
The Efficacy and Safety of Neoadjuvant Immunotherapy in Patients with Non-Small Cell Lung Cancer


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Data Extraction
2.3. Meta-Analyses
3. Results
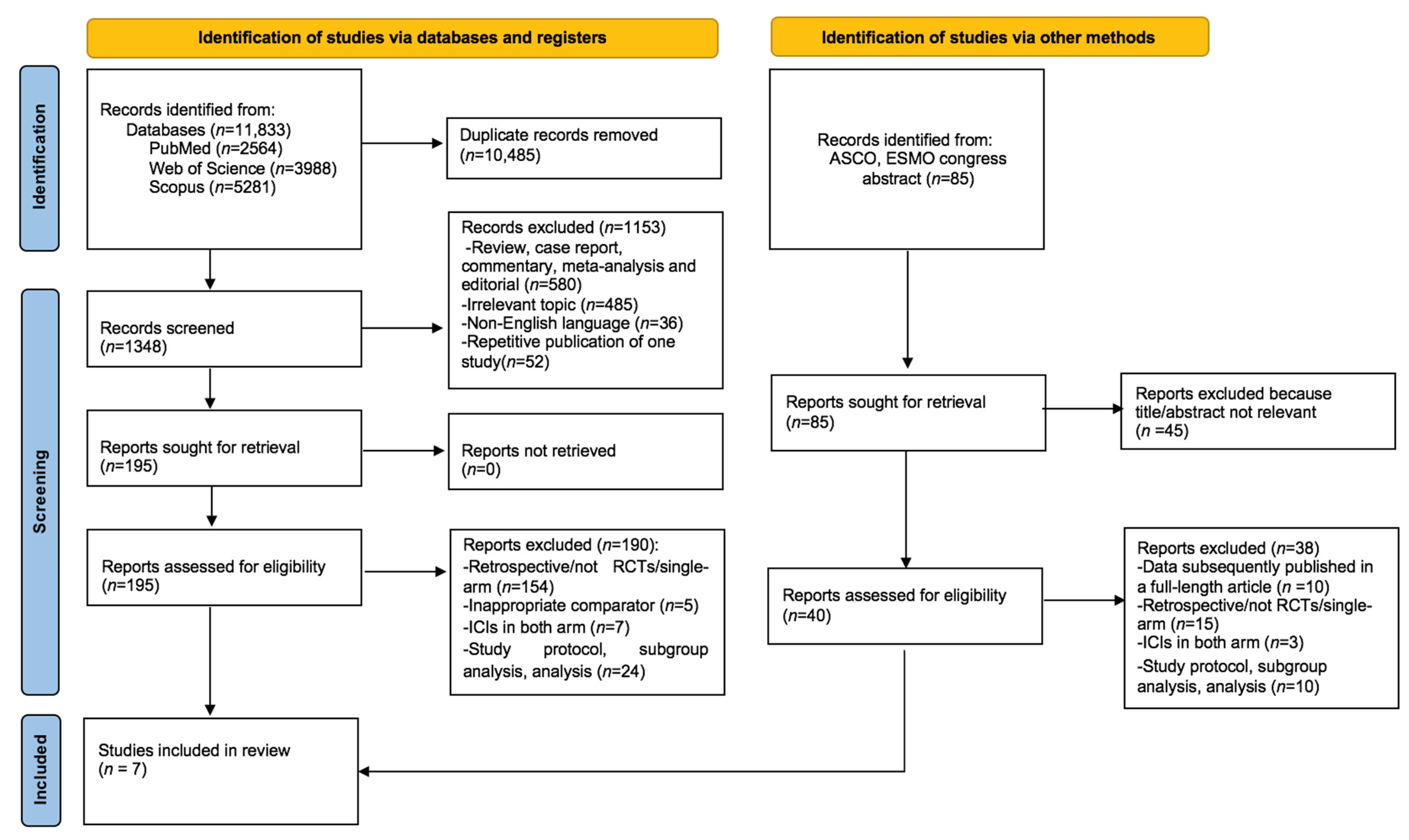
3.1. Study Selection and Baseline Study Characteristics
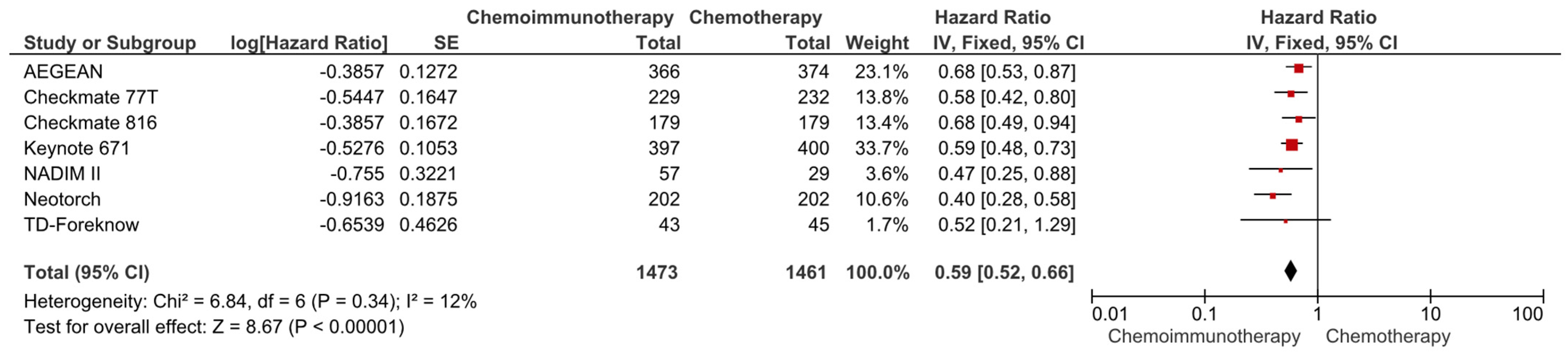
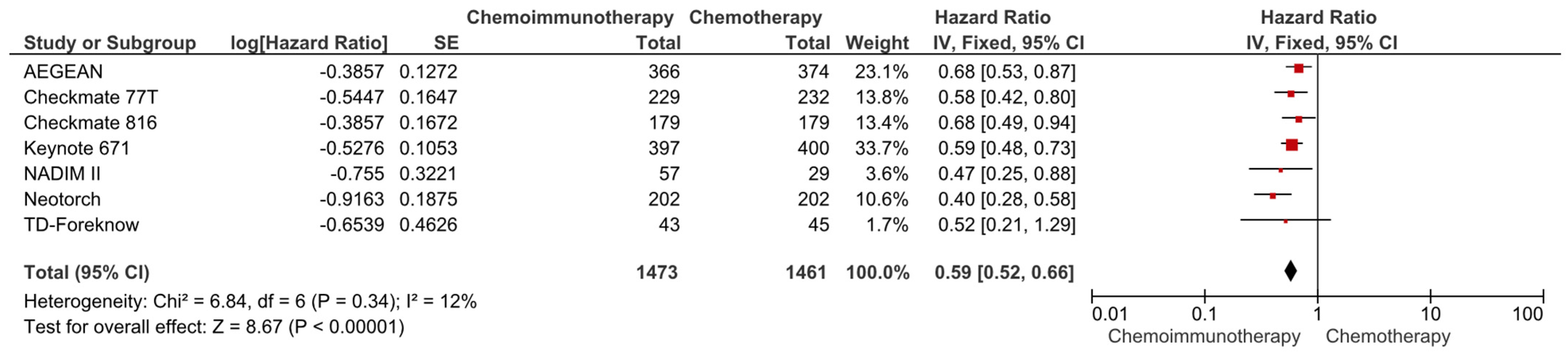
3.2. The Comparison of EFS and OS with Chemoimmunotherapy versus Chemotherapy
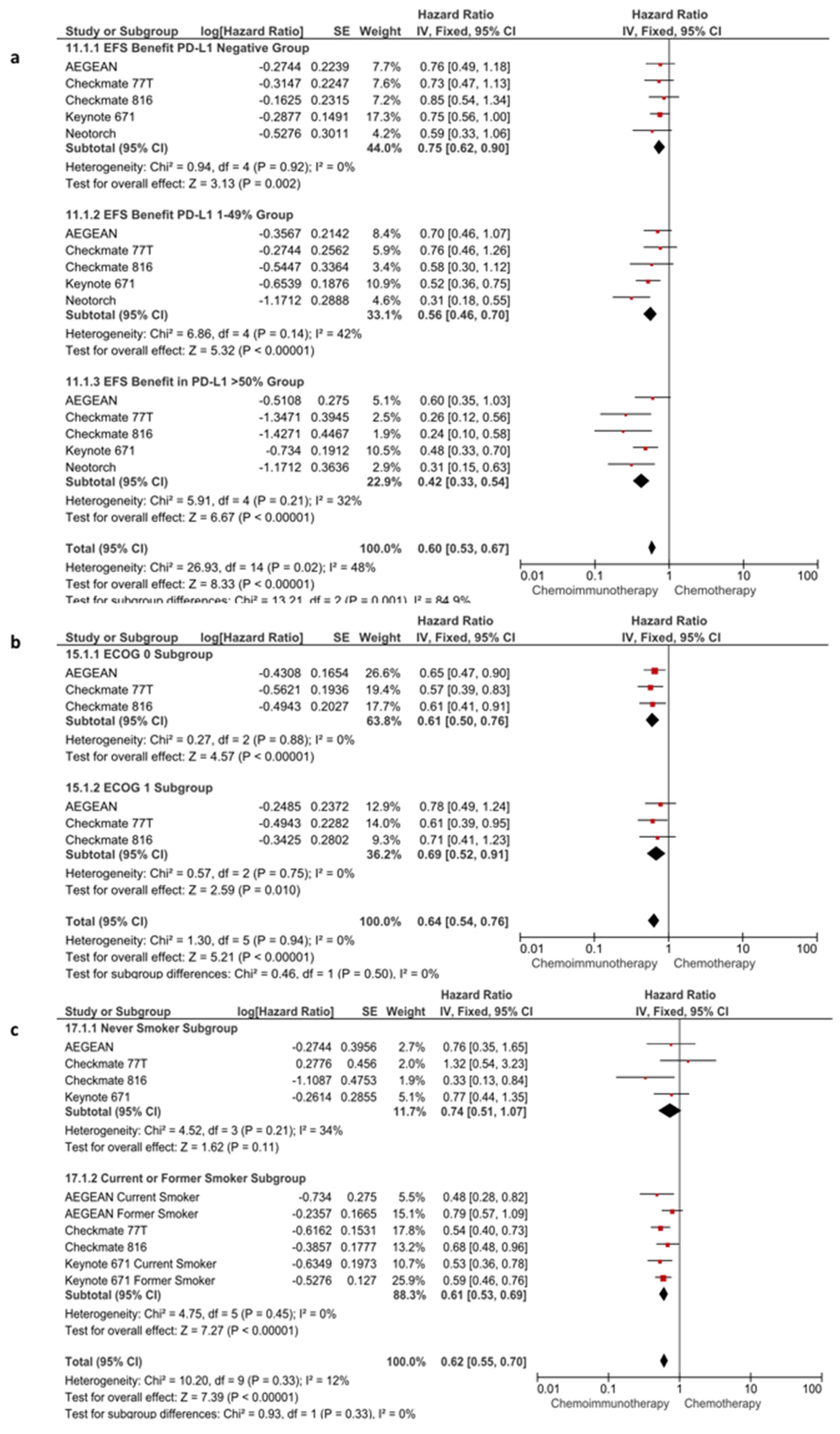
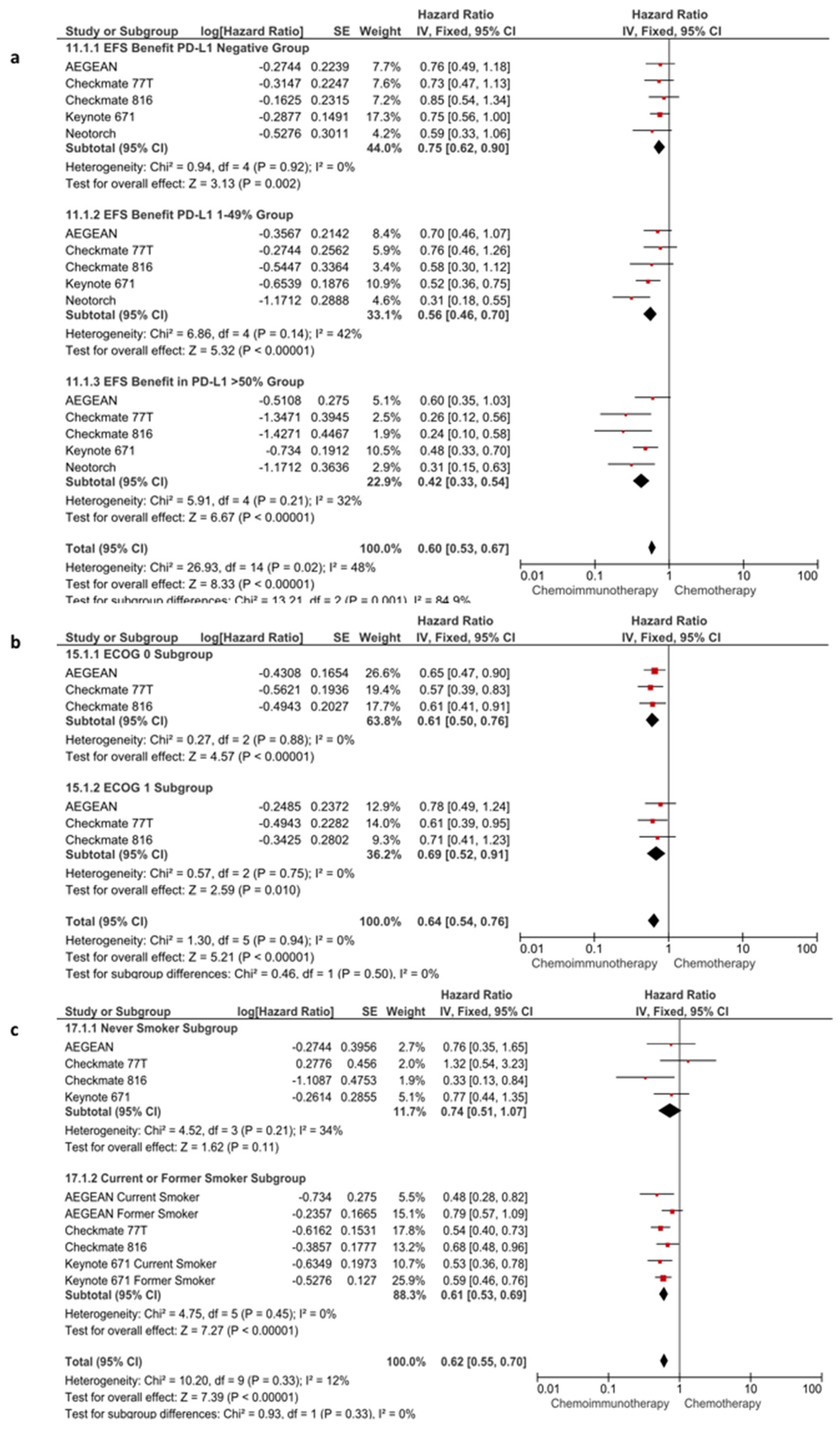
3.3. Subgroup Analyses for EFS
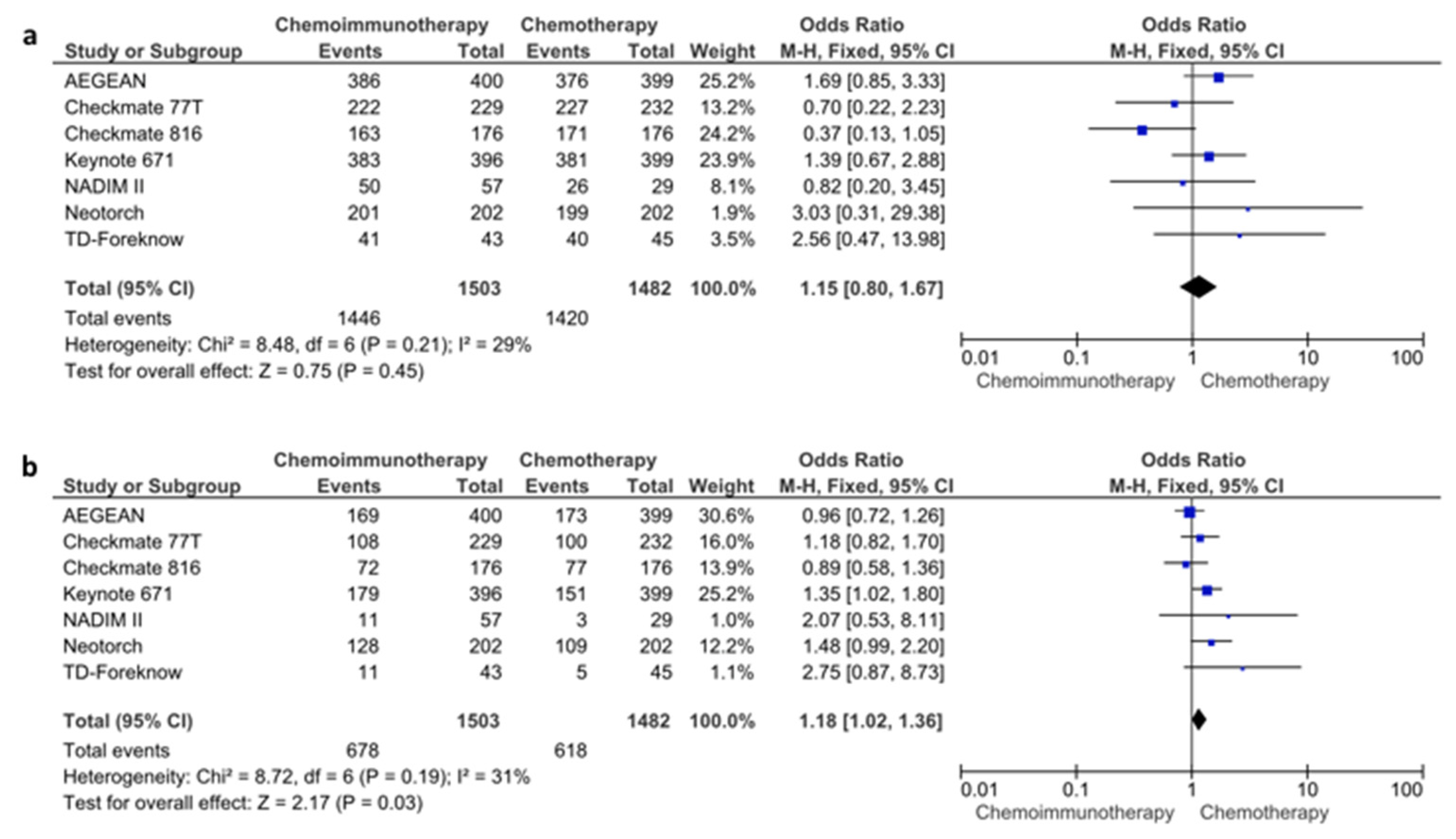
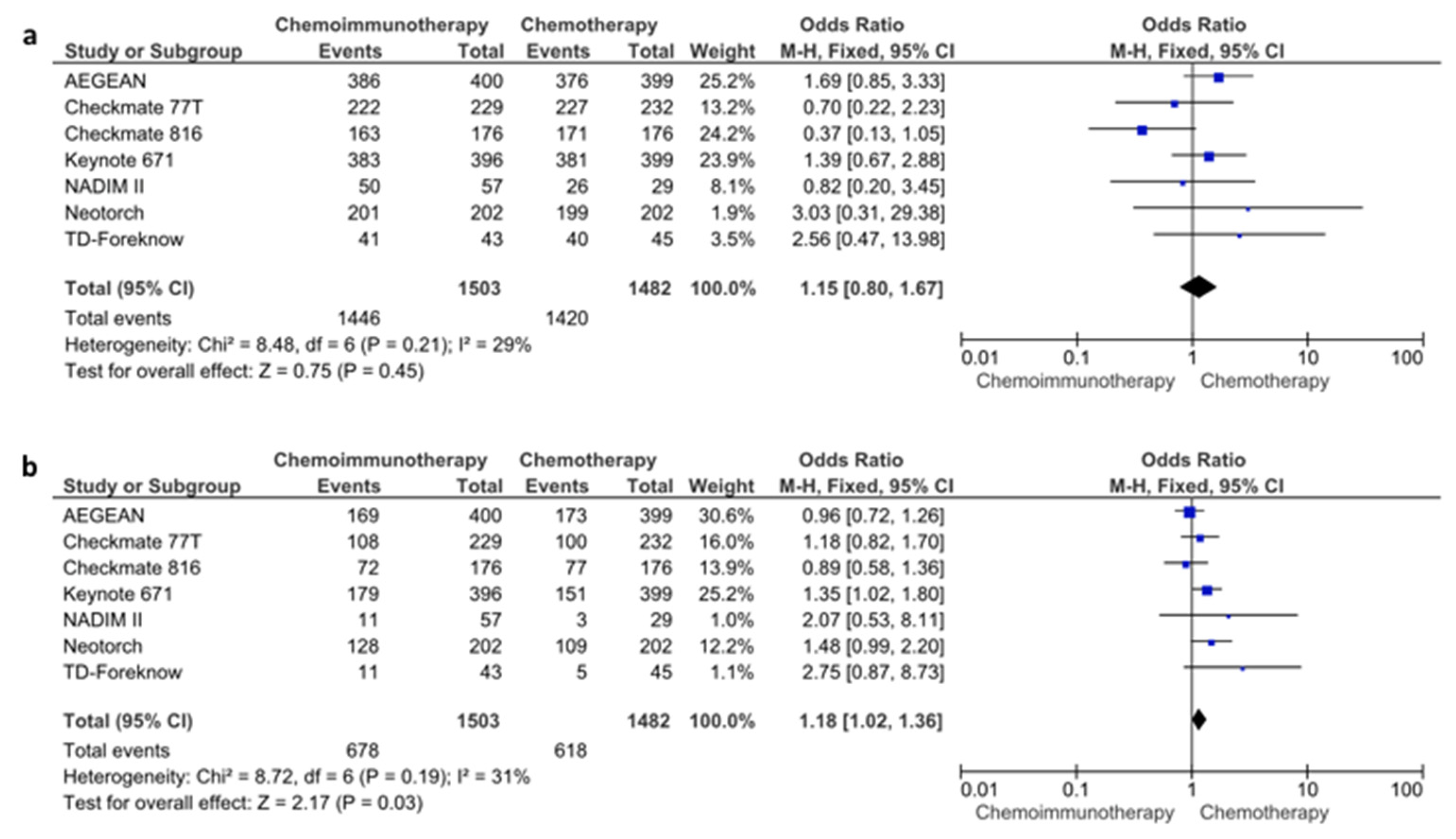
3.4. The Comparison of Pathological Complete Response, R0 Resection Rates, and Adverse Events with Chemoimmunotherapy versus Chemotherapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Horn, L.; Mansfield, A.S.; Szczęsna, A.; Havel, L.; Krzakowski, M.; Hochmair, M.J.; Huemer, F.; Losonczy, G.; Johnson, M.L.; Nishio, M.; et al. First-Line Atezolizumab plus Chemotherapy in Extensive-Stage Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2220–2229. [Google Scholar] [CrossRef]
- Garon, E.B.; Hellmann, M.D.; Rizvi, N.A.; Carcereny, E.; Leighl, N.B.; Ahn, M.J.; Eder, J.P.; Balmanoukian, A.S.; Aggarwal, C.; Horn, L.; et al. Five-Year Overall Survival for Patients with Advanced Non-Small-Cell Lung Cancer Treated with Pembrolizumab: Results from the Phase I KEYNOTE-001 Study. J. Clin. Oncol. 2019, 37, 2518–2527. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Uramoto, H.; Tanaka, F. Recurrence after surgery in patients with NSCLC. Transl. Lung Cancer Res. 2014, 3, 242–249. [Google Scholar] [CrossRef]
- Pignon, J.P.; Tribodet, H.; Scagliotti, G.V.; Douillard, J.Y.; Shepherd, F.A.; Stephens, R.J.; Dunant, A.; Torri, V.; Rosell, R.; Seymour, L.; et al. Lung adjuvant cisplatin evaluation: A pooled analysis by the LACE Collaborative Group. J. Clin. Oncol. 2008, 26, 3552–3559. [Google Scholar] [CrossRef]
