
Use of Different Anti-PD-1 Checkpoint Combination Strategies for First-Line Advanced NSCLC Treatment—The Experience of Ion Chiricuță Oncology Institute

 , , , and
, , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Procedures
2.2. Outcomes
2.3. Statistical Analysis
3. Results
3.1. Patients and Treatment
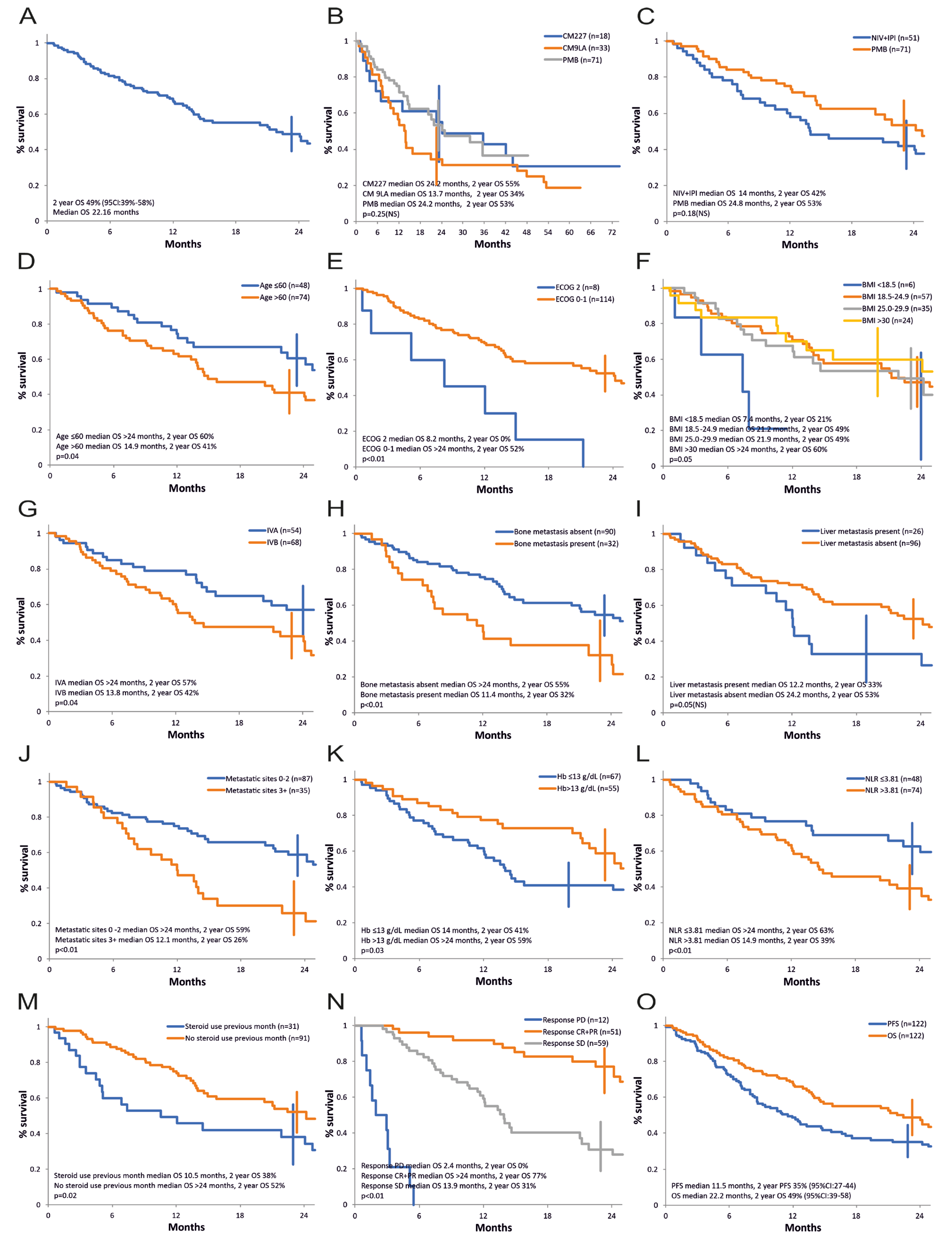
3.2. Overall Survival
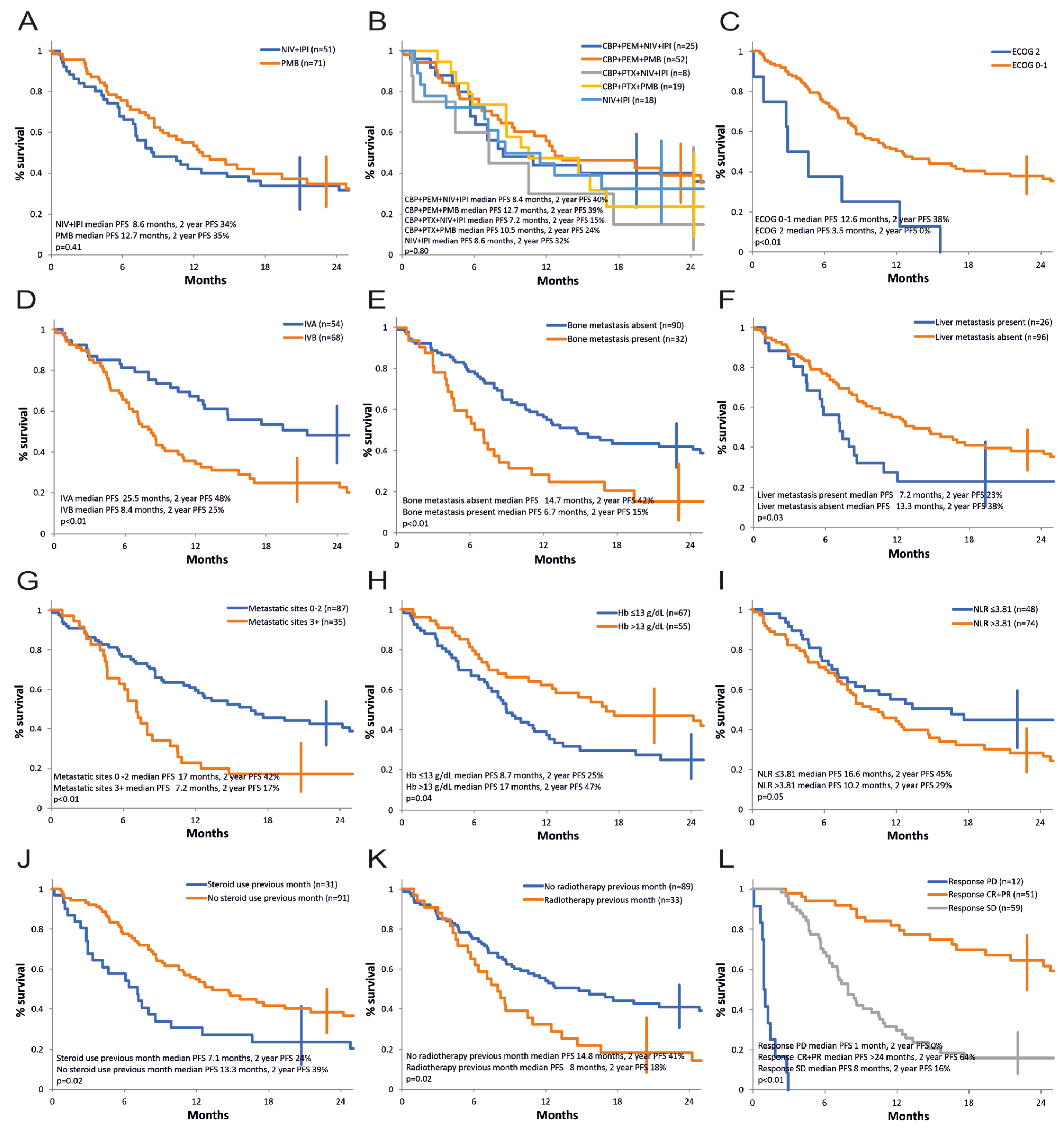
3.3. Progression-Free Survival
3.4. Tumor Response
3.5. Treatment beyond Progression
3.6. Subsequent Treatments
3.7. Long-Term Survivors
3.8. Toxicity
4. Discussion
4.1. Landscape of the Immunotherapy Combinations
4.2. Rationale for the Immunotherapy Combinations—The Complementary Mechanisms of Action
4.3. Purpose and Limitations of the Study
4.4. Overall Survival, Progression-Free Survival, and Long-Term Survivors
4.5. Univariate and Multivariate Analysis of the Prognostic Factors
- -
- Four independent prognostic factors for OS (unfavorable being deteriorated ECOG performance status (2 vs. 0–1) (p = 0.02, OR 2.17, 95% CI 1.08 to 4.36), older age at study entry (p = 0.02, OR 1.03, 95% CI 1.004 to 1.07), use of corticotherapy in the first month of the treatment (yes vs. no) (p = 0.04, OR 1.79, 95% CI 1.01 to 3.16), neutrophil/leukocyte ratio (>3.81 vs. ≤3.81) (p = 0.03, OR 1.81, 95% CI 1.04 to 3.15).
- -
- One independent prognostic factor for PFS: ECOG status (2 vs. 0–1) (p = 0.02, OR 2.03, 95% CI 1.08 to 3.79).
- -
- Three independent prognostic factors for obtaining a clinical benefit: ECOG PS (2 vs. 0–1) (OR 12, 95% CI 1.59 to 90.35, p = 0.015), age (≥61 vs. <61) (OR 1.17, 95% CI 1.03 to 1.34, p = 0.01), and use of corticotherapy in the first month of the treatment (yes vs. no) (OR 9.56, 95% CI 1.75 to 52.13, p = 0.009).
4.6. Performance Status
4.7. Age
4.8. Corticosteroids
4.9. Neutrophil-to-Lymphocyte Ratio
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Gogishvili, M.; Melkadze, T.; Makharadze, T.; Giorgadze, D.; Dvorkin, M.; Penkov, K.; Laktionov, K.; Nemsadze, G.; Nechaeva, M.; Rozhkova, I.; et al. Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer: A randomized, controlled, double-blind phase 3 trial. Nat. Med. 2022, 28, 2374–2380. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Paz-Ares, L.; Bernabe Caro, R.; Zurawski, B.; Kim, S.W.; Carcereny Costa, E.; Park, K.; Alexandru, A.; Lupinacci, L.; de la Mora Jimenez, E.; et al. Nivolumab plus Ipilimumab in Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for First-Line Treatment of PD-L1-Selected Patients with NSCLC. N. Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef]
- Johnson, M.L.; Cho, B.C.; Luft, A.; Alatorre-Alexander, J.; Geater, S.L.; Laktionov, K.; Kim, S.W.; Ursol, G.; Hussein, M.; Lim, F.L.; et al. Durvalumab With or Without Tremelimumab in Combination With Chemotherapy as First-Line Therapy for Metastatic Non-Small-Cell Lung Cancer: The Phase III POSEIDON Study. J. Clin. Oncol. 2023, 41, 1213–1227. [Google Scholar] [CrossRef]
- Mok, T.S.K.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): An international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Sezer, A.; Kilickap, S.; Gümüş, M.; Bondarenko, I.; Özgüroğlu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: A multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet 2021, 397, 592–604. [Google Scholar] [CrossRef] [PubMed]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- West, H.; McCleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, H.J.; Kopp, H.G.; Daniel, D.; McCune, S.; Mekhail, T.; et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef]
- O’Quigley, J. Survival Analysis: Proportional and Non-Proportional Hazards Regression; Springer International Publishing: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Rosner, B. Fundamentals of Biostatistics; Cengage Learning: Boston, MA, USA, 2015. [Google Scholar]
