
Exercise Intervention for Bone Metastasis: Safety, Efficacy and Method of Delivery

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Eligibility Criteria
2.2.1. Population
2.2.2. Intervention
2.2.3. Comparator
2.3. Information Sources
2.4. Search Strategies
2.5. Selection of Sources of Evidence
2.6. Data Charting Process
2.7. Synthesis of Results
3. Results
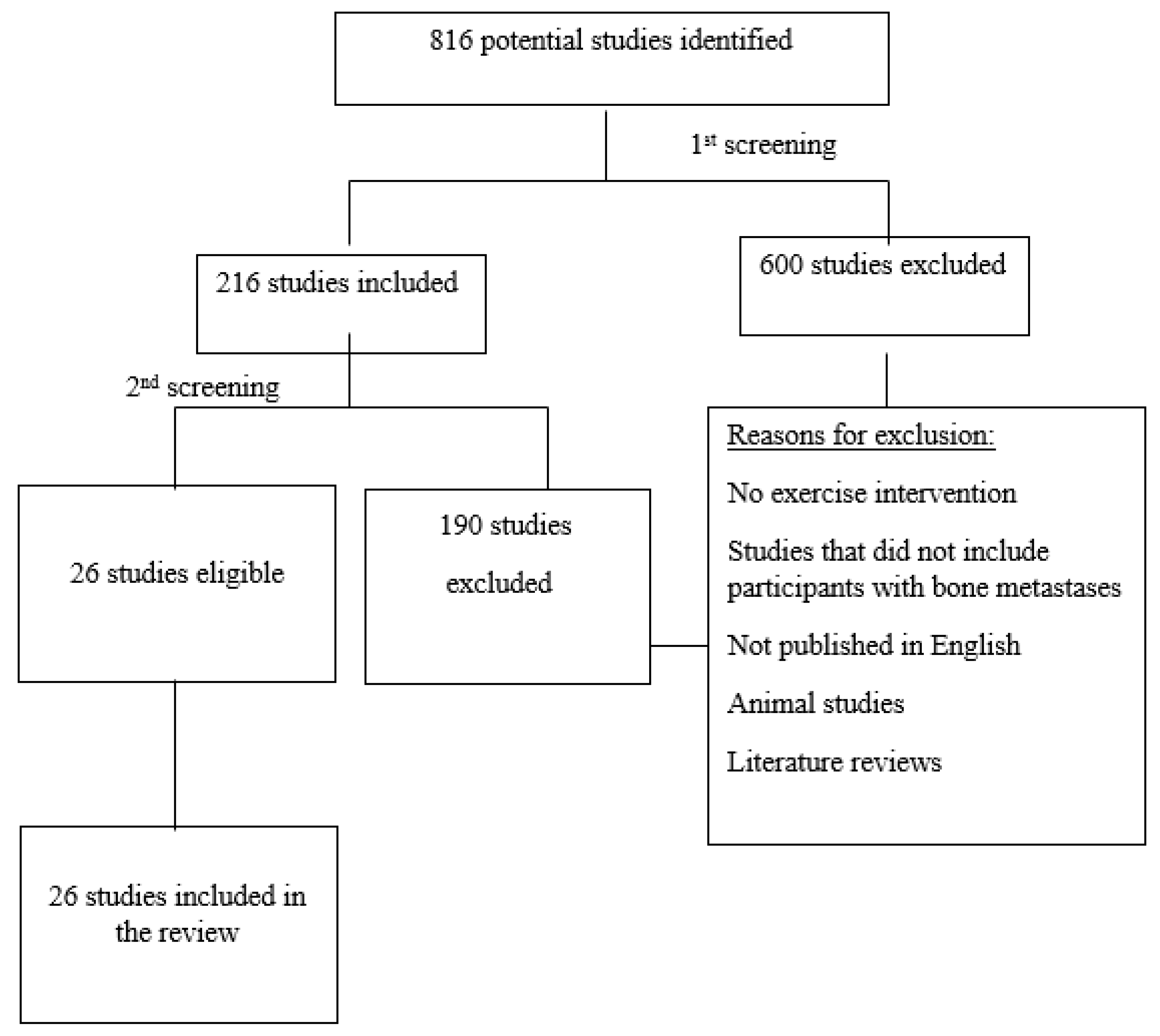
3.1. Selection of Sources of Evidence
3.2. Characteristics of Sources of Evidence
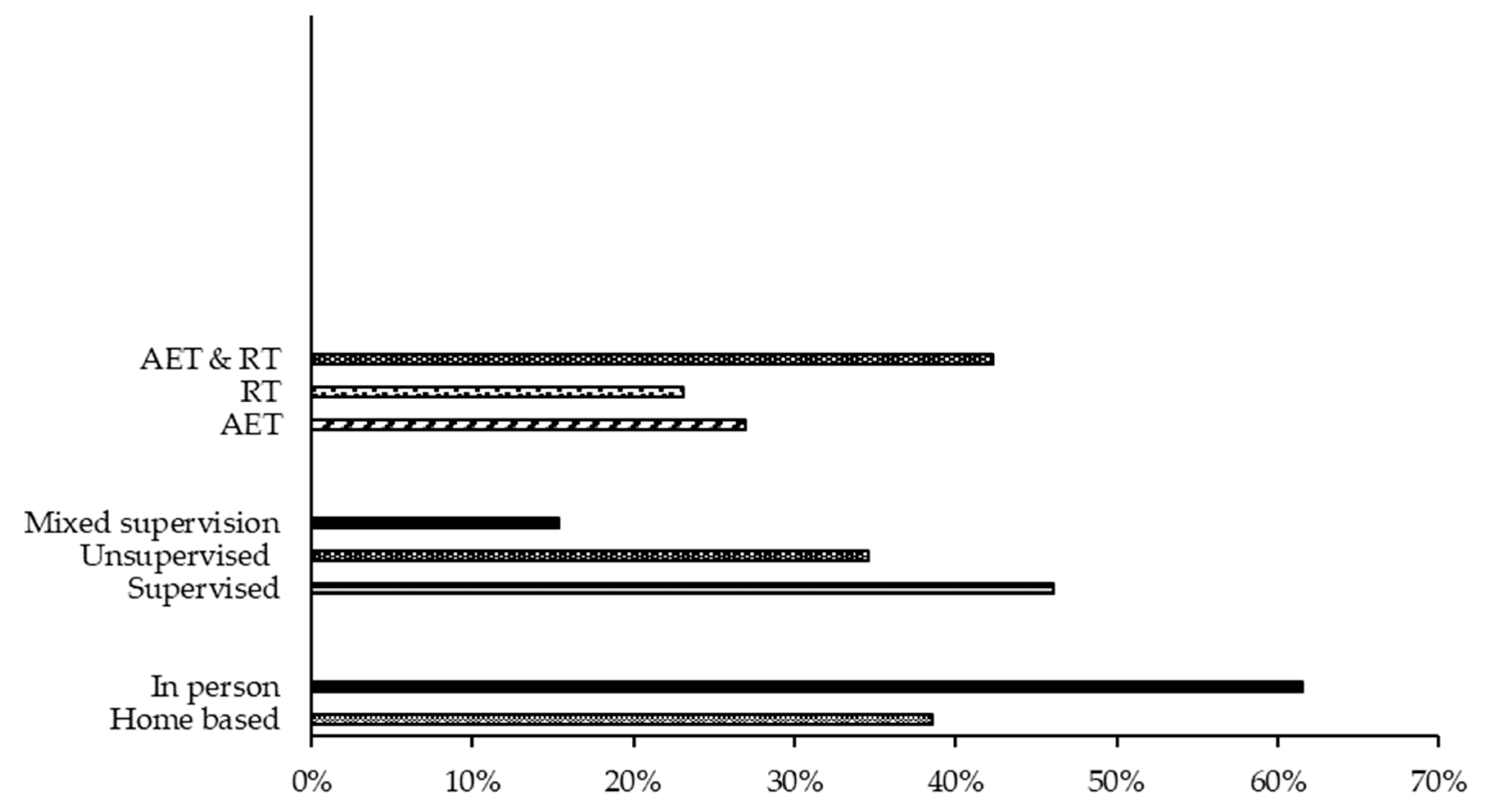
3.3. Intervention Characteristics
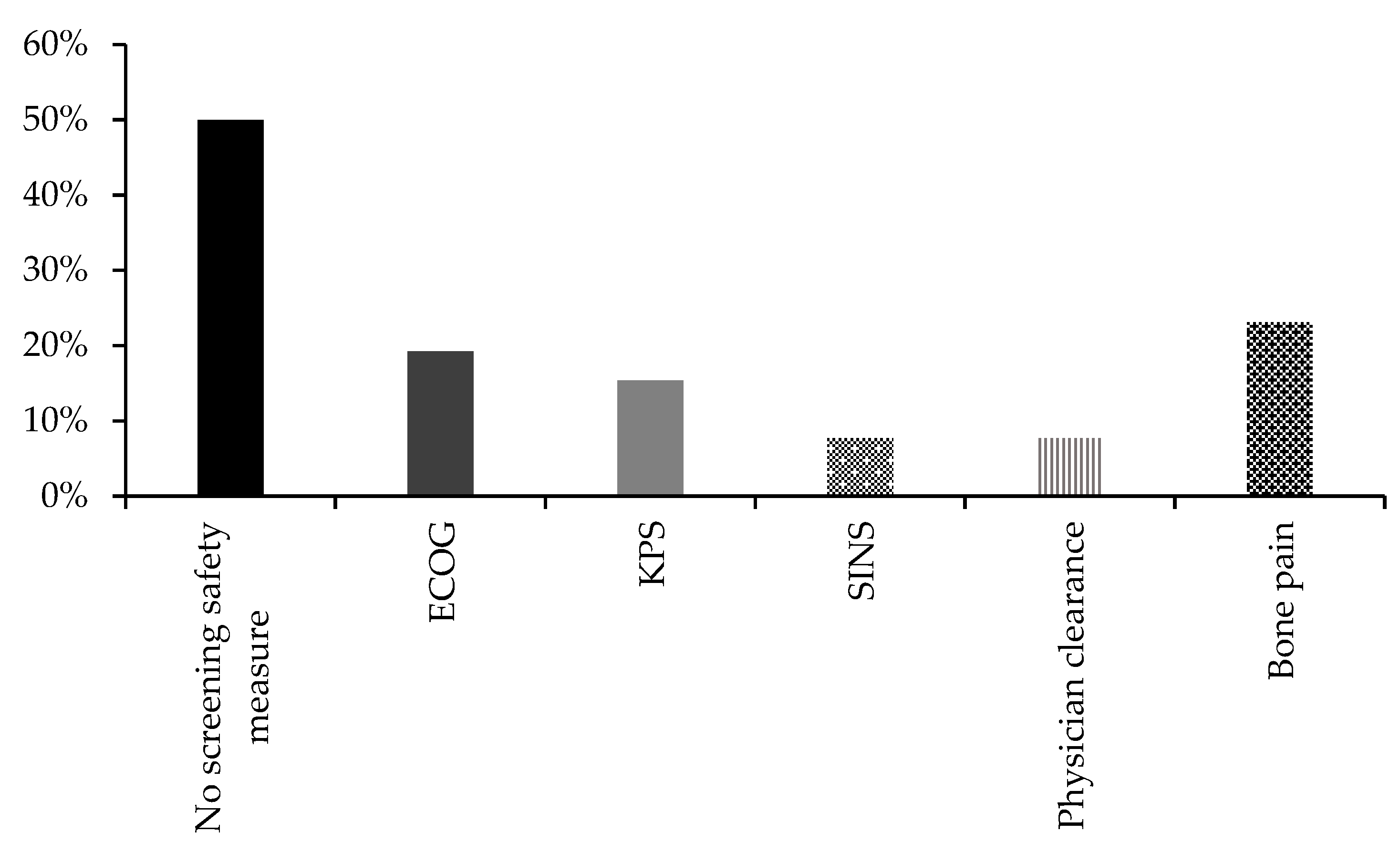
3.4. Safety of Exercise Intervention
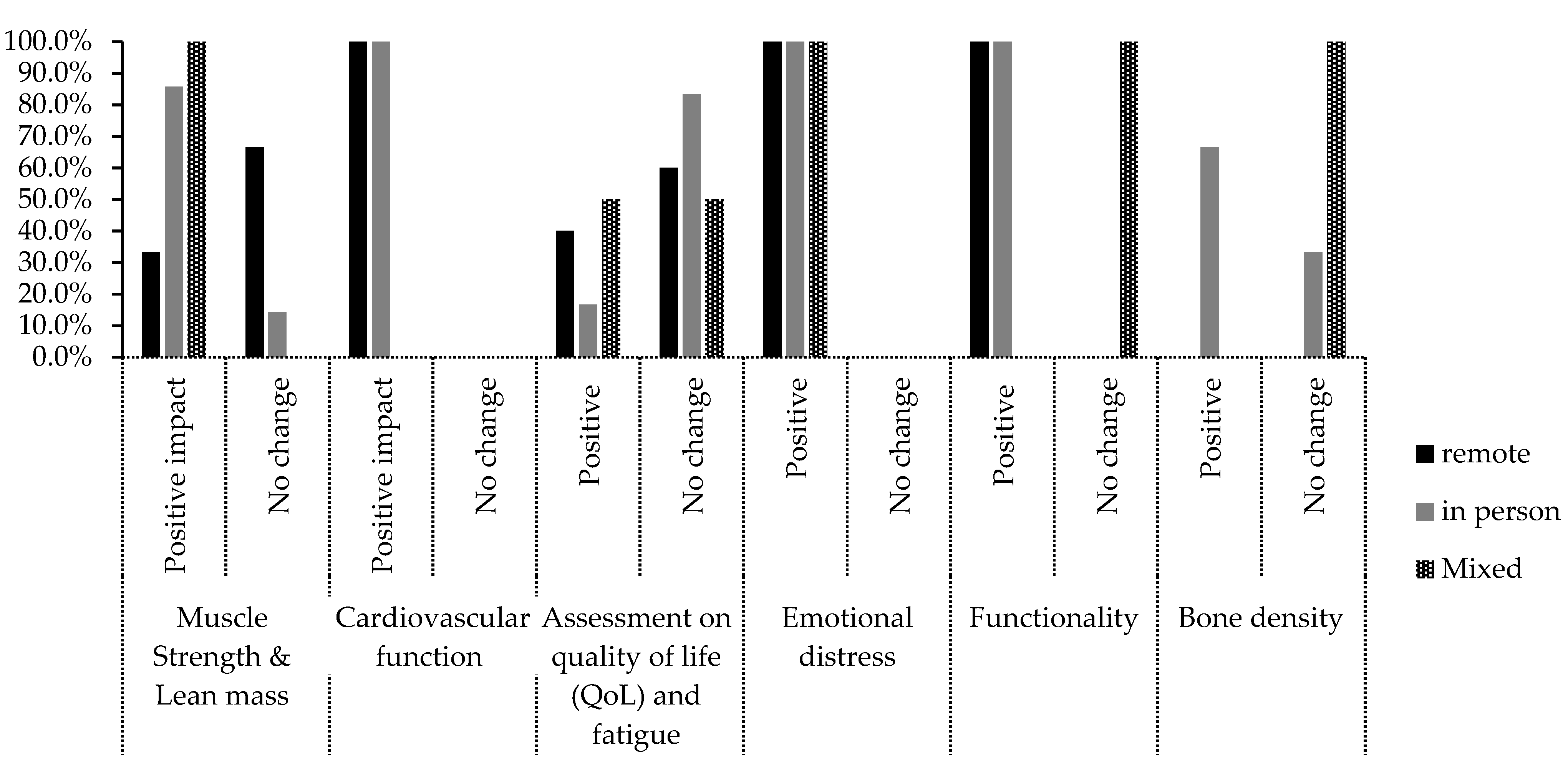
3.5. Intervention Efficacy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Campbell, K.L.; Cormie, P.; Weller, S.; Alibhai, S.M.H.; Bolam, K.A.; Campbell, A.; Cheville, A.L.; Dalzell, M.-A.; Hart, N.H.; Higano, C.S.; et al. Exercise Recommendation for People With Bone Metastases: Expert Consensus for Health Care Providers and Exercise Professionals. JCO Oncol. Pract. 2022, 18, e697–e709. [Google Scholar] [CrossRef]
- Weller, S.; Hart, N.H.; Bolam, K.A.; Mansfield, S.; Santa Mina, D.; Winters-Stone, K.M.; Campbell, A.; Rosenberger, F.; Wiskemann, J.; Quist, M.; et al. Exercise for Individuals with Bone Metastases: A Systematic Review. Crit. Rev. Oncol. Hematol. 2021, 166, 103433. [Google Scholar] [CrossRef]
- Hart, N.H.; Poprawski, D.M.; Ashbury, F.; Fitch, M.I.; Chan, R.J.; Newton, R.U.; Campbell, K.L. Exercise for People with Bone Metastases: MASCC Endorsed Clinical Recommendations Developed by the International Bone Metastases Exercise Working Group. Support. Care Cancer 2022, 30, 7061–7065. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping Studies: Advancing the Methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley: New York, NY, USA, 2008; ISBN 9780470699515. [Google Scholar]
