
Prognostic Value of Combined Hematological/Biochemical Indexes and Tumor Clinicopathologic Features in Colorectal Cancer Patients—A Pilot Single Center Study
 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Patient Characteristics
2.3. Preoperative Laboratory Measurements and Other Prognostic Scores
2.4. Tumor Characteristics
2.5. Follow-Up
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
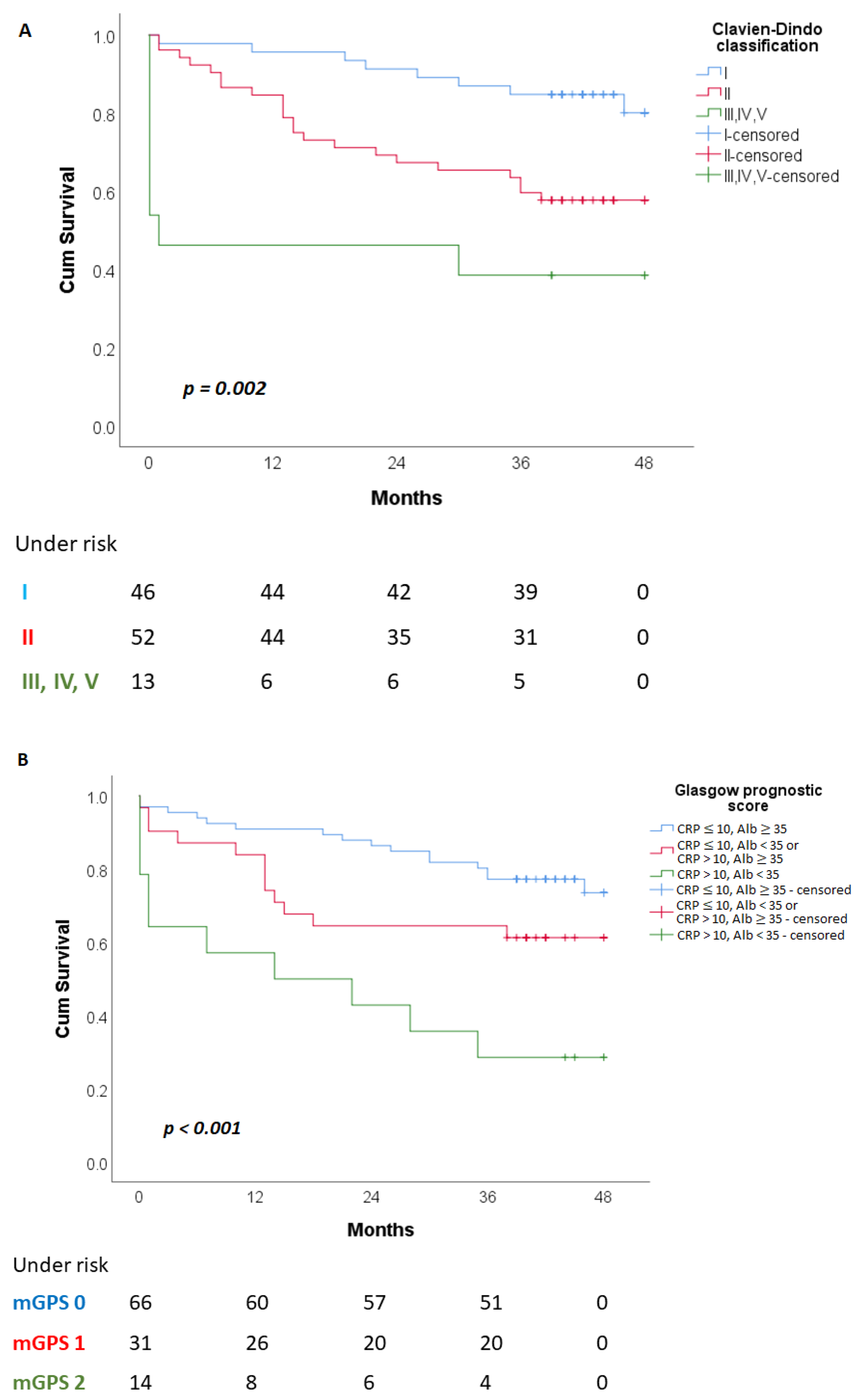
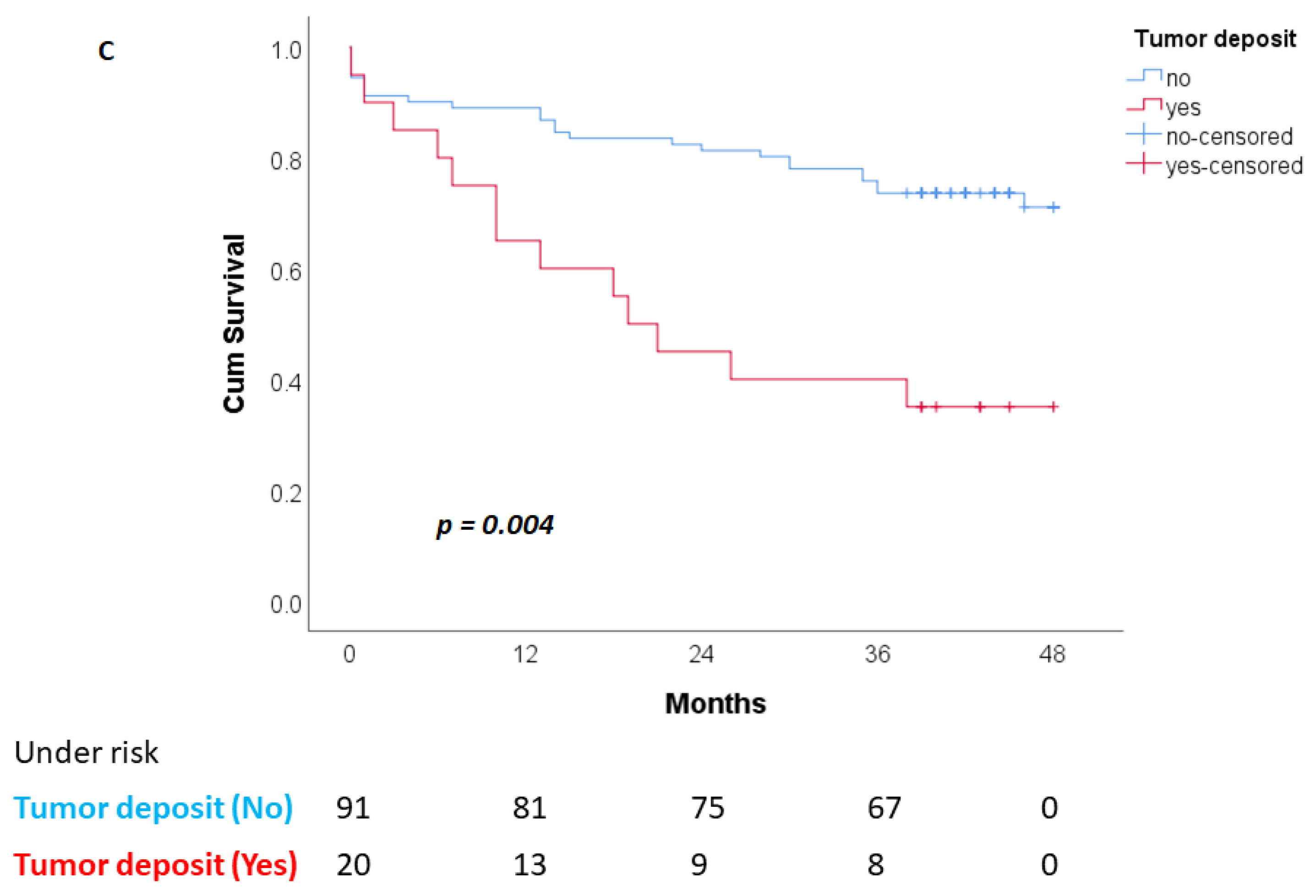
3.2. Overall Patient Survival (OS)
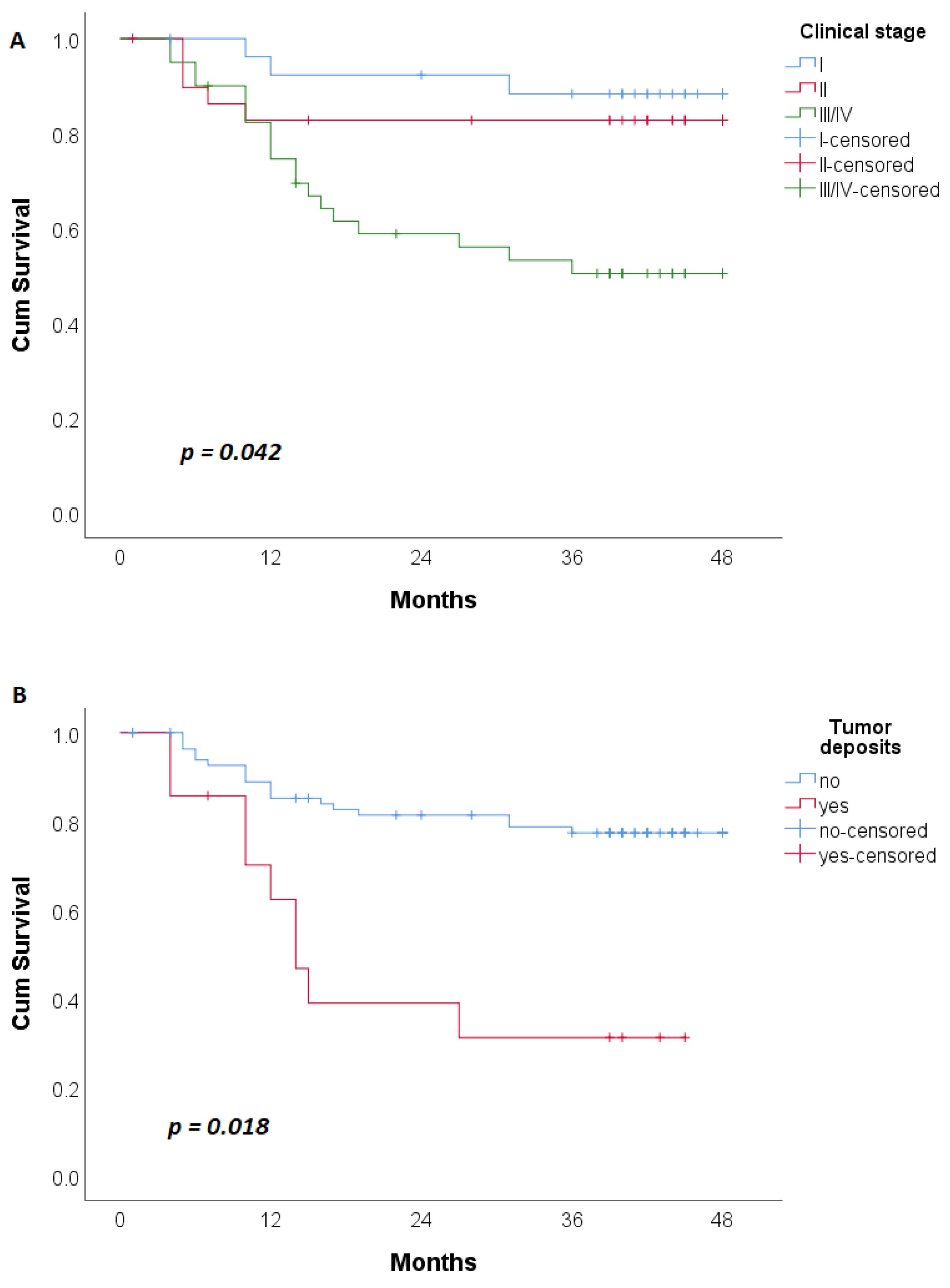
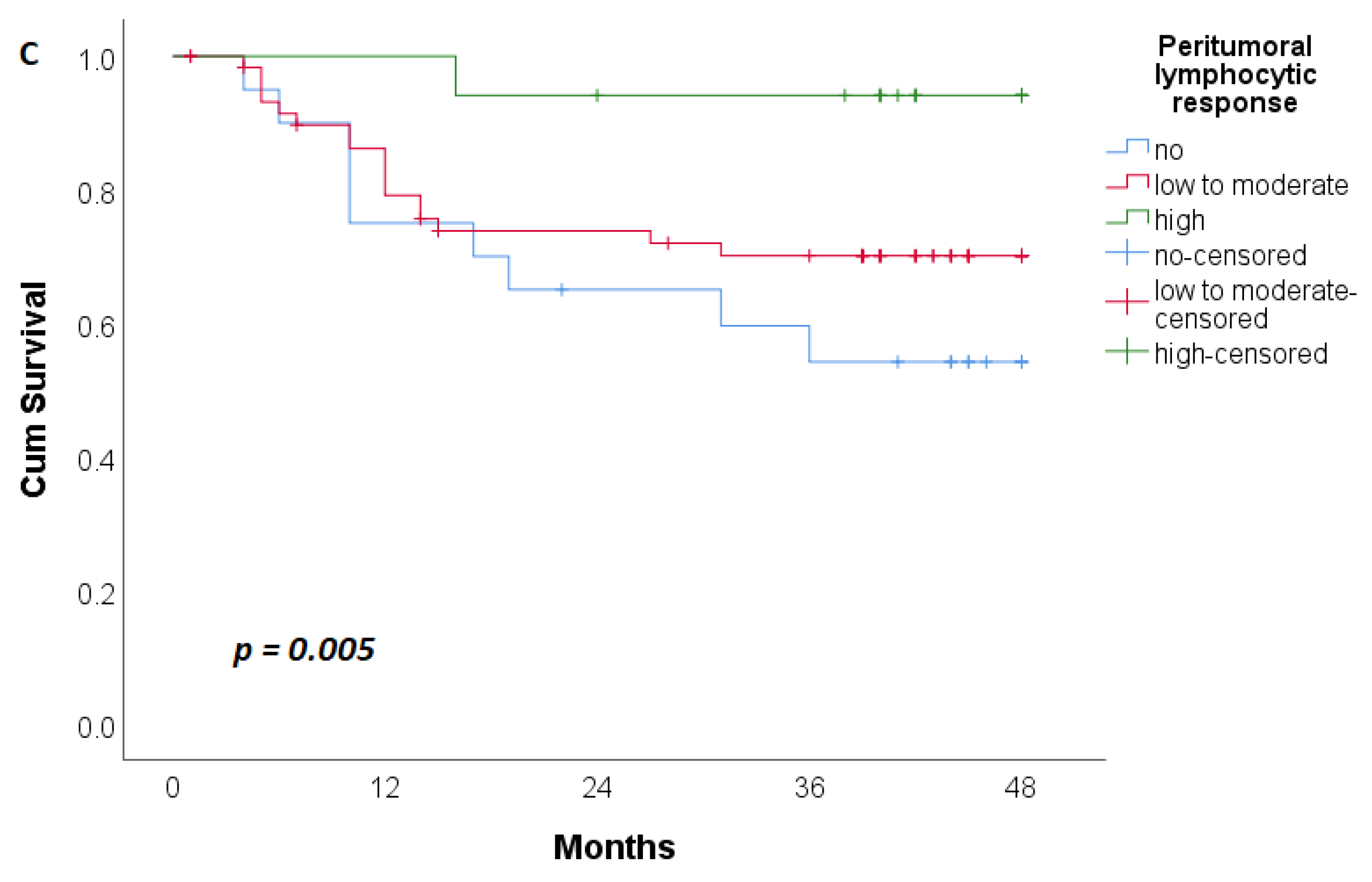
3.3. Disease-Free Patient Survival (DFS)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Hashiguchi, Y.; Muro, K.; Saito, Y.; Ito, Y.; Ajioka, Y.; Hamaguchi, T.; Hasegawa, K.; Hotta, K.; Ishida, H.; Ishiguro, M.; et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int. J. Clin. Oncol. 2020, 25, 1–42. [Google Scholar] [CrossRef]
- O’Connell, J.B.; Maggard, M.A.; Ko, C.Y. Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J. Natl. Cancer Inst. 2004, 96, 1420–1425. [Google Scholar] [CrossRef]