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; Wiley: Hoboken, NJ, USA, 2013. [Google Scholar]
- Wang, Y.; Han, H.; Zhang, F.; Lv, T.; Zhan, P.; Ye, M.; Song, Y.; Liu, H. Immune checkpoint inhibitors alone vs immune checkpoint inhibitors-combined chemotherapy for NSCLC patients with high PD-L1 expression: A network meta-analysis. Br. J. Cancer 2022, 127, 948–956. [Google Scholar] [CrossRef]
- Das, R.; Verma, R.; Sznol, M.; Boddupalli, C.S.; Gettinger, S.N.; Kluger, H.; Callahan, M.; Wolchok, J.D.; Halaban, R.; Dhodapkar, M.V.; et al. Combination therapy with anti-CTLA-4 and anti-PD-1 leads to distinct immunologic changes in vivo. J. Immunol. 2015, 194, 950–959. [Google Scholar] [CrossRef]
- Sharma, P.; Allison, J.P. Dissecting the mechanisms of immune checkpoint therapy. Nat. Rev. Immunol. 2020, 20, 75–76. [Google Scholar] [CrossRef]
- Wei, S.C.; Duffy, C.R.; Allison, J.P. Fundamental Mechanisms of Immune Checkpoint Blockade Therapy. Cancer Discov. 2018, 8, 1069–1086. [Google Scholar] [CrossRef]
- Bracci, L.; Schiavoni, G.; Sistigu, A.; Belardelli, F. Immune-based mechanisms of cytotoxic chemotherapy: Implications for the design of novel and rationale-based combined treatments against cancer. Cell Death Differ. 2014, 21, 15–25. [Google Scholar] [CrossRef]
- Judd, J.; Borghaei, H. Combining Immunotherapy and Chemotherapy for Non-Small Cell Lung Cancer. Thorac. Surg. Clin. 2020, 30, 199–206. [Google Scholar] [CrossRef]
- Leonetti, A.; Wever, B.; Mazzaschi, G.; Assaraf, Y.G.; Rolfo, C.; Quaini, F.; Tiseo, M.; Giovannetti, E. Molecular basis and rationale for combining immune checkpoint inhibitors with chemotherapy in non-small cell lung cancer. Drug Resist. Updat. 2019, 46, 100644. [Google Scholar] [CrossRef]
- Palmer, A.C.; Izar, B.; Hwangbo, H.; Sorger, P.K. Predictable Clinical Benefits without Evidence of Synergy in Trials of Combination Therapies with Immune-Checkpoint Inhibitors. Clin. Cancer Res. 2022, 28, 368–377. [Google Scholar] [CrossRef]
- Peng, J.; Hamanishi, J.; Matsumura, N.; Abiko, K.; Murat, K.; Baba, T.; Yamaguchi, K.; Horikawa, N.; Hosoe, Y.; Murphy, S.K.; et al. Chemotherapy Induces Programmed Cell Death-Ligand 1 Overexpression via the Nuclear Factor-κB to Foster an Immunosuppressive Tumor Microenvironment in Ovarian Cancer. Cancer Res. 2015, 75, 5034–5045. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, T.; Lycan, T.; Dothard, A.; Ehrlichman, P.; Ruiz, J.; Farris, M.; Topaloglu, U.; Levine, B.; Grant, S.; Klepin, H.D.; et al. Performance Status and Age as Predictors of Immunotherapy Outcomes in Advanced Non-Small-Cell Lung Cancer. Clin Lung Cancer 2020, 21, e286–e293. [Google Scholar] [CrossRef] [PubMed]
- Dall’Olio, F.G.; Maggio, I.; Massucci, M.; Mollica, V.; Fragomeno, B.; Ardizzoni, A. ECOG performance status ≥2 as a prognostic factor in patients with advanced non small cell lung cancer treated with immune checkpoint inhibitors-A systematic review and meta-analysis of real world data. Lung Cancer 2020, 145, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, F.; Di Maio, M.; Perrone, F.; Tiseo, M. First-line immunotherapy in non-small cell lung cancer patients with poor performance status: A systematic review and meta-analysis. Transl. Lung Cancer Res 2021, 10, 2917–2936. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Garon, E.B.; Kim, D.W.; Cho, B.C.; Gervais, R.; Perez-Gracia, J.L.; Han, J.Y.; Majem, M.; Forster, M.D.; Monnet, I.; et al. Five Year Survival Update From KEYNOTE-010: Pembrolizumab Versus Docetaxel for Previously Treated, Programmed Death-Ligand 1-Positive Advanced NSCLC. J. Thorac. Oncol. 2021, 16, 1718–1732. [Google Scholar] [CrossRef] [PubMed]
- Spigel, D.R.; McCleod, M.; Jotte, R.M.; Einhorn, L.; Horn, L.; Waterhouse, D.M.; Creelan, B.; Babu, S.; Leighl, N.B.; Chandler, J.C.; et al. Safety, Efficacy, and Patient-Reported Health-Related Quality of Life and Symptom Burden with Nivolumab in Patients with Advanced Non-Small Cell Lung Cancer, Including Patients Aged 70 Years or Older or with Poor Performance Status (CheckMate 153). J. Thorac. Oncol. 2019, 14, 1628–1639. [Google Scholar] [CrossRef] [PubMed]