- Preoperative chemotherapy for non-small-cell lung cancer: A systematic review and meta-analysis of individual participant data. Lancet 2014, 383, 1561–1571. [CrossRef]
- Rosner, S.; Liu, C.; Forde, P.M.; Hu, C. Association of Pathologic Complete Response and Long-Term Survival Outcomes among Patients Treated with Neoadjuvant Chemotherapy or Chemoradiotherapy for NSCLC: A Meta-Analysis. JTO Clin. Res. Rep. 2022, 3, 100384. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- Dafni, U.; Tsourti, Z.; Vervita, K.; Peters, S. Immune checkpoint inhibitors, alone or in combination with chemotherapy, as first-line treatment for advanced non-small cell lung cancer. A systematic review and network meta-analysis. Lung Cancer 2019, 134, 127–140. [Google Scholar] [CrossRef]
- West, H.; McCleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, H.J.; Kopp, H.G.; Daniel, D.; McCune, S.; Mekhail, T.; et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef]
- Forde, P.M.; Chaft, J.E.; Smith, K.N.; Anagnostou, V.; Cottrell, T.R.; Hellmann, M.D.; Zahurak, M.; Yang, S.C.; Jones, D.R.; Broderick, S.; et al. Neoadjuvant PD-1 Blockade in Resectable Lung Cancer. N. Engl. J. Med. 2018, 378, 1976–1986. [Google Scholar] [CrossRef] [PubMed]
- Uprety, D.; Mandrekar, S.J.; Wigle, D.; Roden, A.C.; Adjei, A.A. Neoadjuvant Immunotherapy for NSCLC: Current Concepts and Future Approaches. J. Thorac. Oncol. 2020, 15, 1281–1297. [Google Scholar] [CrossRef]
- Chaft, J.E.; Oezkan, F.; Kris, M.G.; Bunn, P.A.; Wistuba, I.I.; Kwiatkowski, D.J.; Owen, D.H.; Tang, Y.; Johnson, B.E.; Lee, J.M. Neoadjuvant atezolizumab for resectable non-small cell lung cancer: An open-label, single-arm phase II trial. Nat. Med. 2022, 28, 2155–2161. [Google Scholar] [CrossRef] [PubMed]
- Provencio, M.; Serna-Blasco, R.; Nadal, E.; Insa, A.; García-Campelo, M.R.; Rubio, J.C.; Dómine, M.; Majem, M.; Rodríguez-Abreu, D.; Martínez-Martí, A. Overall survival and biomarker analysis of neoadjuvant nivolumab plus chemotherapy in operable stage IIIA non–small-cell lung cancer (NADIM phase II trial). J. Clin. Oncol. 2022, 40, 2924. [Google Scholar] [CrossRef] [PubMed]
