
Diagnostic and Prognostic Roles of Urine Nectin-2 and Nectin-4 in Human Bladder Cancer

 , , , ,
, , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patient Selection and Data Collection
2.2. Processing of Voided Urine and Serum Samples
2.3. Measurement of Nectins in Urine and Serum
2.4. Immunohistochemical (IHC) Staining Analysis of Tumor Expression of Nectins
2.5. Statistical Analysis
3. Results
3.1. Levels of Urine Nectin-2 and Nectin-4
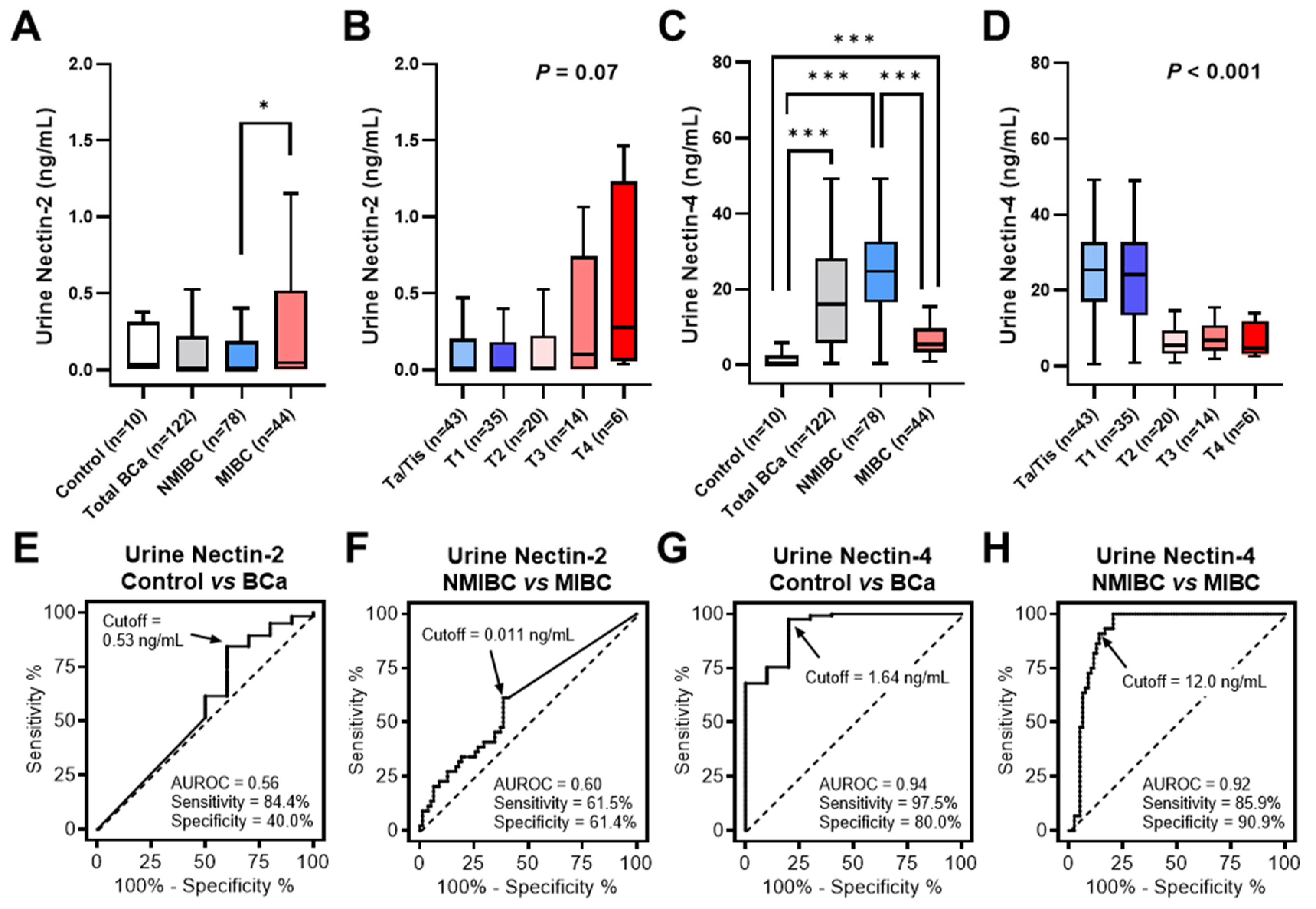
3.2. Diagnostic Performance of Urine Nectin-2 and Nectin-4
3.3. Prognostic Performance of Urine Nectin-2 and Nectin-4
3.4. Correlation among Urine Nectins, Serum Nectins, and Tumor Nectins in MIBC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miyake, M.; Owari, T.; Hori, S.; Nakai, Y.; Fujimoto, K. Emerging biomarkers for the diagnosis and monitoring of urothelial carcinoma. Res. Rep. Urol. 2018, 10, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Rosenberg, J.E.; Sonpavde, G.P.; Loriot, Y.; Durán, I.; Lee, J.L.; Matsubara, N.; Vulsteke, C.; Castellano, D.; Wu, C.; et al. Enfortumab Vedotin in Previously Treated Advanced Urothelial Carcinoma. N. Engl. J. Med. 2021, 384, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Challita-Eid, P.M.; Satpayev, D.; Yang, P.; An, Z.; Morrison, K.; Shostak, Y.; Raitano, A.; Nadell, R.; Liu, W.; Lortie, D.R.; et al. Enfortumab vedotin antibody-drug conjugate targeting nectin-4 is a highly potent therapeutic agent in multiple preclinical cancer models. Cancer Res. 2016, 76, 3003–3013. [Google Scholar] [CrossRef] [PubMed]
- Takai, Y.; Miyoshi, J.; Ikeda, W.; Ogita, H. Nectins andnectin-like molecules: Roles in contact inhibition of cell movement and proliferation. Nat. Rev. Mol. Cell Biol. 2008, 9, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Sakisaka, T.; Ikeda, W.; Ogita, H.; Fujita, N.; Takai, Y. The roles of nectins in cell adhesions: Cooperation with other cell adhesion molecules and growthf actor receptors. Curr. Opin. Cell Biol. 2007, 19, 593–602. [Google Scholar] [CrossRef]
- Yamada, A.; Fujita, N.; Sato, T.; Okamoto, R.; Ooshio, T.; Hirota, T.; Morimoto, K.; Irie, K.; Takai, Y. Requirement of nectin, but not cadherin, for formation of claudin-based tight junctions in annexin II-knockdown MDCK cells. Oncogene 2006, 25, 5085–5102. [Google Scholar] [CrossRef]