- Felip, E.; Ardizzoni, A.; Ciuleanu, T.; Cobo, M.; Laktionov, K.; Szilasi, M.; Califano, R.; Carcereny, E.; Griffiths, R.; Paz-Ares, L.; et al. CheckMate 171: A phase 2 trial of nivolumab in patients with previously treated advanced squamous non-small cell lung cancer, including ECOG PS 2 and elderly populations. Eur. J. Cancer 2020, 127, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Ready, N.E.; Audigier-Valette, C.; Goldman, J.W.; Felip, E.; Ciuleanu, T.E.; Rosario García Campelo, M.; Jao, K.; Barlesi, F.; Bordenave, S.; Rijavec, E.; et al. First-line nivolumab plus ipilimumab for metastatic non-small cell lung cancer, including patients with ECOG performance status 2 and other special populations: CheckMate 817. J. Immunother. Cancer 2023, 11, e006127. [Google Scholar] [CrossRef] [PubMed]
- Middleton, G.; Brock, K.; Savage, J.; Mant, R.; Summers, Y.; Connibear, J.; Shah, R.; Ottensmeier, C.; Shaw, P.; Lee, S.M.; et al. Pembrolizumab in patients with non-small-cell lung cancer of performance status 2 (PePS2): A single arm, phase 2 trial. Lancet Respir. Med. 2020, 8, 895–904. [Google Scholar] [CrossRef]
- Veluswamy, R.R.; Levy, B.; Wisnivesky, J.P. Chemotherapy in elderly patients with nonsmall cell lung cancer. Curr. Opin. Pulm. Med. 2016, 22, 336–343. [Google Scholar] [CrossRef]
- Piccirillo, J.F.; Tierney, R.M.; Costas, I.; Grove, L.; Spitznagel, E.L., Jr. Prognostic importance of comorbidity in a hospital-based cancer registry. JAMA 2004, 291, 2441–2447. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef] [PubMed]
- Aldea, M.; Orillard, E.; Mansi, L.; Marabelle, A.; Scotte, F.; Lambotte, O.; Michot, J.M. How to manage patients with corticosteroids in oncology in the era of immunotherapy? Eur. J. Cancer 2020, 141, 239–251. [Google Scholar] [CrossRef] [PubMed]
- Libert, C.; Dejager, L. How steroids steer T cells. Cell Rep. 2014, 7, 938–939. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.C.; Pennell, N.A. Early Use of Systemic Corticosteroids in Patients with Advanced NSCLC Treated with Nivolumab. J. Thorac. Oncol. 2018, 13, 1771–1775. [Google Scholar] [CrossRef] [PubMed]
- Arbour, K.C.; Mezquita, L.; Long, N.; Rizvi, H.; Auclin, E.; Ni, A.; Martínez-Bernal, G.; Ferrara, R.; Lai, W.V.; Hendriks, L.E.L.; et al. Impact of Baseline Steroids on Efficacy of Programmed Cell Death-1 and Programmed Death-Ligand 1 Blockade in Patients With Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 2872–2878. [Google Scholar] [CrossRef] [PubMed]
- Fucà, G.; Galli, G.; Poggi, M.; Lo Russo, G.; Proto, C.; Imbimbo, M.; Ferrara, R.; Zilembo, N.; Ganzinelli, M.; Sica, A.; et al. Modulation of peripheral blood immune cells by early use of steroids and its association with clinical outcomes in patients with metastatic non-small cell lung cancer treated with immune checkpoint inhibitors. ESMO Open 2019, 4, e000457. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Signorelli, D.; Ghidini, M.; Ghidini, A.; Pizzutilo, E.G.; Ruggieri, L.; Cabiddu, M.; Borgonovo, K.; Dognini, G.; Brighenti, M.; et al. Association of Steroids use with Survival in Patients Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Cancers 2020, 12, 546. [Google Scholar] [CrossRef] [PubMed]
- De Giglio, A.; Mezquita, L.; Auclin, E.; Blanc-Durand, F.; El-Amarti, L.; Caramella, C.; Bernal, G.M.; Hendriks, L.; Ferrara, R.; Naltet, C.; et al. 46O—Impact of early introduction of steroid on immune-checkpoint inhibitors (ICI) in patients with advanced non-small cell lung cancer treated. Ann. Oncol. 2019, 30, xi16. [Google Scholar] [CrossRef]