- Forde, P.M.; Spicer, J.; Lu, S.; Provencio, M.; Mitsudomi, T.; Awad, M.M.; Felip, E.; Broderick, S.R.; Brahmer, J.R.; Swanson, S.J.; et al. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer. N. Engl. J. Med. 2022, 386, 1973–1985. [Google Scholar] [CrossRef] [PubMed]
- Heymach, J.V.; Harpole, D.; Mitsudomi, T.; Taube, J.M.; Galffy, G.; Hochmair, M.; Winder, T.; Zukov, R.; Garbaos, G.; Gao, S.; et al. Abstract CT005: AEGEAN: A phase 3 trial of neoadjuvant durvalumab + chemotherapy followed by adjuvant durvalumab in patients with resectable NSCLC. Cancer Res. 2023, 83, CT005. [Google Scholar] [CrossRef]
- Lei, J.; Zhao, J.; Gong, L.; Ni, Y.; Zhou, Y.; Tian, F.; Liu, H.; Gu, Z.; Huang, L.; Lu, Q.; et al. Neoadjuvant Camrelizumab Plus Platinum-Based Chemotherapy vs Chemotherapy Alone for Chinese Patients with Resectable Stage IIIA or IIIB (T3N2) Non–Small Cell Lung Cancer: The TD-FOREKNOW Randomized Clinical Trial. JAMA Oncol. 2023, 9, 1348. [Google Scholar] [CrossRef]
- Provencio, M.; Nadal, E.; González-Larriba, J.L.; Martínez-Martí, A.; Bernabé, R.; Bosch-Barrera, J.; Casal-Rubio, J.; Calvo, V.; Insa, A.; Ponce, S.; et al. Perioperative Nivolumab and Chemotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2023, 389, 504–513. [Google Scholar] [CrossRef]
- Wakelee, H.; Liberman, M.; Kato, T.; Tsuboi, M.; Lee, S.H.; Gao, S.; Chen, K.N.; Dooms, C.; Majem, M.; Eigendorff, E.; et al. Perioperative Pembrolizumab for Early-Stage Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2023, 389, 491–503. [Google Scholar] [CrossRef]
- Lu, S.; Wu, L.; Zhang, W.; Zhang, P.; Wang, W.; Fang, W.; Xing, W.; Chen, Q.; Mei, J.; Yang, L.; et al. Perioperative toripalimab + platinum-doublet chemotherapy vs chemotherapy in resectable stage II/III non-small cell lung cancer (NSCLC): Interim event-free survival (EFS) analysis of the phase III Neotorch study. J. Clin. Oncol. 2023, 41, 425126. [Google Scholar] [CrossRef]