- Boskey, A.L.; Coleman, R. Aging and Bone. J. Dent. Res. 2010, 89, 1333–1348. [Google Scholar] [CrossRef]
- Rosenberger, F.; Wiskemann, J.; Vallet, S.; Haag, G.M.; Schembri, E.; Jäger, D.; Grüllich, C. Resistance Training as Supportive Measure in Advanced Cancer Patients Undergoing TKI Therapy-a Controlled Feasibility Trial. Support. Care Cancer 2017, 25, 3655–3664. [Google Scholar] [CrossRef] [PubMed]
- Carver, J.L. Feasibility Study of a Home-Based Exercise Intervention Program for Patients with Metastatic Castration-Resistant Prostate Cancer Receiving Androgen—Deprivation Therapy; The University of North Carolina at Chapel Hill: Ann Arbor, MI, USA, 2018. [Google Scholar]
- Litterini, A.J.; Fieler, V.K.; Cavanaugh, J.T.; Lee, J.Q. Differential Effects of Cardiovascular and Resistance Exercise on Functional Mobility in Individuals with Advanced Cancer: A Randomized Trial. Arch. Phys. Med. Rehabil. 2013, 94, 2329–2335. [Google Scholar] [CrossRef] [PubMed]
- Cormie, P.; Newton, R.U.; Spry, N.; Joseph, D.; Taaffe, D.R.; Galvão, D.A. Safety and Efficacy of Resistance Exercise in Prostate Cancer Patients with Bone Metastases. Prostate Cancer Prostatic Dis. 2013, 16, 328–335. [Google Scholar] [CrossRef]
- Yee, J.; Davis, G.M.; Hackett, D.; Beith, J.M.; Wilcken, N.; Currow, D.; Emery, J.; Phillips, J.; Martin, A.; Hui, R.; et al. Physical Activity for Symptom Management in Women With Metastatic Breast Cancer: A Randomized Feasibility Trial on Physical Activity and Breast Metastases. J. Pain Symptom Manag. 2019, 58, 929–939. [Google Scholar] [CrossRef] [PubMed]
