



A Comparison between the Online Prognostic Tool PREDICT and myBeST for Women with Breast Cancer in Malaysia
 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
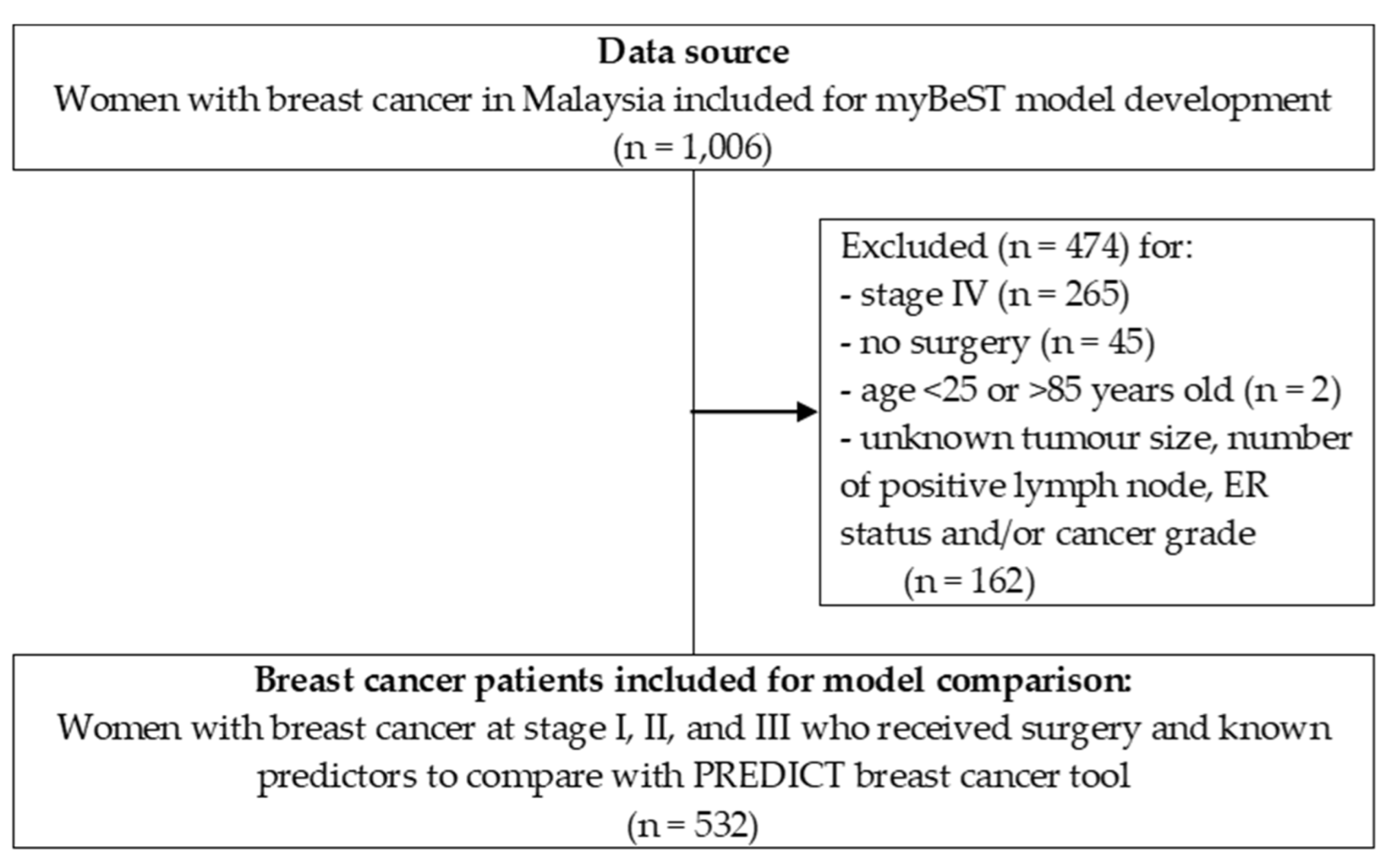
2.1. Data Source and Study Design
2.2. Analysis Method
2.3. Ethics Statement
3. Results
3.1. Patients’ Profile
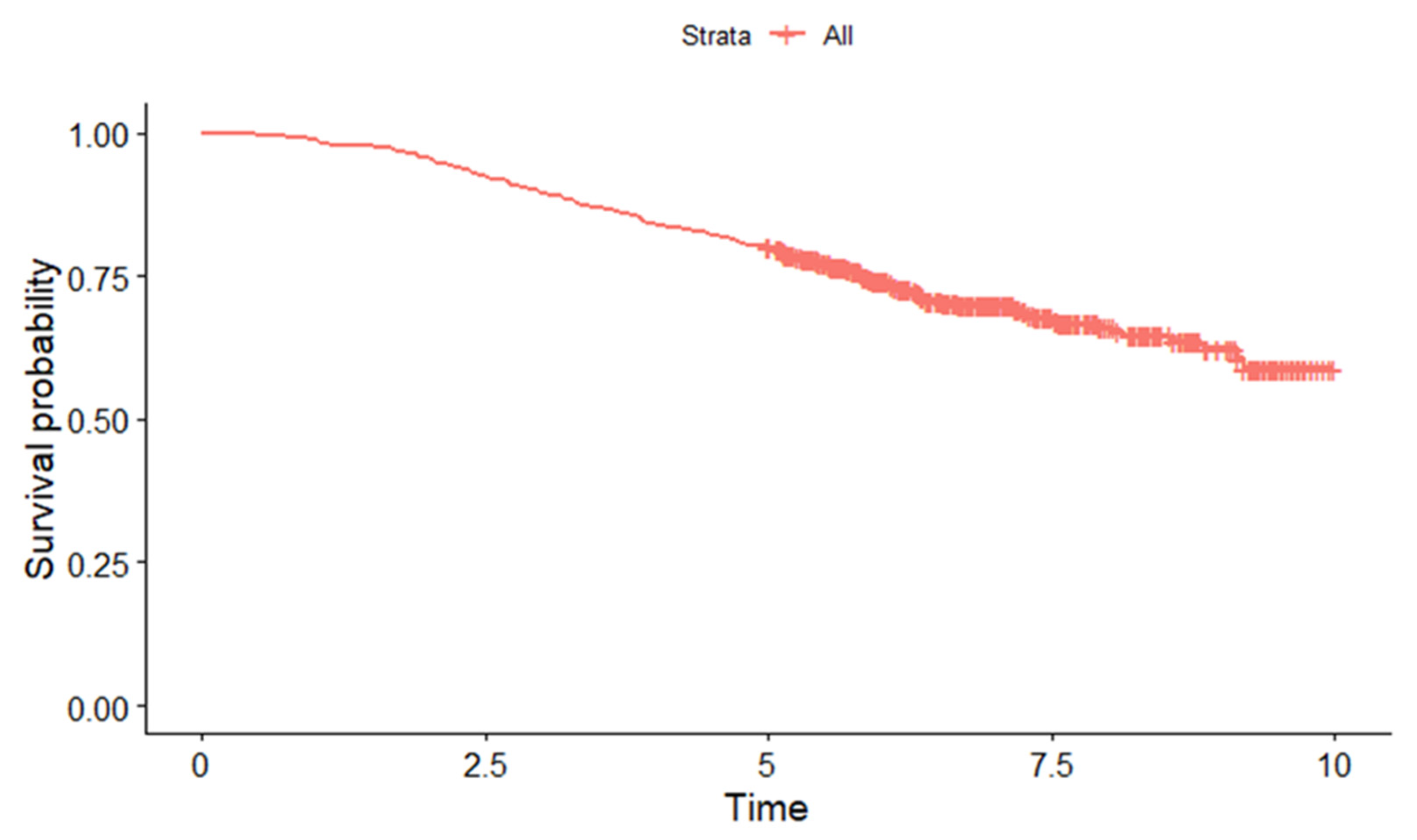
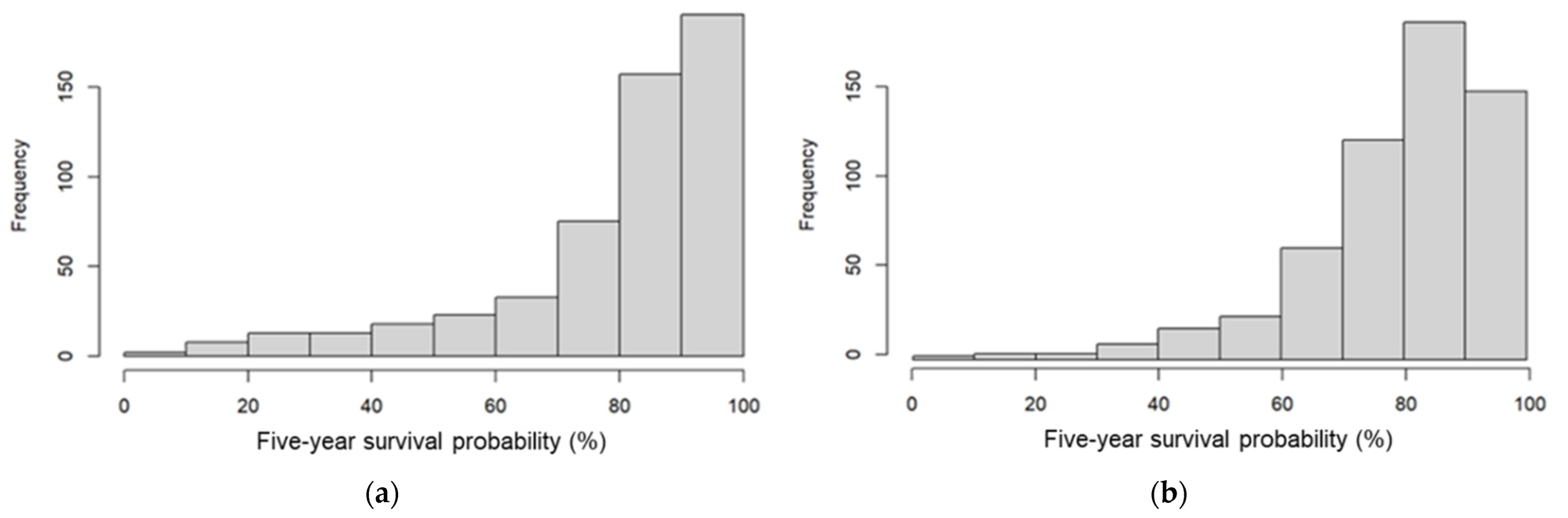
3.2. Five-Year Observed Survival and Predicted Survival Probability
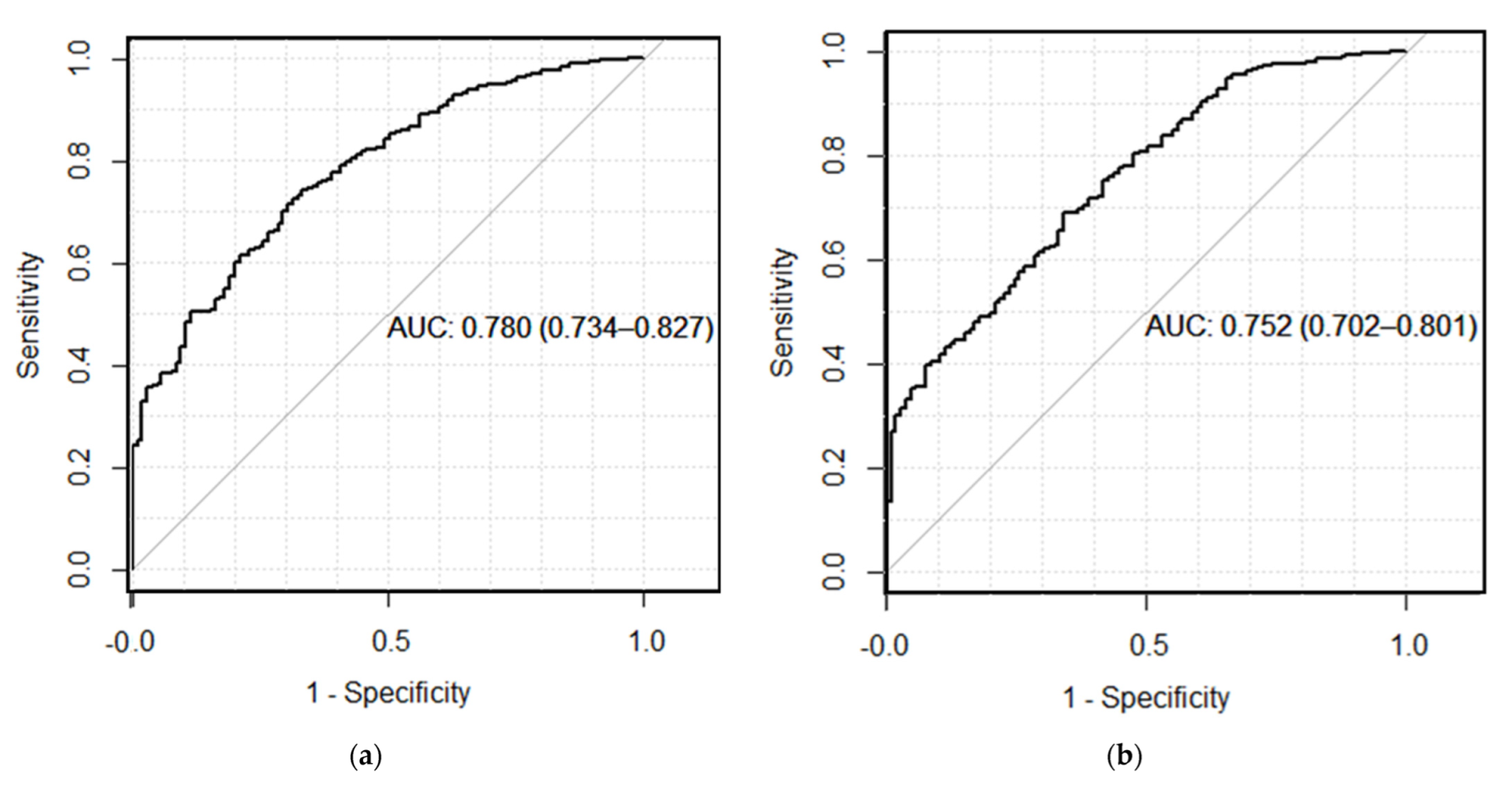
3.3. Performance of PREDICT and myBeST
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Ji, P.; Gong, Y.; Jin, M.-L.; Hu, X.; Di, G.-H.; Shao, Z.-M. The Burden and Trends of Breast Cancer from 1990 to 2017 at the Global, Regional, and National Levels: Results from the Global Burden of Disease Study 2017. Front. Oncol. 2020, 10, 650. [Google Scholar] [CrossRef]
- National Cancer Institute Ministry of Health (NCI MOH) Malaysia. Malaysia National Cancer Registry Report 2012–2016; NCI MOH Malaysia: Putrajaya, Malaysia, 2019. [Google Scholar]
- Yusoff, J.; Ismail, A. Out of Pockets Spending among Breast Cancer Women Receiving Out-Patient Treatment in a Tertiary Teaching Hospital in Kuala Lumpur Malaysia. Malaysian J. Public Health Med. 2021, 21, 240–249. [Google Scholar] [CrossRef]
- Dean, L.T.; Moss, S.L.; Ransome, Y.; Frasso-Jaramillo, L.; Zhang, Y.; Visvanathan, K.; Nicholas, L.H.; Schmitz, K.H. “It Still Affects Our Economic Situation”: Long-Term Economic Burden of Breast Cancer and Lymphedema. Support. Care Cancer 2019, 27, 1697–1708. [Google Scholar] [CrossRef]
