
Pragmatic, Prospective Comparative Effectiveness Trial of Carbon Ion Therapy, Surgery, and Proton Therapy for the Management of Pelvic Sarcomas (Soft Tissue/Bone) Involving the Bone: The PROSPER Study Rationale and Design
 , , , , ,
, , , , ,  ,
,  , ,
, , 
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
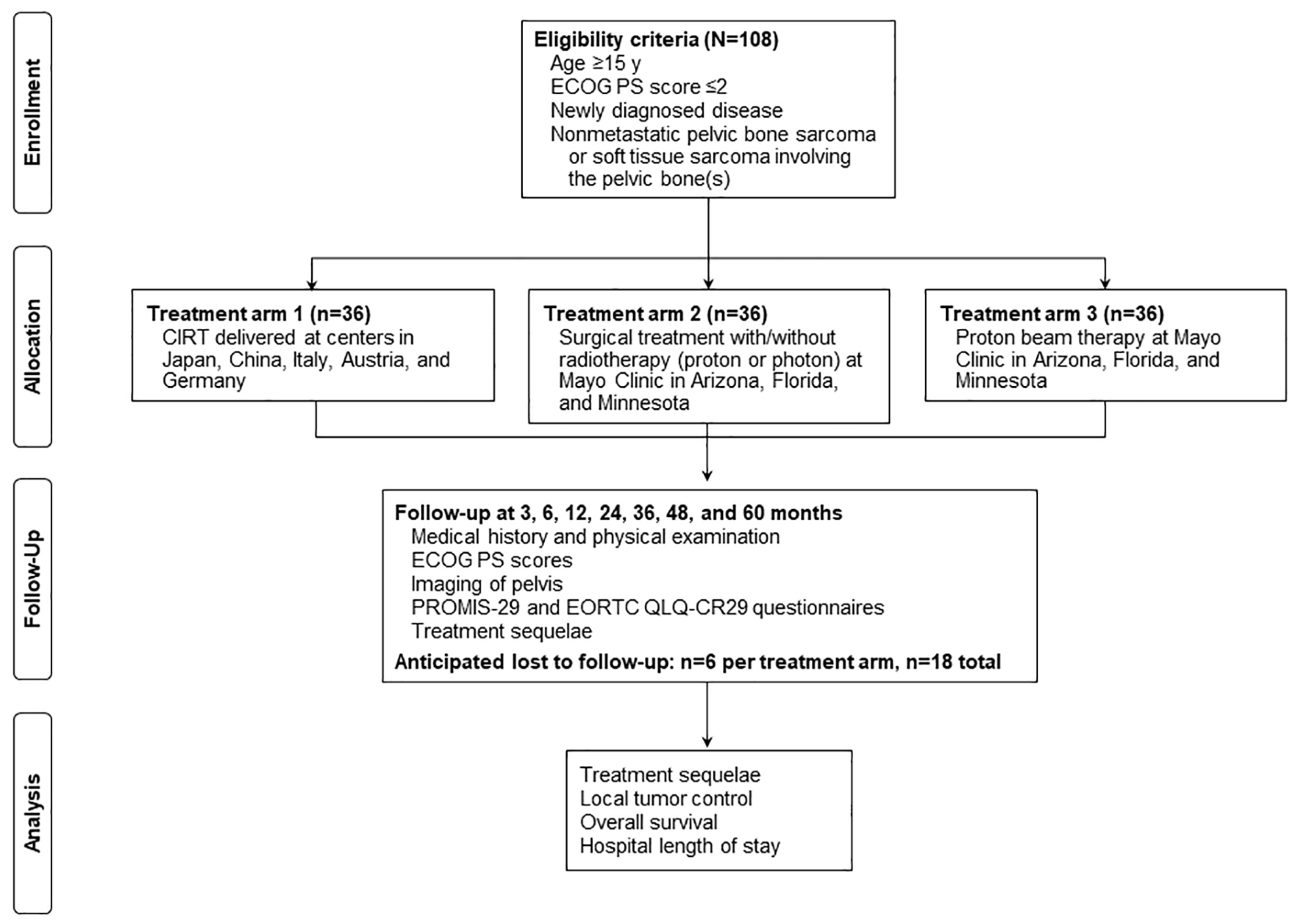
2. Research Methods and Analysis
2.1. Treatment Arm 1
2.2. Treatment Arm 2
2.3. Treatment Arm 3
2.4. Outcomes Measures
2.5. Follow-Up
2.6. Statistical Consideration
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Cancer Institute. Cancer Stat Facts: Bone and Joint Cancer 2022. Available online: https://seer.cancer.gov/statfacts/html/bones.html (accessed on 17 October 2022).