- Cascone, T.; Awad, M.M.; Spicer, J.D.; He, J.; Lu, S.; Sepesi, B.; Tanaka, F.; Taube, J.M.; Cornelissen, R.; Havel, L.; et al. LBA1 CheckMate 77T: Phase III study comparing neoadjuvant nivolumab (NIVO) plus chemotherapy (chemo) vs neoadjuvant placebo plus chemo followed by surgery and adjuvant NIVO or placebo for previously untreated, resectable stage II–IIIb NSCLC. Ann. Oncol. 2023, 34, S1295. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, G.M.; Bunn, P.A.; Chaft, J.E.; McCoach, C.E.; Perez, E.A.; Scagliotti, G.V.; Carbone, D.P.; Aerts, H.J.W.L.; Aisner, D.L.; Bergh, J.; et al. Current Status and Future Perspectives on Neoadjuvant Therapy in Lung Cancer. J. Thorac. Oncol. 2018, 13, 1818–1831. [Google Scholar] [CrossRef]
- Kasimir-Bauer, S.; Bittner, A.-K.; König, L.; Reiter, K.; Keller, T.; Kimmig, R.; Hoffmann, O. Does primary neoadjuvant systemic therapy eradicate minimal residual disease? Analysis of disseminated and circulating tumor cells before and after therapy. Breast Cancer Res. 2016, 18, 20. [Google Scholar] [CrossRef] [PubMed]
- Imyanitov, E.N.; Yanus, G.A. Neoadjuvant therapy: Theoretical, biological and medical consideration. Chin. Clin. Oncol. 2018, 7, 55. [Google Scholar] [CrossRef] [PubMed]
- Korde, L.A.; Somerfield, M.R.; Carey, L.A.; Crews, J.R.; Denduluri, N.; Hwang, E.S.; Khan, S.A.; Loibl, S.; Morris, E.A.; Perez, A.; et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J. Clin. Oncol. 2021, 39, 1485–1505. [Google Scholar] [CrossRef] [PubMed]
- Junior, P.U.; e Silva, D.D.; de Castro, N.; Victor, E.d.S.; Rother, E.; Araújo, S.; Borad, M.; Moura, F. Does neoadjuvant treatment in resectable pancreatic cancer improve overall survival? A systematic review and meta-analysis of randomized controlled trials. ESMO Open 2023, 8, 100771. [Google Scholar] [CrossRef] [PubMed]
- Spring, L.M.; Fell, G.; Arfe, A.; Sharma, C.; Greenup, R.; Reynolds, K.L.; Smith, B.L.; Alexander, B.; Moy, B.; Isakoff, S.J.; et al. Pathologic Complete Response after Neoadjuvant Chemotherapy and Impact on Breast Cancer Recurrence and Survival: A Comprehensive Meta-analysis. Clin. Cancer Res. 2020, 26, 2838–2848. [Google Scholar] [CrossRef]