- Toivonen, K.I.; Williamson, T.M.; Carlson, L.E.; Walker, L.M.; Campbell, T.S. Potentially Modifiable Factors Associated with Adherence to Adjuvant Endocrine Therapy among Breast Cancer Survivors: A Systematic Review. Cancers 2020, 13, 107. [Google Scholar] [CrossRef] [PubMed]
- Mohd Mujar, N.M.; Dahlui, M.; Emran, N.A.; Hadi, I.A.; Yan, Y.W.; Arulanantham, S.; Chea, C.H.; Mohd Taib, N.A. Breast Cancer Care Timeliness Framework: A Quality Framework for Cancer Control. JCO Glob. Oncol. 2022, 8, e2100250. [Google Scholar] [CrossRef] [PubMed]
- Phung, M.T.; Tin Tin, S.; Elwood, J.M. Prognostic Models for Breast Cancer: A Systematic Review. BMC Cancer 2019, 19, 230. [Google Scholar] [CrossRef] [PubMed]
- Shachar, S.S.; Muss, H.B. Internet Tools to Enhance Breast Cancer Care. npj Breast Cancer 2016, 2, 16011. [Google Scholar] [CrossRef]
- Michaelson, J.S.; Chen, L.L.; Bush, D.; Fong, A.; Smith, B.; Younger, J. Improved Web-Based Calculators for Predicting Breast Carcinoma Outcomes. Breast Cancer Res. Treat. 2011, 128, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Ravdin, P.M.; Siminoff, L.A.; Davis, G.J.; Mercer, M.B.; Hewlett, J.; Gerson, N.; Parker, H.L. Computer Program to Assist in Making Decisions about Adjuvant Therapy for Women with Early Breast Cancer. J. Clin. Oncol. 2001, 19, 980–991. [Google Scholar] [CrossRef]
- Haybittle, J.L.; Blamey, R.W.; Elston, C.W.; Johnson, J.; Doyle, P.J.; Campbell, F.C.; Nicholson, R.I.; Griffiths, K. A Prognostic Index in Primary Breast Cancer. Br. J. Cancer 1982, 45, 361–366. [Google Scholar] [CrossRef]
- Wishart, G.C.; Azzato, E.M.; Greenberg, D.C.; Rashbass, J.; Kearins, O.; Lawrence, G.; Caldas, C.; Pharoah, P.D.P. PREDICT: A New UK Prognostic Model That Predicts Survival Following Surgery for Invasive Breast Cancer. Breast Cancer Res. 2010, 12, R1. [Google Scholar] [CrossRef] [PubMed]
