
Influence of the Planning Parameters of a New Algorithm on the Dosimetric Quality, Beam-On Time and Delivery Accuracy of Tomotherapy Plans

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Optimization Parameters
2.3. Metrics Used for Treatment Plan Quality Assessment
2.4. Impact of the LOT Cutoff on the Delivery Accuracy
2.5. Statistical Analysis
3. Results
4. Discussion
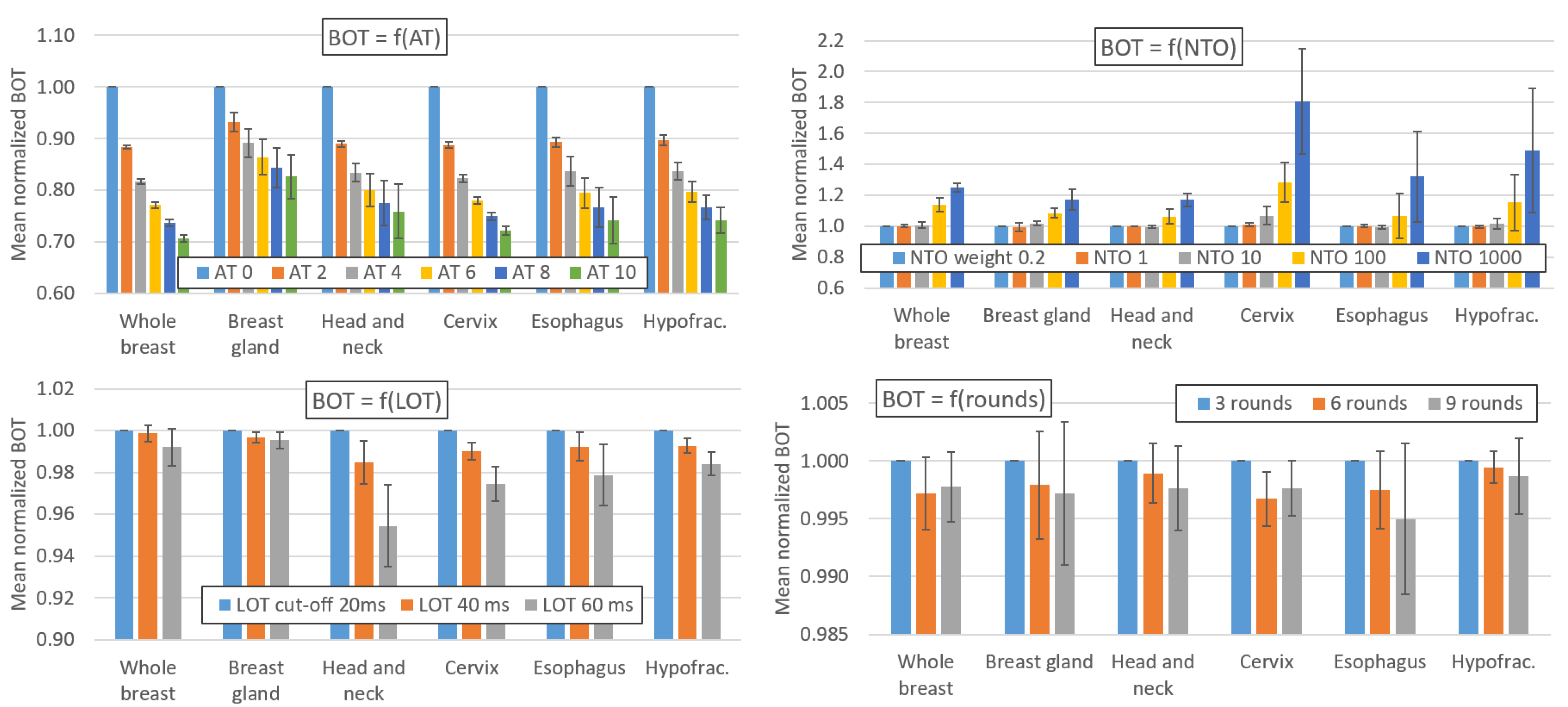
4.1. Effect of the AT Parameter on the Beam-On Time
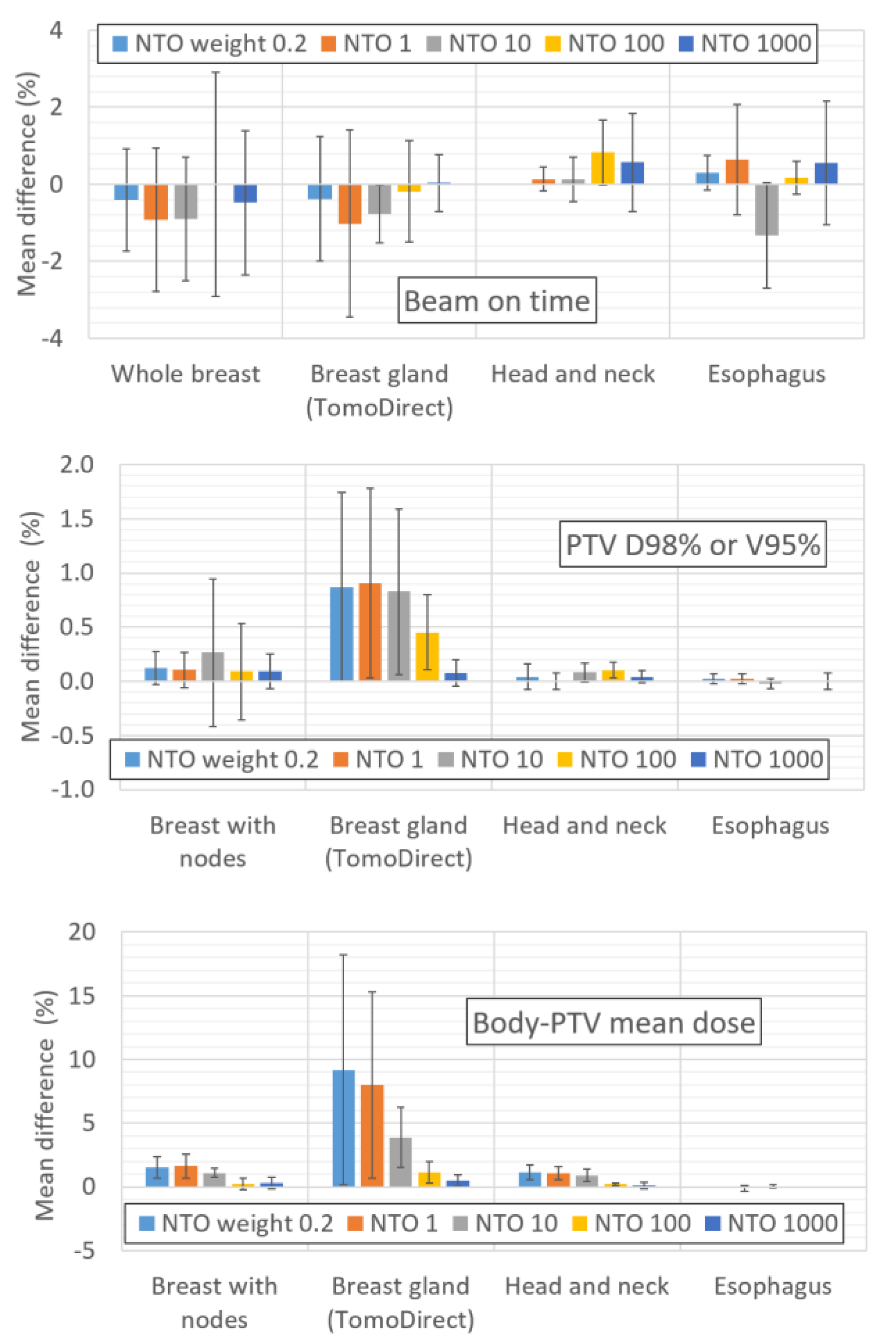
4.2. Effect of the LOT, NTO and Number of Rounds on the Beam-On Time
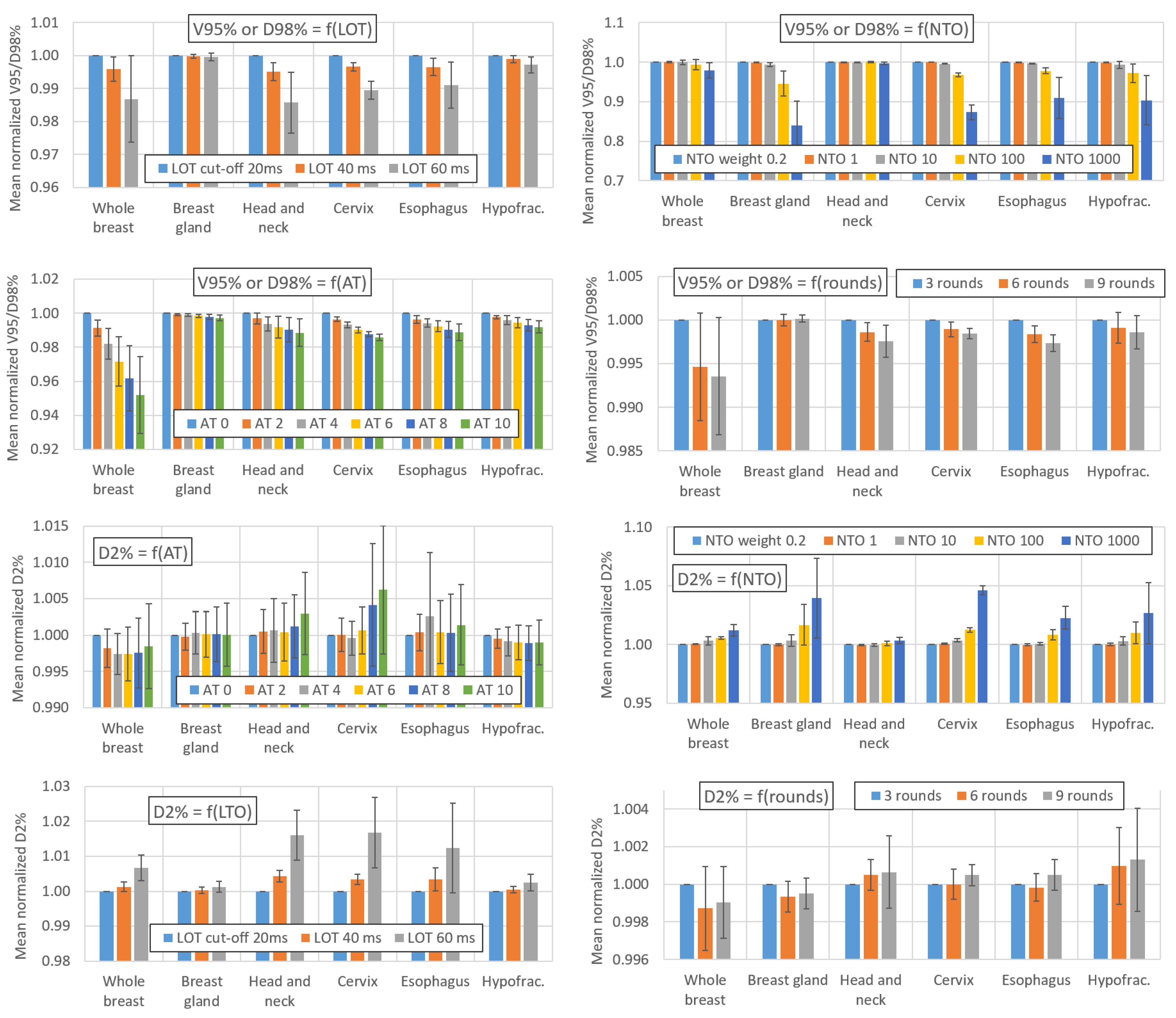
4.3. Effect of the AT, LOT, NTO and Number of Rounds on the PTV Coverage
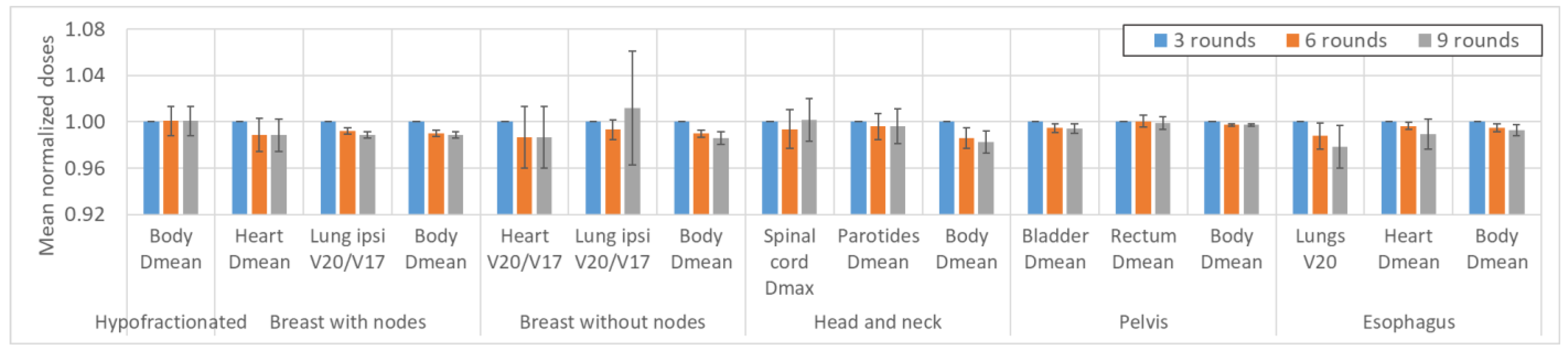
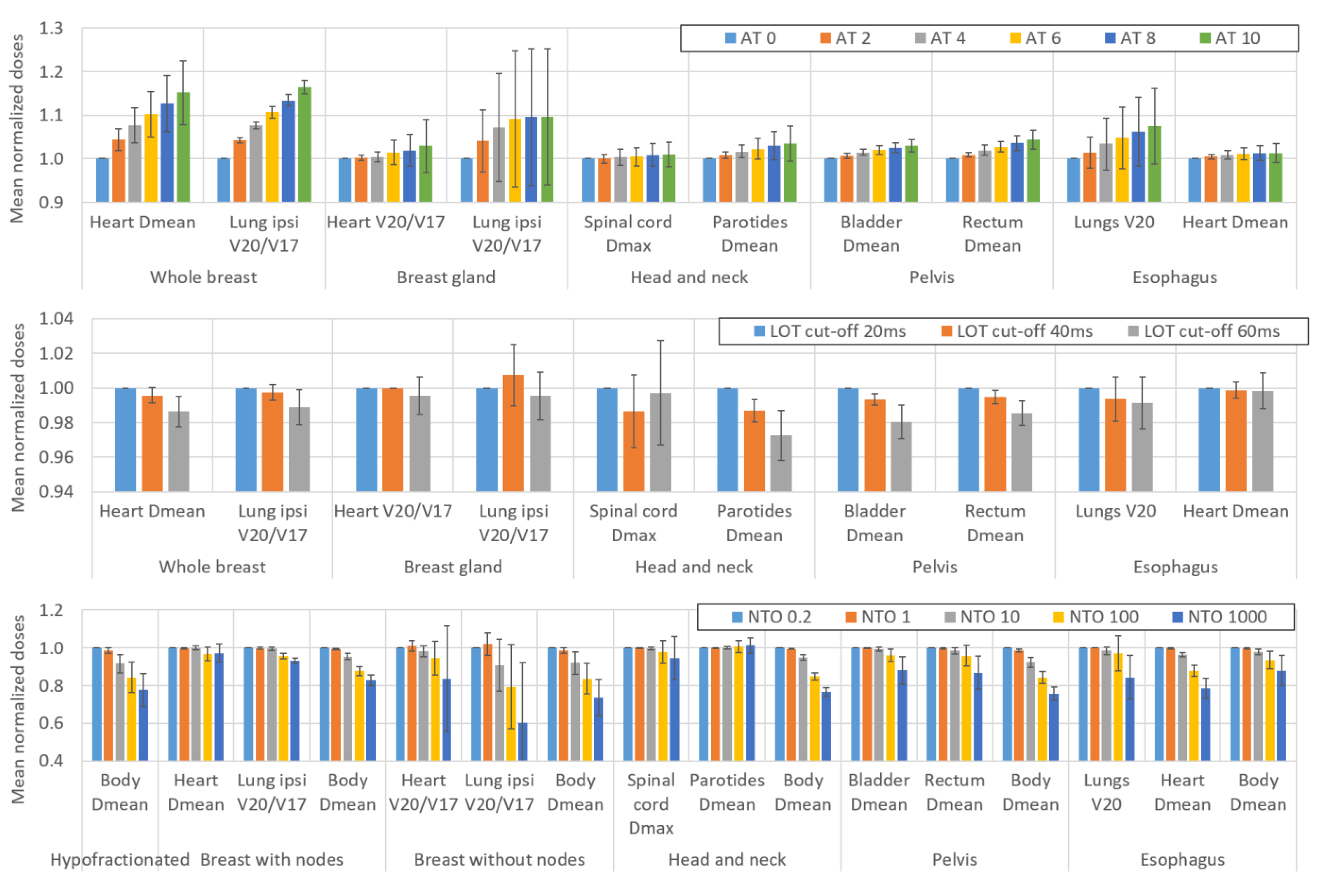
4.4. Effect of the AT, LOT, NTO and Number of Rounds on the Dose to the Organs at Risk
4.5. Effect of Using a Ring on the NTO Weight
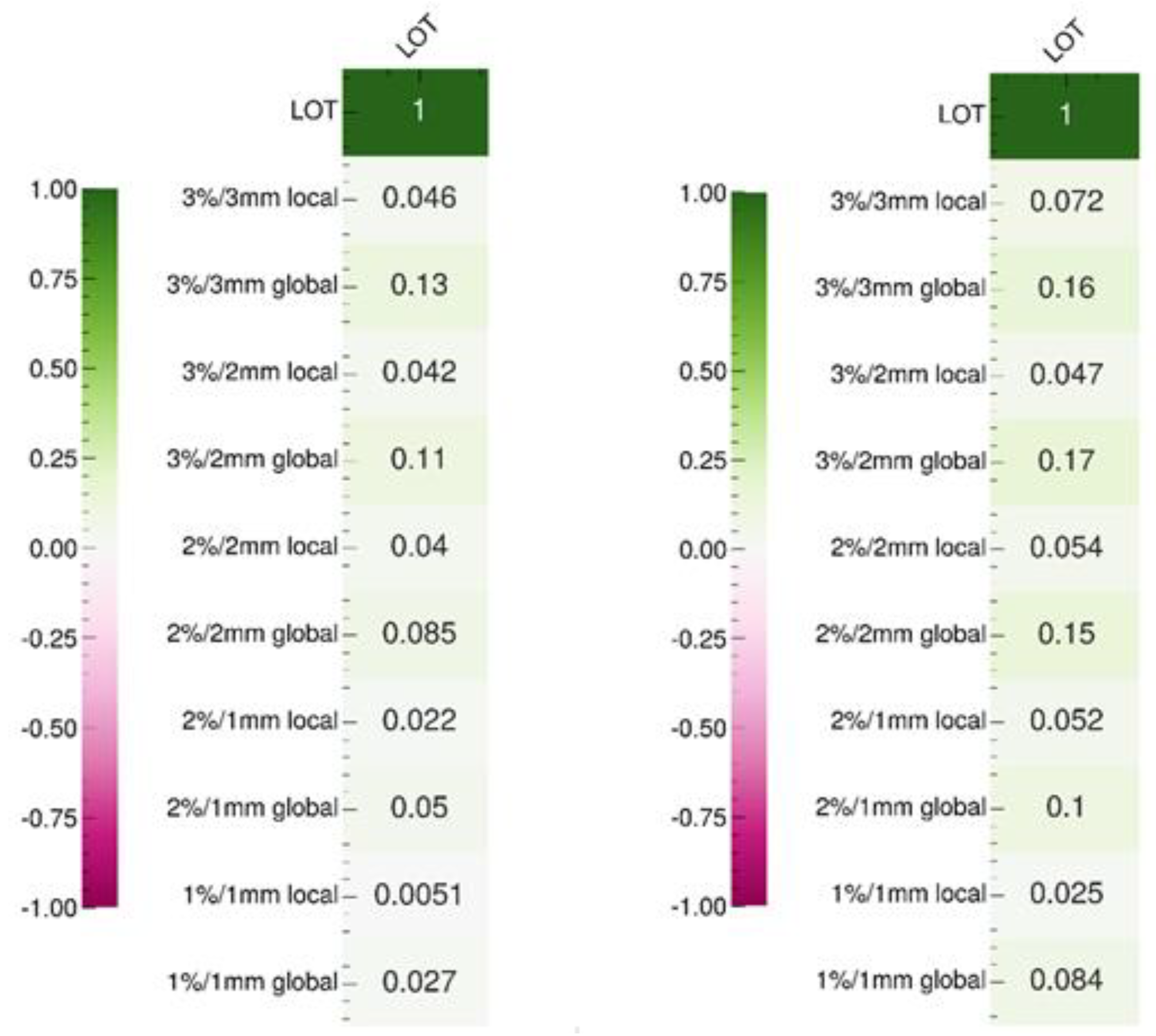
4.6. Effect of the LOT Cutoff Parameter on the Delivery Accuracy
4.7. Synthesis and Suggested Planning Parameter Values
4.8. Limitations and Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Localization | OAR | Dosimetric Parameter | |
|---|---|---|---|
| Whole Breast (with nodes) | Heart, ipsilateral lung | Dmean (Gy), V20 or V17Gy (%) a | |
| Controlateral lung and breast, esophagus, spinal canal, body-PTV | Dmean (Gy) | ||
| Head-and-neck | Brainstem, spinalcord | Dmax (Gy) | |
| Left and right parotids, larynx, constrictor muscle, oral cavity, body-PTV | Dmean (Gy) | ||
| Cervix | Bowel_Bag | V20 and V45Gy (cm3) | |
| Bladder, rectum anal canal, body-PTV | Dmean (Gy) | ||
| Esophagus | Lungs-PTV | Dmean (Gy), V20 and V30Gy (%) | |
| Heart | Dmean (Gy) and V30Gy (%) | ||