- Huober, J.; van Mackelenbergh, M.; Schneeweiss, A.; Seither, F.; Blohmer, J.-U.; Denkert, C.; Tesch, H.; Hanusch, C.; Salat, C.; Rhiem, K.; et al. Identifying breast cancer patients at risk of relapse despite pathological complete response after neoadjuvant therapy. NPJ Breast Cancer 2023, 9, 23. [Google Scholar] [CrossRef]
- Herbst, R.S.; Sznol, M. Diminished but not dead: Chemotherapy for the treatment of NSCLC. Lancet Oncol. 2016, 17, 1464–1465. [Google Scholar] [CrossRef]
- Doroshow, D.B.; Sanmamed, M.F.; Hastings, K.; Politi, K.; Rimm, D.L.; Chen, L.; Melero, I.; Schalper, K.A.; Herbst, R.S. Immunotherapy in non–small cell lung cancer: Facts and hopes. Clin. Cancer Res. 2019, 25, 4592–4602. [Google Scholar] [CrossRef] [PubMed]
- Luo, Q.; Zhang, L.; Luo, C.; Jiang, M. Emerging strategies in cancer therapy combining chemotherapy with immunotherapy. Cancer Lett. 2019, 454, 191–203. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.G.; Ramalingam, S.S.; Ciuleanu, T.E.; Lee, J.S.; Urban, L.; Caro, R.B.; Park, K.; Sakai, H.; Ohe, Y.; Nishio, M.; et al. First-Line Nivolumab Plus Ipilimumab in Advanced NSCLC: 4-Year Outcomes from the Randomized, Open-Label, Phase 3 CheckMate 227 Part 1 Trial. J. Thorac. Oncol. 2022, 17, 289–308. [Google Scholar] [CrossRef] [PubMed]
- Garassino, M.C.; Gadgeel, S.; Speranza, G.; Felip, E.; Esteban, E.; Dómine, M.; Hochmair, M.J.; Powell, S.F.; Bischoff, H.G.; Peled, N.; et al. Pembrolizumab Plus Pemetrexed and Platinum in Nonsquamous Non-Small-Cell Lung Cancer: 5-Year Outcomes from the Phase 3 KEYNOTE-189 Study. J. Clin. Oncol. 2023, 41, 1992–1998. [Google Scholar] [CrossRef] [PubMed]