- Garant, A.; Guilbault, C.; Ekmekjian, T.; Greenwald, Z.; Murgoi, P.; Vuong, T. Concomitant use of corticosteroids and immune checkpoint inhibitors in patients with hematologic or solid neoplasms: A systematic review. Crit. Rev. Oncol. Hematol. 2017, 120, 86–92. [Google Scholar] [CrossRef]
- Kapoor, A.; Noronha, V.; Patil, V.M.; Joshi, A.; Menon, N.; Abraham, G.; Talreja, V.; D’Souza, H.; Prabhash, K. Concomitant use of corticosteroids and immune checkpoint inhibitors in patients with solid neoplasms: A real-world experience from a tertiary cancer center. Cancer Res. Stat. Treat. 2019, 2, 204–208. [Google Scholar]
- Buonacera, A.; Stancanelli, B.; Colaci, M.; Malatino, L. Neutrophil to Lymphocyte Ratio: An Emerging Marker of the Relationships between the Immune System and Diseases. Int. J. Mol. Sci. 2022, 23, 3636. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, W.; Yang, F.; Xu, Y.; Feng, C.; Zhao, Y. The regulatory roles of neutrophils in adaptive immunity. Cell Commun. Signal. 2019, 17, 147. [Google Scholar] [CrossRef] [PubMed]
- Fest, J.; Ruiter, T.R.; Groot Koerkamp, B.; Rizopoulos, D.; Ikram, M.A.; van Eijck, C.H.J.; Stricker, B.H. The neutrophil-to-lymphocyte ratio is associated with mortality in the general population: The Rotterdam Study. Eur. J. Epidemiol. 2019, 34, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Hibino, S.; Kawazoe, T.; Kasahara, H.; Itoh, S.; Ishimoto, T.; Sakata-Yanagimoto, M.; Taniguchi, K. Inflammation-Induced Tumorigenesis and Metastasis. Int. J. Mol. Sci. 2021, 22, 5421. [Google Scholar] [CrossRef] [PubMed]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef]
- Banna, G.L.; Di Quattro, R.; Malatino, L.; Fornarini, G.; Addeo, A.; Maruzzo, M.; Urzia, V.; Rundo, F.; Lipari, H.; De Giorgi, U.; et al. Neutrophil-to-lymphocyte ratio and lactate dehydrogenase as biomarkers for urothelial cancer treated with immunotherapy. Clin. Transl. Oncol. 2020, 22, 2130–2135. [Google Scholar] [CrossRef]
- Lianos, G.D.; Alexiou, G.A.; Exarchos, C.; Rausei, S.; Mitsis, M.; Voulgaris, S. Prognostic significance of neutrophil-to-lymphocyte ratio in several malignancies: Where do we stand? Biomark. Med. 2020, 14, 169–172. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Patients * (n = 122) n (%) | Cohort 1A (n = 18) n (%) | Cohort 1B (n = 33) n (%) | Cohort 2 (n = 71) n (%) | p |
|---|---|---|---|---|---|
| Age (years), median (range) | 62 (41–82) | 62.5 (48–75) | 62 (44–76) | 62 (41–82) | 0.91 |
| ≤65 | 83 (68) | 13 (72.2) | 22 (66.7) | 48 (67.6) | |
| >65 | 39 (32) | 5 (27.8) | 11 (33.3) | 23 (32.4) | |
| Gender | 0.94 | ||||
| Male | 90 (73.8) | 14 (77.8) | 23 (69.7) | 53 (74.6) | |
| Female | 32 (26.2) | 12 (22.2) | 10 (30.3) | 18 (25.4) | |
| ECOG PS | 0.7 | ||||
| 0 | 5 (4.1) | - | 2 (6.1) | 3 (4.2) | |
| 1 | 109 (89.3) | 18 (100) | 31 (93.9) | 60 (84.5) | |
| 2 | 8 (6.6) | - | - | 8 (11.3) | |
| BMI, median (range) | 24.9 (14.4–36.5) | 24.9 (18.1–34.5) | 24.2 (18.2–35.3) | 25.5 (14.3–36.4) | 0.97 |
| ≤18.5 | 6 (4.9) | 1 (5.6) | 1 (3) | 4 (5.6) | |
| 18.5–24.9 | 57 (46.7) | 9 (50) | 18 (54.5) | 30 (42.3) | |
| 25–29.9 | 35 (28.7) | 5 (27.8) | 7 (21.2) | 23 (32.4) | |
| ≥30 | 24 (19.7) | 3 (16.7) | 7 (21.2) | 14 (19.7) | |
| Smoking status | 0.97 | ||||
| Never smoker | 17 (13.9) | 3 (16.7) | 6 (18.2) | 8 (11.3) | |
| Active smoker | 27 (22.1) | 1 (5.6) | 5 (15.2) | 21 (29.6) | |
| Ex-smoker | 78 (64) | 14 (77.8) | 22 (66.7) | 42 (59.2) | |
| Histology | 0.72 | ||||
| Non-squamous adenocarcinoma | 82 (67.2) | 9 (50) | 23 (69.7) | 50 (70.4) | |
| Non-squamous other | 1 (0.8) | - | 1 (3) | - | |
| Non-squamous large cell | 3 (2.5) | - | 1 (3) | 2 (2.8) | |
| Squamous | 36 (29.5) | 9 (50) | 8 (24.2) | 19 (26.8) | |
| Stage (AJCC 8) | 0.29 | ||||
| IVA | 54 (44.3) | 11 (61.1) | 14 (42.4) | 29 (40.8) | |
| IVB | 68 (55.7) | 7 (38.9) | 19 (57.6) | 42 (59.2) | |
| Metastatic site | 0.81 | ||||
| Lung | 77 (63.1) | 10 (55.6) | 23 (69.7) | 44 (62) | |
| Pleural | 37 (30.3) | 8 (44.4) | 15 (45.5) | 14 (19.7) | |
