

Mixed Reality Biopsy Navigation System Utilizing Markerless Needle Tracking and Imaging Data Superimposition
 , ,
, ,  , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
Related Work
2. Materials and Methods
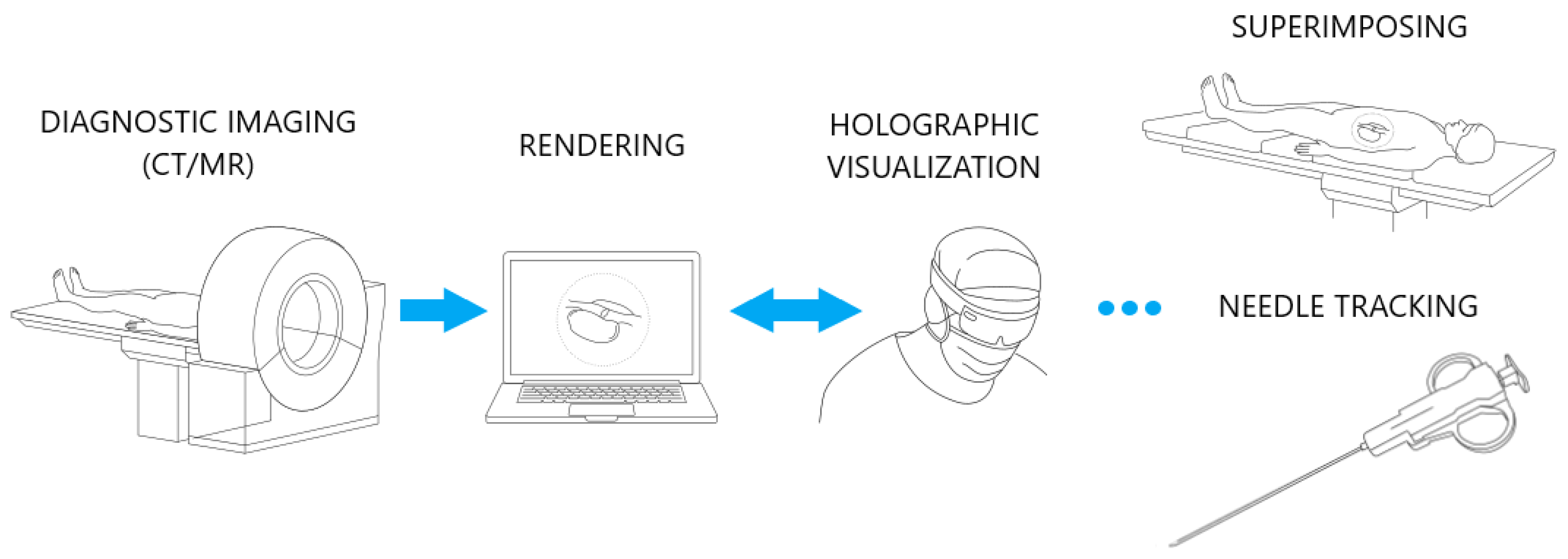
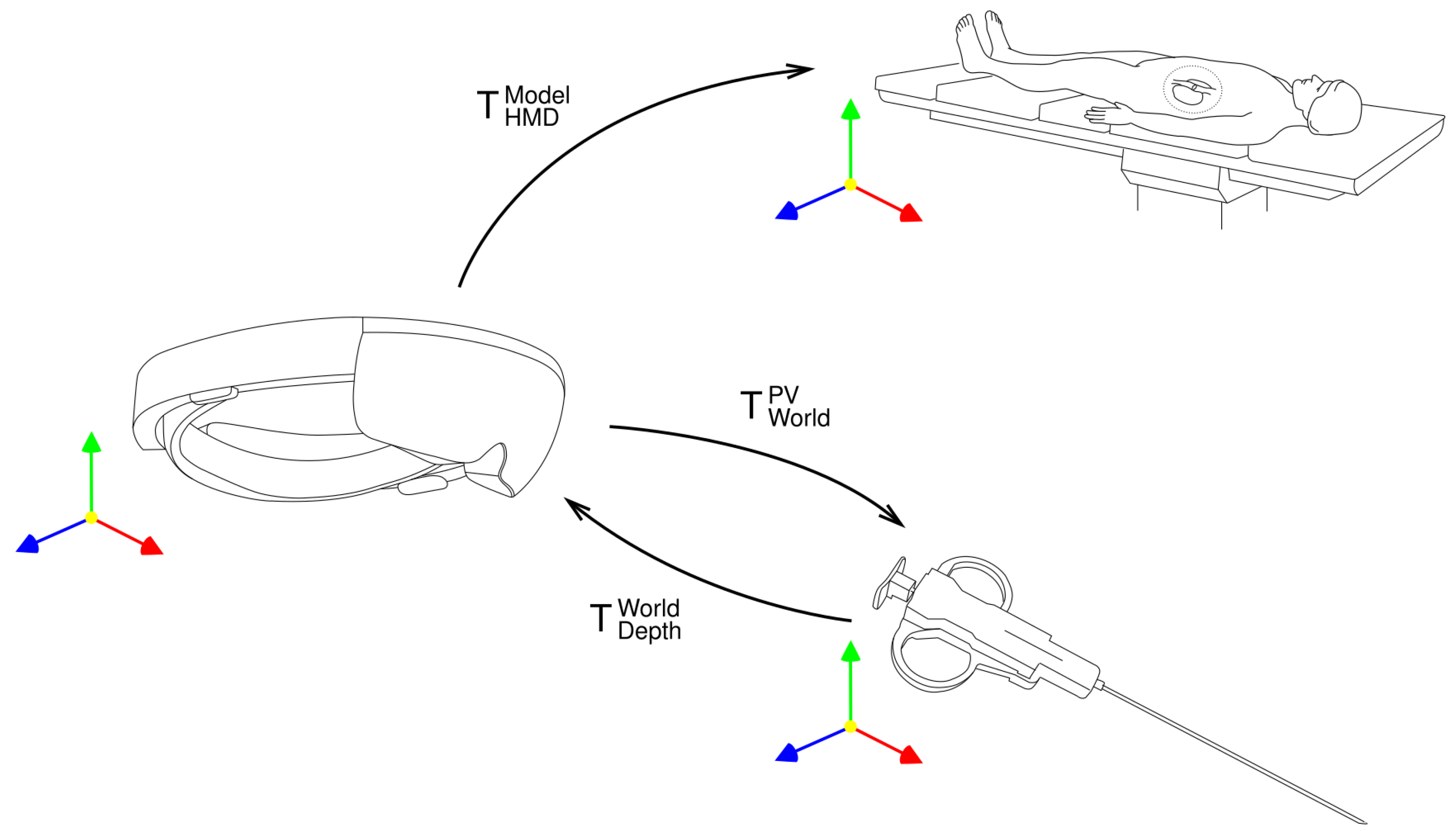
2.1. Proposed Solution
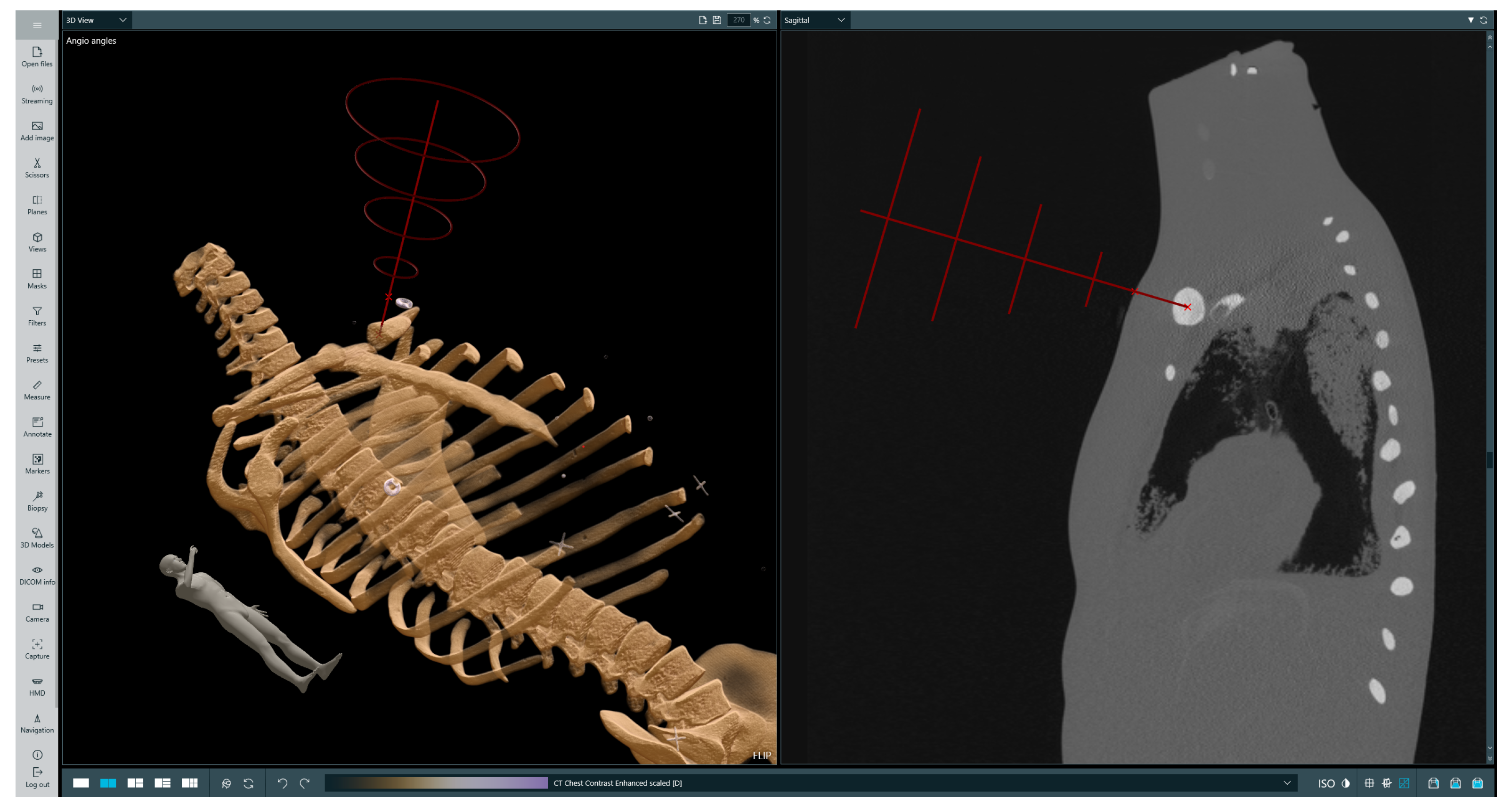
2.2. Clinical Workflow
3. Results
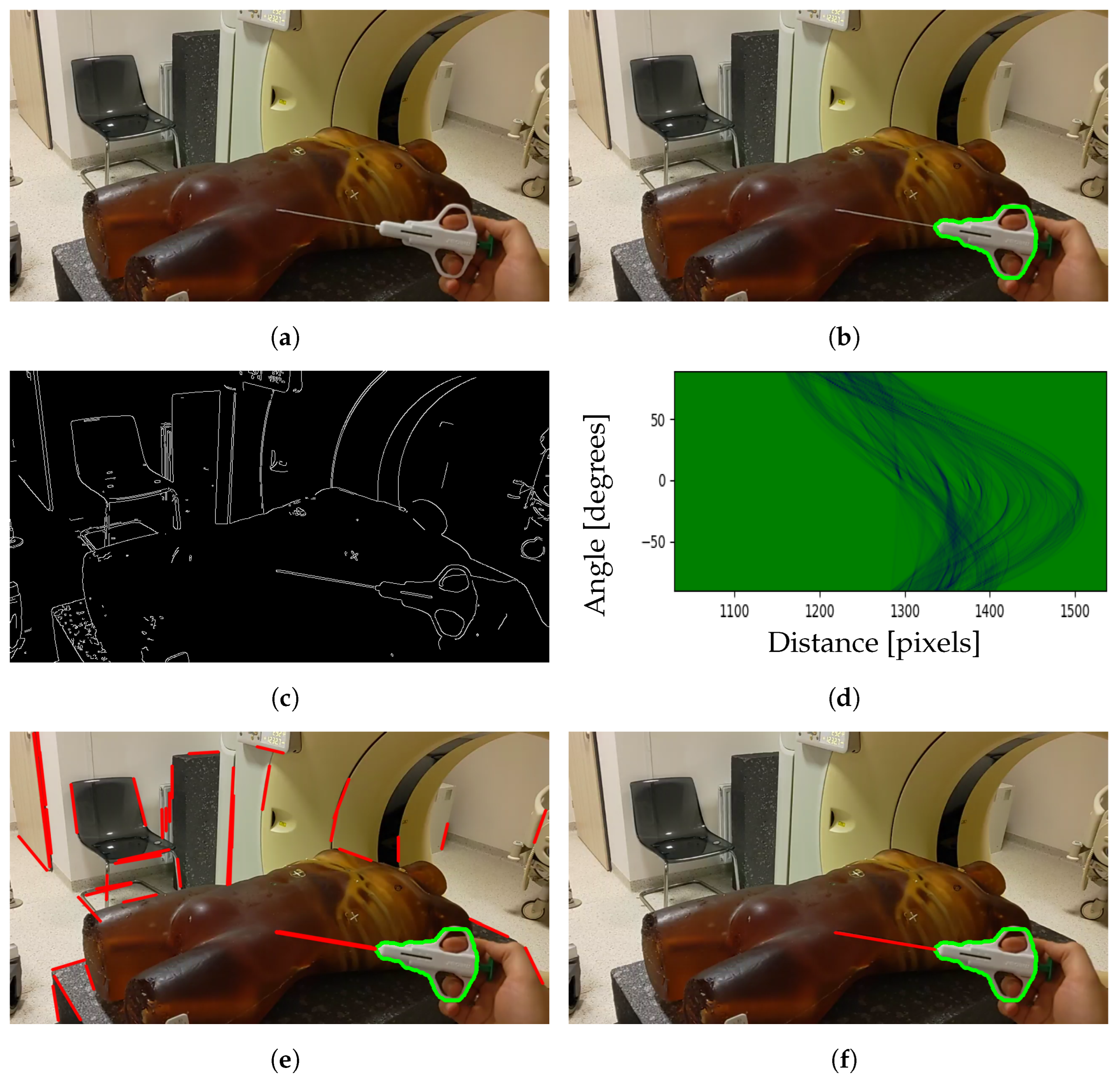
3.1. Needle Pose Estimation Accuracy
3.2. Final Location Error
3.3. Material Collection Efficiency
3.4. Injection Time
4. Discussion
4.1. Results Analysis
4.2. Advantages of the Proposed Approach
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PNB | Percutaneous Needle Biopsy |
| US | Ultrasound |
| CT | Computer Tomography |
| MR | Magnetic Resonance |
| HMD | Head-Mounted Display |
| PV | Photo–Video |
| AHAT | Articulated Hand Tracking |
| AR | Augmented Reality |
| CBCT | Cone–Beam CT |
References
- Veltri, A.; Bargellini, I.; Giorgi, L.; Almeida, P.A.M.S.; Akhan, O. CIRSE Guidelines on Percutaneous Needle Biopsy (PNB). Cardiovasc. Interv. Radiol. 2017, 40, 1501–1513. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Madoff, D.C. Image-Guided Percutaneous Needle Biopsy in Cancer Diagnosis and Staging. Tech. Vasc. Interv. Radiol. 2007, 10, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Ponti, F.; Arioli, A.; Longo, C.; Miceli, M.; Colangeli, M.; Papalexis, N.; Spinnato, P. Ultrasound-Guided Percutaneous Bone Biopsy: Feasibility, Diagnostic Yield and Technical Notes. Diagnostics 2023, 13, 1773. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, N.; Watanabe, T.; Yamada, K.; Nakai, T.; Suzumura, T.; Sakagami, K.; Yoshimoto, N.; Sato, K.; Tanaka, H.; Mitsuoka, S.; et al. Efficacy and safety of ultrasound (US) guided percutaneous needle biopsy for peripheral lung or pleural lesion: Comparison with computed tomography (CT) guided needle biopsy. J. Thorac. Dis. 2019, 11, 936–943. [Google Scholar] [CrossRef]
