
CASCADE: Context-Aware Data-Driven AI for Streamlined Multidisciplinary Tumor Board Recommendations in Oncology


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Tumor Board Composition
2.3. Machine Learning Algorithm
3. Results
3.1. Patient Population
3.2. Tumor Board Recommendations
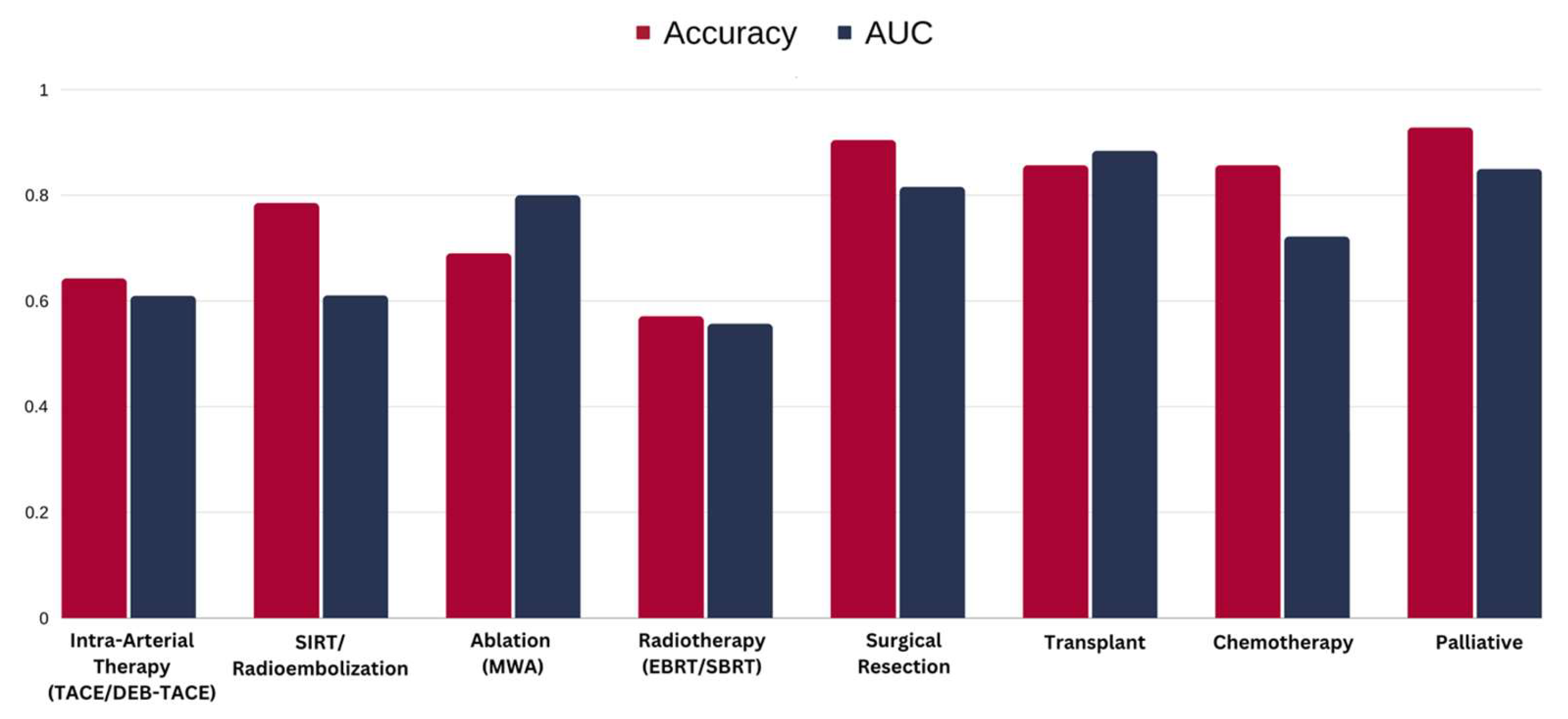
3.3. Model Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dixon, E.; Abdalla, E.; Schwarz, R.E.; Vauthey, J.-N. AHPBA/SSO/SSAT Sponsored Consensus Conference on Multidisciplinary Treatment of Hepatocellular Carcinoma. HPB 2010, 12, 287–288. [Google Scholar] [CrossRef] [PubMed]
- Gøtzsche, P.C. Rational Diagnosis and Treatment: Evidence-Based Clinical Decision-Making; Wulff, H.R., Ed.; John Wiley & Sons: Chichester, UK, 2007. [Google Scholar]
- Vauthey, J.-N.; Brouquet, A. (Eds.) Recent results in cancer research. Fortschritte der Krebsforschung. Progres dans les recherches sur le cancer. In Multidisciplinary Treatment of Hepatocellular Carcinoma; Springer: Berlin/Heidelberg, Germany, 2013; ISBN 9783642160363. [Google Scholar]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD Guidelines for the Treatment of Hepatocellular Carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef]
- Management of Hepatocellular Carcinoma. Available online: https://www.aasld.org/practice-guidelines/management-hepatocellular-carcinoma (accessed on 14 May 2024).
