
A Scoping Review and a Taxonomy to Assess the Impact of Mobile Apps on Cancer Care Management


 , and
, and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection and Data Extraction
2.4. Taxonomy
3. Results
3.1. Scoping Review
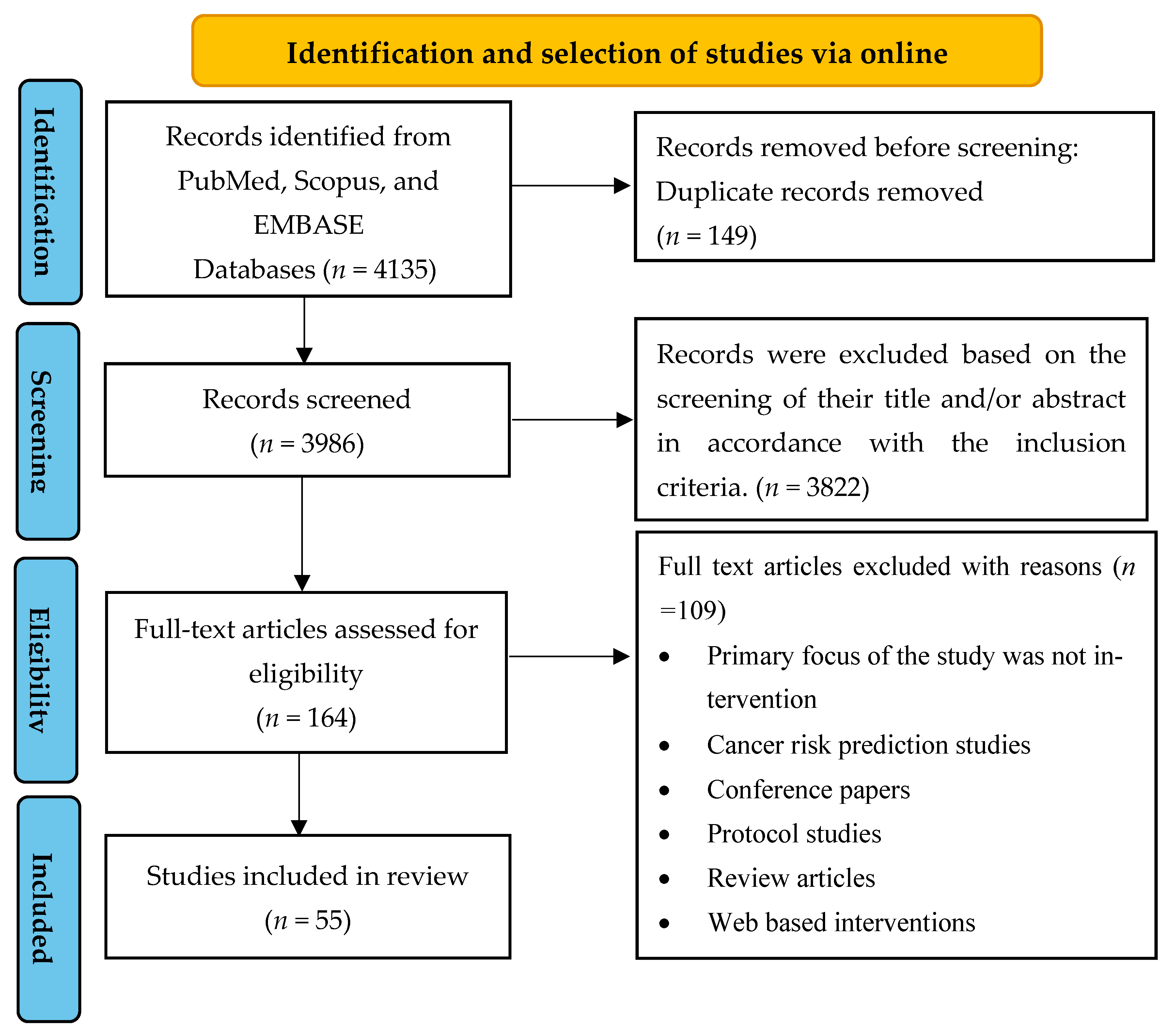
3.1.1. Study Selection
3.1.2. General Characteristics of the Studies
3.1.3. Characteristics of Research Participants
3.1.4. Measurement Tools
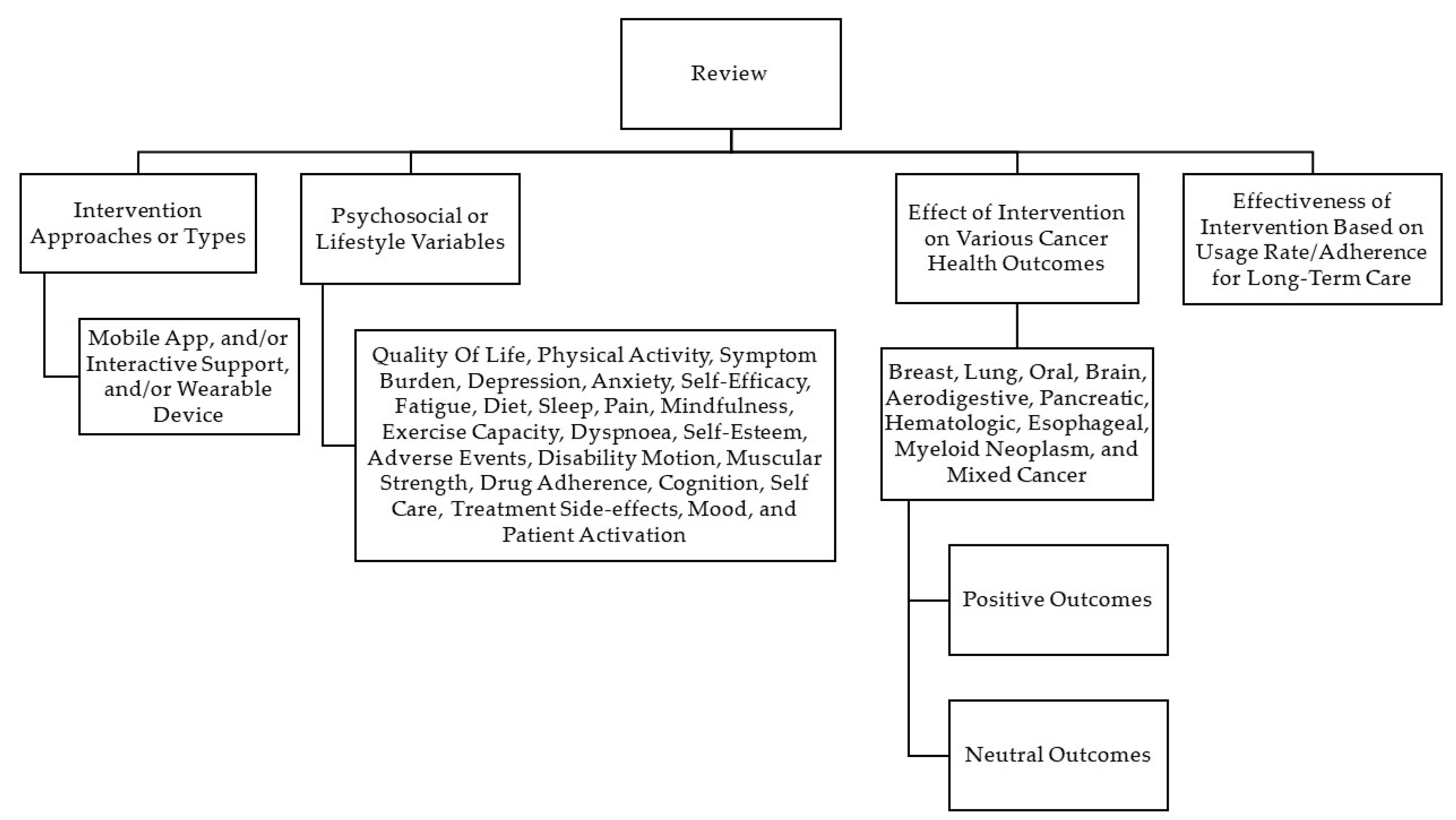
3.2. Categorisation of Studies
3.2.1. Interventional Approaches/Types
3.2.2. Psychosocial/Lifestyle Variables Assessed
3.2.3. Effects of Interventions on Various Cancer Health Outcomes

{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country | Cancer Type | Sample Size | Study Design | Gender (%) Mean Age (Years) | Mobile App and/or Interactive Support and/or Wearables Device | Study Focus | Study Duration | Improvements in Health Outcomes |
|---|---|---|---|---|---|---|---|---|
| Egbring et al., 2016 [18] Switzerland | Breast Cancer | 139 | RCT | 100% females 53 (yrs) | Mobile app + interactive support | Daily functional activity and adverse events | 6 weeks | Daily functional activity and patient awareness of severity of symptoms |
| Lozano et al., 2019 [37] Spain | Breast Cancer | 80 | Prospective test-retest quasi-experimental study | 100% females 51.80 (yrs) | Mobile app only | QoL, physical activity, body composition and physical activity motivation | 8 weeks | QoL, physical activity and body weight |
| Allicock et al., 2021 [38] USA Ballcock | Breast Cancer | 22 | Feasibility study | 100% females 52.23 (yrs) | Mobile app + wearable device | Physical activity and diet | 8 weeks | Physical activity and diet habits |
| Yanez et al., 2020 [39] USA | Breast Cancer | 78 | RCT | 100% females 52.54 (yrs) | Mobile app + interactive support | QoL, symptom burden (breast cancer related) | 6 weeks | Breast cancer well-being (disease specific QoL) and symptom burden |
| Cinar et al., 2021 [40] Turkey | Breast Cancer | 64 | RCT | 100% females 45.7 (yrs) | Mobile app + interactive support | QoL, distress | 12 weeks | QoL and distress |
| Handa et al., 2020 [29] Japan | Breast Cancer | 95 | RCT | 100% females 49.9 (yrs) | Mobile app only | QoL (Anxiety and depression), health literacy | 12 weeks | No improvement |
| Uhm et al., 2017 [16] South Korea | Breast Cancer | 339 | Quasi-experimental study | 100% females 50.3 (yrs) | Mobile app + wearable device | QoL, physical measurements and self-reported physical activity | 12 weeks | QoL and physical activity |
| XU et al., 2021 [41] China | Breast Cancer | 126 | RCT | 100% females 47.93 (yrs) | Mobile app + interactive support | QoL (anxiety and depression), discomfort symptoms and self-efficacy | 16 weeks | QoL and self-efficacy |
| Ghanbari et al., 2021 [42] Iran | Breast Cancer | 82 | RCT | 100% females 46.45 (yrs) | Mobile app + interactive support | Anxiety and self-esteem | 4 weeks | Anxiety and self-esteem |
| Sheean et al., 2021 [43] USA | Breast Cancer | 35 | RCT | 100% females 55.11 (yrs) | Mobile app + interactive support | QoL, symptom burden, lifestyle behaviours (nutrition and physical activity) | 12 weeks | QoL and physical activity |
| Kuhar et al., 2020 [44] Slovenia | Breast Cancer | 91 | Non-randomized controlled prospective cohort Study | 100% females 51.7 (yrs) | Mobile app only | QoL | Throughout chemotherapy | QoL |
| Lozano-Lozano et al., 2020 [45] Spain | Breast Cancer | 78 | RCT | 100% females 52.5 (yrs) | Mobile app only | QoL, disability, motion, muscular strength | 8 weeks | QoL, disability, motion and muscular strength |
| Kim et al., 2018 [46] South Korea | Breast Cancer | 72 | RCT | 100% females 51 (yrs) | Mobile app only | QoL, drug adherence, side effects depression and anxiety | 3 weeks | QoL, compliance to medication and side effects |
| Rosen et al., 2018 [47] USA | Breast Cancer | 84 | RCT | 100% females 53 (yrs) | Mobile app only | QoL and mindfulness | 8 weeks | QoL and mindfulness |
| Lengacher et al., 2018 [48] USA | Breast Cancer | 13 | Pilot Study | 100% females 57 (yrs) | Mobile app only | QoL, fatigue, depression, pain, sleep quality, stress, FOR, anxiety, cognition and mindfulness | 6 weeks | QoL, fatigue, depression, pain, sleep quality, anxiety, stress, FOR, anxiety, cognition and mindfulness |
| Ferrante et al., 2020 [49] USA | Breast Cancer | 35 | RCT | 100% females 61.54 (yrs) | Mobile app + wearable device | QoL, weight management, diet and physical activity, cardiopulmonary fitness, social cognitive theory variables and anthropometric outcomes | 24 weeks | QoL, waist circumference, healthy eating and calorie reduction techniques |
| Hou et al., 2020 [50] Taiwan | Breast Cancer | 112 | RCT | 100% females 42 (yrs) | Mobile app only | QoL | 12 weeks | QoL |
| Fjell et al., 2020 [51] Sweden | Breast Cancer | 149 | RCT | 100% females 49 (yrs) | Mobile app + interactive support | QoL and symptom burden | 18 weeks | QoL and symptom burden |
| Öztürk et al., 2021 [52] Turkey | Breast Cancer | 57 | RCT | 100% females 51.44 (yrs) | Mobile app only | QoL and symptom burden | 8 weeks | QoL and symptom burden |
| Bandani-Susan et al., 2021 [53] Iran | Breast Cancer | 38 | RCT | 100% females 46.34 (yrs) | Mobile app only | Cancer-related fatigue | 7 weeks | Fatigue |
| Mendoza et al., 2017 [27] USA | Mixed Cancer | 59 | RCT | 59.3% females 16.6 (yrs) | Mobile app + wearable device + interactive support | QoL and physical activity | 10 weeks | No improvement |