- Portela-Oliveira, E.; Souza, C.A.; Gupta, A.; Bayanati, H.; Inacio, J.; Rakhra, K. Ultrasound-guided percutaneous biopsy of thoracic lesions: High diagnostic yield and low complication rate. Clin. Radiol. 2021, 76, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Nikodinovska, V.V.; Ivanoski, S.; Kostadinova-Kunovska, S.; Samardziski, M. Ultrasound-guided biopsy of musculoskeletal soft-tissue tumors: Basic principles, usefulness and limitations. J. Ultrason. 2022, 22, 109–116. [Google Scholar] [CrossRef]
- Beigi, P.; Salcudean, S.E.; Ng, G.C.; Rohling, R. Enhancement of needle visualization and localization in ultrasound. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 169–178. [Google Scholar] [CrossRef]
- Pasha, I.; Singh, A.K.; Hashim, Z.; Nath, A.; Neyaz, Z.; Mishra, R.; Agrawal, V. Role of percutaneous CT-guided biopsy in the characterisation of pleural diseases. Lung India 2023, 40, 514. [Google Scholar] [CrossRef]
- Chojniak, R.; Isberner, R.K.; Viana, L.M.; Yu, L.S.; Aita, A.A.; Soares, F.A. Computed tomography guided needle biopsy: Experience from 1300 procedures. Sao Paulo Med. J. 2006, 124, 10–14. [Google Scholar] [CrossRef]
- Chiang, H.; Chen, L.K.; Hsieh, W.P.; Tang, Y.X.; Lo, C.Y. Complications during CT-Guided Lung Nodule Localization: Impact of Needle Insertion Depth and Patient Characteristics. Diagnostics 2023, 13, 1881. [Google Scholar] [CrossRef]
- Wu, C.C.; Maher, M.M.; Shepard, J.A.O. Complications of CT-Guided Percutaneous Needle Biopsy of the Chest: Prevention and Management. Am. J. Roentgenol. 2011, 196, W678–W682. [Google Scholar] [CrossRef]