- Nakanishi, H.; Takai, Y. Roles of nectins in cell adhesion, migration and polarization. Biol. Chem. 2004, 385, 885–892. [Google Scholar] [CrossRef]
- Reymond, N.; Fabre, S.; Lecocq, E.; Adelaïde, J.; Dubreuil, P.; Lopez, M. Nectin4/PRR4, a new afadin-associated member of the nectin family that trans-interacts with nectin1/PRR1 through V domain interaction. J. Biol. Chem. 2001, 276, 43205–43215. [Google Scholar] [CrossRef]
- Fabre, S.; Reymond, N.; Cocchi, F.; Menotti, L.; Dubreuil, P.; Campadelli-Fiume, G.; Lopez, M. Prominent role of the Ig-like V domain in trans-interactions of nectins. Nectin3 and nectin4 bind to the predicted C-C’-C’’-D beta-strands of the nectin1 V domain. J. Biol. Chem. 2002, 277, 27006–27013. [Google Scholar] [CrossRef]
- Derycke, M.S.; Pambuccian, S.E.; Gilks, C.B.; Kalloger, S.E.; Ghidouche, A.; Lopez, M.; Bliss, R.L.; Geller, M.A.; Argenta, P.A.; Harrington, K.M.; et al. Nectin 4 overexpression in ovarian cancer tissues and serum: Potential role as a serum biomarker. Am. J. Clin. Pathol. 2010, 134, 835–845. [Google Scholar] [CrossRef]
- Rogmans, C.; Feuerborn, J.; Treeck, L.; Tribian, N.; Flörkemeier, I.; Arnold, N.; Weimer, J.P.; Maass, N.; Jansen, P.; Lieb, W.; et al. Nectin-4 as Blood-Based Biomarker Enables Detection of Early Ovarian Cancer Stages. Cancers 2022, 14, 5867. [Google Scholar] [CrossRef] [PubMed]
- Fabre-Lafay, S.; Monville, F.; Garrido-Urbani, S.; Berruyer-Pouyet, C.; Ginestier, C.; Reymond, N.; Finetti, P.; Sauvan, R.; Adélaïde, J.; Geneix, J.; et al. Nectin-4 is a new histological and serological tumor associated marker for breast cancer. BMC Cancer 2007, 7, 73. [Google Scholar] [CrossRef] [PubMed]
- Takano, A.; Ishikawa, N.; Nishino, R.; Masuda, K.; Yasui, W.; Inai, K.; Nishimura, H.; Ito, H.; Nakayama, H.; Miyagi, Y.; et al. Identification of nectin-4 oncoprotein as a diagnostic and therapeutic target for lung cancer. Cancer Res. 2009, 69, 6694–6703. [Google Scholar] [CrossRef]
- Erturk, K.; Karaman, S.; Dagoglu, N.; Serilmez, M.; Duranyildiz, D.; Tas, F. Serum nectin-2 and nectin-4 are diagnostic in lung cancer: Which is superior? Wien. Klin. Wochenschr. 2019, 131, 419–426. [Google Scholar] [CrossRef]