| Blair et al.,2021 [54] USA | Mixed Cancer | 54 | RCT | 55% females 69.6 (yrs) | Mobile app + wearable device + Interactive support | QoL and physical activity | 13 weeks | Physical activity |
| Kubo et al., 2019 [55] USA | Mixed Cancer | 97 | RCT | 69% females 59 (yrs) | Mobile app only | QoL, fatigue, distress, sleep, mindfulness, pain, anxiety and depression, and posttraumatic growth | 8 weeks | QoL |
| Puszkiewicz et al., 2016 [56] UK | Mixed Cancer | 11 | Pre–post study | 82% females 45 (yrs) | Mobile app only | QoL, physical activity, well-being, fatigue, sleep, anxiety and depression | 6 weeks | Physical activity and sleep quality |
| Yang et al., 2019 [57] China | Mixed Cancer | 58 | RCT | 34% females 52.53 (yrs) | Mobile app only | QoL and pain | 4 weeks | QoL and pain |
| Mikolasek et al., 2021 [58] Switzerland | Mixed Cancer | 100 | Feasibility study | 74% females 53.2 (yrs) | Mobile app only | QoL, anxiety, fatigue, distress, sleep and mindfulness | 20 weeks | QoL, anxiety, fatigue, distress, sleep disruptions and mindfulness |
| Walsh et al., 2021 [59] Ireland | Mixed Cancer | 123 | RCT | 86% females 57.42 (yrs) | Mobile app + Wearable device | QoL, fatigue, self-efficacy, loneliness, exercise self-efficacy, social support for physical activity, functional exercise capacity, diet and physical activity | 12 weeks | BMI, waist circumference and physical activity |
| Poort et al., 2021 [30] USA | Mixed Cancer | 25 | Pilot study | 56% females 28 (yrs) | Mobile app only | QoL, self-efficacy for coping with cancer, self-efficacy for managing emotions and perceived emotional support | 12 weeks | No improvement |
| Robertson et al., 2020 [60] USA | Mixed Cancer | 78 | RCT | 91% females 55.1 (yrs) | Mobile app + wearable device | Physical activity | 16 weeks | Physical activity |
| Pappot et al., 2019 [12] Denmark | Mixed Cancer | 20 | Pre–post study | 70% females 25 (yrs) | Mobile app only | QoL | 6 weeks | QoL |
| Jibb et al., 2017 [28] Canada | Mixed Cancer | 38 | One-group baseline/poststudy | 43% females 14.2 (yrs) | Mobile app only | QoL, pain and self-efficacy | 4 weeks | QoL and pain |
| Livingston et al., 2020 [31] Australia | Mixed Cancer | 82 | RCT | 71% females 59.5 (yrs) | Mobile app only | Unmet psychological needs | 16 weeks | No improvement |
| Børøsund et al., 2020 [61] Norway | Mixed Cancer | 25 | Feasibility study | 84% females 48 (yrs) | Mobile app + interactive support | QoL, anxiety and depression, fatigue, stress | 8 weeks | QoL, anxiety, fatigue and stress |
| Ham et al., 2019 [62] South Korea | Mixed Cancer | 63 | RCT | 86% females 44.1 (yrs) | Mobile app only | QoL, depression and anxiety | 10 weeks | Depression and anxiety |
| Benze et al., 2019 [63] Germany | Mixed Cancer | 40 | Feasibility study | 70% females 57 (yrs) | Mobile app only | QoL, pain, distress and symptoms | 24 weeks | QoL and symptom burden |
| Greer et al., 2019 [64] USA | Mixed Cancer (high anxiety) | 145 | RCT | 74% females 56.45 (yrs) | Mobile app only | QoL, anxiety and depression | 12 weeks | QoL, anxiety and depression |
| Maguire et al., 2021 [65] Austria, Greece, Ireland, Norway and UK | Mixed Cancer | 829 | RCT | 82% females 52.4 (yrs) | Mobile app + interactive support | QoL, symptom burden, supportive care needs, work limitations, anxiety and self-efficacy | 18 weeks | QoL, symptom burden, anxiety and self-efficacy |
| Ormel et al., 2018 [66] Netherland | Mixed Cancer | 32 | RCT | 13% females 33.6 (yrs) | Mobile app only | Physical activity | 12 weeks | Physical activity |
| Krebs et al., 2019 [67] USA | Mixed Cancer | 38 | RCT | 71% females 57.11 (yrs) | Mobile app + interactive support | Smoking cessation | 4 weeks | Higher confidence to quit |
| Casillas et al., 2019 [68] USA | Mixed Cancer | 71 | RCT | 53% females 21 (yrs) | Mobile app + interactive support | Survivorship care knowledge and self-efficacy | 8 weeks | Survivorship care attitude and self-efficacy |
| Rico et al., 2020 [69] Brazil | Mixed Cancer | 87 | RCT | 56% females 45.2 (yrs) | Mobile app + interactive support | QoL side effects | 12 weeks | QoL (side effects) |
| Chung et al., 2022 [70] South Korea | Mixed Cancer | 41 | RCT | 80% females 41.78 (yrs) | Mobile app only | QoL and sleep quality | 10 weeks | Sleep quality |
| Merz et al., 2022 [33] USA | Mixed Cancer | 45 | RCT | 60% females | Mobile app only | QoL, utilization of supportive care services and patient activation (self-management of illnesses) | 12 weeks | No Improvement |
| Sundberg et al., 2017 [71] Sweden | Prostate cancer | 130 | Feasibility study | 100% males 69 (yrs) | Mobile app + interactive support | QoL and symptom burden | 5–8 weeks | QoL and symptom burden |
| Lee at al., 2019 [72] South Korea | Prostate cancer | 100 | Randomized open-label trial | 100% males 69.44 (yrs) | Mobile app + wearable device+ interactive support | Physical functions | 12 ± 1 weeks | Physical functions |
| Ji et al., 2019 [73] South Korea | Non-small cell lung cancer | 64 | Prospective clinical trial | 70% males 59.23 (yrs) | Mobile app + wearable Device | QoL, exercise capacity and dyspnea | 12 weeks | QoL, exercise capacity and dyspnea |
| Park et al., 2019 [74] South Korea | Lung cancer | 90 | Pilot study | 46% males 55.1 (yrs) | Mobile app + wearable + interactive support | QoL, exercise capacity and symptom management | 12 weeks | Exercise capacity and symptom management. |
| Wang et al., 2020 [75] Taiwan | Oral cancer | 100 | Quasi experimental | 92% males 57.01 (yrs) | Mobile app + interactive support | QoL (symptoms), cancer needs | 12 weeks | QoL and cancer care needs |