- Candido dos Reis, F.J.; Wishart, G.C.; Dicks, E.M.; Greenberg, D.; Rashbass, J.; Schmidt, M.K.; van den Broek, A.J.; Ellis, I.O.; Green, A.; Rakha, E.; et al. An Updated PREDICT Breast Cancer Prognostication and Treatment Benefit Prediction Model with Independent Validation. Breast Cancer Res. 2017, 19, 58. [Google Scholar] [CrossRef] [PubMed]
- Bhoo-Pathy, N.; Yip, C.-H.; Hartman, M.; Saxena, N.; Taib, N.A.; Ho, G.F.; Looi, L.-M.; Bulgiba, A.M.; van der Graaf, Y.; Verkooijen, H.M. Adjuvant! Online Is Overoptimistic in Predicting Survival of Asian Breast Cancer Patients. Eur. J. Cancer 2012, 48, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Miao, H.; Hartman, M.; Verkooijen, H.M.; Taib, N.A.; Wong, H.S.; Subramaniam, S.; Yip, C.H.; Tan, E.Y.; Chan, P.; Lee, S.C.; et al. Validation of the CancerMath Prognostic Tool for Breast Cancer in Southeast Asia. BMC Cancer 2016, 16, 820. [Google Scholar] [CrossRef]
- Wong, H.S.; Subramaniam, S.; Alias, Z.; Taib, N.A.; Ho, G.F.; Ng, C.H.; Yip, C.H.; Verkooijen, H.M.; Hartman, M.; Bhoo-Pathy, N. The Predictive Accuracy of PREDICT: A Personalized Decision-Making Tool for Southeast Asian Women with Breast Cancer. Medicine 2015, 94, e593. [Google Scholar] [CrossRef]
- Gray, E.; Marti, J.; Brewster, D.H.; Wyatt, J.C.; Hall, P.S. Independent Validation of the PREDICT Breast Cancer Prognosis Prediction Tool in 45,789 Patients Using Scottish Cancer Registry Data. Br. J. Cancer 2018, 119, 808–814. [Google Scholar] [CrossRef]
- van Maaren, M.C.; van Steenbeek, C.D.; Pharoah, P.D.P.; Witteveen, A.; Sonke, G.S.; Strobbe, L.J.A.; Poortmans, P.M.P.; Siesling, S. Validation of the Online Prediction Tool PREDICT v. 2.0 in the Dutch Breast Cancer Population. Eur. J. Cancer 2017, 86, 364–372. [Google Scholar] [CrossRef]