- Karabulut, M.; Gunaldi, M.; Alis, H.; Afsar, C.U.; Karabulut, S.; Serilmez, M.; Akarsu, C.; Seyit, H.; Aykan, N.F. Serum nectin-2 levels are diagnostic and prognostic in patients with colorectal carcinoma. Clin. Transl. Oncol. 2016, 18, 160–171. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.; Miyamoto, T.; Shimizu, T.; Ohnishi, S.; Fujii, T.; Nishimura, N.; Oda, Y.; Morizawa, Y.; Hori, S.; Gotoh, D.; et al. Tumor expression of Nectin-1-4 and its clinical implication in muscle invasive bladder cancer: An intra-patient variability of Nectin-4 expression. Pathol. Res. Pract. 2022, 237, 154072. [Google Scholar] [CrossRef]
- Miyake, M.; Gotoh, D.; Shimada, K.; Tatsumi, Y.; Nakai, Y.; Anai, S.; Torimoto, K.; Aoki, K.; Tanaka, N.; Konishi, N.; et al. Exploration of risk factors predicting outcomes for primary T1 high-grade bladder cancer and validation of the Spanish Urological Club for Oncological Treatment scoring model: Long-term follow-up experience at a single institute. Int. J. Urol. 2015, 22, 541–547. [Google Scholar] [CrossRef]
- Morizawa, Y.; Miyake, M.; Shimada, K.; Hori, S.; Tatsumi, Y.; Nakai, Y.; Anai, S.; Tanaka, N.; Konishi, N.; Fujimoto, K. Neutrophil-to-lymphocyte ratio as a detection marker of tumor recurrence in patients with muscle-invasive bladder cancer after radical cystectomy. Urol. Oncol. 2016, 34, 257.e11–257.e17. [Google Scholar] [CrossRef]
- Papanicolaou, G.N.; Marshall, V.F. Urine sediment smears as a diagnostic procedure in cancers of the urinary tract. Science 1945, 101, 519–520. [Google Scholar] [CrossRef]
- Landman, J.; Chang, Y.; Kavaler, E.; Droller, M.J.; Liu, B.C. Sensitivity and specificity of NMP-22, telomerase, and BTA in the detection of human bladder cancer. Urology 1998, 52, 398–402. [Google Scholar] [CrossRef]
- Sözen, S.; Biri, H.; Sinik, Z.; Küpeli, B.; Alkibay, T.; Bozkirli, I. Comparison of the nuclear matrix protein 22 with voided urine cytology and BTA stat test in the diagnosis of transitional cell carcinoma of the bladder. Eur. Urol. 1999, 36, 225–229. [Google Scholar] [PubMed]
- Miyake, M.; Goodison, S.; Giacoia, E.G.; Rizwani, W.; Ross, S.; Rosser, C.J. Influencing factors on the NMP-22 urine assay: An experimental model. BMC Urol. 2012, 12, 23. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.; Morizawa, Y.; Hori, S.; Tatsumi, Y.; Onishi, S.; Owari, T.; Iida, K.; Onishi, K.; Gotoh, D.; Nakai, Y.; et al. Diagnostic and prognostic role of urinary collagens in primary human bladder cancer. Cancer Sci. 2017, 108, 2221–2228. [Google Scholar] [CrossRef] [PubMed]