| Liver | V15Gy (cm3) | ||
| SpinalCanal, body-PTV | Dmax (Gy) | ||
| Palliative | Stomach (3 patients) | Kidneys, liver, heart, body-PTV | Dmean (Gy) |
| Rectum | Bladder, bowel bag, body-PTV | Dmean (Gy) | |
| Cervix | Rectum, bladder, bowel bag, body-PTV | Dmean (Gy) | |
| Nasal cavity | Left and right eyes, oral cavity, body-PTV | Dmean (Gy) | |
| Breast gland (without nodes) | Heart | Dmean (Gy) | |
| Heart, ipsilateral lung | V20 or V17Gy (%) a | ||
| Controlateral lung | V4 or V3.5Gy (%) a | ||
| Body-PTV | Dmean (Gy) | ||
Appendix C
| 3%/3 mm 10% Local | 3%/3 mm 10% Global | 2%/2 mm 10% Local | 2%/2 mm 10% Global | 1%/1 mm 10% Local | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient | Localization | AT | LOT 20 | LOT 40 | LOT 60 | LOT 20 | LOT 40 | LOT 60 | LOT 20 | LOT 40 | LOT 60 | LOT 20 | LOT 40 | LOT 60 | LOT 20 | LOT 40 | LOT 60 |
| 1 | Whole Breast | AT 0 | 91 | 91.6 | 92 | 99.4 | 99.1 | 99.5 | 73.2 | 73.5 | 74.4 | 95.1 | 95.4 | 96.5 | 45.1 | 44.5 | 45.4 |
| 1 | Whole Breast | AT 4 | 91.8 | 91.4 | 93 | 99.4 | 99.7 | 99.7 | 74 | 71.3 | 74 | 95.6 | 96.2 | 96.4 | 45.2 | 42.5 | 44.8 |
| 1 | Whole Breast | AT 10 | 92.5 | 91.5 | 92.3 | 99.7 | 99.7 | 99.7 | 74.5 | 74.1 | 74.2 | 96.4 | 96.6 | 97.8 | 43.9 | 43.3 | 44.7 |
| 2 | Whole Breast | AT 4 | 92.1 | 93 | 92 | 98.3 | 98.4 | 98.4 | 76.5 | 77.3 | 77.5 | 93.3 | 93.2 | 93.5 | 46.4 | 45 | 45.8 |
| 3 | Whole Breast | AT 4 | 96 | 95.7 | 96.6 | 99.5 | 99.5 | 99.8 | 84.9 | 85.4 | 86.8 | 95.1 | 95.7 | 96.9 | 54.4 | 53.8 | 54.7 |
| 4 | Whole Breast | AT 4 | 89.6 | 89.1 | 89.3 | 98.8 | 99 | 99.1 | 72.9 | 72.6 | 74.7 | 92 | 92.9 | 92.6 | 42.9 | 42.8 | 45.4 |
| 5 | Whole Breast | AT 4 | 86.6 | 85.7 | 85.2 | 99.8 | 99.6 | 99.8 | 69.3 | 66.2 | 66.1 | 95.2 | 94.6 | 95 | 38.4 | 35.6 | 35.3 |