- Naxerova, K.; Reiter, J.G.; Brachtel, E.; Lennerz, J.K.; van de Wetering, M.; Rowan, A.; Cai, T.; Clevers, H.; Swanton, C.; Nowak, M.A.; et al. Origins of lymphatic and distant metastases in human colorectal cancer. Science 2017, 357, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Percario, R.; Panaccio, P.; di Mola, F.F.; Grottola, T.; Di Sebastiano, P. The Complex Network between Inflammation and Colorectal Cancer: A Systematic Review of the Literature. Cancers 2021, 13, 6237. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Yao, S.; Lu, P.; Ma, Y.; Xu, H.; Yin, Z.; Hu, J.; Liu, Y.; Wei, S. The Prognostic Value of New Index (LANR) Composed of Pre-operative Lymphocytes, Albumin, and Neutrophils in Patients with Resectable Colorectal Cancer. Front. Oncol. 2021, 11, 610264. [Google Scholar] [CrossRef]
- Hayama, T.; Ozawa, T.; Asako, K.; Kondo, R.; Ono, K.; Okada, Y.; Tsukamoto, M.; Fukushima, Y.; Shimada, R.; Nozawa, K.; et al. Impact of Colon Cancer Location on the Prognostic Significance of Nutritional Indexes and Inflammatory Markers. In Vivo 2021, 35, 1261–1269. [Google Scholar] [CrossRef]
- Ishizuka, M.; Nagata, H.; Takagi, K.; Iwasaki, Y.; Shibuya, N.; Kubota, K. Clinical Significance of the C-Reactive Protein to Albumin Ratio for Survival After Surgery for Colorectal Cancer. Ann. Surg. Oncol. 2016, 23, 900–907. [Google Scholar] [CrossRef]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; O’Reilly, D.S.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. An inflammation-based prognostic score (mGPS) predicts cancer survival independent of tumour site: A Glasgow Inflammation Outcome Study. Br. J. Cancer 2011, 104, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Man, W.; Lin, H.; Liu, Z.; Jin, L.; Wang, J.; Zhang, J.; Bai, Z.; Yao, H.; Zhang, Z.; Deng, W. Usefulness of Inflammation-Based Prognostic Scores for Predicting the Risk of Complications After Radical Resection of Colorectal Carcinoma. Cancer Manag. Res. 2020, 12, 1029–1038. [Google Scholar] [CrossRef] [PubMed]
- Sato, R.; Oikawa, M.; Kakita, T.; Okada, T.; Abe, T.; Yazawa, T.; Tsuchiya, H.; Akazawa, N.; Sato, M.; Ohira, T.; et al. Preoperative change of modified Glasgow prognostic score after stenting predicts the long-term outcomes of obstructive colorectal cancer. Surg. Today 2020, 50, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA A Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Roxburgh, C.S.; McMillan, D.C. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010, 6, 149–163. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of the Republic of Serbia. Available online: https://www.zdravlje.gov.rs/view_file.php?file_id=648&cache=sr (accessed on 7 December 2022).