| Bone | 32 (26.2) | 3 (16.7) | 10 (30.3) | 19 (26.8) | |
| CNS (pretreated, asymptomatic) | 27 (22.1) | 5 (27.8) | 7 (21.2) | 15 (21.1) | |
| Liver | 26 (21.3) | 3 (16.7) | 10 (30.3) | 13 (18.3) | |
| Adrenal | 24 (19.7) | 2 (11.1) | 8 (24.2) | 14 (19.7) | |
| Other | 24 (19.7) | 1 (5.6) | 5 (15.2) | 18 (25.4) | |
| Number of metastatic sites | 0.04 | ||||
| 1–2 | 87 (71.3) | 15 (83.3) | 18 (54.5) | 54 (76.1) | |
| ≥3 | 35 (28.7) | 3 (16.7) | 15 (45.5) | 17 (23.9) | |
| PD-L1 | <0.01 | ||||
| Not evaluated | 67 (54.9) | - | 30 (90.9) | 37 (52.1) | |
| <1% | 26 (21.3) | 6 (33.3) | - | 20 (28.2) | |
| ≥1% | 13 (10.7) | 12 (66.7) | - | 1 (1.4) | |
| ≥50% | 6 (4.9) | - | 1 (3) | 5 (7) | |
| 1–49% | 10 (8.2) | - | 2 (6.1) | 8 (11.3) | |
| Actionable mutations ** | |||||
| Yes | 8 (6.6) | ||||
| KRAS G12C | 3 (2.5) | ||||
| cMET amplification | 2 (1.6) | ||||
| RET | 1 (0.8) | ||||
| ALK (rebiopsy at progression) | 1 (0.8) | ||||
| EGFR (rebiopsy at progression) | 1 (0.8) | ||||
| No | 114 (93.4) | ||||
| Hemoglobin (g/dL), median (range) | 12.9 (8.4–16.1) | 12.8 (9.8–15.1) | 13.4 (8.5–16.1) | 12.9 (8.4–15.8) | 0.64 |
| ≤13 | 67 (54.9) | 11 (61.1) | 16 (48.5) | 40 (56.3) | |
| >13 | 55 (45.1) | 7 (38.9) | 17 (51.5) | 31 (43.7) | |
| Neutrophils (×103/µL), median (range) | 7.05 (1.9–67.1) | 6.6 (3.6–67.1) | 6.9 (2.1–26.4) | 7.2 (1.9–27.8) | 0.56 |
| 1.8–6.98 | 60 (49.2) | 10 (55.6) | 18 (54.5) | 32 (45.1) | |
| ≥6.99 | 62 (50.8) | 8 (44.4) | 15 (45.5) | 39 (54.9) | |
| Lymphocytes (×103/µL), median (range) | 1.6 (0.5–6.9) | 1.9 (0.9–3.0) | 1.7 (0.5–6.9) | 1.4 (0.5–4.4) | 0.03 |
| ≤1.5 | 53 (43.4) | 5 (27.8) | 10 (30.3) | 38 (53.5) | |
| >1.5 | 69 (56.6) | 13 (72.2) | 23 (69.7) | 33 (46.5) | |
| Neut./Lymph. ratio, median (range) | 4.3 (0.9–22.3) | 3.7 (1.5–22.2) | 4.0 (0.9–18.2) | 4.8 (1.3–18.2) | 0.32 |
| ≤3.81 | 48 (39.3) | 9 (50) | 15 (45.5) | 24 (33.8) | |
| >3.81 | 74 (60.7) | 9 (50) | 18 (54.5) | 47 (66.2) | |
| Platelets (×103/µL), median (range) | 316.5 (127–875) | 279 (158–586) | 326 (127–875) | 317 (147–722) | 0.96 |
| ≤450 | 102 (83.6) | 15 (83.3) | 28 (84.8) | 59 (83.1) | |
| >450 | 20 (16.4) | 3 (16.7) | 5 (15.2) | 12 (16.9) | |
| LDH (U/L), median (range) | 231 (130–1523) | 209 (140–1523) | 231 (130–1523) | 225 (130–799) | 0.1 |
| ≤225 | 42 (34.4) | 11(61.1) | 11(33.3) | 20(28.2) | |
| >225 | 46 (37.7) | 7(38.9) | 22(66.7) | 17(23.9) | |
| Not determined | 34 (27.9) | - | - | 34(47.9) | |
| Corticoids in the first month | 0.54 | ||||
| Yes | 31 (25.4) | 7 (38.9) | 7 (21.2) | 17 (23.9) | |
| No | 91 (74.6) | 11 (61.1) | 26 (78.8) | 54 (76.1) | |
| Previous palliative radiotherapy | 0.94 | ||||
| Yes | 33 (27) | 5 (27.8) | 10 (30.3) | 18 (25.4) | |
| No | 89 (73) | 13 (72.2) | 23 (69.7) | 53 (74.6) | |
| Treatment group | |||||
| Cohort 1A (CheckMate-227 protocol) | 18 (14.8) | ||||
| Cohort 1B (CheckMate-9LA protocol) | 33 (27) | ||||
| Non-squamous | 25 (20.5) | ||||
| Squamous | 8 (6.5) | ||||
| Cohort 2 | 71 (58.2) | ||||
| Non-squamous, KeyNote-189 protocol | 52 (42.6) | ||||
| Squamous, KeyNote-407 protocol | 19 (15.6) |
| Treatment Protocol | n | Median Follow-Up, Range (Months) |
|---|---|---|
| Cohort 1A (CM-227) (Jan 2016–Dec 2017) | 18 | 83 (77.8–84.4) |
| Cohort 1B (CM-9LA) (Jan 2018–Jul 2019) | 33 | 59 (49.1–63.1) |
| Cohort 2 (KN-189 and KN-407) Aug 2019–Jun 2023 | 71 | 14.2 (2.9–48.3) |
| Total | 122 | 20 (2.9–84.4) |
| Progression-Free Survival | Overall Survival | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Category | Prognostic Factor | n | Median Survival (Mo.) | 2-Year Survival Rate (%) | 95% CI (%) | Univariate Analysis, p | Multivariate Analysis | Median Survival (Mo.) | 2-year Survival Rate (%) | 95% CI (%) | Univariate Analysis, p | Multivariate Analysis | ||
| HR (95%CI) | p | HR (95%CI) | p | |||||||||||
| Cohort | 1A (CheckMate 227) | 18 | 10.1 | 32 | 15.4–55.8 | 0.71 | 24.2 | 55% | 33–75.1 | 0.25 | ||||