- Bjerre, E.D.; Petersen, T.H.; Jørgensen, A.B.; Johansen, C.; Krustrup, P.; Langdahl, B.; Poulsen, M.H.; Madsen, S.S.; Østergren, P.B.; Borre, M.; et al. Community-Based Football in Men with Prostate Cancer: 1-Year Follow-up on a Pragmatic, Multicentre Randomised Controlled Trial. PLoS Med. 2019, 16, e1002936. [Google Scholar] [CrossRef] [PubMed]
- Rosenberger, F.; Sprave, T.; Clauss, D.; Hoffmann, P.; Welzel, T.; Debus, J.; Rief, H.; Wiskemann, J. Spinal Stabilization Exercises for Cancer Patients with Spinal Metastases of High Fracture Risk: Feasibility of the DISPO-II Training Program. Cancers 2021, 13, 201. [Google Scholar] [CrossRef]
- Galvão, D.A.; Taaffe, D.R.; Spry, N.; Cormie, P.; Joseph, D.; Chambers, S.K.; Chee, R.; Peddle-McIntyre, C.J.; Hart, N.H.; Baumann, F.T.; et al. Exercise Preserves Physical Function in Prostate Cancer Patients with Bone Metastases. Med. Sci. Sport. Exerc. 2018, 50, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Coleman, E.A.; Hall-Barrow, J.; Coon, S.; Stewart, C.B. Facilitating Exercise Adherence for Patients with Multiple Myeloma. Clin. J. Oncol. Nurs. 2003, 7, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Cormie, P.; Galvão, D.A.; Spry, N.; Joseph, D.; Taaffe, D.R.; Newton, R.U. Functional Benefits Are Sustained after a Program of Supervised Resistance Exercise in Cancer Patients with Bone Metastases: Longitudinal Results of a Pilot Study. Support. Care Cancer 2014, 22, 1537–1548. [Google Scholar] [CrossRef] [PubMed]
- Crevenna, R.; Schmidinger, M.; Keilani, M.; Nuhr, M.; Fialka-Moser, V.; Zettinig, G.; Quittan, M. Aerobic Exercise for a Patient Suffering from Metastatic Bone Disease. Support. Care Cancer 2003, 11, 120–122. [Google Scholar] [CrossRef]
- Delrieu, L.; Vallance, J.K.; Morelle, M.; Fervers, B.; Pialoux, V.; Friedenreich, C.; Dufresne, A.; Bachelot, T.; Heudel, P.-E.; Trédan, O.; et al. Physical Activity Preferences before and after Participation in a 6-Month Physical Activity Intervention among Women with Metastatic Breast Cancer. Eur. J. Cancer Care 2020, 29, e13169. [Google Scholar] [CrossRef]