- Pfister, D.G.; Benson, A.B., 3rd; Somerfield, M.R. Clinical practice. Surveillance strategies after curative treatment of colorectal cancer. N. Engl. J. Med. 2004, 350, 2375–2382. [Google Scholar] [CrossRef] [PubMed]
- Majek, O.; Gondos, A.; Jansen, L.; Emrich, K.; Holleczek, B.; Katalinic, A.; Nennecke, A.; Eberle, A.; Brenner, H.; GEKID Cancer Survival Working Group. Sex differences in colorectal cancer survival: Population-based analysis of 164,996 colorectal cancer patients in Germany. PLoS ONE 2013, 8, e68077. [Google Scholar] [CrossRef]
- Clendenen, T.V.; Koenig, K.L.; Shore, R.E.; Levitz, M.; Arslan, A.A.; Zeleniuch-Jacquotte, A. Postmenopausal levels of endogenous sex hormones and risk of colorectal cancer. Cancer epidemiology, biomarkers & prevention: A publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. Cancer Epidemiol. Biomark. Prev. 2009, 18, 275–281. [Google Scholar]
- Barzi, A.; Lenz, A.M.; Labonte, M.J.; Lenz, H.J. Molecular pathways: Estrogen pathway in colorectal cancer. Clinical cancer research. Off. J. Am. Assoc. Cancer Res. 2013, 19, 5842–5848. [Google Scholar] [CrossRef]
- Abancens, M.; Bustos, V.; Harvey, H.; McBryan, J.; Harvey, B.J. Sexual Dimorphism in Colon Cancer. Front. Oncol. 2020, 10, 607909. [Google Scholar] [CrossRef]
- Jiang, L.; Fei, H.; Yang, A.; Zhu, J.; Sun, J.; Liu, X.; Xu, W.; Yang, J.; Zhang, S. Estrogen inhibits the growth of colon cancer in mice through reversing extracellular vesicle-mediated immunosuppressive tumor microenvironment. Cancer Lett. 2021, 520, 332–343. [Google Scholar] [CrossRef]
- Salehi Far, S.; Soltani, M.; Zardast, M.; Zhu, J.; Sun, J.; Liu, X.; Xu, W.; Yang, J.; Zhang, S. Investigating the Factors Associated with the Level of Expression of Estrogen and Progesterone Receptors in Patients Suffering from Colorectal Cancer. J. Cancer Epidemiol. 2021, 2021, 4478155. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Duraes, L.C.; Stocchi, L.; Steele, S.R.; Kalady, M.F.; Church, J.M.; Gorgun, E.; Liska, D.; Kessler, H.; Lavryk, O.A.; Delaney, C.P. The Relationship between Clavien-Dindo Morbidity Classification and Oncologic Outcomes After Colorectal Cancer Resection. Ann. Surg. Oncol. 2018, 25, 188–196. [Google Scholar] [CrossRef]
- Aoyama, T.; Oba, K.; Honda, M.; Sadahiro, S.; Hamada, C.; Mayanagi, S.; Kanda, M.; Maeda, H.; Kashiwabara, K.; Sakamoto, J.; et al. Impact of postoperative complications on the colorectal cancer survival and recurrence: Analyses of pooled individual patients’ data from three large phase III randomized trials. Cancer Med. 2017, 6, 1573–1580. [Google Scholar] [CrossRef]
- Tuomisto, A.E.; Mäkinen, M.J.; Väyrynen, J.P. Systemic inflammation in colorectal cancer: Underlying factors, effects, and prognostic significance. World J. Gastroenterol. 2019, 25, 4383–4404. [Google Scholar] [CrossRef]
- Xia, L.J.; Li, W.; Zhai, J.C.; Yan, C.W.; Chen, J.B.; Yang, H. Significance of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, lymphocyte-to-monocyte ratio and prognostic nutritional index for predicting clinical outcomes in T1-2 rectal cancer. BMC Cancer 2020, 20, 208. [Google Scholar] [CrossRef]
- Mizuno, H.; Yuasa, N.; Takeuchi, E.; Miyake, H.; Nagai, H.; Yoshioka, Y.; Miyata, K. Blood cell markers that can predict the long-term outcomes of patients with colorectal cancer. PLoS ONE 2019, 14, e0220579. [Google Scholar] [CrossRef]
- Ozawa, T.; Ishihara, S.; Nishikawa, T.; Tanaka, T.; Tanaka, J.; Kiyomatsu, T.; Hata, K.; Kawai, K.; Nozawa, H.; Kazama, S.; et al. The preoperative platelet to lymphocyte ratio is a prognostic marker in patients with stage II colorectal cancer. Int. J. Color. Dis. 2015, 30, 1165–1171. [Google Scholar] [CrossRef]
- Argilés, J.M.; Busquets, S.; Stemmler, B.; López-Soriano, F.J. Cancer cachexia: Understanding the molecular basis. Nat. Rev. Cancer 2014, 14, 754–762. [Google Scholar] [CrossRef]
- Son, W.; Shin, S.J.; Park, S.H.; Lee, S.K.; Park, E.J.; Baik, S.H.; Lee, K.Y.; Kang, J. Clinical Impact of Combined Modified Glasgow Prognostic Score and C-Reactive Protein/Albumin Ratio in Patients with Colorectal Cancer. Diagnostics 2020, 10, 859. [Google Scholar] [CrossRef]