| 1B (CheckMate 9LA) | 33 | 8.4 | 34 | 20.5–51.8 | 13.7 | 34% | 20.4–51.7 | |||||||
| 2 (KeyNote 189/407) | 71 | 12.7 | 35 | 23.4–48.1 | 24.2 | 53% | 39.3–66.9 | |||||||
| Treatment group | Nivolumab + Ipilimumab | 51 | 8.6 | 34 | 22.3–47.8 | 0.41 | 14 | 42% | 29.2–55.6 | 0.18 | ||||
| Pembrolizumab | 71 | 12.7 | 35 | 23.4–48.1 | >24 | 53% | 39.3–66.9 | |||||||
| 1st line objective response | PD | 12 | 1 | 0 | 0–0 | <0.01 | 2.4 | 0% | 0–0 | <0.01 | ||||
| CR + PR | 51 | >24 | 64 | 49.6–77.0 | >24 | 77% | 62.5–87.1 | |||||||
| SD | 59 | 8 | 16 | 8–28.8 | 13.9 | 31% | 18.9–46.3 | |||||||
| Age | ≤60 | 48 | 16.6 | 42 | 28.9–57.3 | 0.12 | >24 | 60% | 45–74 | 0.04 | 1.03 (1.00–1.07) | 0.02 | ||
| >60 | 74 | 9.9 | 30 | 20–42.2 | 14.9 | 41% | 29.2–53.7 | |||||||
| Gender | Female | 32 | 16.6 | 47 | 30.6–64.7 | 0.29 | >24 | 67% | 49.1–81 | 0.29 | ||||
| Male | 90 | 10.7 | 31 | 21.4–41.7 | 20.3 | 43% | 31.9–54.2 | |||||||
| ECOG PS | 2 | 8 | 3.5 | 0 | 0–0 | <0.01 | 2.04 (1.09–3.81) | 0.02 | 8.2 | 0% | 0–0 | <0.01 | 2.17 (1.08–4.36) | 0.02 |
| 0–1 | 114 | 12.6 | 38 | 28.9–47.7 | >24 | 52% | 28.8–47.6 | |||||||
| BMI | <18.5 | 6 | 5.1 | 17 | 3–56.4 | 0.14 | 7.4 | 21% | 3.8–63.6 | 0.05 | 1.00 (0.95–1.06) | 0.75 | ||
| 18.5–24.9 | 57 | 11.5 | 31 | 19.9–45.3 | 21.2 | 49% | 33.3–61.2 | |||||||
| 25.0–29.9 | 35 | 12 | 37 | 22.4–54.3 | 21.9 | 49% | 32–66.2 | |||||||
| 30+ | 24 | 14.8 | 48 | 28.8–67.4 | >24 | 60% | 39.1–77.3 | |||||||
| Smoking status | Former smoker | 78 | 10.5 | 32 | 22.4–44.4 | 0.13 | 21.5 | 48% | 36.1–60.1 | 0.23 | ||||
| Active smoker | 27 | 21.7 | 49 | 30.7–67.3 | >24 | 61% | 40–77.8 | |||||||
| Never smoker | 17 | 8.4 | 26 | 10.1–51.6 | 13.6 | 34% | 14.5–61.5 | |||||||
| Histology | Non-squamous | 86 | 12.5 | 40 | 30.1–51.7 | 0.34 | >24 | 55% | 44.1–66.2 | 0.45 | ||||
| Squamous | 36 | 9.9 | 22 | 11–39.6 | 17.4 | 33% | 18.5–52.1 | |||||||
| AJCC stage | IVA | 54 | 8.4 | 48 | 34.4–62.4 | <0.01 | 1.35 (0.77–2.38) | 0.28 | >24 | 57% | 42.4–70.5 | 0.04 | 1.43 (0.74–2.76) | 0.28 |
| IVB | 68 | 25.5 | 25 | 15.7–37 | 13.8 | 42% | 29.9–55.4 | |||||||
| Steroid use in the first month | No | 91 | 13.3 | 39 | 28.4–49.8 | 0.02 | 1.44 (0.87–2.39) | 0.15 | 10.5 | 38% | 22.6–56.4 | 0.02 | 1.79 (1.01–3.16) | 0.04 |
| Yes | 31 | 4.1 | 24 | 12.1–41.5 | >24 | 52% | 40.4–63.3 | |||||||
| Palliative radiotherapy | No | 89 | 14.8 | 41 | 30.8–52.2 | 0.02 | 24.1 | 52% | 40.2–62.6 | 0.14 | ||||
| Yes | 33 | 8 | 18 | 8.1–35.5 | 13.9 | 41% | 24.4–59.8 | |||||||
| Number of metastatic sites | 0–2 | 87 | 17 | 42 | 31.6–54 | <0.01 | >24 | 59% | 46.9–69.5 | <0.01 | ||||
| 3+ | 35 | 7.2 | 17 | 8.1–32.7 | 12.1 | 26% | 13.3–43.6 | |||||||
| Bone metastases | No | 90 | 14.7 | 42 | 31.6–53.1 | <0.01 | 1.67 (0.99–2.81) | 0.05 | >24 | 55% | 43–65.6 | <0.01 | 1.64 (0.91–2.95) | 0.09 |
| Yes | 32 | 6.7 | 15 | 6.1–33.7 | 11.4 | 32% | 17.6–51.3 | |||||||
| Liver metastases | No | 96 | 13.3 | 38 | 28.6–49 | 0.03 | 1.25 (0.70–2.25) | 0.44 | 12.2 | 33% | 16.8–54.2 | 0.05 | 1.23 (0.63–2.4) | 0.53 |
| Yes | 26 | 7.2 | 23 | 10.6–42.9 | 24.2 | 53% | 41.6–63.3 | |||||||
| CNS metastasis | No | 95 | 12.2 | 36 | 26.7–47.2 | 0.42 | >24 | 52% | 32.9–70.2 | 0.73 | ||||
| Yes | 27 | 10.5 | 30 | 15.6–49.5 | 21.2 | 48% | 36.8–58.9 | |||||||
| Adrenal metastasis | No | 98 | 12.7 | 36 | 26.3–46.3 | 0.35 | 24.2 | 51% | 40.4–61.9 | 0.2 | ||||
| Yes | 24 | 7.4 | 32 | 16–52.8 | 13 | 38% | 20.5–59.7 | |||||||
| Pleural metastasis | No | 85 | 11 | 37 | 26.5–48 | 0.87 | 24.1 | 52% | 39.7–63.4 | 0.6 | ||||
| Yes | 37 | 12.5 | 33 | 20.1–50 | 18.4 | 43% | 28.3–59.8 | |||||||
| Lung metastasis | No | 45 | 5.2 | 25 | 14.1–40.4 | 0.08 | 13.3 | 43% | 28.5–58.7 | 0.08 | ||||
| Yes | 77 | 12.6 | 41 | 29.8–52.7 | 24.1 | 52% | 39.5–63.9 | |||||||
| Other metastasis | No | 98 | 12.5 | 39 | 29.2–49.5 | 0.17 | 14.5 | 30% | 12–56.8 | 0.95 | ||||