- Dorion, V.; Lambert, L.; Frazzi, A.; Cayer, J.-F.; Wong, P. A Pilot Study in the Use of Activity Trackers for Assessing Response to Palliative Radiotherapy. Cureus 2017, 9, e1871. [Google Scholar] [CrossRef]
- Evans, H.E.L.; Galvão, D.A.; Forbes, C.C.; Girard, D.; Vandelanotte, C.; Newton, R.U.; Vincent, A.D.; Wittert, G.; Kichenadasse, G.; Chambers, S.; et al. Acceptability and Preliminary Efficacy of a Web- and Telephone-Based Personalised Exercise Intervention for Individuals with Metastatic Prostate Cancer: The ExerciseGuide Pilot Randomised Controlled Trial. Cancers 2021, 13, 5925. [Google Scholar] [CrossRef]
- Tabacof, L.; Delgado, A.; Dewil, S.; Reis, F.; Velar, C.M.; Corteline, M.E.D.; Cecatto, R.B.; Putrino, D.; Imamura, M.; Battistella, L.R.; et al. Safety and Feasibility of Outpatient Rehabilitation in Patients With Secondary Bone Cancer: A Preliminary Study. Rehabil. Oncol. 2021, 39, E42. [Google Scholar] [CrossRef]
- Zopf, E.M.; Newton, R.U.; Taaffe, D.R.; Spry, N.; Cormie, P.; Joseph, D.; Chambers, S.K.; Baumann, F.T.; Bloch, W.; Galvão, D.A. Associations between Aerobic Exercise Levels and Physical and Mental Health Outcomes in Men with Bone Metastatic Prostate Cancer: A Cross-Sectional Investigation. Eur. J. Cancer Care 2017, 26, e12575. [Google Scholar] [CrossRef]
- Bourke, L.; Gilbert, S.; Hooper, R.; Steed, L.A.; Joshi, M.; Catto, J.W.F.; Saxton, J.M.; Rosario, D.J. Lifestyle Changes for Improving Disease-Specific Quality of Life in Sedentary Men on Long-Term Androgen-Deprivation Therapy for Advanced Prostate Cancer: A Randomised Controlled Trial. Eur. Urol. 2014, 65, 865–872. [Google Scholar] [CrossRef]