- Drago, J.Z.; Modi, S.; Chandarlapaty, S. Unlocking the potential of antibody-drug conjugates for cancer therapy. Nat. Rev. Clin. Oncol. 2021, 18, 327–344. [Google Scholar] [CrossRef]
- Chu, C.E.; Sjöström, M.; Egusa, E.A.; Gibb, E.A.; Badura, M.L.; Zhu, J.; Koshkin, V.S.; Stohr, B.A.; Meng, M.V.; Pruthi, R.S.; et al. Heterogeneity in NECTIN4 Expression Across Molecular Subtypes of Urothelial Cancer Mediates Sensitivity to Enfortumab Vedotin. Clin. Cancer. Res. 2021, 27, 5123–5130. [Google Scholar] [CrossRef]
- Nagai, T.; Naiki, T.; Etani, T.; Iida, K.; Noda, Y.; Shimizu, N.; Isobe, T.; Nozaki, S.; Okamura, T.; Ando, R.; et al. UroVysion fluorescence in situ hybridization in urothelial carcinoma: A narrative review and future perspectives. Transl. Androl. Urol. 2021, 10, 1908–1917. [Google Scholar] [CrossRef]
- Laukhtina, E.; Shim, S.R.; Mori, K.; D’Andrea, D.; Soria, F.; Rajwa, P.; Mostafaei, H.; Compérat, E.; Cimadamore, A.; Moschini, M.; et al. Diagnostic Accuracy of Novel Urinary Biomarker Tests in Non-muscle-invasive Bladder Cancer: A Systematic Review and Network Meta-analysis. Eur. Urol. Oncol. 2021, 4, 927–942. [Google Scholar] [CrossRef]
- Soorojebally, Y.; Neuzillet, Y.; Roumiguié, M.; Lamy, P.J.; Allory, Y.; Descotes, F.; Ferlicot, S.; Kassab-Chahmi, D.; Oudard, S.; Rébillard, X.; et al. Urinary biomarkers for bladder cancer diagnosis and NMIBC follow-up: A systematic review. World J. Urol. 2023, 41, 345–359. [Google Scholar] [CrossRef]
- Koya, M.; Osborne, S.; Chemaslé, C.; Porten, S.; Schuckman, A.; Kennedy-Smith, A. An evaluation of the real-world use and clinical utility of the Cxbladder Monitor assay in the follow-up of patients previously treated for bladder cancer. BMC Urol. 2020, 20, 12. [Google Scholar] [CrossRef]
- Kavalieris, L.; O’Sullivan, P.; Frampton, C.; Guilford, P.; Darling, D.; Jacobson, E.; Suttie, J.; Raman, J.D.; Shariat, S.F.; Lotan, Y. Performance characteristics of a multigene urine biomarker test for monitoring for recurrent urothelial carcinoma in a multicenter study. J. Urol. 2017, 197, 1419–1426. [Google Scholar] [CrossRef]