| Yes | 24 | 8.7 | 18 | 6.9–40.3 | 24.2 | 52% | 41.2–62.1 | |||||||
| Hemoglobin (g/dL) | ≤13 | 67 | 8.7 | 25 | 15.5–37.8 | 0.04 | 0.64 (0.40–1.05) | 0.08 | 14 | 41% | 28.9–53.7 | 0.03 | 0.70 (0.41–1.19) | 0.19 |
| >13 | 55 | 17 | 47 | 33.6–60.6 | >24 | 59% | 43.8–72.2 | |||||||
| LDH (U/L) | ≤225 | 42 | 8.7 | 36 | 22.6–52.6 | 0.24 | >24 | 50% | 34.5–65.9 | 0.29 | ||||
| >225 | 46 | 8.4 | 26 | 15.2–40.6 | 13.9 | 36% | 22.6–52.4 | |||||||
| Platelets (×1000/µL) | ≤450 | 102 | 11.3 | 33 | 23.8–43.1 | 0.22 | 21.9 | 48% | 37.1–58.6 | 0.92 | ||||
| >450 | 20 | 19.4 | 46 | 26.1–68.1 | >24 | 52% | 30.5–72.3 | |||||||
| Neutrophils (×1000/µL) | 1.8–6.98 | 60 | 10.9 | 39 | 26.5–52.1 | 0.6 | >24 | 55% | 40.7–68.1 | 0.08 | ||||
| 6.99+ | 62 | 12 | 32 | 21.1–45.2 | 20.3 | 43% | 30.5–56.6 | |||||||
| Lymphocytes (×1000/µL) | ≤1.5 | 53 | 10.4 | 41 | 15.4–40.7 | 0.33 | 14.9 | 40% | 26.8–55.6 | 0.25 | ||||
| >1.5 | 69 | 12.6 | 26 | 29.9–53.8 | >24 | 55% | 42.4–67.1 | |||||||
| Neutrophil-to-lymphocyte ratio | ≤3.81 | 48 | 16.6 | 45 | 31.1–59.5 | 0.05 | 1.23 (0.76–1.99) | 0.39 | >24 | 63% | 47.1–75.8 | <0.01 | 1.81 (1.04–3.15) | 0.03 |
| 3.81+ | 74 | 10.2 | 29 | 18.8–40.7 | 14.9 | 39% | 27.6–52.1 | |||||||
| PDL1 status | Undetermined | 67 | 9.9 | 29 | 19.3–42.1 | 0.23 | 18 | 40% | 27.6–53.8 | 0.36 | ||||
| Negative | 26 | 12.2 | 48 | 30.2–67.2 | >24 | 62% | 41.4–78.7 | |||||||
| Positive | 29 | 16.6 | 36 | 19.9–56.1 | >24 | 55% | 36.3–72.5 | |||||||
| Actionable mutations | Yes | 8 | 11.5 | 12 | 2.2–47.1 | 0.26 | 17.4 | 50% | 21.5–78.4 | 0.44 | ||||
| No | 114 | 11 | 37 | 28.4–47 | 21.9 | 48% | 38.1–58.4 | |||||||
| Objective Response | Clinical Benefit | ||||||
|---|---|---|---|---|---|---|---|
| Category | Prognostic Factor | PD n (%) | SD n (%) | CR + PR n (%) | p | CR + PR + SD n (%) | p |
| Age | ≤65 | 7 (8.4%) | 37 (44.6%) | 39 (47%) | 0.36 | 76 (91.6%) | 0.67 |
| >65 | 5 (12.8%) | 22 (56.4%) | 12 (30.8%) | 34 (87.2%) | |||
| ≤61 * | 2 (3.7%) | 25 (46.3%) | 27 (50%) | 0.07 | 52 (96.3%) | 0.04 | |
| >61 | 10 (14.7%) | 34 (50%) | 24 (35.3%) | 58 (85.3%) | |||
| Gender | Female | 3 (9.4%) | 12 (37.5%) | 17 (53.1%) | 0.4 | 29 (90.6%) | 0.81 |
| Male | 9 (10%) | 47 (52.2%) | 34 (37.8%) | 81 (90%) | |||
| ECOG PS | 0 | 3 (60%) | 2 (40%) | 0.03 | 5 (100%) | <0.01 | |
| 1 | 8 (7.3%) | 53 (48.6%) | 48 (44%) | 101 (92.7%) | |||
| 2 | 4 (50%) | 3 (37.5%) | 1 (12.5%) | 4 (50%) | |||
| BMI | <18.5 | 2 (33.3%) | 4 (66.7%) | 0.72 | 4 (66.7%) | 0.61 | |
| 18.5–24.9 | 4 (7%) | 25 (43.9%) | 28 (49.1%) | 53 (93%) | |||
| 25.0–29.9 | 4 (11.4%) | 19 (54.3%) | 12 (34.3%) | 31 (88.6%) | |||
| ≥30 | 2 (8.3%) | 11 (45.8%) | 11 (45.8%) | 22 (91.7%) | |||
| Histology | Non-squamous | 6 (7%) | 41 (47.7%) | 39 (45.3%) | 0.34 | 80 (93%) | 0.19 |
| Squamous | 6 (16.7%) | 18 (50%) | 12 (33.3%) | 30 (83.3%) | |||
| AJCC stage | IVA | 5 (9.3%) | 21 (38.9%) | 28 (51.9%) | 0.12 | 49 (90.7%) | 0.85 |
| IVB | 7 (10.3%) | 38 (55.9%) | 23 (33.8%) | 61 (89.7%) | |||
| Metastasis site | |||||||
| Lung | Yes | 4 (5.2%) | 38 (49.4%) | 35 (45.5%) | 0.15 | 73 (94.8%) | 0.05 |
| No | 8 (17.8%) | 21 (46.7%) | 16 (35.6%) | 37 (82.2%) | |||
| Pleural | Yes | 6 (16.2%) | 16 (43.2%) | 15 (40.5%) | 0.47 | 31 (83.8%) | 0.22 |
| No | 6 (7.1%) | 43 (50.6%) | 36 (42.4%) | 79 (92.9%) | |||
| Bone | Yes | 4 (12.5%) | 19 (59.4%) | 9 (28.1%) | 0.3 | 28 (87.5%) | 0.81 |
| No | 8 (8.9%) | 40 (44.4%) | 42 (46.7%) | 82 (91.1%) | |||
| CNS | Yes | 2 (7.4%) | 16 (59.3%) | 9 (33.3%) | 0.62 | 25 (92.6%) | 0.91 |
| No | 10 (10.5%) | 43 (45.3%) | 42 (44.2%) | 85 (89.5%) | |||
| Liver | Yes | 4 (15.4%) | 15 (57.7%) | 7 (26.9%) | 0.34 | 22 (84.6%) | 0.48 |
| No | 8 (8.3%) | 44 (45.8%) | 44 (45.8%) | 88 (91.7%) | |||
| Adrenal | Yes | 2 (8.3%) | 12 (50%) | 10 (41.7%) | 0.98 | 22 (91.7%) | 0.92 |
| No | 10 (10.2%) | 47 (48%) | 41 (41.8%) | 88 (89.8%) | |||
| Other | Yes | 1 (4.2%) | 13 (54.2%) | 10 (41.7%) | 0.78 | 23 (95.8%) | 0.51 |