- Cheville, A.L.; Moynihan, T.; Herrin, J.; Loprinzi, C.; Kroenke, K. Effect of Collaborative Telerehabilitation on Functional Impairment and Pain Among Patients With Advanced-Stage Cancer: A Randomized Clinical Trial. JAMA Oncol. 2019, 5, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.K.; Dorff, T.B.; Todd Schroeder, E.; Lane, C.J.; Gross, M.E.; Dieli-Conwright, C.M. Impact of Resistance Training on Body Composition and Metabolic Syndrome Variables during Androgen Deprivation Therapy for Prostate Cancer: A Pilot Randomized Controlled Trial. BMC Cancer 2018, 18, 368. [Google Scholar] [CrossRef]
- Scott, J.M.; Iyengar, N.M.; Nilsen, T.S.; Michalski, M.; Thomas, S.M.; Herndon, J., 2nd; Sasso, J.; Yu, A.; Chandarlapaty, S.; Dang, C.T.; et al. Feasibility, Safety, and Efficacy of Aerobic Training in Pretreated Patients with Metastatic Breast Cancer: A Randomized Controlled Trial. Cancer 2018, 124, 2552–2560. [Google Scholar] [CrossRef] [PubMed]
- Solheim, T.S.; Laird, B.J.A.; Balstad, T.R.; Stene, G.B.; Bye, A.; Johns, N.; Pettersen, C.H.; Fallon, M.; Fayers, P.; Fearon, K.; et al. A Randomized Phase II Feasibility Trial of a Multimodal Intervention for the Management of Cachexia in Lung and Pancreatic Cancer. J. Cachexia Sarcopenia Muscle 2017, 8, 778–788. [Google Scholar] [CrossRef] [PubMed]
- Uster, A.; Ruehlin, M.; Mey, S.; Gisi, D.; Knols, R.; Imoberdorf, R.; Pless, M.; Ballmer, P.E. Effects of Nutrition and Physical Exercise Intervention in Palliative Cancer Patients: A Randomized Controlled Trial. Clin. Nutr. 2018, 37, 1202–1209. [Google Scholar] [CrossRef]
- Uth, J.; Hornstrup, T.; Schmidt, J.F.; Christensen, J.F.; Frandsen, C.; Christensen, K.B.; Helge, E.W.; Brasso, K.; Rørth, M.; Midtgaard, J.; et al. Football Training Improves Lean Body Mass in Men with Prostate Cancer Undergoing Androgen Deprivation Therapy. Scand. J. Med. Sci. Sport. 2014, 24 (Suppl. S1), 105–112. [Google Scholar] [CrossRef]