- Hiraki, T.; Kamegawa, T.; Matsuno, T.; Sakurai, J.; Komaki, T.; Yamaguchi, T.; Tomita, K.; Uka, M.; Matsui, Y.; Iguchi, T.; et al. Robotic needle insertion during computed tomography fluoroscopy–guided biopsy: Prospective first-in-human feasibility trial. Eur. Radiol. 2020, 30, 927–933. [Google Scholar] [CrossRef]
- Weiss, C.R.; Nour, S.G.; Lewin, J.S. MR-guided biopsy: A review of current techniques and applications. J. Magn. Reson. Imaging 2008, 27, 311–325. [Google Scholar] [CrossRef]
- Niketa, C.; Pang, K.A.; Lim, J.W. Challenges in MRI-Guided Breast Biopsy and Some Suggested Strategies: Case Based Review. Diagnostics 2022, 12, 1985. [Google Scholar] [CrossRef] [PubMed]
- Chevrier, M.C.; David, J.; Khoury, M.E.; Lalonde, L.; Labelle, M.; Trop, I. Breast Biopsies Under Magnetic Resonance Imaging Guidance: Challenges of an Essential but Imperfect Technique. Curr. Probl. Diagn. Radiol. 2016, 45, 193–204. [Google Scholar] [CrossRef] [PubMed]
- AL-Maatoq, M.; Fachet, M.; Rao, R.; Hoeschen, C. Artifacts’ Detection for MRI Non-Metallic Needles: Comparative Analysis for Artifact Evaluation Using K-Means and Manual Quantification. Magnetochemistry 2023, 9, 79. [Google Scholar] [CrossRef]
- Witowski, J.; Darocha, S.; Kownacki, L.; Pietrasik, A.; Pietura, R.; Banaszkiewicz, M.; Kamiński, J.; Biederman, A.; Torbicki, A.; Kurzyna, M. Augmented reality and three-dimensional printing in percutaneous interventions on pulmonary arteries. Quant. Imaging Med. Surg. 2019, 9, 23–29. [Google Scholar] [CrossRef]
- Khokhar, A.A.; Zlahoda-Huzior, A.; Stanuch, M.; Ponticelli, F.; Ruggiero, R.; Chandra, K.; Kim, W.K.; Giannini, F.; Dudek, D. Advanced CT-Based Imaging Techniques to Evaluate Coronary Access After TAVI for Degenerated Surgical Bioprosthesis. Can. J. Cardiol. 2022, 38, 392–394. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.Y.; Kageyama, S.; He, X.; Pompilio, G.; Andreini, D.; Pontone, G.; La Meir, M.; De Mey, J.; Tanaka, K.; Doenst, T.; et al. Feasibility and accuracy of real-time 3D-holographic graft length measurements. Eur. Heart J.—Digit. Health 2024, 5, 101–104. [Google Scholar] [CrossRef]
- Kasprzak, J.D.; Pawlowski, J.; Peruga, J.Z.; Kaminski, J.; Lipiec, P. First-in-man experience with real-time holographic mixed reality display of three-dimensional echocardiography during structural intervention: Balloon mitral commissurotomy. Eur. Heart J. 2020, 41, 801. [Google Scholar] [CrossRef]
- Lu, L.; Wang, H.; Liu, P.; Liu, R.; Zhang, J.; Xie, Y.; Liu, S.; Huo, T.; Xie, M.; Wu, X.; et al. Applications of Mixed Reality Technology in Orthopedics Surgery: A Pilot Study. Front. Bioeng. Biotechnol. 2022, 10, 740507. [Google Scholar] [CrossRef]
- Łęgosz, P.; Starszak, K.; Stanuch, M.; Otworowski, M.; Pulik, L.; Złahoda-Huzior, A.; Skalski, A. The Use of Mixed Reality in Custom-Made Revision Hip Arthroplasty: A First Case Report. JoVE (J. Vis. Exp.) 2022, 186, e63654. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, T.; Kobayashi, T.; Hirata, H.; Otani, K.; Sugimoto, M.; Tsukamoto, M.; Yoshihara, T.; Ueno, M.; Mawatari, M. XR (Extended Reality: Virtual Reality, Augmented Reality, Mixed Reality) Technology in Spine Medicine: Status Quo and Quo Vadis. J. Clin. Med. 2022, 11, 470. [Google Scholar] [CrossRef] [PubMed]
- Mialhe, C.; Chaudhuri, A.; Raffort, J.; Lareyre, F. Feasibility of the Application of Holographic Augmented Reality in Endovascular Surgery Using Microsoft HoloLens Head-Mounted Display. Ann. Vasc. Surg. 2021, 76, 597–598. [Google Scholar] [CrossRef] [PubMed]