- NICE. Early and Locally Advanced Breast Cancer: Diagnosis and Management; NICE National Institute for Health and Care Excellence: Ra’anana, Israel, 2018. [Google Scholar]
- Nik Ab Kadir, M.N.; Yaacob, N.M.; Yusof, S.N.; Ab Hadi, I.S.; Musa, K.I.; Mohd Isa, S.A.; Bahtiar, B.; Adam, F.; Yahya, M.M.; Mohd Hairon, S. Development of Predictive Models for Survival among Women with Breast Cancer in Malaysia. Int. J. Environ. Res. Public Health 2022, 19, 15335. [Google Scholar] [CrossRef]
- Yip, C.; Bhoo-Pathy, N.; Teo, S. A Review of Breast Cancer Research in Malaysia. Med. J. Malaysia 2014, 69, 8–22. [Google Scholar]
- Saxena, N.; Hartman, M.; Bhoo-Pathy, N.; Lim, J.N.W.; Aw, T.C.; Iau, P.; Taib, N.A.; Lee, S.C.; Yip, C.H.; Verkooijen, H.M. Breast Cancer in South East Asia: Comparison of Presentation and Outcome between a Middle Income and a High Income Country. World J. Surg. 2012, 36, 2838–2846. [Google Scholar] [CrossRef]
- Yu, F.Q.; Murugiah, M.K.; Khan, A.H.; Mehmood, T. Meta-Synthesis Exploring Barriers to Health Seeking Behaviour among Malaysian Breast Cancer Patients. Asian Pac. J. Cancer Prev. 2015, 16, 145–152. [Google Scholar] [CrossRef]
- Nordin, N.; Yaacob, N.M.; Abdullah, N.H.; Hairon, S.M. Survival Time and Prognostic Factors for Breast Cancer among Women in North-East Peninsular Malaysia. Asian Pac. J. Cancer Prev. 2018, 19, 497–502. [Google Scholar]