- Villumsen, B.R.; Jorgensen, M.G.; Frystyk, J.; Hørdam, B.; Borre, M. Home-Based “exergaming” Was Safe and Significantly Improved 6-Min Walking Distance in Patients with Prostate Cancer: A Single-Blinded Randomised Controlled Trial. BJU Int. 2019, 124, 600–608. [Google Scholar] [CrossRef]
- Sprave, T.; Rosenberger, F.; Verma, V.; Förster, R.; Bruckner, T.; Schlampp, I.; Bostel, T.; Welzel, T.; Akbaba, S.; Rackwitz, T.; et al. Paravertebral Muscle Training in Patients with Unstable Spinal Metastases Receiving Palliative Radiotherapy: An Exploratory Randomized Feasibility Trial. Cancers 2019, 11, 1771. [Google Scholar] [CrossRef]
- Rief, H.; Akbar, M.; Keller, M.; Omlor, G.; Welzel, T.; Bruckner, T.; Rieken, S.; Häfner, M.F.; Schlampp, I.; Gioules, A.; et al. Quality of Life and Fatigue of Patients with Spinal Bone Metastases under Combined Treatment with Resistance Training and Radiation Therapy- a Randomized Pilot Trial. Radiat. Oncol. 2014, 9, 151. [Google Scholar] [CrossRef] [PubMed]
- Rief, H.; Welzel, T.; Omlor, G.; Akbar, M.; Bruckner, T.; Rieken, S.; Haefner, M.F.; Schlampp, I.; Gioules, A.; Debus, J. Pain Response of Resistance Training of the Paravertebral Musculature under Radiotherapy in Patients with Spinal Bone Metastases—A Randomized Trial. BMC Cancer 2014, 14, 485. [Google Scholar] [CrossRef] [PubMed]
- Coleman, R.E. Skeletal Complications of Malignancy. Cancer 1997, 80, 1588–1594. [Google Scholar] [CrossRef]
- Rief, H.; Petersen, L.C.; Omlor, G.; Akbar, M.; Bruckner, T.; Rieken, S.; Haefner, M.F.; Schlampp, I.; Förster, R.; Debus, J.; et al. The Effect of Resistance Training during Radiotherapy on Spinal Bone Metastases in Cancer Patients-a Randomized Trial. Radiother. Oncol. 2014, 112, 133–139. [Google Scholar] [CrossRef]