- Ryder, S.D. British Society of Gastroenterology. Guidelines for the Diagnosis and Treatment of Hepatocellular Carcinoma (HCC) in Adults. Gut 2003, 52 (Suppl. 3), iii1–iii8. [Google Scholar]
- Kaneko, J.; Kokudo, T.; Inagaki, Y.; Hasegawa, K. Innovative Treatment for Hepatocellular Carcinoma (HCC). Transl. Gastroenterol. Hepatol. 2018, 3, 78. [Google Scholar] [CrossRef] [PubMed]
- Hahlweg, P.; Didi, S.; Kriston, L.; Haaaaaeanrter, M.; Nestoriuc, Y.; Scholl, I. Process Quality of Decision-Making in Multidisciplinary Cancer Team Meetings: A Structured Observati. BMC Cancer 2017, 17, 772. [Google Scholar] [CrossRef]
- Wright, F.C.; De Vito, C.; Langer, B.; Hunter, A. Multidisciplinary Cancer Conferences: A Systematic Review and Development of Practice Standards. Eur. J. Cancer 2007, 43, 1002–1010. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.; Munro, A.J.; Glynne-Jones, R.; Griffith, C.; Trevatt, P.; Richards, M.; Ramirez, A.J. Multidisciplinary Team Working in Cancer: What Is the Evidence? BMJ 2010, 340, c951. [Google Scholar] [CrossRef] [PubMed]
- Patkar, V.; Acosta, D.; Davidson, T.; Jones, A.; Fox, J.; Keshtgar, M. Cancer Multidisciplinary Team Meetings: Evidence, Challenges, and the Role of Clinical Decision Support Technology. Int. J. Breast Cancer 2011, 2011, 831605. [Google Scholar] [CrossRef] [PubMed]
- Maness, D.L.; Riley, E.; Studebaker, G. Hepatitis C: Diagnosis and Management. Am. Fam. Phys. 2021, 104, 626–635. [Google Scholar]
- Awaysheh, A.; Wilcke, J.; Elvinger, F.; Rees, L.; Fan, W.; Zimmerman, K.L. Review of Medical Decision Support and Machine-Learning Methods. Vet. Pathol. 2019, 56, 512–525. [Google Scholar] [CrossRef]
- Ross, E.G.; Shah, N.H.; Dalman, R.L.; Nead, K.T.; Cooke, J.P.; Leeper, N.J. The Use of Machine Learning for the Identification of Peripheral Artery Disease and Future Mortality Risk. J. Vasc. Surg. 2016, 64, 1515–1522.e3. [Google Scholar] [CrossRef]
- Sinha, I.; Aluthge, D.P.; Chen, E.S.; Sarkar, I.N.; Ahn, S.H. Machine Learning Offers Exciting Potential for Predicting Postprocedural Outcomes: A Framework for Developing Random Forest Models in IR. J. Vasc. Interv. Radiol. 2020, 31, 1018–1024.e4. [Google Scholar] [CrossRef]
- Lin, F.P.Y.; Pokorny, A.; Teng, C.; Dear, R.; Epstein, R.J. Computational Prediction of Multidisciplinary Team Decision-Making for Adjuvant Breast Cancer Drug Therapies: A Machine Learning Approach. BMC Cancer 2016, 16, 929. [Google Scholar] [CrossRef] [PubMed]
- Hanley, J.A.; McNeil, B.J. The Meaning and Use of the Area under a Receiver Operating Characteristic (ROC) Curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef]
- Tripathi, S.; Musiolik, T.H. Fairness and Ethics in Artificial Intelligence-Based Medical Imaging. In Research Anthology on Improving Medical Imaging Techniques for Analysis and Intervention; IGI Global: Hershey, PA, USA, 2023; pp. 79–90. [Google Scholar]