- Galyfos, G.; Pikula, M.; Skalski, A.; Vagena, S.; Filis, K.; Sigala, F. Using a novel three-dimensional holographic technology to perform open vascular surgery procedures. J. Vasc. Surg. Cases Innov. Tech. 2024, 10, 101440. [Google Scholar] [CrossRef] [PubMed]
- Wierzbicki, R.; Pawłowicz, M.; Job, J.; Balawender, R.; Kostarczyk, W.; Stanuch, M.; Janc, K.; Skalski, A. 3D mixed-reality visualization of medical imaging data as a supporting tool for innovative, minimally invasive surgery for gastrointestinal tumors and systemic treatment as a new path in personalized treatment of advanced cancer diseases. J. Cancer Res. Clin. Oncol. 2022, 148, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Taciuc, I.A.; Dumitru, M.; Vrinceanu, D.; Gherghe, M.; Manole, F.; Marinescu, A.; Serboiu, C.; Neagos, A.; Costache, A. Applications and challenges of neural networks in otolaryngology (Review). Biomed. Rep. 2024, 20, 92. [Google Scholar] [CrossRef]
- Shimizu, H.; Nakayama, K.I. Artificial intelligence in oncology. Cancer Sci. 2020, 111, 1452–1460. [Google Scholar] [CrossRef]
- Rezazade Mehrizi, M.H.; van Ooijen, P.; Homan, M. Applications of artificial intelligence (AI) in diagnostic radiology: A technography study. Eur. Radiol. 2021, 31, 1805–1811. [Google Scholar] [CrossRef]
- Wang, C.; Zhu, X.; Hong, J.C.; Zheng, D. Artificial Intelligence in Radiotherapy Treatment Planning: Present and Future. Technol. Cancer Res. Treat. 2019, 18, 1533033819873922. [Google Scholar] [CrossRef]
- Ward, T.M.; Mascagni, P.; Ban, Y.; Rosman, G.; Padoy, N.; Meireles, O.; Hashimoto, D.A. Computer vision in surgery. Surgery 2021, 169, 1253–1256. [Google Scholar] [CrossRef] [PubMed]
- Skyrman, S.; Lai, M.; Edström, E.; Burström, G.; Förander, P.; Homan, R.; Kor, F.; Holthuizen, R.; Hendriks, B.H.W.; Persson, O.; et al. Augmented reality navigation for cranial biopsy and external ventricular drain insertion. Neurosurg. Focus 2021, 51, E7. [Google Scholar] [CrossRef]