- Galvão, D.A.; Taaffe, D.R.; Chambers, S.K.; Fairman, C.M.; Spry, N.; Joseph, D.; Newton, R.U. Exercise Intervention and Sexual Function in Advanced Prostate Cancer: A Randomised Controlled Trial. BMJ Support. Palliat. Care 2022, 12, 29–32. [Google Scholar] [CrossRef]
- Jones, L.W.; Alfano, C.M. Exercise-Oncology Research: Past, Present, and Future. Acta Oncol. 2013, 52, 195–215. [Google Scholar] [CrossRef]
- Nadler, M.; Bainbridge, D.; Tomasone, J.; Cheifetz, O.; Juergens, R.A.; Sussman, J. Oncology Care Provider Perspectives on Exercise Promotion in People with Cancer: An Examination of Knowledge, Practices, Barriers, and Facilitators. Support. Care Cancer 2017, 25, 2297–2304. [Google Scholar] [CrossRef]
- Sheill, G.; Guinan, E.; Neill, L.O.; Hevey, D.; Hussey, J. The Views of Patients with Metastatic Prostate Cancer towards Physical Activity: A Qualitative Exploration. Support. Care Cancer 2018, 26, 1747–1754. [Google Scholar] [CrossRef]
- Horyna, A. Psychosocial Considerations for Patients with Metastatic Bone Disease. Metastatic Bone Dis. 2016, 14, 145–154. [Google Scholar]
- Dittus, K.L.; Gramling, R.E.; Ades, P.A. Exercise Interventions for Individuals with Advanced Cancer: A Systematic Review. Prev. Med. 2017, 104, 124–132. [Google Scholar] [CrossRef]
- Ward, P.; Randolph Hecht, J.; Wang, H.-J.; Dichmann, R.; Liem, A.K.D.; Chan, D.; Patel, R.; Hu, E.H.L.; Tchekmedyian, N.S.; Wainberg, Z.A.; et al. Physical Function and Quality of Life in Frail and/or Elderly Patients with Metastatic Colorectal Cancer Treated with Capecitabine and Bevacizumab: An Exploratory Analysis. J. Geriatr. Oncol. 