| 6 | Whole Breast | AT 4 | 93.5 | 93.8 | 93.9 | 100 | 99.5 | 100 | 81.5 | 82.2 | 81.6 | 96.9 | 96.4 | 96.7 | 48.4 | 46.6 | 46.7 |
| 7 | Head and neck | AT 4 | 88 | 88.5 | 88.7 | 96.7 | 97.1 | 97.5 | 68.5 | 70.5 | 71.6 | 89.1 | 89.2 | 90 | 36 | 35.5 | 37.5 |
| 8 | Cervix | AT 4 | 87.7 | 88.8 | 90.2 | 96.8 | 97.5 | 98.2 | 66.9 | 67.2 | 66.8 | 88.5 | 90 | 89.4 | 38.5 | 38.6 | 36.6 |
| 9 | Esophagus | AT 4 | 88.1 | 88.1 | 87.5 | 99.2 | 99.6 | 99.6 | 66.8 | 65.7 | 67.7 | 92.2 | 93.3 | 93.8 | 36.8 | 37.2 | 38.2 |
| 10 | Paliative hypofrac. | AT 4 | 92 | 91.3 | 91.9 | 97.9 | 97.5 | 97.9 | 68.1 | 66.9 | 68.6 | 81.8 | 80.9 | 83.1 | 37.4 | 36.8 | 39.1 |
| 1%/1 mm 10% global | 3%/2 mm 10% local | 3%/2 mm 10% global | 2%/1 mm 10% local | 2%/1 mm 10% global | |||||||||||||
| 1 | Whole Breast | AT 0 | 63.1 | 63.7 | 64.8 | 80 | 79.3 | 80.7 | 98.6 | 98.4 | 98.7 | 50.2 | 50.2 | 50.3 | 88.6 | 89.1 | 90.4 |
| 1 | Whole Breast | AT 4 | 67.2 | 62.1 | 66.6 | 82 | 79.6 | 82.4 | 98.9 | 99.2 | 98.9 | 49.3 | 47.5 | 50.4 | 90.9 | 90.5 | 91.1 |
| 1 | Whole Breast | AT 10 | 64.2 | 64.6 | 66.2 | 82.7 | 82.6 | 83.9 | 99.4 | 99.4 | 99.5 | 49.8 | 49.1 | 51.2 | 90.3 | 91.1 | 93 |
| 2 | Whole Breast | AT 4 | 57.4 | 56.2 | 57.5 | 84.7 | 85.6 | 85.2 | 97.4 | 97.7 | 98 | 54 | 53.2 | 55.4 | 83 | 82.9 | 83.2 |
| 3 | Whole Breast | AT 4 | 69.7 | 68.8 | 69.3 | 91.6 | 91.2 | 92.2 | 98.6 | 98.6 | 99.4 | 63.8 | 63.7 | 64.8 | 87.6 | 88.4 | 88.8 |
| 4 | Whole Breast | AT 4 | 56.1 | 54.6 | 57.5 | 80.9 | 80.5 | 81.4 | 97.5 | 97.7 | 98 | 50.9 | 49.2 | 51.7 | 83.8 | 84.2 | 85 |
| 5 | Whole Breast | AT 4 | 56.7 | 55 | 54.6 | 76.1 | 73.5 | 74.2 | 98.5 | 98.5 | 98.8 | 43.5 | 41.3 | 41.5 | 85.2 | 84.5 | 85.3 |
