

Machine Learning-Based Radiomic Features on Pre-Ablation MRI as Predictors of Pathologic Response in Patients with Hepatocellular Carcinoma Who Underwent Hepatic Transplant

 ,
, 

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Data Collection
2.3. Treatment Technique
2.4. MRI Technique
2.5. Tumor Segmentation
2.6. Extraction of Radiomic Features, Model Training and Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. MRI-Based Radiomics Features
3.3. Machine Learning for Treatment Response
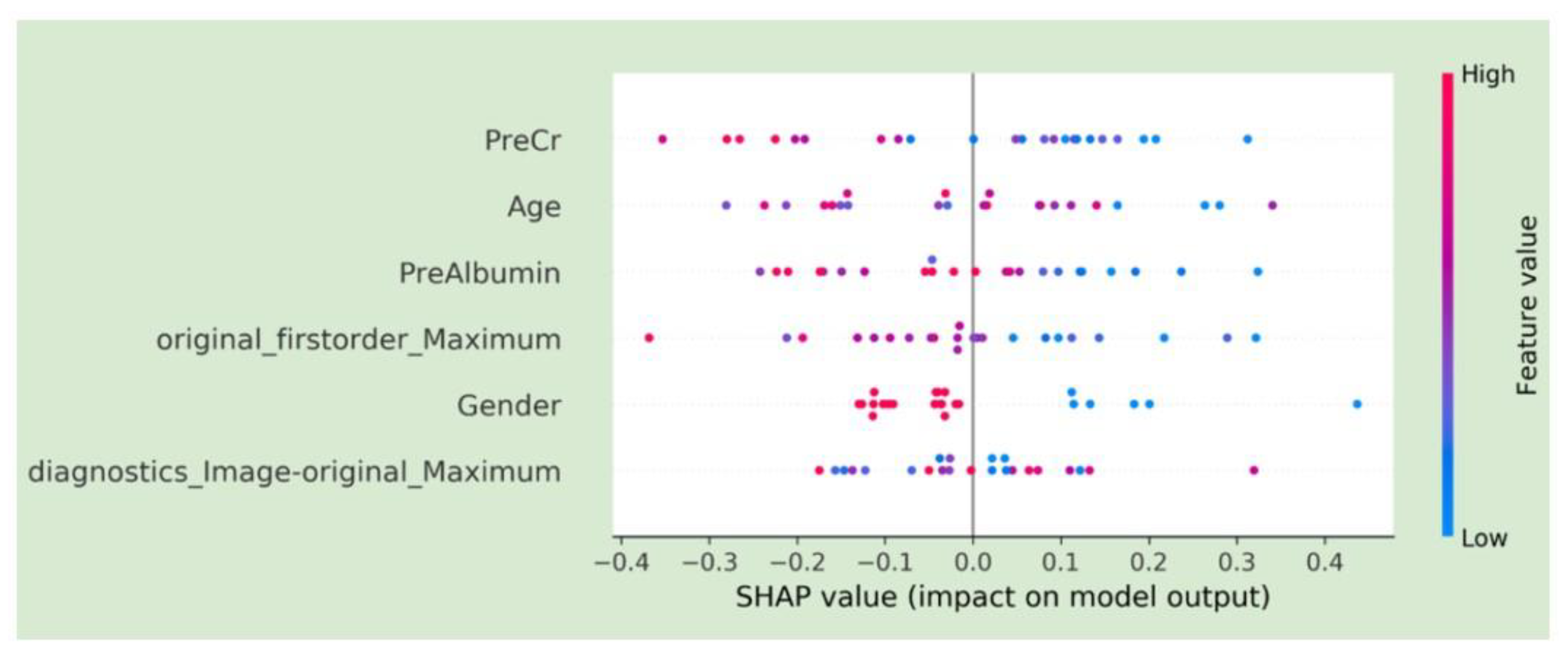
3.4. SHAP Plots for Feature Visualization
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, E.; Viatour, P. Hepatocellular carcinoma: Old friends and new tricks. Exp. Mol. Med. 2020, 52, 1898–1907. [Google Scholar] [CrossRef]
- Freeman, E.; Cheung, W.; Kavnoudias, H.; Majeed, A.; Kemp, W.; Roberts, S.K. Irreversible Electroporation for Hepatocellular Carcinoma: Longer-Term Outcomes at a Single Centre. Cardiovasc. Interv. Radiol. 2020, 44, 247–253. [Google Scholar] [CrossRef]
- Kamarajah, S.K.; Bundred, J.R.; Littler, P.; Reeves, H.; Manas, D.M.; White, S.A. Treatment strategies for early stage hepatocellular carcinoma: A systematic review and network meta-analysis of randomised clinical trials. HPB 2020, 23, 495–505. [Google Scholar] [CrossRef]
- Izzo, F.; Granata, V.; Grassi, R.; Fusco, R.; Palaia, R.; Delrio, P.; Carrafiello, G.; Azoulay, D.; Petrillo, A.; Curley, S.A. Radiofrequency Ablation and Microwave Ablation in Liver Tumors: An Update. Oncologist 2019, 24, e990–e1005. [Google Scholar] [CrossRef]
- Llovet, J.M.; De Baere, T.; Kulik, L.; Haber, P.K.; Greten, T.F.; Meyer, T.; Lencioni, R. Locoregional therapies in the era of molecular and immune treatments for hepatocellular carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 293–313. [Google Scholar] [CrossRef]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2021, 7, 6. [Google Scholar] [CrossRef]
- Chaudhry, M.; McGinty, K.A.; Mervak, B.; Lerebours, R.; Li, C.; Shropshire, E.; Ronald, J.; Commander, L.; Hertel, J.; Luo, S.; et al. The LI-RADS Version 2018 MRI Treatment Response Algorithm: Evaluation of Ablated Hepatocellular Carcinoma. Radiology 2020, 294, 320–326. [Google Scholar] [CrossRef]
- Seo, N.; Kim, M.S.; Park, M.-S.; Choi, J.-Y.; Do, R.K.G.; Han, K.; Kim, M.-J. Evaluation of treatment response in hepatocellular carcinoma in the explanted liver with Liver Imaging Reporting and Data System version 2017. Eur. Radiol. 2020, 30, 261–271. [Google Scholar] [CrossRef]
- Hussein, R.S.; Tantawy, W.; Abbas, Y.A. MRI assessment of hepatocellular carcinoma after locoregional therapy. Insights Into Imaging 2019, 10, 8. [Google Scholar] [CrossRef]
- Severn, C.; Suresh, K.; Görg, C.; Choi, Y.S.; Jain, R.; Ghosh, D. A Pipeline for the Implementation and Visualization of Explainable Machine Learning for Medical Imaging Using Radiomics Features. Sensors 2022, 22, 5205. [Google Scholar] [CrossRef]