2014, 5, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Winters-Stone, K.M.; Dobek, J.; Nail, L.; Bennett, J.A.; Leo, M.C.; Naik, A.; Schwartz, A. Strength Training Stops Bone Loss and Builds Muscle in Postmenopausal Breast Cancer Survivors: A Randomized, Controlled Trial. Breast Cancer Res. Treat. 2011, 127, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Lynch, M.E.; Brooks, D.; Mohanan, S.; Lee, M.J.; Polamraju, P.; Dent, K.; Bonassar, L.J.; van der Meulen, M.C.H.; Fischbach, C. In Vivo Tibial Compression Decreases Osteolysis and Tumor Formation in a Human Metastatic Breast Cancer Model. J. Bone Miner. Res. 2013, 28, 2357–2367. [Google Scholar] [CrossRef] [PubMed]
- Vehmanen, L.; Sievänen, H.; Kellokumpu-Lehtinen, P.; Nikander, R.; Huovinen, R.; Ruohola, J.; Penttinen, H.M.; Utriainen, M.; Tokola, K.; Blomqvist, C.; et al. Five-Year Follow-up Results of Aerobic and Impact Training on Bone Mineral Density in Early Breast Cancer Patients. Osteoporos. Int. 2021, 32, 473–482. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duong, H.; Walker, M.; Maugham-Macan, M. Exercise Intervention for Bone Metastasis: Safety, Efficacy and Method of Delivery. Cancers 2023, 15, 1786. https://doi.org/10.3390/cancers15061786
Duong H, Walker M, Maugham-Macan M. Exercise Intervention for Bone Metastasis: Safety, Efficacy and Method of Delivery. Cancers. 2023; 15(6):1786. https://doi.org/10.3390/cancers15061786
Chicago/Turabian StyleDuong, Huong, Meegan Walker, and Michelle Maugham-Macan. 2023. "Exercise Intervention for Bone Metastasis: Safety, Efficacy and Method of Delivery" Cancers 15, no. 6: 1786. https://doi.org/10.3390/cancers15061786
APA StyleDuong, H., Walker, M., & Maugham-Macan, M. (2023). Exercise Intervention for Bone Metastasis: Safety, Efficacy and Method of Delivery. Cancers, 15(6), 1786. https://doi.org/10.3390/cancers15061786