| 6 | Whole Breast | AT 4 | 65.5 | 66.3 | 65 | 87.1 | 88.2 | 87.7 | 98.9 | 98.4 | 98.7 | 56.6 | 55 | 55.3 | 88.5 | 87.9 | 88 |
| 7 | Head and neck | AT 4 | 63.2 | 63.5 | 64.7 | 77.9 | 77.9 | 79.5 | 94.3 | 94.8 | 95.1 | 44.7 | 45.5 | 45.7 | 83.1 | 82.1 | 83.8 |
| 8 | Cervix | AT 4 | 62.9 | 62.8 | 63.6 | 77.2 | 78.4 | 78.5 | 93.8 | 95.3 | 95.4 | 47.5 | 46.9 | 45.8 | 84.6 | 85.7 | 85.4 |
| 9 | Esophagus | AT 4 | 48.8 | 49.1 | 50.2 | 74.3 | 73.9 | 75.3 | 98.2 | 98.6 | 98.7 | 42.1 | 42 | 43.2 | 80.8 | 82.3 | 82.9 |
| 10 | Paliative hypofrac. | AT 4 | 40.8 | 40 | 41.8 | 80.2 | 78.6 | 79.7 | 93.3 | 92.5 | 94.3 | 44 | 43.8 | 45 | 64.5 | 61.7 | 64.4 |
Appendix D
Appendix E
Appendix F
Appendix G
References
- Mackie, T.R. History of Tomotherapy. Phys. Med. Biol. 2006, 51, R427–R453. [Google Scholar] [CrossRef] [PubMed]
- Rong, Y.; Chen, Y.; Shang, L.; Zuo, L.; Lu, W.; Chen, Q. Helical Tomotherapy with Dynamic Running-Start-Stop Delivery Compared to Conventional Tomotherapy Delivery. Med. Phys. 2014, 41, 051709. [Google Scholar] [CrossRef] [PubMed]
- Ferris, W.S.; Kissick, M.W.; Bayouth, J.E.; Culberson, W.S.; Smilowitz, J.B. Evaluation of Radixact Motion Synchrony for 3D Respiratory Motion: Modeling Accuracy and Dosimetric Fidelity. J. Appl. Clin. Med. Phys. 2020, 21, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Tegtmeier, R.C.; Ferris, W.S.; Bayouth, J.E.; Miller, J.R.; Culberson, W.S. Characterization of Imaging Performance of a Novel Helical kVCT for Use in Image-Guided and Adaptive Radiotherapy. J. Appl. Clin. Med. Phys. 2022, 23, e13648. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Lu, W.; Chen, Y.; Chen, M.; Henderson, D.; Sterpin, E. Validation of GPU Based TomoTherapy Dose Calculation Engine. Med. Phys. 2012, 39, 1877–1886. [Google Scholar] [CrossRef] [PubMed]
