (0.0%) |
| Chemotherapy | 7 (100%) |
| T0 (n = 7) | T1 (n = 7) | T2 (n = 7) | T0–T1 | T0–T2 | MCID | T0–T1 | T0–T2 | |
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean | p Value | p Value | |
| HGS (kg) | 31.07 ± 4.51 | 34.10 ± 9.1 | 33.5 ± 6.65 | −3.03 ± 6.74 | −2.43 ± 3.20 | 5.5 | 0.375 | 0.1094 |
| SPPB | 11.42 ± 0.79 | 11 ± 0.82 | 10.71 ± 1.11 | 0.43 ± 1.40 | 0.71 ± 1.60 | 1 | 0.625 | 0.3125 |
| Submaximal Exercise Capacity | ||||||||
| 2MWT (m) | 132 ± 17.15 | 149.43 ± 27.61 | 131.43 ± 23.60 | −17.43 ± 23.86 | 0.57 ± 21.77 | 5.5 | 0.1875 | 0.9531 |
| 2MWT (RPE Borg) | 2.36 ± 2.14 | 2.43 ± 1.90 | 1.86 ± 1.57 | −0.07 ± 2.86 | 0.5 ± 2.7 | 1 | >0.9999 | 0.67 |
| 2MWT (SpO2) | 96.14 ± 0.9 | 95.42 ± 43 | 90.86 ± 3.39 | 0.71 ± 3.35 | 5.28 ± 4.07 | - | 0.7031 | 0.03 * |
| 30secSTS | 9.71 ± 2.29 | 11.42 ± 2.37 | 15.57 ± 4.08 | −1.71 ± 3.30 | −5.86 ± 5.11 | 2 | 0.4375 | 0.046 * |
| T0 (n = 7) | T1 (n = 7) | T2 (n = 7) | T0–T1 | T0–T2 | |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | p Value | p Value | |
| Arterial Blood Gas Test | |||||
| PaO2 | 78 ± 4.64 | 83.84 ± 6.21 | 75.68 ± 10.99 | 0.58 | 0.99 |
| PaCO2 | 39.79 ± 4.6 | 41.51 ± 3.15 | 40.74 ± 4.80 | 0.16 | 0.12 |
| pH | 7.44 ± 0.04 | 7.42 ± 0.02 | 7.40 ± 0.03 | 0.12 | 0.12 |
| Pulmonary Function | |||||
| FEV1 (L) | 2.41 ± 0.81 | 2.35 ± 0.72 | 2.14 ± 0.54 | 0.50 | 0.16 |
| FVC (L) | 2.86 ± 0.92 | 2.89 ± 0.88 | 2.66 ± 0.69 | 0.34 | 0.22 |
| DLCO (% predicted) | 68.17 ± 13.93 | 65.71 ± 12.43 | 61.43 ± 12.42 | 0.91 | 0.22 |
| PEF | 6.61 ± 2.04 | 7.58 ± 2.09 | 7.67 ± 1.91 | 0.09 | 0.62 |
| T0 (n = 7) | T1 (n = 7) | T2 (n = 7) | T0–T1 | T0–T2 | MCID | T0–T1 | T0–T2 | |
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean | p Value | p Value | |
| VAS | 20.00 ± 23.27 | 8.14 ± 10.37 | 9.29 ± 7.87 | 11.86 ±18.33 | 10.71 ± 22.07 | 10 | 0.19 | 0.36 |
| MNA | 25.2 ± 2.36 | 26.57 ± 1.64 | 25.36 ± 2.72 | −1.43 ± 2.32 | −0.21 ± 2.46 | - | 0.89 | 0.36 |
| EORTC QLQ-C30 | ||||||||
| Functional score | 25.83 ± 9.30 | 23.86 ± 7.03 | 21.57 ± 5.50 | 2.00 ± 3.37 | 4.28 ± 4.49 | 7.5 | 0.12 | 0.09 |
| Symptom score | 20.67 ± 5.24 | 18.86 ± 4.78 | 18.71 ± 3.04 | 1.57 ± 3.69 | 1.71 ± 1.98 | 7.5 | 0.34 | 0.12 |
| Global Health score | 6.50 ± 1.23 | 5.85 ± 0.69 | 6.00 ± 1.00 | 0.57 ± 1.27 | 0.43 ± 0.98 | 7.5 | 0.50 | 0.50 |
| PROMIS | 131.29 ± 44.35 | 121.14 ± 35.93 | 116 ± 32.90 | 10.14 ± 31.20 | 15. 29 ± 26.54 | 4 | 0.45 | 0.30 |
| LCSS-meso | 29.05 ± 20.25 | 34.63 ± 20.45 | 36.75 ± 16.9 | −5.57 ± 6.44 | −7.70 ± 7.86 | - | 0.08 | 0.047 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lippi, L.; de Sire, A.; Folli, A.; Curci, C.; Calafiore, D.; Lombardi, M.; Bertolaccini, L.; Turco, A.; Ammendolia, A.; Fusco, N.; et al. Comprehensive Pulmonary Rehabilitation for Patients with Malignant Pleural Mesothelioma: A Feasibility Pilot Study. Cancers 2024, 16, 2023. https://doi.org/10.3390/cancers16112023
Lippi L, de Sire A, Folli A, Curci C, Calafiore D, Lombardi M, Bertolaccini L, Turco A, Ammendolia A, Fusco N, et al. Comprehensive Pulmonary Rehabilitation for Patients with Malignant Pleural Mesothelioma: A Feasibility Pilot Study. Cancers. 2024; 16(11):2023. https://doi.org/10.3390/cancers16112023
Chicago/Turabian StyleLippi, Lorenzo, Alessandro de Sire, Arianna Folli, Claudio Curci, Dario Calafiore, Mariano Lombardi, Luca Bertolaccini, Alessio Turco, Antonio Ammendolia, Nicola Fusco, and et al. 2024. "Comprehensive Pulmonary Rehabilitation for Patients with Malignant Pleural Mesothelioma: A Feasibility Pilot Study" Cancers 16, no. 11: 2023. https://doi.org/10.3390/cancers16112023
APA StyleLippi, L., de Sire, A., Folli, A., Curci, C., Calafiore, D., Lombardi, M., Bertolaccini, L., Turco, A., Ammendolia, A., Fusco, N., Spaggiari, L., & Invernizzi, M. (2024). Comprehensive Pulmonary Rehabilitation for Patients with Malignant Pleural Mesothelioma: A Feasibility Pilot Study. Cancers, 16(11), 2023. https://doi.org/10.3390/cancers16112023