| De Tommasi et al., 2020 [76] New Zealand | Brain tumour | 10 | Feasibility study | 60% females 53.8 (yrs) | Mobile app only | QoL (illness-related), psychological distress and mindfulness capacity | 8 weeks | QoL and mindfulness |
| Rettig et al., 2018 [77] USA | Aerodigestive cancer | 29 | RCT | 62% males 55 (yrs) | Mobile app + interactive support | Smoking abstinence | 8 weeks | Smoking abstinence |
| Gustavell et al., 2019 [32] Sweden | Pancreatic and Periampullary cancer | 26 | RCT | 61% males 66.5 (yrs) | Mobile app only | QoL, self-care activity | 32 weeks | No Improvement |
| Keum et al., 2021 [78] South Korea | Pancreatic cancer | 33 | RCT | 63% males 61.5 (yrs) | Mobile app + interactive support | QoL and nutrition | 12 weeks | QoL and nutrition |
| Chow et al., 2021 [19] USA | Hematologic cancer | 41 | RCT | 48.8% females 45.1 (yrs) | Mobile app + wearable + interactive support | QoL, physical activity, self-efficacy and diet | 16 weeks | No improvement |
| Loh et al., 2022 [35] USA | Myeloid neoplasm | 22 | Pilot study | 68% males 72 (yrs) | Mobile app + wearable + interactive support | QoL, physical activity, fatigue and mood | 8–12 weeks (two cycles of chemotherapy) | No improvement |
| Yang et al., 2021 [36] South Korea | Oesophageal cancer | 30 | Pilot study | 100% males 59 (yrs) | Mobile app + interactive support | Physical activity and nutrition | 8 weeks | No improvement |
3.2.4. Effectiveness of Mobile-App Based Interventions Based on the Usage Rate/Adherence for Cancer Care Management
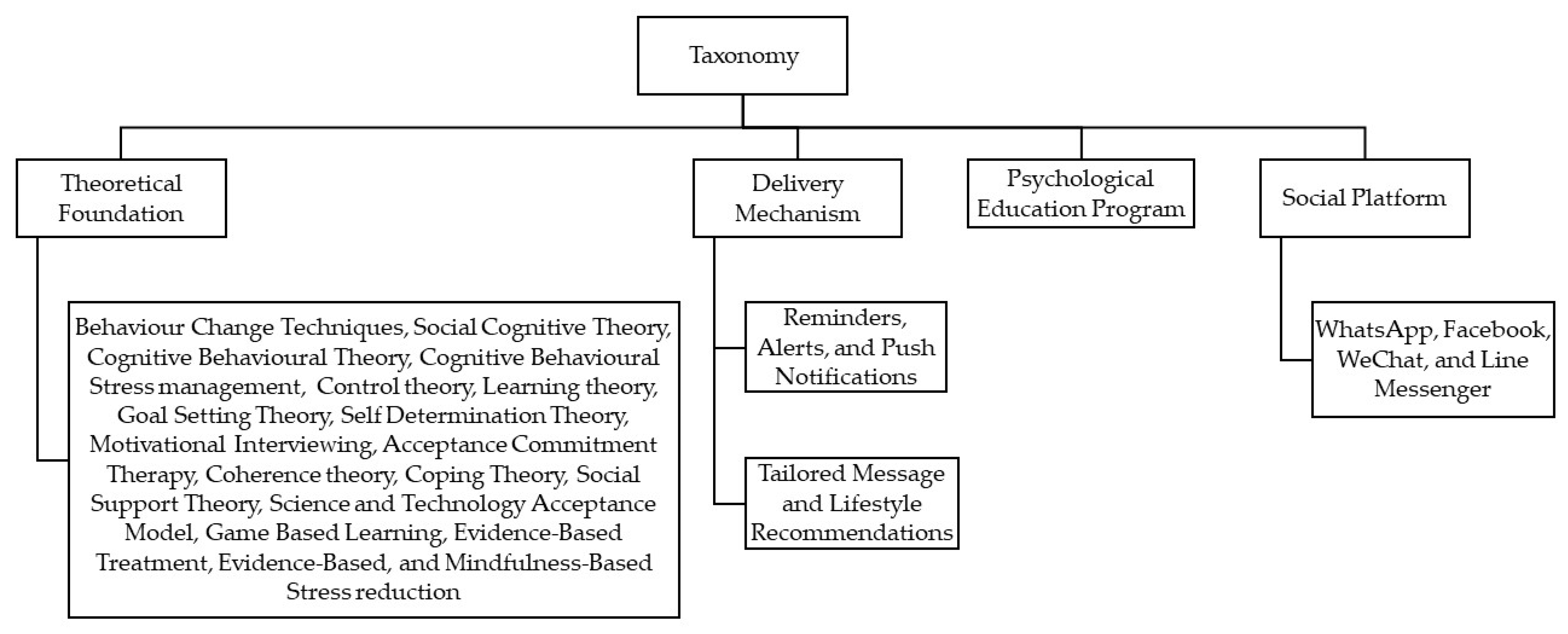
3.3. Taxonomy
3.3.1. Theoretical Foundations or Behavioural Techniques
3.3.2. Delivery Mechanism (Reminders/Alerts or Tailored Messages/Lifestyle Recommendations)
3.3.3. Psychoeducational Program
3.3.4. Various Social Platforms
4. Discussion
4.1. Summary and Findings
4.2. Study Strengths
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Foster, C. The Need for Quality Self-Management Support in Cancer Care. BMJ Qual. Saf. 2021, 31, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Kutikov, A.; Weinberg, D.S.; Edelman, M.J.; Horwitz, E.M.; Uzzo, R.G.; Fisher, R.I. A war on two fronts: Cancer care in the time of COVID-19. Ann. Intern. Med. 2020, 172, 756–758. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Bluethmann, S.M.; Mariotto, A.B.; Rowland, J.H. Anticipating the “silver tsunami”: Prevalence trajectories and comorbidity burden among older cancer survivors in the United States. Cancer Epidemiol. Biomark. Prev. 2016, 25, 1029–1036. [Google Scholar] [CrossRef]
- McCorkle, R.; Ercolano, E.; Lazenby, M.; Schulman-Green, D.; Schilling, L.S.; Lorig, K.; Wagner, E.H. Self-management: Enabling and empowering patients living with cancer as a chronic illness. CA: A Cancer J. Clin. 2011, 61, 50–62. [Google Scholar] [CrossRef]
- D’egidio, V.; Sestili, C.; Mancino, M.; Sciarra, I.; Cocchiara, R.; Backhaus, I.; Mannocci, A.; De Luca, A.; Frusone, F.; Monti, M. Counseling interventions delivered in women with breast cancer to improve health-related quality of life: A systematic review. Qual. Life Res. 2017, 26, 2573–2592. [Google Scholar] [CrossRef]
- Sweegers, M.G.; Altenburg, T.M.; Chinapaw, M.J.; Kalter, J.; Verdonck-de Leeuw, I.M.; Courneya, K.S.; Newton, R.U.; Aaronson, N.K.; Jacobsen, P.B.; Brug, J. Which exercise prescriptions improve quality of life and physical function in patients with cancer during and following treatment? A systematic review and meta-analysis of randomised controlled trials. Br. J. Sport. Med. 2018, 52, 505–513. [Google Scholar] [CrossRef]
- Rummans, T.A.; Clark, M.M.; Sloan, J.A.; Frost, M.H.; Bostwick, J.M.; Atherton, P.J.; Johnson, M.E.; Gamble, G.; Richardson, J.; Brown, P. Impacting quality of life for patients with advanced cancer with a structured multidisciplinary intervention: A randomized controlled trial. J. Clin. Oncol. 2006, 24, 635–642. [Google Scholar] [CrossRef]
- Howell, D.; Mayer, D.K.; Fielding, R.; Eicher, M.; Verdonck-de Leeuw, I.M.; Johansen, C.; Soto-Perez-de-Celis, E.; Foster, C.; Chan, R.; Alfano, C.M. Management of cancer and health after the clinic visit: A call to action for self-management in cancer care. JNCI: J. Natl. Cancer Inst. 2021, 113, 523–531. [Google Scholar] [CrossRef]
- Cooley, M.E.; Nayak, M.M.; Abrahm, J.L.; Braun, I.M.; Rabin, M.S.; Brzozowski, J.; Lathan, C.; Berry, D.L. Patient and caregiver perspectives on decision support for symptom and quality of life management during cancer treatment: Implications for e H ealth. Psycho-Oncol. 2017, 26, 1105–1112. [Google Scholar] [CrossRef]
- Bertucci, F.; Corroller-Soriano, L.; Monneur-Miramon, A.; Moulin, J.-F.; Fluzin, S.; Maraninchi, D.; Gonçalves, A. Outpatient cancer care delivery in the context of e-oncology: A french perspective on “cancer outside the hospital walls”. Cancers 2019, 11, 219. [Google Scholar] [CrossRef] [PubMed]
- Pappot, H.; Taarnhøj, G.A.; Elsbernd, A.; Hjerming, M.; Hanghøj, S.; Jensen, M.; Boisen, K.A. Health-related quality of life before and after use of a smartphone app for adolescents and young adults with cancer: Pre-post interventional study. JMIR Mhealth Uhealth 2019, 7, e13829. [Google Scholar] [CrossRef]
- El Shafie, R.A.; Weber, D.; Bougatf, N.; Sprave, T.; Oetzel, D.; Huber, P.E.; Debus, J.; Nicolay, N.H. Supportive care in radiotherapy based on a mobile app: Prospective multicenter survey. JMIR Mhealth Uhealth 2018, 6, e10916. [Google Scholar] [CrossRef] [PubMed]