- Dooley, J. White Paper: Performance Assessment and Treatment Plan Quality for Radixact® and TomoTherapy® Treatment Delivery Systems; Accuray Incorporated: Sunnyvale, CA, USA, 2021. [Google Scholar]
- Byrd, R.H.; Lu, P.; Nocedal, J.; Zhu, C. A Limited Memory Algorithm for Bound Constrained Optimization. SIAM J. Sci. Comput. 1995, 16, 1190–1208. [Google Scholar] [CrossRef]
- Boyd, R.; Jeong, K.; Tomé, W.A. Determining Efficient Helical IMRT Modulation Factor from the MLC Leaf-open Time Distribution on Precision Treatment Planning System. J. Appl. Clin. Med. Phys. 2019, 20, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Westerly, D.C.; Soisson, E.; Chen, Q.; Woch, K.; Schubert, L.; Olivera, G.; Mackie, T.R. Treatment Planning to Improve Delivery Accuracy and Patient Throughput in Helical Tomotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 1290–1297. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Chen, Y.; Chen, Q.; Lu, W. Theoretical Analysis of the Thread Effect in Helical TomoTherapy: Theoretical Analysis of the Thread Effect. Med. Phys. 2011, 38, 5945–5960. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Verneris, M.R.; Dusenbery, K.E.; Wilke, C.T.; Storme, G.; Weisdorf, D.J.; Hui, S.K. Peripheral Dose Heterogeneity Due to the Thread Effect in Total Marrow Irradiation with Helical Tomotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Cavinato, S.; Fusella, M.; Paiusco, M.; Scaggion, A. Quantitative Assessment of Helical Tomotherapy Plans Complexity. J. Appl. Clin. Med. Phys. 2023, 24, e13781. [Google Scholar] [CrossRef] [PubMed]