- Niu, X.; Xu, H.; Inwards, C.Y.; Li, Y.; Ding, Y.; Letson, G.D.; Bui, M.M. Primary Bone Tumors: Epidemiologic Comparison of 9200 Patients Treated at Beijing Ji Shui Tan Hospital, Beijing, China, with 10,165 Patients at Mayo Clinic, Rochester, Minnesota. Arch. Pathol. Lab. Med. 2015, 139, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Strauss, S.; Frezza, A.; Abecassis, N.; Bajpai, J.; Bauer, S.; Biagini, R.; Bielack, S.; Blay, J.; Bolle, S.; Bonvalot, S.; et al. Bone sarcomas: ESMO–EURACAN–GENTURIS–ERN PaedCan Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2021, 32, 1520–1536. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Guidelines: Bone Cancer v2.2023 2023. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1418 (accessed on 17 October 2022).
- Houdek, M.T.; Rose, P.S.; Hevesi, M.; Schwab, J.H.; Griffin, A.M.; Healey, J.H.; Petersen, I.A.; DeLaney, T.F.; Chung, P.W.; Yaszemski, M.J.; et al. Low dose radiotherapy is associated with local complications but not disease control in sacral chordoma. J. Surg. Oncol. 2019, 119, 856–863. [Google Scholar] [CrossRef] [PubMed]
- DeLaney, T.; Liebsch, N.; Goldberg, S.; Banfield, W.; Iokeim-Ioannidou, M.; Ahmed, S.; Schwab, J.H.; Hornicek, F.J.; Cote, G.; Shin, J.; et al. Definitive high-dose, proton-based radiation for unresected mobile spine and sacral chordomas. CTOS Annu. Meet. 2020, 171, 139–145. [Google Scholar] [CrossRef]
- Aibe, N.; Demizu, Y.; Sulaiman, N.S.; Matsuo, Y.; Mima, M.; Nagano, F.; Terashima, K.; Tokumaru, S.; Hayakawa, T.; Suga, M.; et al. Outcomes of Patients With Primary Sacral Chordoma Treated With Definitive Proton Beam Therapy. Int. J. Radiat. Oncol. 2018, 100, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.K.; Randall, R.L.; DuBois, S.G.; Harmsen, W.S.; Krailo, M.; Marcus, K.J.; Janeway, K.A.; Geller, D.S.; Sorger, J.I.; Womer, R.B.; et al. Identification of Patients with Localized Ewing Sarcoma at Higher Risk for Local Failure: A Report From the Children’s Oncology Group. Int. J. Radiat. Oncol. 2017, 99, 1286–1294. [Google Scholar] [CrossRef]
- Ozaki, T.; Flege, S.; Kevric, M.; Lindner, N.; Maas, R.; Delling, G.; Schwarz, R.; Von Hochstetter, A.R.; Salzer-Kuntschik, M.; Berdel, W.E.; et al. Osteosarcoma of the Pelvis: Experience of the Cooperative Osteosarcoma Study Group. J. Clin. Oncol. 2003, 21, 334–341. [Google Scholar] [CrossRef]
- Goulding, K.A.; Wilke, B.K.; Kiernan, H.C.; Houdek, M.T.; Sherman, C.E. Skeletal Sarcomas: Diagnosis, Treatment, and Follow-up from the Orthopedic Oncologist Perspective. Radiol. Clin. N. Am. 2022, 60, 193–203. [Google Scholar] [CrossRef]
- Stish, B.J.; Ahmed, S.K.; Rose, P.S.; Arndt, C.A.; Laack, N.N. Patient-Reported Functional and Quality of Life Outcomes in a Large Cohort of Long-Term Survivors of Ewing Sarcoma. Pediatr. Blood Cancer 2015, 62, 2189–2196. [Google Scholar] [CrossRef] [PubMed]
- Outani, H.; Hamada, K.; Imura, Y.; Oshima, K.; Sotobori, T.; Demizu, Y.; Kakunaga, S.; Joyama, S.; Imai, R.; Okimoto, T.; et al. Comparison of clinical and functional outcome between surgical treatment and carbon ion radiotherapy for pelvic chondrosarcoma. Int. J. Clin. Oncol. 2016, 21, 186–193. [Google Scholar] [CrossRef]
- Elsässer, T.; Krämer, M.; Scholz, M. Accuracy of the Local Effect Model for the Prediction of Biologic Effects of Carbon Ion Beams In Vitro and In Vivo. Int. J. Radiat. Oncol. 2008, 71, 866–872. [Google Scholar] [CrossRef] [PubMed]