- Sun, G.; Li, Y.; Peng, Y.; Lu, D.; Zhang, F.; Cui, X.; Zhang, Q.; Li, Z. Impact of the preoperative prognostic nutritional index on postoperative and survival outcomes in colorectal cancer patients who underwent primary tumor resection: A systematic review and meta-analysis. Int. J. Color. Dis. 2019, 34, 681–689. [Google Scholar] [CrossRef]
- Climent, M.; Ryan, É.J.; Stakelum, Á.; Khaw, Y.L.; Creavin, B.; Lloyd, A.; Alhassan, D.; Mohan, H.M.; Kennelly, R.; Sheahan, K.; et al. Systemic inflammatory response predicts oncological outcomes in patients undergoing elective surgery for mismatch repair-deficient colorectal cancer. Int. J. Color. Dis. 2019, 34, 1069–1078. [Google Scholar] [CrossRef]
- Nagashima, Y.; Funahashi, K.; Kagami, S.; Ushigome, M.; Kaneko, T.; Miura, Y.; Yoshida, K.; Koda, T.; Kurihara, A. Which preoperative immunonutritional index best predicts postoperative mortality after palliative surgery for malignant bowel obstruction in patients with late-stage cancer? A single-center study in Japan comparing the modified Glasgow prognostic score (mGPS), the prognostic nutritional index (PNI), and the controlling nutritional status (CONUT). Surg. Today 2023, 53, 22–30. [Google Scholar]
- Tamai, K.; Okamura, S.; Makino, S.; Yamamura, N.; Fukuchi, N.; Ebisui, C.; Inoue, A.; Yano, M. C-reactive protein/albumin ratio predicts survival after curative surgery in elderly patients with colorectal cancer. Updates Surg. 2022, 74, 153–162. [Google Scholar] [CrossRef]
- Morris-Stiff, G.; Gomez, D.; Prasad, K.R. C-reactive protein in liver cancer surgery. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2008, 34, 727–729. [Google Scholar] [CrossRef]
- Zhou, J.; Wei, W.; Hou, H.; Ning, S.; Li, J.; Huang, B.; Liu, K.; Zhang, L. Prognostic Value of C-Reactive Protein, Glasgow Prognostic Score, and C-Reactive Protein-to-Albumin Ratio in Colorectal Cancer. Front. Cell Dev. Biol. 2021, 9, 637650. [Google Scholar] [CrossRef]
- Nakazaki, H. Preoperative and postoperative cytokines in patients with cancer. Cancer 1992, 70, 709–713. [Google Scholar] [CrossRef]
- McMillan, D.C.; Watson, W.S.; O’Gorman, P.; Preston, T.; Scott, H.R.; McArdle, C.S. Albumin concentrations are primarily determined by the body cell mass and the systemic inflammatory response in cancer patients with weight loss. Nutr. Cancer 2001, 39, 210–213. [Google Scholar] [CrossRef]
- Finn, O.J. A Believer’s Overview of Cancer Immunosurveillance and Immunotherapy. J. Immunol. 2018, 200, 385–391. [Google Scholar] [CrossRef]
- Liu, F.; Zhao, J.; Li, C.; Wu, Y.; Song, W.; Guo, T.; Chen, S.; Cai, S.; Huang, D.; Xu, Y. The unique prognostic characteristics of tumor deposits in colorectal cancer patients. Ann. Transl. Med. 2019, 7, 769. [Google Scholar] [CrossRef]
- Lord, A.C.; D’Souza, N.; Pucher, P.H.; Moran, B.J.; Abulafi, A.M.; Wotherspoon, A.; Rasheed, S.; Brown, G. Significance of extranodal tumour deposits in colorectal cancer: A systematic review and meta-analysis. Eur. J. Cancer 2017, 82, 92–102. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Knijn, N.; Hugen, N.; Marshall, H.C.; Sugihara, K.; Tot, T.; Ueno, H.; Quirke, P. Tumor Deposits in Colorectal Cancer: Improving the Value of Modern Staging-A Systematic Review and Meta-Analysis. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 1119–1127. [Google Scholar] [CrossRef]
- Jakovljevic, K.; Malisic, E.; Cavic, M.; Krivokuca, A.; Dobricic, J.; Jankovic, R. KRAS and BRAF mutations in Serbian patients with colorectal cancer. J. BUON Off. J. Balk. Union Oncol. 2012, 17, 575–580. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics of Patients | n (%) |
|---|---|
| Sex | |
| Male | 63 (56.8) |
| Age (years) † | 67 (32−88) |
| <40 years | 2 (1.8) |
| 41–50 years | 3 (2.7) |
| 51–60 years | 11 (9.9) |
| >60 years | 95 (85.57) |
| ASA Score ‡ | |
| 1 | 18 (16.2) |
| 2 | 50 (45.0) |
| 3 | 43 (38.7) |
| 4 | 0 (0) |