- Valentin, L.; McCarthy, C.; Do, S.; Flores, E.; Uppot, R. Predicting Multidisciplinary Tumor Board Recommendations: Initial Experience with Machine Learning in Interventional Oncology. J. Vasc. Interv. Radiol. 2017, 28, S19–S20. [Google Scholar] [CrossRef]
- Wani, M.A. Place of Publication Not Identified. In Machine Learning and Applications. Proceedings: International Conference on Machine Learning and Applications; IEEE Computer Society Press: Cincinnati, OH, USA, 2007; Volume 6. [Google Scholar]
- Syrowatka, A.; Krömker, D.; Meguerditchian, A.N.; Tamblyn, R. Features of Computer-Based Decision Aids: Systematic Review, Thematic Synthesis, and Meta-Analyses. J. Med. Internet Res. 2016, 18, e20. [Google Scholar] [CrossRef] [PubMed]
- Tătaru, O.S.; Vartolomei, M.D.; Rassweiler, J.J.; Virgil, O.; Lucarelli, G.; Porpiglia, F.; Amparore, D.; Manfredi, M.; Carrieri, G.; Falagario, U.; et al. Artificial Intelligence and Machine Learning in Prostate Cancer Patient Management—Current Trends and Future Perspectives. Diagnostics 2021, 11, 354. [Google Scholar] [CrossRef]
- Horn, W.; Shahar, Y.; Lindberg, G.; Andreassen, S.; Wyatt, J. Artificial Intelligence in Medicine. In Proceedings of the Joint European Conference on Artificial Intelligence in Medicine and Medical Decision Making, AIMDM’99, Aalborg, Denmark, 20–24 June 1999. [Google Scholar]
- Tripathi, S.; Tabari, A.; Mansur, A.; Dabbara, H.; Bridge, C.P.; Daye, D. From Machine Learning to Patient Outcomes: A Comprehensive Review of AI in Pancreatic Cancer. Diagnostics 2024, 14, 174. [Google Scholar] [CrossRef]
- Zuo, D.; Yang, L.; Jin, Y.; Qi, H.; Liu, Y.; Ren, L. Machine Learning-Based Models for the Prediction of Breast Cancer Recurrence Risk. BMC Med. Inform. Decis. Mak. 2023, 23, 276. [Google Scholar] [CrossRef] [PubMed]
- Ghavidel, A.; Pazos, P. Machine Learning (ML) Techniques to Predict Breast Cancer in Imbalanced Datasets: A Systematic Review. J. Cancer Surviv. 2023, 1–25. [Google Scholar] [CrossRef]
- Sweetlin, E.J.; Saudia, S. A Review of Machine Learning Algorithms on Different Breast Cancer Datasets. In Lecture Notes in Electrical Engineering; Lecture notes in electrical engineering; Springer Nature: Singapore, 2024; pp. 659–673. ISBN 9789819934805. [Google Scholar]
- Islam, M.M.; Poly, T.N. Machine Learning Models of Breast Cancer Risk Prediction. bioRxiv 2019. bioRxiv:723304. [Google Scholar]
- Nazari, E.; Naderi, H.; Tabadkani, M.; ArefNezhad, R.; Farzin, A.H.; Dashtiahangar, M.; Khazaei, M.; Ferns, G.A.; Mehrabian, A.; Tabesh, H.; et al. Breast Cancer Prediction Using Different Machine Learning Methods Applying Multi Factors. J. Cancer Res. Clin. Oncol. 2023, 149, 17133–17146. [Google Scholar] [CrossRef]
- Li, Y.; Wu, X.; Yang, P.; Jiang, G.; Luo, Y. Machine Learning Applications in Lung Cancer Diagnosis, Treatment and Prognosis. arXiv 2022, arXiv:2203.02794. [Google Scholar]
- Tripathi, S.; Moyer, E.J.; Augustin, A.I.; Zavalny, A.; Dheer, S.; Sukumaran, R.; Schwartz, D.; Gorski, B.; Dako, F.; Kim, E. RadGenNets: Deep Learning-Based Radiogenomics Model for Gene Mutation Prediction in Lung Cancer. Inform. Med. Unlocked 2022, 33, 101062. [Google Scholar] [CrossRef]