- Nik Ab Kadir, M.N.; Mohd Hairon, S.; Yaacob, N.M.; Yusof, S.N.; Musa, K.I.; Yahya, M.M.; Seoparjoo Azmel, M.I.; Muhammad Hafizuddin, M.A.; Imi Sairi, A.H. MyBeST-A Web-Based Survival Prognostic Tool for Women with Breast Cancer in Malaysia: Development Process and Preliminary Validation Study. Int. J. Environ. Res. Public Health 2023, 20, 2985. [Google Scholar] [CrossRef]
- Polchai, N.; Sa-Nguanraksa, D.; Numprasit, W.; Thumrongtaradol, T.; O-Charoenrat, E.; O-Charoenrat, P. A Comparison between the Online Prediction Models CancerMath and PREDICT as Prognostic Tools in Thai Breast Cancer Patients. Cancer Manag. Res. 2020, 12, 5549–5559. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Vergouwe, Y. Towards Better Clinical Prediction Models: Seven Steps for Development and an ABCD for Validation. Eur. Heart J. 2014, 35, 1925–1931. [Google Scholar] [CrossRef]
- Zaguirre, K.; Kai, M.; Kubo, M.; Yamada, M.; Kurata, K.; Kawaji, H.; Kaneshiro, K.; Harada, Y.; Hayashi, S.; Shimazaki, A.; et al. Validity of the Prognostication Tool PREDICT Version 2.2 in Japanese Breast Cancer Patients. Cancer Med. 2021, 10, 1605–1613. [Google Scholar] [CrossRef]
- Agostinetto, E.; Ameye, L.; Martel, S.; Aftimos, P.; Pondé, N.; Maurer, C.; El-Abed, S.; Wang, Y.; Vicente, M.; Chumsri, S.; et al. PREDICT Underestimates Survival of Patients with HER2-Positive Early-Stage Breast Cancer. npj Breast Cancer 2022, 8, 87. [Google Scholar] [CrossRef]
- National Cancer Institute Ministry of Health (NCI MOH) Malaysia. Malaysian Study on Cancer Survival (MySCan); NCI MOH Malaysia: Putrajaya, Malaysia, 2018. [Google Scholar]
- Abdullah, N.A.; Mahiyuddin, W.R.W.; Muhammad, N.A.; Mohamad Ali, Z.; Ibrahim, L.; Tamim, N.S.I.; Mustafa, A.N.; Kamaluddin, M.A. Survival Rate of Breast Cancer Patients in Malaysia: A Population-Based Study. Asian Pac. J. Cancer Prev. 2013, 14, 4591–4594. [Google Scholar] [CrossRef]