| 5 | 0 (0) |
| Ten most common comorbidities | |
| Arterial hypertension (HTA) | 81 (73.0) |
| Sideropenic anemia | 30 (27.0) |
| Diabetes mellitus | 29 (26.1) |
| Ischemic heart disease | 21 (18.9) |
| Cardiac arrhythmias | 15 (13.5) |
| Benign prostatic hyperplasia (BPH) | 12 (10.8) |
| Chronic obstructive pulmonary disease | 8 (7.2) |
| Hypothyroidism | 7 (6.3) |
| Stroke | 5 (4.5) |
| Renal failure | 3 (1.8) |
| Hematological/biochemical values and Indexes § | |
| Leukocytes (109/L) | 7 (5.70−8.4) |
| Erythrocytes (109/L) | 4.51 (4.17−4.88) |
| Platelets (109/L) | 293 (243−377) |
| Neutrophils (109/L) | 4.72 (3.78−5.85) |
| Lymphocytes (109/L) | 1.47 (1.14−1.94) |
| Monocytes (109/L) | 0.35 (0.28−0.44) |
| Hemoglobin (g/dL) | 12.10 (10.40−13.60) |
| Hematocrit (%) | 37.70 (33.60−41.80) |
| RBC (RDW-CV) (%) | 14.6 (13.3−17.4) |
| Serum albumin (g/L) | 39 (35.00−42.00) |
| CRP (C-reactive protein) (mg/L) | 4.80 (2.00−17.10) |
| CEA (ng/mL) | 3.37 (2.02−9.11) |
| CA 19-9 (U/mL) | 11.44 (6.28−28.46) |
| Cortisol 8 h (nmol/L) | 425 (349.10−526.70) |
| Testosterone (nmol/L) | 3.12 (0.32−10.64) |
| Estradiol (pmol/L) | 21.18 (13.57−50.56) |
| Estadiol of males | 30.465 (18.35–60.015) |
| Estadiol of females | 18.35 (5–18.35) |
| Estadiol of females <60 years | 30.75 (18.35–201.005) |
| Estadiol of females >60 years | 18.35 (5–18.35) |
| NLR (Neutrophile to Lymphocyte Ratio) | 3.09 (2.21−4.54) |
| MLR (Monocyte to Lymphocyte Ratio) | 0.23 (0.18−0.32) |
| PLR (Platelets to Lymphocyte Ratio) | 190.63 (141.60−276.14) |
| RLR (RBC to Lymphocyte Ratio) | 10.23 (7.62−14.1) |
| MPR (MPV to Platelets Ratio) | 0.03 (0.02−0.04) |
| CAR (CRP to Serum Albumin Ratio) | 0.12 (0.05−0.45) |
| PNI (Prognostic Nutritive Index) | 46.56 (42.30−50.85) |
| LANR (Lymphocyte, Serum Albumin, Neutrophile Ratio) | 12.43 (7.78−17.76) |
| mGPS (modified Glasgow Prognostic Score) ¶: | |
| 0 | 66 (59.5) |
| 1 | 31 (27.9) |
| 2 | 14 (12.6) |
| Parameters | Death | p | Relapse of Disease | p | ||
|---|---|---|---|---|---|---|
| No N (%) | Yes N (%) | No n (%) | Yes n (%) | |||
| Sex | 0.300 * | 0.892 * | ||||
| Male | 44 (60.3) | 19 (50) | 41 (57.7) | 16 (59.3) | ||
| Female | 29 (39.7) | 19 (50) | 30 (42.3) | 11 (40.7) | ||
| Age (years) † | 66 (62−73) | 68 (62−80) | 0.117 ** | 67 (63−75) | 63 (60−68) | 0.045 ** |
| ASA Score | 0.248 * | 0.032 * | ||||
| 1 | 11 (15.1) | 7 (18.4) | 9 (12.7) | 8 (29.6) | ||
| 2 | 37 (50.7) | 13 (34.2) | 31 (43.7) | 14 (51.9) | ||
| 3 | 25 (34.2) | 18 (47.4) | 31 (43.7) | 5 (18.5) | ||
| 4 | / | / | / | / | ||
| 5 | / | / | / | / | ||
| Diabetes mellitus | 21 (28.8) | 8 (21.1) | 0.380 * | 21 (29.6) | 5 (18.5) | 0.268 * |
| HTA | 53 (72.6) | 28 (73.7) | 0.903 * | 53 (74.6) | 17 (63.0) | 0.253 * |
| Leukocytes † | 6.9 (5.80−8.10) | 7.65 (5.6−8.8) | 0.218 ** | 7 (5.88−8.1) | 7.7 (5.4−8.7) | 0.811 ** |
| Erythrocytes † | 4.55 (4.29−4.89) | 4.3 (3.88−4.79) | 0.059 ** | 4.48 (4.17−4.86) | 4.57 (4.14−5.14) | 0.375 ** |
| Platelets † | 282 (228−373) | 317 (258−389) | 0.090 ** | 282 (228−375) | 285 (230−392) | 0.431 ** |
| Neutrophils † | 4.59 (3.78−5.66) | 5.18 (3.84−7.12) | 0.196 ** | 4.68 (3.86−5.77) | 5.05 (3.08−6.58) | 0.880 ** |
| Lymphocytes † | 1.54 (1.25−1.94) | 1.33 (1.05−1.84) | 0.254 ** | 1.51 (1.25−1.94) | 1.56 (1−2) | 0.990 ** |
| Monocytes † | 0.34 (0.29−0.42) | 0.35 (0.26−0.48) | 0.751 ** | 0.36 (0.29−0.44) | 0.32 (0.25−0.39) | 0.183 ** |
| NLR † | 2.89 (2.22−4.44) | 3.73 (2.21−4.8) | 0.160 ** | 2.9 (2.25−4.52) | 2.9 (1.83−4.51) | 0.833 ** |
| MLR † | 0.22 (0.17−0.29) | 0.25 (0.19−0.35) | 0.234 ** | 0.22 (0.18−0.32) | 0.22 (0.17−0.27) | 0.278 ** |
| PLR † | 188.3 (138.14−235.62) | 211.64 (153.26−324.6) | 0.056 ** | 187.5 (140.3−245.03) | 193.88 (138.97−322.45) | 0.559 ** |
| MPR † | 0.03 (0.03−0.04) | 0.03 (0.025−0.04) | 0.229 ** | 0.03 (0.03−0.43) | 0.03 (0.02−0.043) | 0.933 ** |
| RLR † | 9.375 (7.64−12.14) | 12.3 (7.56−16.82) | 0.093 ** | 9.71 (7.64−13.73) | 9.3 (7.51−14.1) | 0.759 ** |
| CRP † | 3.5 (1.7−9.8) | 10.3 (4−34.9) | 0.001 ** | 4 (2−12) | 6.1 (1.7−15.2) | 0.605 ** |