- Felip, E.; Altorki, N.; Zhou, C.; Csőszi, T.; Vynnychenko, I.; Goloborodko, O.; Luft, A.; Akopov, A.; Martinez-Marti, A.; Kenmotsu, H.; et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): A randomised, multicentre, open-label, phase 3 trial. Lancet 2021, 398, 1344–1357. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.; Paz-Ares, L.; Marreaud, S.; Dafni, U.; Oselin, K.; Havel, L.; Esteban, E.; Isla, D.; Martinez-Marti, A.; Faehling, M.; et al. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB-IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): An interim analysis of a randomised, triple-blind, phase 3 trial. Lancet Oncol. 2022, 23, 1274–1286. [Google Scholar] [CrossRef] [PubMed]
- Guven, D.C.; Sahin, T.K.; Dizdar, O.; Kilickap, S. Predictive biomarkers for immunotherapy efficacy in non-small-cell lung cancer: Current status and future perspectives. Biomark. Med. 2020, 14, 1383–1392. [Google Scholar] [CrossRef]
- Zhao, X.; Bao, Y.; Meng, B.; Xu, Z.; Li, S.; Wang, X.; Hou, R.; Ma, W.; Liu, D.; Zheng, J.; et al. From rough to precise: PD-L1 evaluation for predicting the efficacy of PD-1/PD-L1 blockades. Front. Immunol. 2022, 13, 920021. [Google Scholar] [CrossRef]
- Cascone, T.; Leung, C.H.; Weissferdt, A.; Pataer, A.; Carter, B.W.; Godoy, M.C.B.; Feldman, H.; William, W.N.; Xi, Y.; Basu, S.; et al. Neoadjuvant chemotherapy plus nivolumab with or without ipilimumab in operable non-small cell lung cancer: The phase 2 platform NEOSTAR trial. Nat. Med. 2023, 29, 593–604. [Google Scholar] [CrossRef]
- Bahce, I.; Dickhoff, C.; Schneiders, F.L.; Veltman, J.; Heineman, D.J.; Hashemi, S.; Fransen, M.; Vrijmoet, A.; Houda, I.; Ulas, E.; et al. 950O Ipilimumab plus nivolumab and chemoradiotherapy followed by surgery in patients with resectable and borderline resectable lung cancer: The INCREASE trial. Ann. Oncol. 2022, 33, S982. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): An international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trial Name, Year | Phase | Clinical Stage | Total Number of Patients | Study Design | Experimental Arm (n) | Control Arm (n) | Surgical Resection Rate | R0 Resection | pCR, No./Total No. (%) | OS (Median or %) | EFS/DFS/PFS (Median or % | Grade ≥ 3 TRAEs, (%) | Fatal AEs, No. | Median Follow-Up (Months) | Additional