- Faria, E.T.; Ghobad, P.C.; Alves, L.Y.M.; Dos Reis, P.E.D. A Mobile App (AMOR Mama) for Women With Breast Cancer Undergoing Radiation Therapy: Functionality and Usability Study. J. Med. Internet Res. 2021, 23, e24865. [Google Scholar]
- Davis, S.W.; Oakley-Girvan, I. mHealth education applications along the cancer continuum. J. Cancer Educ. 2015, 30, 388–394. [Google Scholar] [CrossRef]
- Uhm, K.E.; Yoo, J.S.; Chung, S.H.; Lee, J.D.; Lee, I.; Kim, J.I.; Lee, S.K.; Nam, S.J.; Park, Y.H.; Lee, J.Y. Effects of exercise intervention in breast cancer patients: Is mobile health (mHealth) with pedometer more effective than conventional program using brochure? Breast Cancer Res. Treat. 2017, 161, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Im, E.-O.; Ji, X.; Kim, S.; Chee, E.; Bao, T.; Mao, J.J.; Chee, W. Challenges in a technology-based cancer pain management program among Asian American breast cancer survivors. Comput. Inform. Nurs. CIN 2019, 37, 243. [Google Scholar] [CrossRef]
- Egbring, M.; Far, E.; Roos, M.; Dietrich, M.; Brauchbar, M.; Kullak-Ublick, G.A.; Trojan, A. A mobile app to stabilize daily functional activity of breast cancer patients in collaboration with the physician: A randomized controlled clinical trial. J. Med. Internet Res. 2016, 18, e238. [Google Scholar] [CrossRef] [PubMed]
- Chow, P.I.; Showalter, S.L.; Gerber, M.; Kennedy, E.M.; Brenin, D.; Mohr, D.C.; Lattie, E.G.; Gupta, A.; Ocker, G.; Cohn, W.F. Use of mental health apps by patients with breast cancer in the united states: Pilot pre-post study. JMIR Cancer 2020, 6, e16476. [Google Scholar] [CrossRef]
- Botha, A.; Weiss, M.; Herselman, M. Towards a taxonomy of mHealth. In Proceedings of the 2018 International Conference on Advances in Big Data, Computing and Data Communication Systems (icABCD), Durban, South Africa, 6–7 August 2018; pp. 1–9. [Google Scholar]
- Bashshur, R.; Shannon, G.; Krupinski, E.; Grigsby, J. The taxonomy of telemedicine. Telemed. E-Health 2011, 17, 484–494. [Google Scholar] [CrossRef]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27, 379. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Fadhil, A.; Lange, J.P.; Reiterer, H. Integrating Taxonomies Into Theory-Based Digital Health Interventions for Behavior Change: A Holistic Framework. JMIR Res. Protoc. 2019, 8, e8055. [Google Scholar] [CrossRef]
- Dahlke, D.V.; Fair, K.; Hong, Y.A.; Beaudoin, C.E.; Pulczinski, J.; Ory, M.G. Apps seeking theories: Results of a study on the use of health behavior change theories in cancer survivorship mobile apps. JMIR Mhealth Uhealth 2015, 3, e3861. [Google Scholar]
- Munn, Z.; Peters, M.D.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Mendoza, J.A.; Baker, K.S.; Moreno, M.A.; Whitlock, K.; Abbey-Lambertz, M.; Waite, A.; Colburn, T.; Chow, E.J. A Fitbit and Facebook mHealth intervention for promoting physical activity among adolescent and young adult childhood cancer survivors: A pilot study. Pediatr. Blood Cancer 2017, 64, e26660. [Google Scholar] [CrossRef] [PubMed]
- Jibb, L.A.; Stevens, B.J.; Nathan, P.C.; Seto, E.; Cafazzo, J.A.; Johnston, D.L.; Hum, V.; Stinson, J.N. Implementation and preliminary effectiveness of a real-time pain management smartphone app for adolescents with cancer: A multicenter pilot clinical study. Pediatr. Blood Cancer 2017, 64, e26554. [Google Scholar] [CrossRef] [PubMed]
- Handa, S.; Okuyama, H.; Yamamoto, H.; Nakamura, S.; Kato, Y. Effectiveness of a smartphone application as a support tool for patients undergoing breast cancer chemotherapy: A randomized controlled trial. Clin. Breast Cancer 2020, 20, 201–208. [Google Scholar] [CrossRef]
- Poort, H.; Ryan, A.; MacDougall, K.; Malinowski, P.; MacDonald, A.; Markin, Z.; Pirl, W.; Greer, J.; Fasciano, K. Feasibility and Acceptability of a Mobile Phone App Intervention for Coping With Cancer as a Young Adult: Pilot Trial and Thematic Analysis. J. Med. Internet Res. 2021, 23, e25069. [Google Scholar] [CrossRef]
- Livingston, P.M.; Heckel, L.; Orellana, L.; Ashley, D.; Ugalde, A.; Botti, M.; Pitson, G.; Woollett, A.; Chambers, S.K.; Parente, P. Outcomes of a randomized controlled trial assessing a smartphone Application to reduce unmet needs among people diagnosed with CancEr (ACE). Cancer Med. 2020, 9, 507–516. [Google Scholar] [CrossRef]
- Gustavell, T.; Sundberg, K.; Segersvärd, R.; Wengström, Y.; Langius-Eklöf, A. Decreased symptom burden following surgery due to support from an interactive app for symptom management for patients with pancreatic and periampullary cancer. Acta Oncol. 2019, 58, 1307–1314. [Google Scholar] [CrossRef]
- Merz, A.; Mohamed, A.; Corbett, C.; Herring, K.; Hildenbrand, J.; Locke, S.C.; Patierno, S.; Troy, J.; Wolf, S.; Zafar, S.Y. A single-site pilot feasibility randomized trial of a supportive care mobile application intervention for patients with advanced cancer and caregivers. Support. Care Cancer 2022, 30, 7853–7861. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.J.; Doody, D.R.; Di, C.; Armenian, S.H.; Baker, K.S.; Bricker, J.B.; Gopal, A.K.; Hagen, A.M.; Ketterl, T.G.; Lee, S.J. Feasibility of a behavioral intervention using mobile health applications to reduce cardiovascular risk factors in cancer survivors: A pilot randomized controlled trial. J. Cancer Surviv. 2021, 15, 554–563. [Google Scholar] [CrossRef] [PubMed]
- Loh, K.P.; Sanapala, C.; Watson, E.E.; Jensen-Battaglia, M.; Janelsins, M.C.; Klepin, H.D.; Schnall, R.; Culakova, E.; Vertino, P.; Susiarjo, M. A single-arm pilot study of a mobile health exercise intervention (GO-EXCAP) in older patients with myeloid neoplasms. Blood Adv. 2022, 6, 3850–3860. [Google Scholar] [CrossRef]
