
Association between Age at Helicobacter pylori Eradication and the Risk of Gastric Cancer Stratified by Family History of Gastric Cancer: A Nationwide Population-Based Study
 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
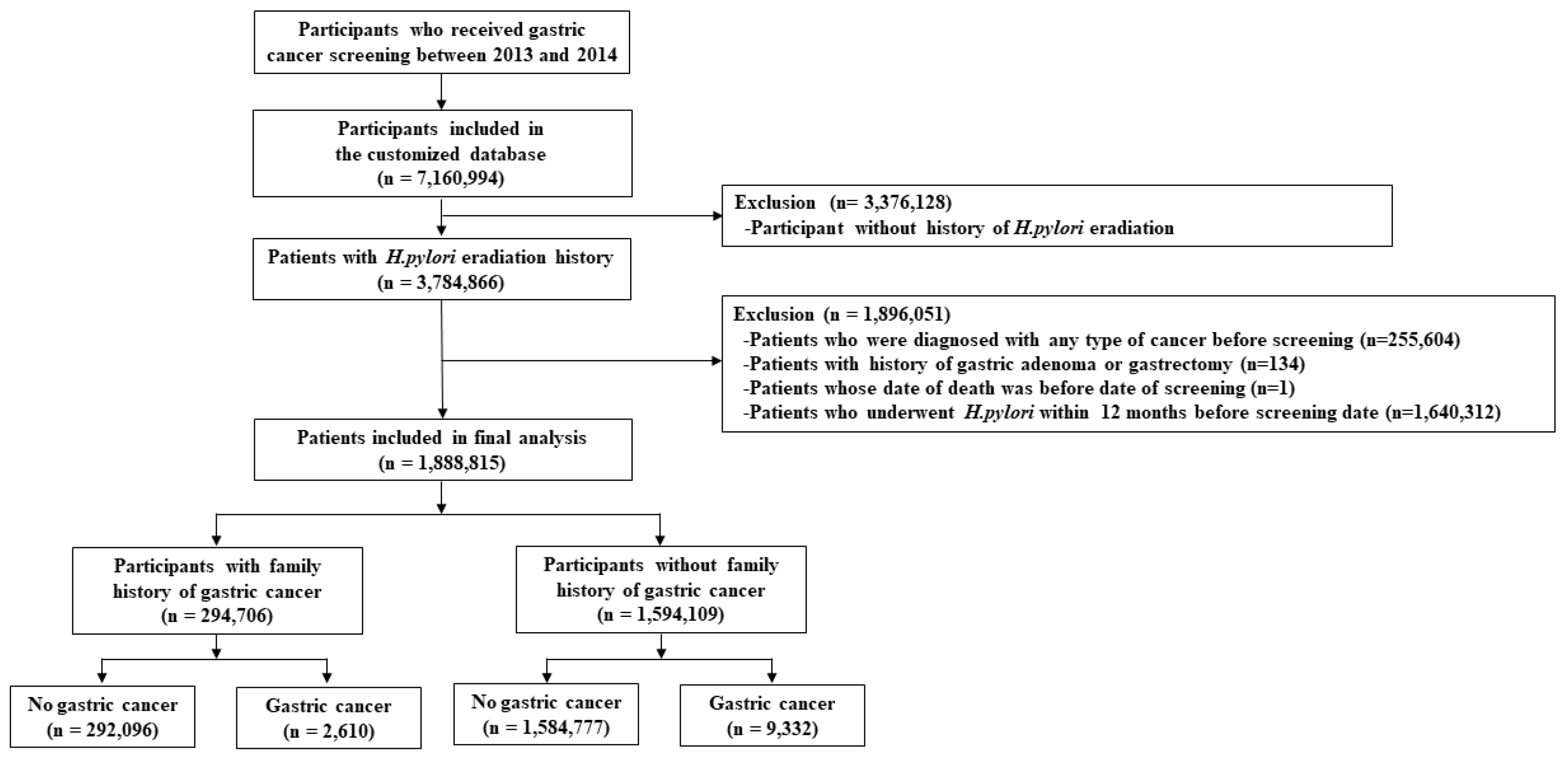
2.1. Data Source and Identification of the Study Population
2.2. Main Outcome and Definition of Variables
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
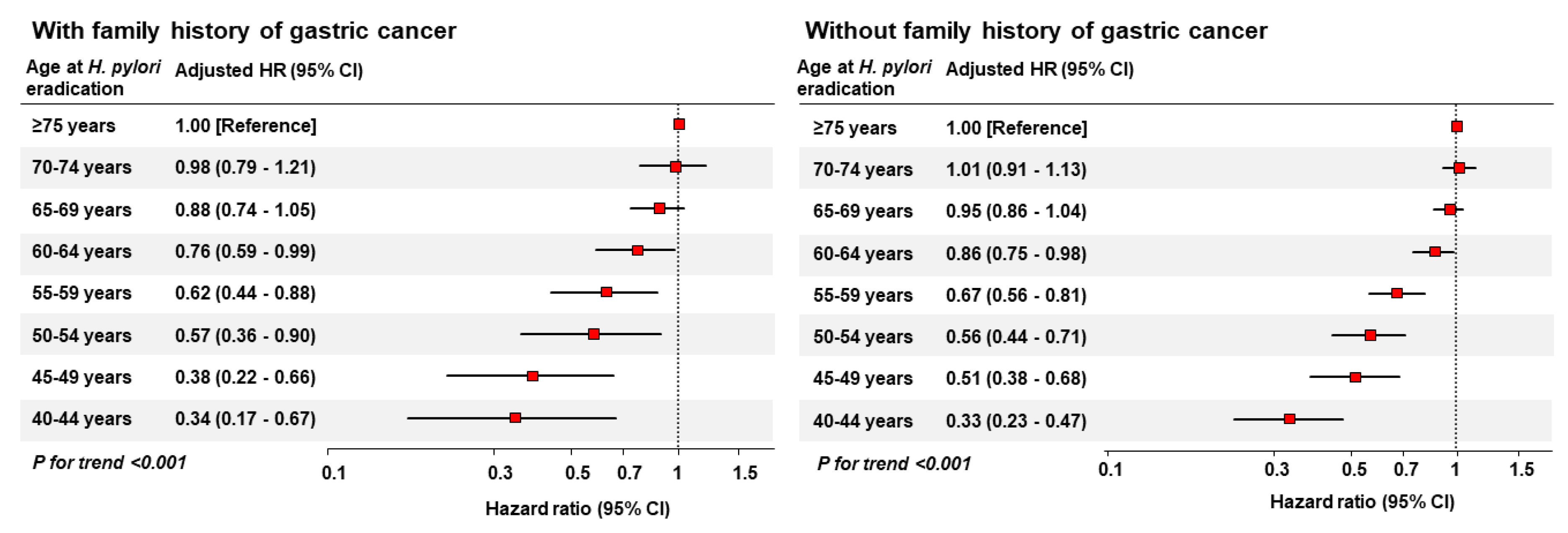
3.2. Risk of GC According to Age at H. pylori Eradication in Patients with a Family History
3.3. Risk of GC According to Age at H. pylori Eradication in Patients without a Family History
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.A.; Brawley, O.W. Association of Helicobacter pylori infection with gastric cancer. Mil. Med. 2000, 165, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Fuccio, L.; Zagari, R.M.; Eusebi, L.H.; Laterza, L.; Cennamo, V.; Ceroni, L.; Grilli, D.; Bazzoli, F. Meta-analysis: Can Helicobacter pylori eradication treatment reduce the risk for gastric cancer? Ann. Intern. Med. 2009, 151, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Forman, D.; Hunt, R.H.; Yuan, Y.; Moayyedi, P. Helicobacter pylori eradication therapy to prevent gastric cancer in healthy asymptomatic infected individuals: Systematic review and meta-analysis of randomised controlled trials. BMJ 2014, 348, g3174. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Yuan, Y.; Moayyedi, P. Helicobacter pylori eradication therapy to prevent gastric cancer: Systematic review and meta-analysis. Gut 2020, 69, 2113–2121. [Google Scholar] [CrossRef]
- Park, J.S.; Jun, J.S.; Seo, J.H.; Youn, H.S.; Rhee, K.H. Changing prevalence of Helicobacter pylori infection in children and adolescents. Clin. Exp. Pediatr. 2021, 64, 21–25. [Google Scholar] [CrossRef]
- Chen, H.N.; Wang, Z.; Li, X.; Zhou, Z.G. Helicobacter pylori eradication cannot reduce the risk of gastric cancer in patients with intestinal metaplasia and dysplasia: Evidence from a meta-analysis. Gastric Cancer 2016, 19, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Rokkas, T.; Rokka, A.; Portincasa, P. A systematic review and meta-analysis of the role of Helicobacter pylori eradication in preventing gastric cancer. Ann. Gastroenterol. 2017, 30, 414–423. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef]