- Albano, D.; Messina, C.; Gitto, S.; Chianca, V.; Sconfienza, L.M. Bone biopsies guided by augmented reality: A pilot study. Eur. Radiol. Exp. 2023, 7, 40. [Google Scholar] [CrossRef] [PubMed]
- Ungureanu, D.; Bogo, F.; Galliani, S.; Sama, P.; Duan, X.; Meekhof, C.; Stühmer, J.; Cashman, T.J.; Tekin, B.; Schönberger, J.L.; et al. HoloLens 2 Research Mode as a Tool for Computer Vision Research. arXiv 2020, arXiv:2008.11239. [Google Scholar] [CrossRef]
- Jocher, G.; Chaurasia, A.; Qiu, J. Ultralytics YOLO (Version 8.0.0). 2023. Available online: https://github.com/ultralytics/ultralytics (accessed on 6 March 2023).
- Mirjalili, S.; Mirjalili, S.M.; Lewis, A. Grey Wolf Optimizer. Adv. Eng. Softw. 2014, 69, 46–61. [Google Scholar] [CrossRef]
- Hassanein, A.S.; Mohammad, S.; Sameer, M.; Ragab, M.E. A Survey on Hough Transform, Theory, Techniques and Applications. arXiv 2015, arXiv:1502.02160. [Google Scholar] [CrossRef]
- Szeliski, R. Computer Vision: Algorithms and Applications; Texts in Computer Science; Springer International Publishing: Berlin/Heidelberg, Germany, 2022. [Google Scholar] [CrossRef]
- Gu, W.; Shah, K.; Knopf, J.; Navab, N.; Unberath, M. Feasibility of image-based augmented reality guidance of total shoulder arthroplasty using microsoft HoloLens 1. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2021, 9, 261–270. [Google Scholar] [CrossRef]
- Zhao, Z.; Poyhonen, J.; Chen Cai, X.; Sophie Woodley Hooper, F.; Ma, Y.; Hu, Y.; Ren, H.; Song, W.; Tsz Ho Tse, Z. Augmented reality technology in image-guided therapy: State-of-the-art review. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2021, 235, 1386–1398. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Modality | Advantages | Disadvantages |