- Wei, F.; Azuma, K.; Nakahara, Y.; Saito, H.; Matsuo, N.; Tagami, T.; Kouro, T.; Igarashi, Y.; Tokito, T.; Kato, T.; et al. Machine Learning for Prediction of Immunotherapeutic Outcome in Non-Small-Cell Lung Cancer Based on Circulating Cytokine Signatures. J. Immunother. Cancer 2023, 11, e006788. [Google Scholar] [CrossRef] [PubMed]
- Benzekry, S.; Grangeon, M.; Karlsen, M.; Alexa, M.; Bicalho-Frazeto, I.; Chaleat, S.; Tomasini, P.; Barbolosi, D.; Barlesi, F.; Greillier, L. Machine Learning for Prediction of Immunotherapy Efficacy in Non-Small Cell Lung Cancer from Simple Clinical and Biological Data. Cancers 2021, 13, 6210. [Google Scholar] [CrossRef] [PubMed]
- Sharma, L.; Choi, S.; Balaji, V.; Joshi, A.; Mporas, I.; Shi, J.; Zhao, Y.; Tailor, V.; Shah, R.N.H.; Waters, J.S.; et al. Novel Machine Learning Algorithm to Predict Response to Immunotherapy in Patients with Small Cell and Non-Small Cell Lung Cancer. J. Clin. Oncol. 2023, 41, e13556. [Google Scholar] [CrossRef]
- Gao, Q.; Yang, L.; Lu, M.; Jin, R.; Ye, H.; Ma, T. The Artificial Intelligence and Machine Learning in Lung Cancer Immunotherapy. J. Hematol. Oncol. 2023, 16, 55. [Google Scholar] [CrossRef] [PubMed]
- Abdul Rahman, H.; Ottom, M.A.; Dinov, I.D. Machine Learning-Based Colorectal Cancer Prediction Using Global Dietary Data. BMC Cancer 2023, 23, 144. [Google Scholar] [CrossRef]
- Talebi, R.; Celis-Morales, C.A.; Akbari, A.; Talebi, A.; Borumandnia, N.; Pourhoseingholi, M.A. Machine Learning-Based Classifiers to Predict Metastasis in Colorectal Cancer Patients. Front. Artif. Intell. 2024, 7, 1285037. [Google Scholar] [CrossRef]
- Kokkinakis, S.; Ziogas, I.A.; Llaque Salazar, J.D.; Moris, D.P.; Tsoulfas, G. Clinical Prediction Models for Prognosis of Colorectal Liver Metastases: A Comprehensive Review of Regression-Based and Machine Learning Models. Cancers 2024, 16, 1645. [Google Scholar] [CrossRef]
- Alboaneen, D.; Alqarni, R.; Alqahtani, S.; Alrashidi, M.; Alhuda, R.; Alyahyan, E.; Alshammari, T. Predicting Colorectal Cancer Using Machine and Deep Learning Algorithms: Challenges and Opportunities. Big Data Cogn. Comput. 2023, 7, 74. [Google Scholar] [CrossRef]
- Cleophas, T.J. Machine Learning in Medicine—A Complete Overview, 1st ed.; Zwinderman, A.H., Ed.; Springer: Berlin, Germany, 2015. [Google Scholar]
- Cook, J.A.; Ranstam, J. Overfitting. Br. J. Surg. 2016, 103, 1814. [Google Scholar] [CrossRef] [PubMed]
- Kakarmath, S.; Golas, S.; Felsted, J.; Kvedar, J.; Jethwani, K.; Agboola, S. Validating a Machine Learning Algorithm to Predict 30-Day Re-Admissions in Patients with Heart Failure: Protocol for a Prospective Cohort Study. JMIR Res. Protoc. 2018, 7, e176. [Google Scholar] [CrossRef] [PubMed]
- Qudrat-Ullah, H.; Spector, J.M.; Davidsen, P.I. Complex Decision Making: Theory and Practice; Springer: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Ayre, L.; Craner, J. Algorithms: Avoiding the Implementation of Institutional Biases. Publ. Libr. Q. 2018, 37, 341–347. [Google Scholar] [CrossRef]