- Bahk, J.; Kim, Y.Y.; Kang, H.Y.; Lee, J.; Kim, I.; Lee, J.; Yun, S.C.; Park, J.H.; Shin, S.A.; Khang, Y.H. Using the National Health Information Database of the National Health Insurance Service in Korea for Monitoring Mortality and Life Expectancy at National and Local Levels. J. Korean Med. Sci. 2017, 32, 1764–1770. [Google Scholar] [CrossRef]
- Cheol Seong, S.; Kim, Y.Y.; Khang, Y.H.; Heon Park, J.; Kang, H.J.; Lee, H.; Do, C.H.; Song, J.S.; Hyon Bang, J.; Ha, S.; et al. Data Resource Profile: The National Health Information Database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar] [CrossRef]
- Yaghoobi, M.; McNabb-Baltar, J.; Bijarchi, R.; Hunt, R.H. What is the quantitative risk of gastric cancer in the first-degree relatives of patients? A meta-analysis. World J. Gastroenterol. 2017, 23, 2435–2442. [Google Scholar] [CrossRef]
- Vitelli-Storelli, F.; Rubin-Garcia, M.; Pelucchi, C.; Benavente, Y.; Bonzi, R.; Rota, M.; Palli, D.; Ferraroni, M.; Lunet, N.; Morais, S.; et al. Family History and Gastric Cancer Risk: A Pooled Investigation in the Stomach Cancer Pooling (STOP) Project Consortium. Cancers 2021, 13, 3844. [Google Scholar] [CrossRef]
- Yang, M.S.; Park, M.; Back, J.H.; Lee, G.H.; Shin, J.H.; Kim, K.; Seo, H.J.; Kim, Y.A. Validation of Cancer Diagnosis Based on the National Health Insurance Service Database versus the National Cancer Registry Database in Korea. Cancer Res. Treat. 2022, 54, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, Y.J.; Seo, S.I.; Shin, W.G.; Park, C.H. Impact of the timing of Helicobacter pylori eradication on the risk of development of metachronous lesions after treatment of early gastric cancer: A population-based cohort study. Gastrointest. Endosc. 2020, 92, 613–622.e611. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.J. A Class of K-Sample Tests for Comparing the Cumulative Incidence of a Competing Risk. Ann. Stat. 1988, 16, 1141–1154. [Google Scholar] [CrossRef]
- Fox, J.G.; Wang, T.C. Inflammation, atrophy, and gastric cancer. J. Clin. Investig. 2007, 117, 60–69. [Google Scholar] [CrossRef]
- Karbalaei, M.; Keikha, M. Statistical proof of Helicobacter pylori eradication in preventing metachronous gastric cancer after endoscopic resection in an East Asian population. World J. Gastrointest. Surg. 2022, 14, 867–873. [Google Scholar] [CrossRef]