|---|---|---|
| US | Fast acquisition time Real-time needle evaluation Lack of radiation exposure Vessel avoidance (Doppler) Shorter procedure time Less expensive | Operator experience-dependent Poor needle visibility Suitable acoustic window needed Reliant on lesion type, size, and location |
| CT | Exceptional contrast High spatial resolution Applicable across various organs | Higher risk of complications Exposure to radiation Fluoroscopy for real-time imaging |
| MR | High soft tissue contrast No ionizing radiation Vessel visualization without contrast Able to elicit tissue characteristics | Challenging lesion access Difficult lesion sampling verification Tough radiology–pathology matching Compatible needles needed |
| Distance from HMD [cm] | Needle 120 mm | Needle 160 mm | ||
|---|---|---|---|---|
|
Needle Base Error [mm] |
Needle Tip Error [mm] |
Needle Base Error [mm] |
>Needle Tip Error [mm] | |
| 30 | 1.53 ± 0.70 | 3.25 ± 1.59 | 0.89 ± 0.49 | 3.25 ± 1.43 |
| 40 | 1.47 ± 0.50 | 1.61 ± 0.95 | 1.19 ± 0.46 | 2.52 ± 1.04 |
| 50 | 1.16 ± 1.00 | 2.24 ± 1.06 | 0.87 ± 0.23 | 2.60 ± 1.38 |
| 60 | 2.68 ± 1.18 | 2.36 ± 1.37 | 2.80 ± 0.43 | 3.20 ± 1.63 |
| Distance from HMD [cm] | Needle 120 mm | Needle 160 mm | ||
|---|---|---|---|---|
|
Needle Base Error [mm] |
Needle Tip Error [mm] |
Needle Base Error [mm] |
Needle Tip Error [mm] | |
| 30 | 1.08 ± 0.25 | 1.25 ± 0.75 | 1.04 ± 0.37 | 1.76 ± 0.82 |
| 40 | 0.88 ± 0.23 | 1.77 ± 0.64 | 0.87 ± 0.24 | 2.56 ± 0.96 |
| 50 | 1.63 ± 0.52 | 3.36 ± 1.37 | 1.65 ± 0.48 | 3.55 ± 1.07 |
| 60 | 3.12 ± 1.04 | 2.05 ± 1.01 | 4.23 ± 0.75 | 3.21 ± 2.19 |
| Exam No. | Puncture Depth [mm] | Distance to Lesion [mm] |
|---|---|---|
| 1 | 62.39 | 0 |
| 2 | 109.15 | 9.74 |
| 3 | 165.96 | 8.17 |
| Lesion Diameter [cm] | Distance to Lesion Range [cm] | Correct Punctures No. | Accuracy |