| No | 11 (11.2%) | 46 (46.9%) | 41 (41.8%) | 87 (88.8%) | |||
| Number of metastatic sites | 0–2 | 9 (10.3%) | 36 (41.4%) | 42 (48.3%) | 0.08 | 78 (89.7%) | 0.97 |
| ≥3 | 3 (8.6%) | 23 (65.7%) | 9 (25.7%) | 32 (91.4%) | |||
| PDL1 status | Undetermined | 5 (7.5%) | 39 (58.2%) | 23 (34.3%) | 0.26 | 62 (92.5%) | 0.14 |
| Negative (<1%) | 1 (3.8%) | 12 (46.2%) | 13 (50%) | 25 (96.2%) | |||
| Positive (≥1%) | 6 (20.7%) | 8 (27.6%) | 15 (51.7%) | 23 (79.3%) | |||
| Hemoglobin (g/dL) | ≤13 | 10 (14.9%) | 32 (47.8%) | 25 (37.3%) | 0.1 | 57 (85.1%) | 0.04 |
| >13 | 2 (3.6%) | 27 (49.1%) | 26 (47.3%) | 53 (96.4%) | |||
| Neutrophils (×1000/µL) | 1.8–6.98 | 5 (8.3%) | 31 (51.7%) | 24 (40%) | 0.11 | 55 (91.7%) | 0.58 |
| 6.99+ | 7 (11.3%) | 28 (45.2%) | 27 (43.5%) | 55 (88.7%) | |||
| Lymphocytes (×1000/µL) | ≤1.5 | 7 (13.2%) | 30 (56.6%) | 16 (30.2%) | 0.07 | 46 (86.8%) | 0.27 |
| >1.5 | 5 (7.2%) | 29 (42%) | 35 (50.7%) | 64 (92.8%) | |||
| Neutrophil-to-lymphocyte ratio | ≤3.81 | 1 (2.1%) | 27 (56.2%) | 20 (41.7%) | 0.11 | 47 (97.9%) | 0.04 |
| 3.81+ | 11 (14.9%) | 32 (43.2%) | 31 (41.9%) | 63 (85.1%) | |||
| Platelets (×1000/µL) | ≤450 | 9 (8.8%) | 51 (50%) | 42 (41.2%) | 0.84 | 93 (91.2%) | 0.66 |
| >450 | 3 (15%) | 8 (40%) | 9 (45%) | 17 (85%) | |||
| LDH (U/L) | ≤225 | 3 (7.1%) | 25 (59.5%) | 14 (33.3%) | 0.71 | 39 (92.9%) | 0.39 |
| >225 | 7 (15.2%) | 25 (54.3%) | 14 (30.4%) | 39 (84.8%) | |||
| Undetermined | 2 (5.9%) | 9 (26.5%) | 23 (67.6%) | 32 (94.1%) | |||
| Steroid use in the first month | Yes | 7 (22.6%) | 16 (51.6%) | 8 (25.8%) | 0.03 | 24 (77.4%) | 0.02 |
| No | 5 (5.5%) | 43 (47.3%) | 43 (47.3%) | 86 (94.5%) | |||
| Treatment group | Nivolumab + Ipilimumab | 7 (13.7%) | 27 (52.9%) | 17 (33.3%) | 0.2 | 44 (86.3%) | 0.22 |
| Pembrolizumab | 5 (7%) | 32 (45.1%) | 34 (47.9%) | 66 (93%) | |||
| Cohort | 1A CheckMate-227 | 4 (22.2%) | 7 (38.9%) | 7 (38.9%) | 0.59 | 14 (77.8%) | 0.53 |
| 1B (non-Sq) CheckMate-9LA | 1 (4%) | 15 (60%) | 9 (36%) | 24 (96%) | |||
| 1B (Sq) CheckMate-9LA | 2 (25%) | 5 (62.5%) | 1 (12.5%) | 6 (75%) | |||
| 2 (non-Sq) KeyNote-189 | 4 (7.7%) | 21 (40.4%) | 27 (51.9%) | 48 (92.3%) | |||
| 2 (Sq) KeyNote-407 | 1 (5.3%) | 11 (57.9%) | 7 (36.8%) | 18 (94.7%) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Preda, A.-C.; Ciuleanu, T.-E.; Todor, N.; Vlad, C.; Iancu, D.I.; Mocan, C.; Bandi-Vasilica, M.; Albu, F.; Todor-Bondei, I.M.; Hapca, M.C.; et al. Use of Different Anti-PD-1 Checkpoint Combination Strategies for First-Line Advanced NSCLC Treatment—The Experience of Ion Chiricuță Oncology Institute. Cancers 2024, 16, 2022. https://doi.org/10.3390/cancers16112022
Preda A-C, Ciuleanu T-E, Todor N, Vlad C, Iancu DI, Mocan C, Bandi-Vasilica M, Albu F, Todor-Bondei IM, Hapca MC, et al. Use of Different Anti-PD-1 Checkpoint Combination Strategies for First-Line Advanced NSCLC Treatment—The Experience of Ion Chiricuță Oncology Institute. Cancers. 2024; 16(11):2022. https://doi.org/10.3390/cancers16112022
Chicago/Turabian StylePreda, Alexandra-Cristina, Tudor-Eliade Ciuleanu, Nicolae Todor, Cătălin Vlad, Dana Ioana Iancu, Cristina Mocan, Mariana Bandi-Vasilica, Florina Albu, Irina Mihaela Todor-Bondei, Mădălina Claudia Hapca, and et al. 2024. "Use of Different Anti-PD-1 Checkpoint Combination Strategies for First-Line Advanced NSCLC Treatment—The Experience of Ion Chiricuță Oncology Institute" Cancers 16, no. 11: 2022. https://doi.org/10.3390/cancers16112022
APA StylePreda, A.-C., Ciuleanu, T.-E., Todor, N., Vlad, C., Iancu, D. I., Mocan, C., Bandi-Vasilica, M., Albu, F., Todor-Bondei, I. M., Hapca, M. C., Kubelac, M.-P., & Kubelac-Varro, A. D. (2024). Use of Different Anti-PD-1 Checkpoint Combination Strategies for First-Line Advanced NSCLC Treatment—The Experience of Ion Chiricuță Oncology Institute. Cancers, 16(11), 2022. https://doi.org/10.3390/cancers16112022