- Cavinato, S.; Bettinelli, A.; Dusi, F.; Fusella, M.; Germani, A.; Marturano, F.; Paiusco, M.; Pivato, N.; Rossato, M.A.; Scaggion, A. Prediction Models as Decision-Support Tools for Virtual Patient-Specific Quality Assurance of Helical Tomotherapy Plans. Phys. Imaging Radiat. Oncol. 2023, 26, 100435. [Google Scholar] [CrossRef] [PubMed]
- Binny, D.; Lancaster, C.M.; Harris, S.; Sylvander, S.R. Effects of Changing Modulation and Pitch Parameters on Tomotherapy Delivery Quality Assurance Plans. J. Appl. Clin. Med. Phys. 2015, 16, 87–105. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Han, M.C.; Lee, Y.K.; Shin, H.-B.; Kim, H.; Kim, J.S. Comprehensive Clinical Evaluation of TomoEQA for Patient-Specific Pre-Treatment Quality Assurance in Helical Tomotherapy. Radiat. Oncol. 2022, 17, 177. [Google Scholar] [CrossRef] [PubMed]
- Binny, D.; Lancaster, C.M.; Byrne, M.; Kairn, T.; Trapp, J.V.; Crowe, S.B. Tomotherapy Treatment Site Specific Planning Using Statistical Process Control. Phys. Medica 2018, 53, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Meyer, P.; Bouhours, H.; Dehaynin, N.; Jarnet, D.; Gantier, M.; Karamanoukian, D.; Niederst, C. The Optimal Tomotherapy Treatment Planning Parameters for Extremity Soft Tissue Sarcomas. Phys. Medica 2015, 31, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Hirata, M.; Hanaoka, K.; Matsumoto, K.; Tamura, M.; Okumura, M.; Monzen, H. The Impact of the Offset Distance between the Planning Target Volume and Isocenter on Irradiation Time in TomoTherapy: A Phantom Study. Phys. Med. 2019, 63, 19–24. [Google Scholar] [CrossRef] [PubMed]
| Location | Number of Patients | Technique | FW/Pitch | Number of Fraction × Dose/Fraction |
|---|---|---|---|---|
| Whole breast (with nodes) | 3 patients: left breast 3 patients: right breast | TomoHelical | 5/[0.285–0.296] | 3 patients: 25 × 2 Gy 3 patients: 15 × 2.67 Gy |