- Pongnikorn, D.; Phinyo, P.; Patumanond, J.; Daoprasert, K.; Phothong, P.; Siribumrungwong, B. Individualized Prediction of Breast Cancer Survival Using Flexible Parametric Survival Modeling: Analysis of a Hospital-based National Clinical Cancer Registry. Cancers 2021, 13, 1567. [Google Scholar] [CrossRef]
- Charumporn, T.; Jarupanich, N.; Rinthapon, C.; Meetham, K.; Pattayakornkul, N.; Taerujjirakul, T.; Tanasombatkul, K.; Ditsatham, C.; Chongruksut, W.; Phanphaisarn, A.; et al. External Validation of the Individualized Prediction of Breast Cancer Survival (IPBS) Model for Estimating Survival after Surgery for Patients with Breast Cancer in Northern Thailand. Cancers 2022, 14, 5726. [Google Scholar] [CrossRef]
- Jung, M.; Choi, E.H.; Nam, C.M.; Rha, S.Y.; Jeung, H.C.; Lee, S.H.; Yang, W.I.; Roh, J.K.; Chung, H.C. Application of the Adjuvant! Online Model to Korean Breast Cancer Patients: An Assessment of Prognostic Accuracy and Development of an Alternative Prognostic Tool. Ann. Surg. Oncol. 2013, 20, 2615–2624. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-C.; Chan, S.-Y.; Lee, W.-C.; Chiang, C.-J.; Lu, T.-P.; Cheng, S.H.-C. Development of a Prediction Model for Breast Cancer Based on the National Cancer Registry in Taiwan. Breast Cancer Res. 2019, 21, 1–9. [Google Scholar] [CrossRef]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global Surveillance of Trends in Cancer Survival 2000–14 (CONCORD-3): Analysis of Individual Records for 37 513 025 Patients Diagnosed with One of 18 Cancers from 322 Population-Based Registries in 71 Countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef]