| Serum Albumin † | 40 (36−42) | 37 (33−41) | 0.005 ** | 40 (36−42) | 41 (35−42) | 1.000 ** |
| Hemoglobin † | 12.4 (10.8−13.7) | 11 (9.4−12.9) | 0.037 ** | 12 (10−13.6) | 12.3 (10.4−13.7) | 0.535 ** |
| Hematocrit † | 38.6 (35.2−41.9) | 35.2 (31.9−41.7) | 0.027 ** | 37.7 (33.6−41.7) | 38.7 (32.6−42.9) | 0.580 ** |
| RBC (RDW-CV) † | 14.2 (13.2−16.7 | 14.9 (14−19.8) | 0.041 ** | 14.7 (13.3−17.4) | 14.4 (13.2−16.7) | 0.404 ** |
| CAR † | 0.08 (0.04−0.24) | 0.257 (0.11−0.85) | 0.001 ** | 0.09 (0.05−0.32) | 0.16 (0.04−0.38) | 0.611 ** |
| PNI † | 47.3 (43.8−51.25) | 54.1 (39.6−48.6) | 0.013 ** | 46.7 (43.3−51.15) | 47 (43.1−50.85) | 0.849 ** |
| LANR † | 13.27 (8.86−18.9) | 9.85 (7.09−16.28) | 0.043 ** | 13.27 (8.69−16.89) | 12.43 (7.72−19) | 0.852 ** |
| CEA † | 2.99 (1.88−6.48) | 5.2 (2.41−10.05) | 0.030 ** | 2.76 (1.88−6.31) | 3.59 (1.94−12.74) | 0.361 ** |
| CA 19−9 † | 10.41 (6.4−27.59) | 14.33 (6.22−37.16) | 0.230 ** | 10.92 (6.28−20.84) | 12.01 (6.22−41.8) | 0.324 ** |
| mGPS | 0.003 * | 0.700 * | ||||
| 0 | 50 (68.5) | 16 (42.1) | 46 (64.8) | 15 (55.6) | ||
| 1 | 19 (26) | 12 (31.6) | 19 (26.8) | 9 (33.3) | ||
| 2 | 4 (5.5) | 10 (26.3) | 6 (8.5) | 3 (11.1) | ||
| Tumor Location | 0.748 * | 0.929 * | ||||
| Right Colon | 25 (34.7) | 14 (37.8) | 24 (34.3) | 9 (33.3) | ||
| Left Colon and Rectum | 47 (65.3) | 23 (62.2) | 46 (65.7) | 18 (66.7) | ||
| Max Diameter of Tumor † | 40 (30−55) | 40 (30−55) | 40 (30−52) | 40 (30−60) | 0.582 ** | |
| TNM Stage | 0.009 * | <0.001 * | ||||
| I/II | 46 (63) | 14 (36.8) | 50 (70.4) | 8 (29.6) | ||
| III/IV | 27 (37) | 24 (63.2) | 21 (29.6) | 19 (70.4) | ||
| Number of Lymph Nodes † | 17 (12−21) | 14 (12−17) | 0.120 * | 15 (12−21) | 18 (13−21) | 0.444 ** |
| Positive Lymph Nodes † | 0 (0−1) | 2 (0−5) | 0.003 ** | 0 (0−1) | 1 (0−5) | 0.008 ** |
| Lymphonodal Ratio (LNR) | 0 (0−0.048) | 0.113 (0−0.353) | 0.001 ** | 0 (0−0.043) | 0 (0−0.231) | 0.008 ** |
| Tumor Configuration | 0.262 * | 0.731 * | ||||
| Exophytic | 29 (39.7) | 11 (28.9) | 29 (40.8) | 10 (37.0) | ||
| Endophytic | 44 (60.3) | 27 (71.1) | 42 (59.2) | 17 (63.0) | ||
| Tumor Gradus | 0.148 * | 0.193 * | ||||
| G1 | 10 (13.7) | 7 (18.4) | 10 (14.1) | 5 (18.5) | ||
| G2 | 60 (82.2) | 26 (68.4) | 59 (83.1) | 19 (70.4) | ||
| G3 | 3 (4.1) | 5 (13.2) | 2 (2.8) | 3 (11.1) | ||
| TIL ‡ | 0.380 * | 0.520 * | ||||
| Without/Easy to Moderate | 52 (71.2) | 30 (78.9) | 52 (73.2) | 18 (66.7) | ||
| Expressed | 21 (28.8) | 8 (21.1) | 19 (26.8) | 9 (33.3) | ||
| PTL Response § | 0.019 * | 0.029 * | ||||
| Without | 14 (19.2) | 12 (31.6) | 11 (15.5) | 9 (33.3) | ||
| Easy to Moderate | 43 (58.9) | 25 (65.8) | 44 (62.0) | 17 (63.0) | ||
| Expressed | 16 (21.9) | 1 (2.6) | 16 (22.5) | 1 (3.7) | ||
| Mucosal Component of The Tumor | 0.401 * | 0.292 * | ||||
| Yes | 23 (31.5) | 15 (39.5) | 21 (29.6) | 11 (40.7) | ||
| No | 50 (68.5) | 23 (60.5) | 50 (70.4) | 16 (59.3) | ||
| Lymphovascular Invasion | 0.205 * | 0.038 * | ||||
| Yes | 45 (61.6) | 28 (73.7) | 39 (54.9) | 21 (77.8) | ||
| No | 28 (38.4) | 10 (26.3) | 32 (45.1) | 6 (22.2) | ||
| Venous Invasion | 0.015 * | 0.020 * | ||||
| Yes | 0 (0) | 3 (7.9) | 0 (0) | 2 (7.4) | ||
| No | 73 (100) | 35 (92.1) | 71 (100) | 25 (92.6) | ||
| Perineural Invasion | 0.001 * | 0.018 * | ||||
| Yes | 10 (13.7) | 16 (42.1) | 9 (12.7) | 9 (33.3) | ||
| No | 63 (86.3) | 22 (57.9) | 62 (87.3) | 18 (66.7) | ||
| Tumor Deposits | 0.001 * | 0.001a * | ||||
| Yes | 7 (9.6) | 13 (34.2) | 5 (7.0) | 9 (33.3) | ||
| No | 66 (90.4) | 25 (65.8) | 66 (93.0) | 18 (66.7) | ||
| Tumor Budding | 0.037 * | 0.838 * | ||||
| Yes | 55 (75.3) | 34 (91.9) | 56 (78.9) | 21 (80.8) | ||
| No | 18 (24.7) | 3 (8.1) | 15 (21.1) | 5 (19.2) | ||
| Tumor Growth | 0.113 * | 0.752 * | ||||
| Expansive | 32 (44.4) | 11 (28.9) | 31 (44.3) | 11 (40.7) | ||
| Infiltrative | 40 (55.6) | 27 (71.1) | 39 (55.7) | 16 (59.3) | ||
| Approach | 0.092 * | 0.926 * | ||||
| Open | 61 (83.6) | 36 (94.7) | 61 (85.9) | 23 (85.2) | ||