- Chetoui, M.; Akhloufi, M.A. Explainable Vision Transformers and Radiomics for COVID-19 Detection in Chest X-rays. J. Clin. Med. 2022, 11, 3013. [Google Scholar] [CrossRef]
- Militello, C.; Prinzi, F.; Sollami, G.; Rundo, L.; La Grutta, L.; Vitabile, S. CT Radiomic Features and Clinical Biomarkers for Predicting Coronary Artery Disease. Cogn. Comput. 2023, 15, 238–253. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef]
- Daye, D.; Tabari, A.; Kim, H.; Chang, K.; Kamran, S.C.; Hong, T.S.; Kalpathy-Cramer, J.; Gee, M.S. Quantitative tumor heterogeneity MRI profiling improves machine learning–based prognostication in patients with metastatic colon cancer. Eur. Radiol. 2021, 31, 5759–5767. [Google Scholar] [CrossRef]
- Daye, D.; Staziaki, P.V.; Furtado, V.F.; Tabari, A.; Fintelmann, F.J.; Frenk, N.E.; Shyn, P.; Tuncali, K.; Silverman, S.; Arellano, R.; et al. CT Texture Analysis and Machine Learning Improve Post-ablation Prognostication in Patients with Adrenal Metastases: A Proof of Concept. Cardiovasc. Interv. Radiol. 2019, 42, 1771–1776. [Google Scholar] [CrossRef]
- Papanikolaou, N.; Matos, C.; Koh, D.M. How to develop a meaningful radiomic signature for clinical use in oncologic patients. Cancer Imaging 2020, 20, 33. [Google Scholar] [CrossRef]
- Kuang, Y.; Li, R.; Jia, P.; Ye, W.; Zhou, R.; Zhu, R.; Wang, J.; Lin, S.; Pang, P.; Ji, W. MRI-Based Radiomics: Nomograms predicting the short-term response after transcatheter arterial chemoembolization (TACE) in hepatocellular carcinoma patients with diameter less than 5 cm. Abdom. Imaging 2021, 46, 3772–3789. [Google Scholar] [CrossRef]
- Fowler, K.J.; Karimova, E.J.; Arauz, A.R.; Saad, N.E.; Brunt, E.M.; Chapman, W.C.; Heiken, J.P. Validation of Organ Procurement and Transplant Network (OPTN)/United Network for Organ Sharing (UNOS) Criteria for Imaging Diagnosis of Hepatocellular Carcinoma. Transplantation 2013, 95, 1506–1511. [Google Scholar] [CrossRef]
- Poulou, L.S. Percutaneous microwave ablation vs. radiofrequency ablation in the treatment of hepatocellular carcinoma. World J. Hepatol. 2015, 7, 1054–1063. [Google Scholar] [CrossRef]
- D’Onofrio, M.; Ciaravino, V.; De Robertis, R.; Barbi, E.; Salvia, R.; Girelli, R.; Paiella, S.; Gasparini, C.; Cardobi, N.; Bassi, C. Percutaneous ablation of pancreatic cancer. World J. Gastroenterol. 2016, 22, 9661–9673. [Google Scholar] [CrossRef]
- Makary, M.S.; Khandpur, U.; Cloyd, J.M.; Mumtaz, K.; Dowell, J.D. Locoregional Therapy Approaches for Hepatocellular Carcinoma: Recent Advances and Management Strategies. Cancers 2020, 12, 1914. [Google Scholar] [CrossRef]