|---|---|---|---|
| 5 | 4–10 | 24 | 100% |
| 2 | 3.6–8 | 23 | 95.83% |
| Exam No. | Experience >3 Years | With System | Without System | Time Difference | ||
|---|---|---|---|---|---|---|
| Punctures No. | Total Time | Punctures No. | Total Time | |||
| 1 | NO | 1 | 03:08 | 2 | 09:13 | 66% |
| 2 | NO | 1 | 00:09 | 1 | 00:17 | 47% |
| 3 | NO | 2 | 00:42 | 4 | 01:27 | 52% |
| 4 | YES | 1 | 00:17 | 3 | 01:08 | 75% |
| 5 | YES | 1 | 00:14 | 4 | 01:37 | 86% |
| 6 | YES | 1 | 00:07 | 1 | 00:13 | 46% |
| 7 | YES | 1 | 00:40 | 2 | 01:21 | 51% |
| 8 | YES | 3 | 02:31 | 3 | 02:14 | −13% |
| 9 | NO | 1 | 00:06 | 2 | 00:23 | 74% |
| 10 | YES | 2 | 00:57 | 3 | 01:42 | 44% |
| Average | 1.4 | 00:53 | 2.5 | 01:57 | 53% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trojak, M.; Stanuch, M.; Kurzyna, M.; Darocha, S.; Skalski, A. Mixed Reality Biopsy Navigation System Utilizing Markerless Needle Tracking and Imaging Data Superimposition. Cancers 2024, 16, 1894. https://doi.org/10.3390/cancers16101894
Trojak M, Stanuch M, Kurzyna M, Darocha S, Skalski A. Mixed Reality Biopsy Navigation System Utilizing Markerless Needle Tracking and Imaging Data Superimposition. Cancers. 2024; 16(10):1894. https://doi.org/10.3390/cancers16101894
Chicago/Turabian StyleTrojak, Michał, Maciej Stanuch, Marcin Kurzyna, Szymon Darocha, and Andrzej Skalski. 2024. "Mixed Reality Biopsy Navigation System Utilizing Markerless Needle Tracking and Imaging Data Superimposition" Cancers 16, no. 10: 1894. https://doi.org/10.3390/cancers16101894
APA StyleTrojak, M., Stanuch, M., Kurzyna, M., Darocha, S., & Skalski, A. (2024). Mixed Reality Biopsy Navigation System Utilizing Markerless Needle Tracking and Imaging Data Superimposition. Cancers, 16(10), 1894. https://doi.org/10.3390/cancers16101894