| Head-and-neck | 6 | TomoHelical | 2.5/[0.428–0.440] | 3 patients: 33 × 1.64–33 × 2.12 Gy (SIB) 3 patients: 33 × 1.65–33 × 2 Gy (SIB) |
| Cervix | 6 | TomoHelical | 5/[0.431–0.435] | 4 patients: 25 × 1.8 Gy 2 patients: 25 × 1.8–25 × 2.2 Gy (SIB) |
| Esophagus | 6 | TomoHelical | 5/[0.427–0.443] | 6 patients: 20 × 2 Gy |
| Hypofractionated | 6 | TomoHelical | 5/[0.221–0.227] | 6 patients: 2 × 6.5 Gy |
| Breast gland (without nodes) | 3 patients: left breast 3 patients: right breast | TomoDirect | 5/0.5 | 3 patients: 25 × 2 Gy 3 patients: 15 × 2.67 Gy |
| AT | LOT Cutoff (ms) | NTO Weight | Iteration Rounds | Use of a 5 cm Ring | Number of Plans |
|---|---|---|---|---|---|
| 0–2–4–6–8–10 | 20–40–60 | 0.2 | 3 or 6 (for BG) | Yes | 648 |
| 4 (for cervix, H&N, WB, and esophagus) or 10 (for BG and HP) | 20 | 0.2–1–10–100–1000 | 3 or 6 (for BG) | No | 180 |
| 4 (for H&N, WB, and esophagus) or 10 (for BG) | 20 | 0.2–1–10–100–1000 | 3 or 6 (for BG) | Yes | 120 a |
| 4 (for cervix, H&N, WB, and esophagus) or 10 (for BG and HP) | 20 | 10 | 3–6–9 | No | 108 |
| Patients | Location/Treatment | AT | LOT Cutoff |
|---|---|---|---|
| 1 | Whole breast | 0–4–10 | 20–40–60 |
| 2–3–4–5–6 | Whole breast | 4 | 20–40–60 |
| 7 | Head and neck | 4 | 20–40–60 |
| 8 | Cervix | 4 | 20–40–60 |
| 9 | Esophagus | 4 | 20–40–60 |
| 10 | Hypofractionated | 4 | 20–40–60 |
| BOT | PTV D98%/V95% | PTV D2% | OAR | ||
|---|---|---|---|---|---|
| AT | 0->2 | −11% (−7% for TD) | −2% (0% for TD) | ≈ 0 | +0 to 15% * |
| 2->4 | −7% (−4% for TD) | ||||
| 4->6 | −5% (−3% for TD) | ||||
| 6->8 | −4% (−2% for TD) | ||||
| 8->10 | −3% (−2% for TD) | ||||
| LOT cutoff | 20->40 | ≈0 | ≈0 | ≈ 0 | ≈0 |