- Fan, R.; Chen, Y.; Nechuta, S.; Cai, H.; Gu, K.; Shi, L.; Bao, P.; Shyr, Y.; Shu, X.O.; Ye, F. Prediction Models for Breast Cancer Prognosis among Asian Women. Cancer 2021, 127, 1758–1769. [Google Scholar] [CrossRef]
- Wu, X.; Ye, Y.; Barcenas, C.H.; Chow, W.H.; Meng, Q.H.; Chavez-MacGregor, M.; Hildebrandt, M.A.T.; Zhao, H.; Gu, X.; Deng, Y.; et al. Personalized Prognostic Prediction Models for Breast Cancer Recurrence and Survival Incorporating Multidimensional Data. JNCI J. Natl. Cancer Inst. 2017, 109, djw314. [Google Scholar] [CrossRef]
- Hofvind, S.; Holen, Å.; Román, M.; Sebuødegård, S.; Puig-Vives, M.; Akslen, L. Mode of Detection: An Independent Prognostic Factor for Women with Breast Cancer. J. Med. Screen. 2016, 23, 89–97. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Age, mean (SD) in years | 52.1 (10.7) |
| Ethnicity | |
| Malay | 309 (58.1) |
| Chinese | 161 (30.3) |
| Indian | 40 (7.5) |
| Others | 22 (4.1) |
| Marital status | |
| Married | 440 (82.7) |
| Not married (single/divorced/widowed) | 92 (17.3) |
| Histological type | |
| Ductal carcinoma (NST) | 474 (89.1) |
| Lobular carcinoma | 26 (4.9) |
| Others | 32 (6.0) |
| Grade | |
| Well-differentiated (Grade I) | 137 (25.8) |
| Moderately differentiated (Grade II) | 229 (43.0) |
| Poorly differentiated (Grade III) | 166 (31.2) |
| ER status | |
| Positive | 372 (69.9) |
| Negative | 160 (30.1) |
| ER and PR status | |
| Both ER and PR positive | 317 (59.6) |
| Either ER or PR positive | 61 (11.5) |
| Both negative | 154 (28.9) |
| HER2 status | |
| Positive | 140 (26.3) |
| Negative | 332 (62.4) |
| Unknown | 60 (11.3) |
| Tumour size, median (IQR) | 29.0 (20.0–45.0) |
| Tumour (T) stage | |
| T1 | 133 (25.0) |
| T2 | 276 (51.9) |
| T3 | 73 (13.7) |