- Yang, K.; Oh, D.; Noh, J.M.; Yoon, H.G.; Sun, J.-M.; Kim, H.K.; Zo, J.I.; Shim, Y.M.; Ko, H.; Lee, J. Feasibility of an interactive health coaching mobile app to prevent malnutrition and muscle loss in esophageal cancer patients receiving neoadjuvant concurrent chemoradiotherapy: Prospective pilot study. J. Med. Internet Res. 2021, 23, e28695. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Lozano, M.; Cantarero-Villanueva, I.; Martin-Martin, L.; Galiano-Castillo, N.; Sanchez, M.-J.; Fernández-Lao, C.; Postigo-Martin, P.; Arroyo-Morales, M. A mobile system to improve quality of life via energy balance in breast cancer survivors (BENECA mHealth): Prospective test-retest Quasiexperimental feasibility study. JMIR Mhealth Uhealth 2019, 7, e14136. [Google Scholar] [CrossRef] [PubMed]
- Allicock, M.; Kendzor, D.; Sedory, A.; Gabriel, K.P.; Swartz, M.D.; Thomas, P.; Yudkin, J.S.; Rivers, A. A Pilot and Feasibility Mobile Health Intervention to Support Healthy Behaviors in African American Breast Cancer Survivors. J. Racial Ethn. Health Disparities 2021, 8, 157–165. [Google Scholar] [CrossRef]
- Yanez, B.; Oswald, L.B.; Baik, S.H.; Buitrago, D.; Iacobelli, F.; Perez-Tamayo, A.; Guitelman, J.; Penedo, F.J.; Buscemi, J. Brief culturally informed smartphone interventions decrease breast cancer symptom burden among Latina breast cancer survivors. Psycho -Oncol. 2020, 29, 195–203. [Google Scholar] [CrossRef]
- Çınar, D.; Karadakovan, A.; Erdoğan, A.P. Effect of mobile phone app-based training on the quality of life for women with breast cancer. Eur. J. Oncol. Nurs. 2021, 52, 101960. [Google Scholar] [CrossRef]
- Xu, Y.F.; Xu, X.F.; Song, K.; Qiu, C.; Zhang, X.; Di, H. Effects of Extended Care Based on the WeChat Platform on Self-Efficacy and Quality of Life of Postoperative Breast Cancer Patients. Indian J. Pharm. Sci. 2021, 83, 23–30. [Google Scholar] [CrossRef]
- Ghanbari, E.; Yektatalab, S.; Mehrabi, M. Effects of Psychoeducational Interventions Using Mobile Apps and Mobile-Based Online Group Discussions on Anxiety and Self-Esteem in Women With Breast Cancer: Randomized Controlled Trial. JMIR Mhealth Uhealth 2021, 9, e19262. [Google Scholar] [CrossRef]
- Sheean, P.; Matthews, L.; Visotcky, A.; Banerjee, A.; Moosreiner, A.; Kelley, K.; Chitambar, C.R.; Papanek, P.E.; Stolley, M. Every Day Counts: A randomized pilot lifestyle intervention for women with metastatic breast cancer. Breast Cancer Res. Treat. 2021, 187, 729–741. [Google Scholar] [CrossRef] [PubMed]
- Kuhar, C.G.; Cepeda, T.G.; Kovač, T.; Kukar, M.; Gorenjec, N.R. Mobile app for symptom management and associated quality of life during systemic treatment in early stage breast cancer: Nonrandomized controlled prospective cohort study. JMIR Mhealth Uhealth 2020, 8, e17408. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Lozano, M.; Martín-Martín, L.; Galiano-Castillo, N.; Fernández-Lao, C.; Cantarero-Villanueva, I.; López-Barajas, I.B.; Arroyo-Morales, M. Mobile health and supervised rehabilitation versus mobile health alone in breast cancer survivors: Randomized controlled trial. Ann. Phys. Rehabil. Med. 2020, 63, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, S.M.; Shin, H.; Jang, J.-S.; Kim, Y.I.; Han, D.H. A mobile game for patients with breast cancer for chemotherapy self-management and quality-of-life improvement: Randomized controlled trial. J. Med. Internet Res. 2018, 20, e9559. [Google Scholar] [CrossRef]
- Rosen, K.D.; Paniagua, S.M.; Kazanis, W.; Jones, S.; Potter, J.S. Quality of life among women diagnosed with breast Cancer: A randomized waitlist controlled trial of commercially available mobile app-delivered mindfulness training. Psycho-oncology 2018, 27, 2023–2030. [Google Scholar] [CrossRef]
- Lengacher, C.A.; Reich, R.R.; Ramesar, S.; Alinat, C.B.; Moscoso, M.; Cousin, L.; Marino, V.R.; Elias, M.N.; Paterson, C.L.; Pleasant, M.L. Feasibility of the mobile mindfulness-based stress reduction for breast cancer (mMBSR (BC)) program for symptom improvement among breast cancer survivors. Psycho -Oncol. 2018, 27, 524–531. [Google Scholar] [CrossRef]
- Ferrante, J.M.; Devine, K.A.; Bator, A.; Rodgers, A.; Ohman-Strickland, P.A.; Bandera, E.V.; Hwang, K.O. Feasibility and potential efficacy of commercial mHealth/eHealth tools for weight loss in African American breast cancer survivors: Pilot randomized controlled trial. Transl. Behav. Med. 2020, 10, 938–948. [Google Scholar] [CrossRef]
- Hou, I.-C.; Lin, H.-Y.; Shen, S.-H.; Chang, K.-J.; Tai, H.-C.; Tsai, A.-J.; Dykes, P.C. Quality of Life of Women After a First Diagnosis of Breast Cancer Using a Self-Management Support mHealth App in Taiwan: Randomized Controlled Trial. JMIR Mhealth Uhealth 2020, 8, e17084. [Google Scholar] [CrossRef]
- Fjell, M.; Langius-Eklöf, A.; Nilsson, M.; Wengström, Y.; Sundberg, K. Reduced symptom burden with the support of an interactive app during neoadjuvant chemotherapy for breast cancer–A randomized controlled trial. Breast 2020, 51, 85–93. [Google Scholar] [CrossRef]
- Öztürk, E.S.; Kutlutürkan, S. The Effect of the Mobile Application-Based Symptom Monitoring Process on the Symptom Control and Quality of Life in Breast Cancer Patients. Semin. Oncol. Nurs. 2021, 37, 151161. [Google Scholar] [CrossRef]