| 40->60 | −2% | −1% | +1% | −1% * | |
| NTO | 0.2->1 | ≈0 | ≈0 | ≈ 0 | −1% ** |
| 1->10 | +2% | ≈0 | ≈ 0 | −5% ** | |
| 10->100 | +12% | −2% | +1% | −8% ** | |
| 100->1000 | +25% | −5% | +2% | −8% ** | |
| Rounds | 3->6 | ≈0 | ≈0 | ≈ 0 | −1% |
| 6->9 | ≈0 | ≈0 | ≈ 0 | ≈0 | |
| No rings | ≈0 | ≈0 | Not studied | +2% ** if NTO < 10 (+10% for TD) ≈0 ** if NTO ≥ 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burckbuchler, T.; Dehaynin, N.; Niederst, C.; Bartolucci, L.; Elazhar, H.; Jarnet, D.; Arbor, F.; Meyer, P. Influence of the Planning Parameters of a New Algorithm on the Dosimetric Quality, Beam-On Time and Delivery Accuracy of Tomotherapy Plans. Cancers 2024, 16, 1883. https://doi.org/10.3390/cancers16101883
Burckbuchler T, Dehaynin N, Niederst C, Bartolucci L, Elazhar H, Jarnet D, Arbor F, Meyer P. Influence of the Planning Parameters of a New Algorithm on the Dosimetric Quality, Beam-On Time and Delivery Accuracy of Tomotherapy Plans. Cancers. 2024; 16(10):1883. https://doi.org/10.3390/cancers16101883
Chicago/Turabian StyleBurckbuchler, Théo, Nicolas Dehaynin, Claudine Niederst, Laurent Bartolucci, Halima Elazhar, Delphine Jarnet, Florence Arbor, and Philippe Meyer. 2024. "Influence of the Planning Parameters of a New Algorithm on the Dosimetric Quality, Beam-On Time and Delivery Accuracy of Tomotherapy Plans" Cancers 16, no. 10: 1883. https://doi.org/10.3390/cancers16101883
APA StyleBurckbuchler, T., Dehaynin, N., Niederst, C., Bartolucci, L., Elazhar, H., Jarnet, D., Arbor, F., & Meyer, P. (2024). Influence of the Planning Parameters of a New Algorithm on the Dosimetric Quality, Beam-On Time and Delivery Accuracy of Tomotherapy Plans. Cancers, 16(10), 1883. https://doi.org/10.3390/cancers16101883