- Tripathi, S.; Gabriel, K.; Dheer, S.; Parajuli, A.; Augustin, A.I.; Elahi, A.; Awan, O.; Dako, F. Understanding Biases and Disparities in Radiology AI Datasets: A Review. J. Am. Coll. Radiol. 2023, 20, 836–841. [Google Scholar] [CrossRef] [PubMed]
- Champagne, F.; Lemieux-Charles, L. Using Knowledge and Evidence in Health Care: Multidisciplinary Perspectives; University of Toronto Press: Toronto, ON, Canada, 2004. [Google Scholar]

{kind=link}
| Total Study Participants (n) | 140 Patients |
|---|---|
| Gender | Male—110 patients (79%) |
| Female—30 patients (21%) | |
| Age years | 67.7 ± 8.9 |
| Patients with extrahepatic disease n | 7 (5%) |
| MELD score | 14.5 ± 5.81 |
| AFP ng/mL | 22,996.7 ± 130,814.5 |
| Total bilirubin mg/dL | 1.8 ± 2.1 |
| Total number of tumors n | 205 |
| Location of tumors per hepatic lobe n (%) | Left hepatic lobe—82 (40%) |
| Right hepatic lobe—123 (60%) | |
| Location of tumors per hepatic segment n (%) | Segment 1—1 (0.5%) |
| Segment 2—11 (5.4%) | |
| Segment 3—11 (5.4%) | |
| Segment 4a—19 (9.3%) | |
| Segment 4b—16 (7.8%) | |
| Segment 5—28 (13.7%) | |
| Segment 6—32 (15.6%) | |
| Segment 7—42 (20.5%) | |
| Segment 8—45 (21.9%) | |
| OPTN 5 tumors n (%) | 156 (76%) |
| Mean tumor size cm | 4.71 ± 3.6 |
| Treatment Recommendation | Number of Patients n (%) |
|---|---|
| Intra-arterial therapy (TACE/DEB-TACE) | 42 (30.00%) |
| SIRT/Radioembolization | 26 (18.57%) |
| Ablation (MWA) | 53 (37.86%) |
| Radiotherapy (EBRT/SBRT) | 37 (26.43%) |
| Surgical resection | 22 (15.71%) |
| Transplant | 18 (12.86%) |
| Chemotherapy | 15 (10.71%) |
| Palliative | 10 (7.14%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daye, D.; Parker, R.; Tripathi, S.; Cox, M.; Brito Orama, S.; Valentin, L.; Bridge, C.P.; Uppot, R.N. CASCADE: Context-Aware Data-Driven AI for Streamlined Multidisciplinary Tumor Board Recommendations in Oncology. Cancers 2024, 16, 1975. https://doi.org/10.3390/cancers16111975
Daye D, Parker R, Tripathi S, Cox M, Brito Orama S, Valentin L, Bridge CP, Uppot RN. CASCADE: Context-Aware Data-Driven AI for Streamlined Multidisciplinary Tumor Board Recommendations in Oncology. Cancers. 2024; 16(11):1975. https://doi.org/10.3390/cancers16111975
Chicago/Turabian StyleDaye, Dania, Regina Parker, Satvik Tripathi, Meredith Cox, Sebastian Brito Orama, Leonardo Valentin, Christopher P. Bridge, and Raul N. Uppot. 2024. "CASCADE: Context-Aware Data-Driven AI for Streamlined Multidisciplinary Tumor Board Recommendations in Oncology" Cancers 16, no. 11: 1975. https://doi.org/10.3390/cancers16111975
APA StyleDaye, D., Parker, R., Tripathi, S., Cox, M., Brito Orama, S., Valentin, L., Bridge, C. P., & Uppot, R. N. (2024). CASCADE: Context-Aware Data-Driven AI for Streamlined Multidisciplinary Tumor Board Recommendations in Oncology. Cancers, 16(11), 1975. https://doi.org/10.3390/cancers16111975