- Bandani-Susan, B.; Montazeri, A.; Haghighizadeh, M.H.; Araban, M. The effect of mobile health educational intervention on body image and fatigue in breast cancer survivors: A randomized controlled trial. Irish J. Med. Sci. (1971) 2021, 191, 1599–1605. [Google Scholar] [CrossRef]
- Blair, C.K.; Harding, E.; Wiggins, C.; Kang, H.; Schwartz, M.; Tarnower, A.; Du, R.; Kinney, A.Y. A Home-Based Mobile Health Intervention to Replace Sedentary Time With Light Physical Activity in Older Cancer Survivors: Randomized Controlled Pilot Trial. JMIR Cancer 2021, 7, e18819. [Google Scholar] [CrossRef] [PubMed]
- Kubo, A.; Kurtovich, E.; McGinnis, M.; Aghaee, S.; Altschuler, A.; Quesenberry, C., Jr.; Kolevska, T.; Avins, A.L. A randomized controlled trial of mHealth mindfulness intervention for cancer patients and informal cancer caregivers: A feasibility study within an integrated health care delivery system. Integr. Cancer Ther. 2019, 18, 1534735419850634. [Google Scholar] [CrossRef] [PubMed]
- Puszkiewicz, P.; Roberts, A.L.; Smith, L.; Wardle, J.; Fisher, A. Assessment of cancer survivors’ experiences of using a publicly available physical activity mobile application. JMIR Cancer 2016, 2, e5380.1. [Google Scholar] [CrossRef]
- Yang, J.; Weng, L.; Chen, Z.; Cai, H.; Lin, X.; Hu, Z.; Li, N.; Lin, B.; Zheng, B.; Zhuang, Q. Development and testing of a mobile app for pain management among cancer patients discharged from hospital treatment: Randomized controlled trial. JMIR Mhealth Uhealth 2019, 7, e12542. [Google Scholar] [CrossRef]
- Mikolasek, M.; Witt, C.M.; Barth, J. Effects and implementation of a mindfulness and relaxation App for patients with cancer: Mixed methods feasibility study. JMIR Cancer 2021, 7, e16785. [Google Scholar] [CrossRef]
- Walsh, J.C.; Richmond, J.; Mc Sharry, J.; Groarke, A.; Glynn, L.; Kelly, M.G.; Harney, O.; Groarke, J.M. Examining the Impact of an mHealth Behavior Change Intervention With a Brief In-Person Component for Cancer Survivors With Overweight or Obesity: Randomized Controlled Trial. JMIR Mhealth Uhealth 2021, 9, e24915. [Google Scholar] [CrossRef]
- Robertson, M.C.; Lyons, E.J.; Liao, Y.; Baum, M.L.; Basen-Engquist, K.M. Gamified text messaging contingent on device-measured steps: Randomized feasibility study of a physical activity intervention for cancer survivors. JMIR Mhealth Uhealth 2020, 8, e18364. [Google Scholar] [CrossRef]
- Børøsund, E.; Varsi, C.; Clark, M.M.; Ehlers, S.L.; Andrykowski, M.A.; Sleveland, H.R.S.; Bergland, A.; Nes, L.S. Pilot testing an app-based stress management intervention for cancer survivors. Transl. Behav. Med. 2020, 10, 770–780. [Google Scholar] [CrossRef]
- Ham, K.; Chin, S.; Suh, Y.J.; Rhee, M.; Yu, E.-S.; Lee, H.J.; Kim, J.-H.; Kim, S.W.; Koh, S.-J.; Chung, K.-M. Preliminary results from a randomized controlled study for an app-based cognitive behavioral therapy program for depression and anxiety in cancer patients. Front. Psychol. 2019, 10, 1592. [Google Scholar] [CrossRef] [PubMed]
- Benze, G.; Nauck, F.; Alt-Epping, B.; Gianni, G.; Bauknecht, T.; Ettl, J.; Munte, A.; Kretzschmar, L.; Gaertner, J. PROutine: A feasibility study assessing surveillance of electronic patient reported outcomes and adherence via smartphone app in advanced cancer. Ann. Palliat Med. 2019, 8, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Greer, J.A.; Jacobs, J.; Pensak, N.; MacDonald, J.J.; Fuh, C.X.; Perez, G.K.; Ward, A.; Tallen, C.; Muzikansky, A.; Traeger, L. Randomized trial of a tailored cognitive-behavioral therapy mobile application for anxiety in patients with incurable cancer. The Oncologist 2019, 24, 1111. [Google Scholar] [CrossRef]
- Maguire, R.; McCann, L.; Kotronoulas, G.; Kearney, N.; Ream, E.; Armes, J.; Patiraki, E.; Furlong, E.; Fox, P.; Gaiger, A. Real time remote symptom monitoring during chemotherapy for cancer: European multicentre randomised controlled trial (eSMART). BMJ 2021, 374, n1647. [Google Scholar] [CrossRef]
- Ormel, H.L.; van der Schoot, G.G.; Westerink, N.-D.L.; Sluiter, W.J.; Gietema, J.A.; Walenkamp, A.M. Self-monitoring physical activity with a smartphone application in cancer patients: A randomized feasibility study (SMART-trial). Support. Care Cancer 2018, 26, 3915–3923. [Google Scholar] [CrossRef] [PubMed]
- Krebs, P.; Burkhalter, J.; Fiske, J.; Snow, H.; Schofield, E.; Iocolano, M.; Borderud, S.; Ostroff, J.S. The QuitIT coping skills game for promoting tobacco cessation among smokers diagnosed with cancer: Pilot randomized controlled trial. JMIR Mhealth Uhealth 2019, 7, e10071. [Google Scholar] [CrossRef] [PubMed]
- Casillas, J.N.; Schwartz, L.F.; Crespi, C.M.; Ganz, P.A.; Kahn, K.L.; Stuber, M.L.; Bastani, R.; Alquaddomi, F.; Estrin, D.L. The use of mobile technology and peer navigation to promote adolescent and young adult (AYA) cancer survivorship care: Results of a randomized controlled trial. J. Cancer Surviv. 2019, 13, 580–592. [Google Scholar] [CrossRef]
- Rico, T.M.; dos Santos Machado, K.; Fernandes, V.P.; Madruga, S.W.; Santin, M.M.; Petrarca, C.R.; Dumith, S.C. Use of Text Messaging (SMS) for the Management of Side Effects in Cancer Patients Undergoing Chemotherapy Treatment: A Randomized Controlled Trial. J. Med. Syst. 2020, 44, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.-M.; Suh, Y.J.; Chin, S.; Seo, D.; Yu, E.-S.; Lee, H.J.; Kim, J.-H.; Kim, S.W.; Koh, S.-J. A Pilot Study Testing the Efficacy of dCBT in Patients With Cancer Experiencing Sleep Problems. Front. Psychol. 2022, 13, 699168. [Google Scholar] [CrossRef]