- Bouleftour, W.; Guillot, A.; Magne, N. The Anti-Nectin 4: A Promising Tumor Cells Target. A Systematic Review. Mol. Cancer Ther. 2022, 21, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Hoffman-Censits, J.H.; Lombardo, K.A.; Parimi, V.; Kamanda, S.; Choi, W.; Hahn, N.M.; McConkey, D.J.; McGuire, B.M.; Bivalacqua, T.J.; Kates, M.; et al. Expression of nectin-4 in bladder urothelial carcinoma, in morphologic variants, and nonurothelial histotypes. Appl. Immunohistochem. Mol. Morphol. 2021, 29, 619–625. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | No. of Cases | Urine Nectin-2 (ng/mL) | Urine Nectin-4 (ng/mL) | |||||
|---|---|---|---|---|---|---|---|---|
| Median (IQR) | Mean ± SEM | p Value | Median (IQR) | Mean ± SEM | p Value | |||
| No. of cases | 122 (100%) | 0.0 (0.0–0.2) | 0.40 ± 0.13 | - | 16.0 (5.8–28.1) | 18.3 ± 1.2 | - | |
| Sex | Male | 103 (84%) | 0.0 (0.0–0.26) | 0.43 ± 0.15 | 0.99 † | 15.9 (5.5–28.8) | 18.2 ± 1.4 | 0.75 † |
| Female | 19 (16%) | 0.02 (0.0–0.21) | 0.21 ± 0.09 | 16.6 (10.5–26.4) | 18.6 ± 3.0 | |||
| Age | 70 yo or less | 51 (42%) | 0.0 (0.0–0.15) | 0.17 ± 0.05 | 0.052 † | 20.4 (9.6–30.3) | 20.5 ± 1.8 | 0.06 † |
| 71 yo or more | 71 (58%) | 0.04 (0.0–0.40) | 0.56 ± 0.22 | 13.1 (5.2–25.3) | 16.6 ± 1.7 | |||
| Urine cytology | Negative | 61 (50%) | 0.0 (0.0–0.21) | 3.0 ± 0.09 | 0.47 † | 18.5 (8.9–27.4) | 18.7 ± 1.5 | 0.42 † |
| Positive | 61 (50%) | 0.03 (0.0–0.36) | 5.0 ± 0.25 | 12.8 (5.4–29.9) | 17.8 ± 1.9 | |||
| Urine NMP-22 # | Negative (£10 U/mL) | 59 (48%) | 0.0 (0.0–0.15) | 0.18 ± 0.08 | 0.002 † | 17.4 (5.9–27.9) | 18.5 ± 1.7 | 0.72 † |
| Positive (>10 U/mL) | 63 (52%) | 0.06 (0.0–0.53) | 0.60 ± 0.24 | 13.4 (5.7–29.8) | 18.0 ± 1.8 | |||
| Tumor grade (WHO2004) | Low grade | 41 (34%) | 0.0 (0.0–0.21) | 0.26 ± 0.11 | 0.64 † | 0 | 24.0 ± 1.6 | <0.001 † |
| High grade | 81 (66%) | 0.0 (0.0–0.38) | 0.46 ± 0.19 | 9.7 (4.3–24.2) | 15.4 ± 1.6 | |||
| Carcinoma in situ | Absent | 75 (61%) | 0.03 (0.0–0.40) | 0.55 ± 0.21 | 0.03 † | 16.6 (8.2–27.5) | 18.7 ± 1.6 | 0.59 † |
| Present | 47 (39%) | 0.0 (0.0–0.14) | 0.15 ± 0.05 | 10.5 (5.4–30.3) | 17.5 ± 2.0 | |||
| Clinical T category ## | Ta/Tis | 43 (35%) | 0.0 (0.0–0.20) | 0.25 ± 0.11 | 0.07 ‡ | 25.3 (16.9–32.7) | 24.9 ± 1.8 | <0.001 ‡ |
| T1 | 35 (29%) | 0.0 (0.0–0.18) | 0.19 ± 0.07 | 24.1 (13.4–32.7) | 24.9 ± 2.4 | |||
| T2 | 24 (20%) | 0.0 (0.0–0.23) | 0.90 ± 0.62 | 5.4 (3.1–9.5) | 6.1 ± 0.7 | |||
| T3 | 14 (11%) | 0.10 (0.0–0.74) | 0.44 ± 0.17 | 6.7 (3.9–10.7) | 7.2 ± 1.1 | |||
| T4 | 6 (5%) | 0.28 (0.05–1.23) | 0.55 ± 0.25 | 4.7 (3.1–11.8) | 6.7 ± 1.9 | |||