Comments |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CheckMate 816, 2022 [15] | III | IB-IIIA | 358 | Neoadjuvant only | Nivolumab + Chemotherapy (179) | Chemotherapy (179) (NSQ: pemetrexed + cisplatin/paclitaxel + carboplatin, SQ: gemcitabine + sisplatin/paclitaxel + carboplatin) | 83.2% vs. 75.4% | 83.2% vs. 77.8% | 43/179 (24) vs. 4/179 (2.2) | NR | 31.6 vs. 20.8 months (median) | 33.5 vs. 36.9 | 0 vs. 3 | 29.5 | No additional ICI in the adjuvant setting |
| NADIM II, 2023 [18] | II | IIIA-IIIB | 86 | Neoadjuvant plus adjuvant | Nivolumab + Chemotherapy (57) | Chemotherapy (29) (paclitaxel + carboplatin) | 96.2% vs. 100% | 94.3% vs. 85.0% | 21/57(37) vs. 2/29 (7) | 1 year (98.2 vs. 82.1) | 1 year PFS (89.5 vs. 58.6) | 19 vs. 10 | 1 vs. 0 | 26.1 | The ICIs were continued for six months for the adjuvant setting in the experimental arm |
| KEYNOTE-671, 2023 [19] | III | II-IIIB | 797 | Neoadjuvant plus adjuvant | Pembrolizumab + Chemotherapy (397) | Chemotherapy (400) (NSQ: cisplatin + pemetrexed, SQ: cisplatin + gemcitabine) | 98.5% vs. 95.3% | 92% vs. 84.2% | 72/397 (18.1) vs. 16/400 (4) | 3 year (71.3 vs. 64.0) 4 years (67.1 vs. 51.5) | 3 year EFS (54.3 vs. 35.4) 4 year EFS (48.4 vs. 26.2) | 45.2 vs. 37.8 | 1 vs. 0 | 36.6 | All patients treated with cisplatin-based combinations, requiring cisplatin eligibility for trial enrollment |
| TD-FOREKNOW, 2023 [17] | II | IIIA-IIIB | 88 | Neoadjuvant only | Camrelizumab + Chemotherapy (43) | Chemotherapy (45) (nab-paclitaxel plus cisplatin, carboplatin or nedaplatin) | 93% vs. 93.3% | 92.5% vs. 85.7% | 14/43 (32.6) vs. 4/45 (8.9) | NR | 1 year EFS (93.0 vs. 76.9) 2 year EFS (76.9 vs. 67.6) | 25.6 vs. 11.1 | 0 vs. 0 | 14.1 | The primary endpoint was the pCR rate. The EFS was a secondary endpoint. No treatment in the adjuvant setting |
| AEGEAN, 2023 [16] | III | II-IIIB | 799 | Neoadjuvant plus adjuvant | Durvalumab + Chemotherapy (400) | Chemotherapy (399) (NSQ: pemetrexed + cisplatin or carboplatin, SQ: carboplatin + paclitaxel/gemcitabine + cisplatin or carboplatin) | 80.6% vs. 80.7% | 94.7% vs. 91.3% | 63/366 (17.2) vs. 16/374 (4.3) | NR | 1 year EFS (73.4 vs. 64.5) | 32.3 vs. 33.1 | 7 vs. 2 | 11.7 m0 | - |