| Laparoscopic | 12 (16.4) | 2 (5.3) | 10 (14.1) | 4 (14.8) | ||
| C-D Clasiffication ¶ | 0.003 * | 0.598 * | ||||
| I | 38 (52.1) | 8 (21.1) | 32 (45.1) | 11 (40.7) | ||
| II | 30 (41.1) | 22 (57.9) | 33 (46.5) | 15 (55.6) | ||
| III, IV, V | 5 (6.8) | 8 (21.1) | 6 (8.5) | 1 (3.7) | ||
| Adjuvant CT # | 0.644 * | <0.001 * | ||||
| Yes | 20 (27.4) | 12 (31.6) | 13 (18.3) | 15 (55.6) | ||
| No | 53 (72.6) | 26 (68.4) | 58 (81.7) | 12 (44.4) | ||
| Neoadjuvant CRT ## | 0.619 * | 0.744 * | ||||
| Yes | 4 (5.5) | 3 (7.9) | 4 (5.6) | 2 (7.4) | ||
| No | 69 (94.5) | 35 (92.1) | 67 (94.4) | 25 (92.6) | ||
| Parameters | Univariate | p Value | Multivariate | p Value | ||
|---|---|---|---|---|---|---|
| HR | 95% CI | HR | 95% CI | |||
| TNM Stage (III/IV) † | 2.430 | 1.254−4.711 | 0.009 | / | / | / |
| LNR (Higher) | 16.706 | 4.890−57.074 | <0.001 | 6.862 | 1.635−28.808 | 0.009 |
| PTL Reponse ‡ (Emphasized) | 0.531 | 0.317−0.890 | 0.016 | / | / | / |
| Perineural Invasion (Presence) | 2.988 | 1.563−5.709 | 0.001 | / | / | / |
| Tumor Deposits (Presence) | 3.254 | 1.652−6.409 | 0.001 | 3.089 | 1.447−6.593 | 0.004 |
| Tumor Budding (Presence) | 3.233 | 0.992−10.540 | 0.052 | / | / | / |
| C-D Classification Gradus III, IV, V | 2.528 | 1.574−4.061 | <0.001 | 2.609 | 1.437−4.737 | 0.002 |
| Hemoglobin (g/dL) | 0.844 | 0.723−0.985 | 0.031 | / | / | / |
| Hematocrit (%) | 0.938 | 0.885−0.994 | 0.030 | / | / | / |
| CRP (mg/L) | 1.009 | 1.003−1.016 | 0.006 | / | / | / |
| Serum Albumin (g/L) | 0.897 | 0.843−0.955 | 0.001 | / | / | / |
| CEA (ng/mL) | 1.010 | 1.000−1.019 | 0.041 | / | / | / |
| PLR | 1.002 | 1.000−1.005 | 0.045 | / | / | / |
| LANR | 0.946 | 0.898−0.996 | 0.035 | / | / | / |
| CAR | 1.335 | 1.102−1.617 | 0.003 | / | / | / |
| PNI | 0.924 | 0.877−0.974 | 0.003 | / | / | / |
| mGPS 2 | 2.145 | 1.431−3.215 | <0.001 | 2.188 | 1.413−3.387 | <0.001 |
| Parameters | Univariate | p Value | Multivariate | p Value | ||
|---|---|---|---|---|---|---|
| HR | 95% CI | HR | 95% CI | |||
| Age | 0.961 | 0.926−0.998 | 0.041 | / | / | / |
| TNM Stage (III/IV) † | 2.486 | 1.390−4.445 | 0.002 | 1.888 | 1.024−3.481 | 0.042 |
| LNR (Higher) | 5.588 | 0.835−37.388 | 0.076 | / | / | / |
| PTL Response (Emphasized) | 0.465 | 0.252−0.858 | 0.014 | 0.391 | 0.196−0.780 | 0.005 |
| Lymphovascular Invasion (Presence) | 2.322 | 0.936−5.756 | 0.069 | / | / | / |
| Perineural Invasion (Presence) | 2.374 | 1.064−5.299 | 0.035 | / | / | / |
| Tumor Deposits (Presence) | 4.194 | 1.869−9.411 | 0.001 | 3.049 | 1.206−7.706 | 0.018 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuk, V.; Karamarkovic, A.; Juloski, J.; Arbutina, D.; Radulovic, R.; Milic, L.; Kovacevic, B.; De Luka, S.; Grahovac, J. Prognostic Value of Combined Hematological/Biochemical Indexes and Tumor Clinicopathologic Features in Colorectal Cancer Patients—A Pilot Single Center Study. Cancers 2023, 15, 1761. https://doi.org/10.3390/cancers15061761
Cuk V, Karamarkovic A, Juloski J, Arbutina D, Radulovic R, Milic L, Kovacevic B, De Luka S, Grahovac J. Prognostic Value of Combined Hematological/Biochemical Indexes and Tumor Clinicopathologic Features in Colorectal Cancer Patients—A Pilot Single Center Study. Cancers. 2023; 15(6):1761. https://doi.org/10.3390/cancers15061761
Chicago/Turabian StyleCuk, Vladica, Aleksandar Karamarkovic, Jovan Juloski, Dragana Arbutina, Radosav Radulovic, Ljiljana Milic, Bojan Kovacevic, Silvio De Luka, and Jelena Grahovac. 2023. "Prognostic Value of Combined Hematological/Biochemical Indexes and Tumor Clinicopathologic Features in Colorectal Cancer Patients—A Pilot Single Center Study" Cancers 15, no. 6: 1761. https://doi.org/10.3390/cancers15061761
APA StyleCuk, V., Karamarkovic, A., Juloski, J., Arbutina, D., Radulovic, R., Milic, L., Kovacevic, B., De Luka, S., & Grahovac, J. (2023). Prognostic Value of Combined Hematological/Biochemical Indexes and Tumor Clinicopathologic Features in Colorectal Cancer Patients—A Pilot Single Center Study. Cancers, 15(6), 1761. https://doi.org/10.3390/cancers15061761