- DeLaney, T.F.; Liebsch, N.J.; Pedlow, F.X.; Adams, J.; Weyman, E.A.; Yeap, B.Y.; Depauw, N.; Nielsen, G.P.; Harmon, D.C.; Yoon, S.S.; et al. Long-term results of Phase II study of high dose photon/proton radiotherapy in the management of spine chordomas, chondrosarcomas, and other sarcomas. J. Surg. Oncol. 2014, 110, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Uezono, H.; Indelicato, D.J.; Rotondo, R.L.; Vega, R.B.M.; Bradfield, S.M.; Morris, C.G.; Bradley, J.A. Treatment Outcomes After Proton Therapy for Ewing Sarcoma of the Pelvis. Int. J. Radiat. Oncol. 2020, 107, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Indelicato, D.J.; Rotondo, R.L.; Krasin, M.J.; Vega, R.B.M.; Uezono, H.; Bradfield, S.; Agarwal, V.; Morris, C.G.; Bradley, J.A. Outcomes Following Proton Therapy for Group III Pelvic Rhabdomyosarcoma. Int. J. Radiat. Oncol. 2020, 106, 968–976. [Google Scholar] [CrossRef] [PubMed]
- Ciernik, I.F.; Niemierko, A.; Harmon, D.C.; Kobayashi, W.; Chen, Y.-L.; Yock, T.I.; Ebb, D.H.; Choy, E.; Raskin, K.A.; Liebsch, N.; et al. Proton-based radiotherapy for unresectable or incompletely resected osteosarcoma. Cancer 2011, 117, 4522–4530. [Google Scholar] [CrossRef] [PubMed]
- Hamada, N.; Imaoka, T.; Masunaga, S.-I.; Ogata, T.; Okayasu, R.; Takahashi, A.; Kato, T.A.; Kobayashi, Y.; Ohnishi, T.; Ono, K.; et al. Recent Advances in the Biology of Heavy-Ion Cancer Therapy. J. Radiat. Res. 2010, 51, 365–383. [Google Scholar] [CrossRef]
- Malouff, T.D.; Mahajan, A.; Krishnan, S.; Beltran, C.; Seneviratne, D.S.; Trifiletti, D.M. Carbon Ion Therapy: A Modern Review of an Emerging Technology. Front. Oncol. 2020, 10, 82. [Google Scholar] [CrossRef]
- Demizu, Y.; Imai, R.; Kiyohara, H.; Matsunobu, A.; Okamoto, M.; Okimoto, T.; Tsuji, H.; Ohno, T.; Shioyama, Y.; Nemoto, K.; et al. Carbon ion radiotherapy for sacral chordoma: A retrospective nationwide multicentre study in Japan. Radiother. Oncol. 2021, 154, 1–5. [Google Scholar] [CrossRef]
- Imai, R.; Kamada, T.; Sugahara, S.; Tsuji, H. Carbon ion radiotherapy for sacral chordoma. Br. J. Radiol. 2011, 84, S48–S54. [Google Scholar] [CrossRef]
- Imai, R.; Kamada, T.; Tsuji, H.; Sugawara, S.; Serizawa, I.; Tsujii, H.; Tatezaki, S.-I. Effect of Carbon Ion Radiotherapy for Sacral Chordoma: Results of Phase I-II and Phase II Clinical Trials. Int. J. Radiat. Oncol. 2010, 77, 1470–1476. [Google Scholar] [CrossRef]
- Cuccia, F.; Fiore, M.R.; Barcellini, A.; Iannalfi, A.; Vischioni, B.; Ronchi, S.; Bonora, M.; Riva, G.; Vai, A.; Facoetti, A.; et al. Outcome and Toxicity of Carbon Ion Radiotherapy for Axial Bone and Soft Tissue Sarcomas. Anticancer Res. 2020, 40, 2853–2859. [Google Scholar] [CrossRef]
- Imai, R.; Kamada, T.; Araki, N.; The Working Group for Bone and Soft Tissue Sarcoma. Clinical Efficacy of Carbon Ion Radiotherapy for Unresectable Chondrosarcomas. Anticancer Res. 2017, 37, 6959–6964. [Google Scholar] [CrossRef] [PubMed]
- Mohamad, O.; Imai, R.; Kamada, T.; Nitta, Y.; Araki, N.; The Working Group for Bone and Soft Tissue Sarcoma. Carbon ion radiotherapy for inoperable pediatric osteosarcoma. Oncotarget 2018, 9, 22976–22985. [Google Scholar] [CrossRef] [PubMed]