- Sundberg, K.; Wengström, Y.; Blomberg, K.; Hälleberg-Nyman, M.; Frank, C.; Langius-Eklöf, A. Early detection and management of symptoms using an interactive smartphone application (Interaktor) during radiotherapy for prostate cancer. Support. Care Cancer 2017, 25, 2195–2204. [Google Scholar] [CrossRef]
- Lee, B.J.; Park, Y.H.; Lee, J.Y.; Kim, S.J.; Jang, Y.; Lee, J.I. Smartphone application versus pedometer to promote physical activity in prostate cancer patients. Telemed. E-Health 2019, 25, 1231–1236. [Google Scholar] [CrossRef]
- Ji, W.; Kwon, H.; Lee, S.; Kim, S.; Hong, J.S.; Park, Y.R.; Kim, H.R.; Lee, J.C.; Jung, E.J.; Kim, D. Mobile health management platform–based pulmonary rehabilitation for patients with non–small cell lung cancer: Prospective clinical trial. JMIR Mhealth Uhealth 2019, 7, e12645. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kim, J.Y.; Lee, J.C.; Kim, H.R.; Song, S.; Kwon, H.; Ji, W.; Choi, C.M. Mobile phone app–based pulmonary rehabilitation for chemotherapy-treated patients with advanced lung cancer: Pilot study. JMIR Mhealth Uhealth 2019, 7, e11094. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.-F.; Huang, R.-C.; Yang, S.-C.; Chou, C.; Chen, L.-C. Evaluating the Effects of a Mobile Health App on Reducing Patient Care Needs and Improving Quality of Life After Oral Cancer Surgery: Quasiexperimental Study. JMIR Mhealth Uhealth 2020, 8, e18132. [Google Scholar] [CrossRef]
- De Tommasi, C.; Richardson, E.; Reale, M.; Jordan, J. Evaluation of a novel application of a mindfulness phone application for patients with brain tumours: A feasibility study. J. Neuro-Oncol. 2020, 149, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Rettig, E.M.; Fakhry, C.; Hales, R.K.; Kisuule, F.; Quon, H.; Kiess, A.P.; Yin, L.X.; Zhang, Y.; Blackford, A.L.; Drummond, M.B. Pilot randomized controlled trial of a comprehensive smoking cessation intervention for patients with upper aerodigestive cancer undergoing radiotherapy. Head Neck 2018, 40, 1534–1547. [Google Scholar] [CrossRef] [PubMed]
- Keum, J.; Chung, M.J.; Kim, Y.; Ko, H.; Sung, M.J.; Jo, J.H.; Park, J.Y.; Bang, S.; Park, S.W.; Song, S.Y. Usefulness of smartphone apps for improving nutritional status of pancreatic cancer patients: Randomized controlled trial. JMIR Mhealth Uhealth 2021, 9, e21088. [Google Scholar] [CrossRef]
- Meyerowitz-Katz, G.; Ravi, S.; Arnolda, L.; Feng, X.; Maberly, G.; Astell-Burt, T. Rates of attrition and dropout in app-based interventions for chronic disease: Systematic review and meta-analysis. J. Med. Internet Res. 2020, 22, e20283. [Google Scholar] [CrossRef]
- Melissant, H.C.; Verdonck-de Leeuw, I.M.; Lissenberg-Witte, B.I.; Konings, I.R.; Cuijpers, P.; Van Uden-Kraan, C.F. ‘Oncokompas’, a web-based self-management application to support patient activation and optimal supportive care: A feasibility study among breast cancer survivors. Acta Oncol. 2018, 57, 924–934. [Google Scholar] [CrossRef]
- Wang, Y.; Lin, Y.; Chen, J.; Wang, C.; Hu, R.; Wu, Y. Effects of Internet-based psycho-educational interventions on mental health and quality of life among cancer patients: A systematic review and meta-analysis. Support. Care Cancer 2020, 28, 2541–2552. [Google Scholar] [CrossRef] [PubMed]
- Buneviciene, I.; Mekary, R.A.; Smith, T.R.; Onnela, J.-P.; Bunevicius, A. Can mHealth interventions improve quality of life of cancer patients? A systematic review and meta-analysis. Crit. Rev. Oncol. /Hematol. 2021, 157, 103123. [Google Scholar] [CrossRef] [PubMed]
- Ning, Y.; Jia, Z.; Zhu, R.; Ding, Y.; Wang, Q.; Han, S. Effect and feasibility of gamification interventions for improving physical activity and health-related outcomes in cancer survivors: An early systematic review and meta-analysis. Support. Care Cancer 2022, 31, 92. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Kim, S.; Kim, S.H.; Yoo, S.-H.; Sung, J.H.; Oh, E.G.; Kim, N.; Lee, J. Digital Health Interventions for Adult Patients With Cancer Evaluated in Randomized Controlled Trials: Scoping Review. J. Med. Internet Res. 2023, 25, e38333. [Google Scholar] [CrossRef]
- World Health Organization. Classification of Digital Health Interventions v1. 0: A Shared Language to Describe the Uses of Digital Technology for Health; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Wald, D.S.; Butt, S.; Bestwick, J.P. One-way versus two-way text messaging on improving medication adherence: Meta-analysis of randomized trials. Am. J. Med. 2015, 128, 1139.e1131–1139.e1135. [Google Scholar] [CrossRef]
- Rincon, E.; Monteiro-Guerra, F.; Rivera-Romero, O.; Dorronzoro-Zubiete, E.; Sanchez-Bocanegra, C.L.; Gabarron, E. Mobile phone apps for quality of life and well-being assessment in breast and prostate cancer patients: Systematic review. JMIR mHealth uHealth 2017, 5, e8741. [Google Scholar] [CrossRef]
- Cheung, A.T.; Li, W.H.C.; Ho, L.L.K.; Ho, K.Y.; Chan, G.C.F.; Chung, J.O.K. Physical activity for pediatric cancer survivors: A systematic review of randomized controlled trials. J. Cancer Surviv. 2021, 15, 876–889. [Google Scholar] [CrossRef]
- Escriva Boulley, G.; Leroy, T.; Bernetière, C.; Paquienseguy, F.; Desfriches-Doria, O.; Préau, M. Digital health interventions to help living with cancer: A systematic review of participants’ engagement and psychosocial effects. Psycho-Oncol. 2018, 27, 2677–2686. [Google Scholar] [CrossRef] [PubMed]
- Dixon, D.; Johnston, M. Health Behaviour Change Competency Framework: Competences to Deliver Interventions to Change Lifestyle Behaviours that Affect Health; Division of Health Psychology, The British Psychological Association, The Scottish Government: Edinburgh, Scotland, 2010.