| T4 | 50 (9.4) |
| Number of positive nodes, median (IQR) | 1.0 (0–2.0) |
| Node (N) stage | |
| N0 | 261 (49.1) |
| N1 | 186 (35.0) |
| N2 | 50 (9.4) |
| N3 | 35 (6.6) |
| Overall TNM stage | |
| I | 91 (17.1) |
| II | 285 (53.6) |
| III | 156 (29.3) |
| Chemotherapy | |
| No | 155 (29.1) |
| Yes | 377 (70.9) |
| Radiotherapy | |
| No | 188 (35.3) |
| Yes | 344 (64.7) |
| Follow-up time, median (IQR) | 6.1 (5.2–7.5) |
| Five-year survival status | |
| Alive | 427 (80.3) |
| Dead | 105 (19.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nik Ab Kadir, M.N.; Mohd Hairon, S.; Ab Hadi, I.S.; Yusof, S.N.; Muhamat, S.M.; Yaacob, N.M. A Comparison between the Online Prognostic Tool PREDICT and myBeST for Women with Breast Cancer in Malaysia. Cancers 2023, 15, 2064. https://doi.org/10.3390/cancers15072064
Nik Ab Kadir MN, Mohd Hairon S, Ab Hadi IS, Yusof SN, Muhamat SM, Yaacob NM. A Comparison between the Online Prognostic Tool PREDICT and myBeST for Women with Breast Cancer in Malaysia. Cancers. 2023; 15(7):2064. https://doi.org/10.3390/cancers15072064
Chicago/Turabian StyleNik Ab Kadir, Mohd Nasrullah, Suhaily Mohd Hairon, Imi Sairi Ab Hadi, Siti Norbayah Yusof, Siti Maryam Muhamat, and Najib Majdi Yaacob. 2023. "A Comparison between the Online Prognostic Tool PREDICT and myBeST for Women with Breast Cancer in Malaysia" Cancers 15, no. 7: 2064. https://doi.org/10.3390/cancers15072064
APA StyleNik Ab Kadir, M. N., Mohd Hairon, S., Ab Hadi, I. S., Yusof, S. N., Muhamat, S. M., & Yaacob, N. M. (2023). A Comparison between the Online Prognostic Tool PREDICT and myBeST for Women with Breast Cancer in Malaysia. Cancers, 15(7), 2064. https://doi.org/10.3390/cancers15072064