- Wedd, J.P.; Nordstrom, E.; Nydam, T.; Durham, J.; Zimmerman, M.; Johnson, T.; Purcell, W.T.; Biggins, S.W. Hepatocellular carcinoma in patients listed for liver transplantation: Current and future allocation policy and management strategies for the individual patient. Liver Transplant. 2015, 21, 1543–1552. [Google Scholar] [CrossRef] [PubMed]
- Virzì, A.; Muller, C.O.; Marret, J.-B.; Mille, E.; Berteloot, L.; Grévent, D.; Boddaert, N.; Gori, P.; Sarnacki, S.; Bloch, I. Comprehensive Review of 3D Segmentation Software Tools for MRI Usable for Pelvic Surgery Planning. J. Digit. Imaging 2019, 33, 99–110. [Google Scholar] [CrossRef]
- Bodalal, Z.; Trebeschi, S.; Nguyen-Kim, T.D.L.; Schats, W.; Beets-Tan, R. Radiogenomics: Bridging imaging and genomics. Abdom. Imaging 2019, 44, 1960–1984. [Google Scholar] [CrossRef]
- Tomaszewski, M.R.; Gillies, R.J. The Biological Meaning of Radiomic Features. Radiology 2021, 298, 505–516. [Google Scholar] [CrossRef]
- Yuan, C.; Wang, Z.; Gu, D.; Tian, J.; Zhao, P.; Wei, J.; Yang, X.; Hao, X.; Dong, D.; He, N.; et al. Prediction early recurrence of hepatocellular carcinoma eligible for curative ablation using a Radiomics nomogram. Cancer Imaging 2019, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tabari, A.; Chan, S.M.; Omar, O.M.F.; Iqbal, S.I.; Gee, M.S.; Daye, D. Role of Machine Learning in Precision Oncology: Applications in Gastrointestinal Cancers. Cancers 2022, 15, 63. [Google Scholar] [CrossRef]
- Wu, M.; Tan, H.; Gao, F.; Hai, J.; Ning, P.; Chen, J.; Zhu, S.; Wang, M.; Dou, S.; Shi, D. Predicting the grade of hepatocellular carcinoma based on non-contrast-enhanced MRI radiomics signature. Eur. Radiol. 2018, 29, 2802–2811. [Google Scholar] [CrossRef] [PubMed]
- Iseke, S.; Zeevi, T.; Kucukkaya, A.S.; Raju, R.; Gross, M.; Haider, S.P.; Petukhova-Greenstein, A.; Kuhn, T.N.; Lin, M.; Nowak, M.; et al. Machine Learning Models for Prediction of Posttreatment Recurrence in Early-Stage Hepatocellular Carcinoma Using Pretreatment Clinical and MRI Features: A Proof-of-Concept Study. Am. J. Roentgenol. 2023, 220, 245–255. [Google Scholar] [CrossRef]
- Liu, Q.-P.; Yang, K.-L.; Xu, X.; Liu, X.-S.; Qu, J.-R.; Zhang, Y.-D. Radiomics analysis of pretreatment MRI in predicting tumor response and outcome in hepatocellular carcinoma with transarterial chemoembolization: A two-center collaborative study. Abdom. Imaging 2021, 47, 651–663. [Google Scholar] [CrossRef]
- Sheen, H.; Kim, J.S.; Lee, J.K.; Choi, S.Y.; Baek, S.Y.; Kim, J.Y. A radiomics nomogram for predicting transcatheter arterial chemoembolization refractoriness of hepatocellular carcinoma without extrahepatic metastasis or macrovascular invasion. Abdom. Imaging 2021, 46, 2839–2849. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Value | |
|---|---|
| No. of subjects | 97 |
| Mean age a (years ± SD) | 57.3 ± 7.8 |
| Sex (F:M) | 18:79 |
| Interval between ablation and transplantation (d) | 336.22 ± 179.60 |
| Total bilirubin level (mg/dL) | 1.31 ± 0.81 |
| Albumin level | 3.65 ± 0.68 |