| Muscle invasiveness | NMIBC (Ta/Tis/T1) | 78 (64%) | 0.0 (0.0–0.19) | 0.22 ± 0.07 | 0.04 † | 24.7 (16.6–32.7) | 24.9 ± 1.4 | <0.001 † |
| MIBC (T2-4) | 44 (36%) | 0.05 (0.0–0.52) | 0.70 ± 0.34 | 5.4 (3.3–9.7) | 6.5 ± 0.6 | |||
| Performance Characteristics | Urine Nectin-2 | Urine Nectin-4 | NMP-22 | VUC | ||
|---|---|---|---|---|---|---|
| Control vs. BCa | NMIBC vs. MIBC | Control vs. BCa | NMIBC vs. MIBC | Control vs. BCa | Control vs. BCa | |
| AUROC | 0.56 | 0.60 | 0.94 | 0.92 | - | - |
| Cutoff value | 0.53 ng/mL † | 0.011 ng/mL † | 1.64 ng/mL † | 12.0 ng/mL † | 10 U/mL ‡ | - |
| Sensitivity (%) | 84 (77–90) | 61 (46–74) | 98 (93–99) | 91 (79–96) | 52 (43–60) | 47 (38–56) |
| Specificity (%) | 40 (17–69) | 61 (50–72) | 80 (49–96) | 86 (76–92) | 100 (72–100) | 100 (72–100) |
| Positive predictive value (%) | 95 (89–97) | 47 (35–60) | 98 (94–99) | 78 (65–88) | 100 (94–100) | 100 (94–100) |
| Negative predictive value (%) | 17 (7.0–37) | 74 (52–83) | 73 (43–90) | 94 (86–98) | 14 (8.1–25) | 13 (7.4–23) |
| Accuracy (%) | 81 | 57 | 96 | 81 | 55 | 51 |
| McNemar test, p value for comparison with VUC | p < 0.001 | - | p < 0.001 | - | p = 0.50 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyake, M.; Nishimura, N.; Ohnishi, S.; Oda, Y.; Owari, T.; Ohnishi, K.; Morizawa, Y.; Hori, S.; Gotoh, D.; Nakai, Y.; et al. Diagnostic and Prognostic Roles of Urine Nectin-2 and Nectin-4 in Human Bladder Cancer. Cancers 2023, 15, 2565. https://doi.org/10.3390/cancers15092565
Miyake M, Nishimura N, Ohnishi S, Oda Y, Owari T, Ohnishi K, Morizawa Y, Hori S, Gotoh D, Nakai Y, et al. Diagnostic and Prognostic Roles of Urine Nectin-2 and Nectin-4 in Human Bladder Cancer. Cancers. 2023; 15(9):2565. https://doi.org/10.3390/cancers15092565
Chicago/Turabian StyleMiyake, Makito, Nobutaka Nishimura, Sayuri Ohnishi, Yuki Oda, Takuya Owari, Kenta Ohnishi, Yosuke Morizawa, Shunta Hori, Daisuke Gotoh, Yasushi Nakai, and et al. 2023. "Diagnostic and Prognostic Roles of Urine Nectin-2 and Nectin-4 in Human Bladder Cancer" Cancers 15, no. 9: 2565. https://doi.org/10.3390/cancers15092565
APA StyleMiyake, M., Nishimura, N., Ohnishi, S., Oda, Y., Owari, T., Ohnishi, K., Morizawa, Y., Hori, S., Gotoh, D., Nakai, Y., Torimoto, K., Fujii, T., Tanaka, N., & Fujimoto, K. (2023). Diagnostic and Prognostic Roles of Urine Nectin-2 and Nectin-4 in Human Bladder Cancer. Cancers, 15(9), 2565. https://doi.org/10.3390/cancers15092565