- Michie, S.; Hyder, N.; Walia, A.; West, R. Development of a taxonomy of behaviour change techniques used in individual behavioural support for smoking cessation. Addict. Behav. 2011, 36, 315–319. [Google Scholar] [CrossRef]
- McGrady, M.E.; Schwartz, L.E.; Noser, A.E.; Klages, K.L.; Sweenie, R.; Breen, G.; Ramsey, R.R. Systematic Evaluation of the Behavior Change Techniques and Quality of Commercially Available Cancer Self-Management Apps. JCO Oncol. Pract. 2022, 19, e228–e237. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Gentile, D.; Markham, M.J.; Eaton, T. Patients with cancer and social media: Harness benefits, avoid drawbacks. J. Oncol. Pract. 2018, 14, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Pope, Z.; Lee, J.E.; Zeng, N.; Lee, H.Y.; Gao, Z. Feasibility of smartphone application and social media intervention on breast cancer survivors’ health outcomes. Transl. Behav. Med. 2019, 9, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Attai, D.J.; Cowher, M.S.; Al-Hamadani, M.; Schoger, J.M.; Staley, A.C.; Landercasper, J. Twitter social media is an effective tool for breast cancer patient education and support: Patient-reported outcomes by survey. J. Med. Internet Res. 2015, 17, e4721. [Google Scholar] [CrossRef] [PubMed]
- Dugas, M.; Gao, G.; Agarwal, R. Unpacking mHealth interventions: A systematic review of behavior change techniques used in randomized controlled trials assessing mHealth effectiveness. Digit. Health 2020, 6, 2055207620905411. [Google Scholar] [CrossRef]



| Cancer Type (n-Number of Studies) | Positive Outcome(+) | Neutral Outcome | Duration (Min-Max) (Weeks) | Usage Rate (Max-Min) (%) |
|---|---|---|---|---|
| Breast Cancer (n = 20) | 19 | 1 | 4–24 | 100–74.5% |
| Mixed Cancer (n = 23) | 19 | 4 | 4–24 | 100–25% |
| Prostate Cancer (n = 2) | 2 | 0 | 8–12 | 89.4–79% |
| Lung Cancer (n = 2) | 2 | 0 | 12 | 100–90% |
| Pancreatic Cancer (n = 2) | 1 | 1 | 12–32 | 82.5–79% |
| Oral Cancer (n = 1) | 12 | 0 | 12 | 100% |
| Brain Tumour (n = 1) | 1 | 0 | 8 | 80% |
| Aerodigestive Cancer (n = 1) | 1 | 0 | 8 | 100% |
| Hematologic Cancer (n = 1) | 0 | 1 | 16 | 90% |
| Myeloid Neoplasm (n = 1) | 0 | 1 | 8 to 12 | 88% |
| Oesophageal Cancer (n = 1) | 0 | 1 | 8 | 83.3% |
| Completion/Usage Rate (%) | Study Duration ≤ 12 Weeks | Study Duration 13–32 Weeks |
|---|---|---|
| =≥80% | 33 studies | 8 studies |
| <80% | 10 studies | 4 studies |
| Total studies | 43 studies | 12 studies |
| 1. Theoretical foundation or behavioural techniques | ||||||||||||||||
| BCTs | SCT | CBT | CBSM | CT | LTs | GST | SDT | MI | ACT | CohT | CopT | SST | TAM | GBL | EBT | MBSR |
| [37,45,56,59,66] | [37,38,43,45,49,54,67] | [62,64,70] | [61] | [37,38,45] | [37,45,60] | [37,45,60] | [27,34] | [60] | [60] | [30] | [30] | [30] | [81] | [46] | [39] | [48] |
| 2. Delivery Mechanisms | ||||||||||||||||
| Reminders/Alerts/Push Notifications | Tailored Messages/Lifestyle Recommendations | |||||||||||||||
| [28,31,32,34,37,40,44,45,47,51,52,55,57,58,61,63,69,71,74,81] | [16,27,29,35,36,38,59,65,68,72,73,77,78] | |||||||||||||||
| 3. Psycho-educational Program | ||||||||||||||||
| [31,40,42,53,54,64,81] | ||||||||||||||||
| 4. Social Platform | ||||||||||||||||
| Line App | ||||||||||||||||
| [41] | [27,34] | [42] | [75] | |||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dhar, E.; Bah, A.N.; Chicchi Giglioli, I.A.; Quer, S.; Fernandez-Luque, L.; Núñez-Benjumea, F.J.; Malwade, S.; Uddin, M.; Upadhyay, U.; Syed-Abdul, S. A Scoping Review and a Taxonomy to Assess the Impact of Mobile Apps on Cancer Care Management. Cancers 2023, 15, 1775. https://doi.org/10.3390/cancers15061775
Dhar E, Bah AN, Chicchi Giglioli IA, Quer S, Fernandez-Luque L, Núñez-Benjumea FJ, Malwade S, Uddin M, Upadhyay U, Syed-Abdul S. A Scoping Review and a Taxonomy to Assess the Impact of Mobile Apps on Cancer Care Management. Cancers. 2023; 15(6):1775. https://doi.org/10.3390/cancers15061775
Chicago/Turabian StyleDhar, Eshita, Adama Ns Bah, Irene Alice Chicchi Giglioli, Silvia Quer, Luis Fernandez-Luque, Francisco J. Núñez-Benjumea, Shwetambara Malwade, Mohy Uddin, Umashankar Upadhyay, and Shabbir Syed-Abdul. 2023. "A Scoping Review and a Taxonomy to Assess the Impact of Mobile Apps on Cancer Care Management" Cancers 15, no. 6: 1775. https://doi.org/10.3390/cancers15061775
APA StyleDhar, E., Bah, A. N., Chicchi Giglioli, I. A., Quer, S., Fernandez-Luque, L., Núñez-Benjumea, F. J., Malwade, S., Uddin, M., Upadhyay, U., & Syed-Abdul, S. (2023). A Scoping Review and a Taxonomy to Assess the Impact of Mobile Apps on Cancer Care Management. Cancers, 15(6), 1775. https://doi.org/10.3390/cancers15061775