| Neotorch, 2023 [20] | III | II-III | 404 | Neoadjuvant plus adjuvant | Toripalimab + Chemotherapy (202) | Chemotherapy (202) | 82.2% vs. 73.3% | 95.8% vs. 92.6% | 50/202 (24.8) vs. 2/202 (1) | 1 year (94.4 vs. 89.6) | 1 year EFS (84.4 vs. 57.0) | 63.4 vs. 54.0 | 0 vs. 2 | 18.25 mo | Included patients with multi-station N2 disease, 33 and 31% of the patients in the experimental and control arms had multi-station N2 disease, respectively |
| CheckMate 77T, 2023 [21] | III | IIA-IIIB | 461 | Neoadjuvant plus adjuvant | Nivolumab + Chemotherapy (229) | Chemotherapy (232) (NSQ: pemetrexed + cisplatin or carboplatin/carboplatin + paclitaxel, SQ: cisplatin + docetaxel/ carboplatin + paclitaxel) | 78% vs. 77% | 89% vs. 90% | 58/229 (25.3) vs. 11/232 (4.7) | NR | 1 year EFS (73 vs. 59) | 27.0 vs. 23.0 | 2 vs. 0 | 25.4 | Included patients with multi-station N2 disease and had separate subgroup data for these patients |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guven, D.C.; Sahin, T.K.; Kilickap, S. The Efficacy and Safety of Neoadjuvant Immunotherapy in Patients with Non-Small Cell Lung Cancer. Cancers 2024, 16, 156. https://doi.org/10.3390/cancers16010156
Guven DC, Sahin TK, Kilickap S. The Efficacy and Safety of Neoadjuvant Immunotherapy in Patients with Non-Small Cell Lung Cancer. Cancers. 2024; 16(1):156. https://doi.org/10.3390/cancers16010156
Chicago/Turabian StyleGuven, Deniz Can, Taha Koray Sahin, and Saadettin Kilickap. 2024. "The Efficacy and Safety of Neoadjuvant Immunotherapy in Patients with Non-Small Cell Lung Cancer" Cancers 16, no. 1: 156. https://doi.org/10.3390/cancers16010156
APA StyleGuven, D. C., Sahin, T. K., & Kilickap, S. (2024). The Efficacy and Safety of Neoadjuvant Immunotherapy in Patients with Non-Small Cell Lung Cancer. Cancers, 16(1), 156. https://doi.org/10.3390/cancers16010156