| INR level | 1.24 ± 0.16 |
| Creatinine level | 0.89 ± 0.22 |
| MELD score | |
| Mean | 10.56 ± 3.4 |
| Median | 11 |
| Range | 6–21 |
| Underlying cause of liver disease * | |
| Hepatitis C only | 60 |
| Alcohol only | 10 |
| Hepatitis B only | 9 |
| Hepatitis C and Alcohol | 5 |
| Nonalcoholic Steatohepatitis | 4 |
| Nonalcoholic Fatty Liver Disease | 2 |
| Hemochromatosis | 2 |
| Hepatitis B and C | 1 |
| Primary Biliary Cholangitis | 1 |
| Autoimmune Hepatitis | 1 |
| Budd-Chiari | 1 |
| Cryptogenic | 1 |
| Pre-embolization lesion size (mm) | 2.41 ± 0.69 |
| Treatment modality | |
| Percutaneous Microwave ablation | 31 |
| Percutaneous Radiofrequency ablation | 66 |
| Repeat Procedure | 22 |
| Features | Coefficient (B) | 95% Confidence Interval | p-Value |
|---|---|---|---|
| First−order_Energy | −3.98 × 10−5 | (−9.27 × 10−6 to 7.04 × 10−5) | 0.011 |
| First−order_TotalEnergy | −4.80 × 10−5 | (−1.12 × 10−5 to 8.47 × 10−5) | 0.011 |
| Glrlm_LongRunEmphasis | −5.4 × 10−3 | (−1.98 × 10−4 to −1.06 × 10−2) | 0.042 |
| Glrlm_LongRunHighGrayLevelEmphasis | −5.9 × 10−3 | (−9.92 × 10−4 to −1.08 × 10−2) | 0.019 |
| Model | AUC | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|
| Clinical features only | 0.75 | 0.73 | 0.58 | 0.62 | 0.70 |
| Radiomics only | 0.73 | 0.45 | 0.83 | 0.62 | 0.71 |
| Combined Radiomics and clinical features | 0.83 | 0.82 | 0.67 | 0.69 | 0.80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabari, A.; D’Amore, B.; Cox, M.; Brito, S.; Gee, M.S.; Wehrenberg-Klee, E.; Uppot, R.N.; Daye, D. Machine Learning-Based Radiomic Features on Pre-Ablation MRI as Predictors of Pathologic Response in Patients with Hepatocellular Carcinoma Who Underwent Hepatic Transplant. Cancers 2023, 15, 2058. https://doi.org/10.3390/cancers15072058
Tabari A, D’Amore B, Cox M, Brito S, Gee MS, Wehrenberg-Klee E, Uppot RN, Daye D. Machine Learning-Based Radiomic Features on Pre-Ablation MRI as Predictors of Pathologic Response in Patients with Hepatocellular Carcinoma Who Underwent Hepatic Transplant. Cancers. 2023; 15(7):2058. https://doi.org/10.3390/cancers15072058
Chicago/Turabian StyleTabari, Azadeh, Brian D’Amore, Meredith Cox, Sebastian Brito, Michael S. Gee, Eric Wehrenberg-Klee, Raul N. Uppot, and Dania Daye. 2023. "Machine Learning-Based Radiomic Features on Pre-Ablation MRI as Predictors of Pathologic Response in Patients with Hepatocellular Carcinoma Who Underwent Hepatic Transplant" Cancers 15, no. 7: 2058. https://doi.org/10.3390/cancers15072058
APA StyleTabari, A., D’Amore, B., Cox, M., Brito, S., Gee, M. S., Wehrenberg-Klee, E., Uppot, R. N., & Daye, D. (2023). Machine Learning-Based Radiomic Features on Pre-Ablation MRI as Predictors of Pathologic Response in Patients with Hepatocellular Carcinoma Who Underwent Hepatic Transplant. Cancers, 15(7), 2058. https://doi.org/10.3390/cancers15072058