- Bostel, T.; Mattke, M.; Nicolay, N.H.; Welzel, T.; Wollschläger, D.; Akbaba, S.; Mayer, A.; Sprave, T.; Debus, J.; Uhl, M. High-dose carbon-ion based radiotherapy of primary and recurrent sacrococcygeal chordomas: Long-term clinical results of a single particle therapy center. Radiat. Oncol. 2020, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Liu, R.; Zhang, Q.; Luo, H.; Wang, D.; Wang, Y.; Chen, J.; Ou, Y.; Wang, X. Efficacy and safety of carbon ion radiotherapy for bone sarcomas: A systematic review and meta-analysis. Radiat. Oncol. 2022, 17, 206. [Google Scholar] [CrossRef]
- Yolcu, Y.U.; Zreik, J.; Wahood, W.; Bhatti, A.U.R.; Bydon, M.; Houdek, M.T.; Rose, P.S.; Mahajan, A.; Petersen, I.A.; Haddock, M.G.; et al. Comparison of Oncologic Outcomes and Treatment-Related Toxicity of Carbon Ion Radiotherapy and En Bloc Resection for Sacral Chordoma. JAMA Netw. Open 2022, 5, e2141927. [Google Scholar] [CrossRef]
- Lazar, A.A.; Schulte, R.; Faddegon, B.; Blakely, E.A.; Roach, M. Clinical trials involving carbon-ion radiation therapy and the path forward. Cancer 2018, 124, 4467–4476. [Google Scholar] [CrossRef]
- Yi, S.K.; Mak, W.; Yang, C.C.; Liu, T.; Cui, J.; Chen, A.M.; Purdy, J.A.; Monjazeb, A.M.; Do, L. Development of a Standardized Method for Contouring the Lumbosacral Plexus: A Preliminary Dosimetric Analysis of this Organ at Risk Among 15 Patients Treated With Intensity-Modulated Radiotherapy for Lower Gastrointestinal Cancers and the Incidence of Radiation-Induced Lumbosacral Plexopathy. Int. J. Radiat. Oncol. 2012, 84, 376–382. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoppe, B.S.; Petersen, I.A.; Wilke, B.K.; DeWees, T.A.; Imai, R.; Hug, E.B.; Fiore, M.R.; Debus, J.; Fossati, P.; Yamada, S.; et al. Pragmatic, Prospective Comparative Effectiveness Trial of Carbon Ion Therapy, Surgery, and Proton Therapy for the Management of Pelvic Sarcomas (Soft Tissue/Bone) Involving the Bone: The PROSPER Study Rationale and Design. Cancers 2023, 15, 1660. https://doi.org/10.3390/cancers15061660
Hoppe BS, Petersen IA, Wilke BK, DeWees TA, Imai R, Hug EB, Fiore MR, Debus J, Fossati P, Yamada S, et al. Pragmatic, Prospective Comparative Effectiveness Trial of Carbon Ion Therapy, Surgery, and Proton Therapy for the Management of Pelvic Sarcomas (Soft Tissue/Bone) Involving the Bone: The PROSPER Study Rationale and Design. Cancers. 2023; 15(6):1660. https://doi.org/10.3390/cancers15061660
Chicago/Turabian StyleHoppe, Bradford S., Ivy A. Petersen, Benjamin K. Wilke, Todd A. DeWees, Reiko Imai, Eugen B. Hug, Maria Rosaria Fiore, Jürgen Debus, Piero Fossati, Shigeru Yamada, and et al. 2023. "Pragmatic, Prospective Comparative Effectiveness Trial of Carbon Ion Therapy, Surgery, and Proton Therapy for the Management of Pelvic Sarcomas (Soft Tissue/Bone) Involving the Bone: The PROSPER Study Rationale and Design" Cancers 15, no. 6: 1660. https://doi.org/10.3390/cancers15061660
APA StyleHoppe, B. S., Petersen, I. A., Wilke, B. K., DeWees, T. A., Imai, R., Hug, E. B., Fiore, M. R., Debus, J., Fossati, P., Yamada, S., Orlandi, E., Zhang, Q., Bao, C., Seidensaal, K., May, B. C., Harrell, A. C., Houdek, M. T., Vallow, L. A., Rose, P. S., ... Ahmed, S. K. (2023). Pragmatic, Prospective Comparative Effectiveness Trial of Carbon Ion Therapy, Surgery, and Proton Therapy for the Management of Pelvic Sarcomas (Soft Tissue/Bone) Involving the Bone: The PROSPER Study Rationale and Design. Cancers, 15(6), 1660. https://doi.org/10.3390/cancers15061660