- Yanaoka, K.; Oka, M.; Ohata, H.; Yoshimura, N.; Deguchi, H.; Mukoubayashi, C.; Enomoto, S.; Inoue, I.; Iguchi, M.; Maekita, T.; et al. Eradication of Helicobacter pylori prevents cancer development in subjects with mild gastric atrophy identified by serum pepsinogen levels. Int. J. Cancer 2009, 125, 2697–2703. [Google Scholar] [CrossRef]
- Kato, M.; Hayashi, Y.; Nishida, T.; Oshita, M.; Nakanishi, F.; Yamaguchi, S.; Kitamura, S.; Nishihara, A.; Akasaka, T.; Ogiyama, H.; et al. Helicobacter pylori eradication prevents secondary gastric cancer in patients with mild-to-moderate atrophic gastritis. J. Gastroenterol. Hepatol. 2021, 36, 2083–2090. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Metz, D.C.; Ellenberg, S.; Kaplan, D.E.; Goldberg, D.S. Risk Factors and Incidence of Gastric Cancer After Detection of Helicobacter pylori Infection: A Large Cohort Study. Gastroenterology 2020, 158, 527–536.e527. [Google Scholar] [CrossRef]
- Leung, W.K.; Wong, I.O.L.; Cheung, K.S.; Yeung, K.F.; Chan, E.W.; Wong, A.Y.S.; Chen, L.; Wong, I.C.K.; Graham, D.Y. Effects of Helicobacter pylori Treatment on Incidence of Gastric Cancer in Older Individuals. Gastroenterology 2018, 155, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Chen, H.; Zhang, Y.; Yin, X.; Man, J.; Yang, X.; Lu, M. Global changing trends in incidence and mortality of gastric cancer by age and sex, 1990–2019: Findings from Global Burden of Disease Study. J. Cancer 2021, 12, 6695–6705. [Google Scholar] [CrossRef] [PubMed]
- Choi, I.J.; Kim, C.G.; Lee, J.Y.; Kim, Y.I.; Kook, M.C.; Park, B.; Joo, J. Family History of Gastric Cancer and Helicobacter pylori Treatment. N. Engl. J. Med. 2020, 382, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.G.; Jung, H.K.; Lee, H.L.; Jang, J.Y.; Lee, H.; Kim, C.G.; Shin, W.G.; Shin, E.S.; Lee, Y.C.; Korean College of Helicobacter and Upper Gastrointestinal Research. Guidelines for the diagnosis and treatment of Helicobacter pylori infection in Korea, 2013 revised edition. J. Gastroenterol. Hepatol. 2014, 29, 1371–1386. [Google Scholar] [CrossRef] [PubMed]
- Liou, J.M.; Lee, Y.C.; El-Omar, E.M.; Wu, M.S. Efficacy and Long-Term Safety of H. pylori Eradication for Gastric Cancer Prevention. Cancers 2019, 11, 593. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Family History of GC (n = 294,706) | No Family History of GC (n = 1,594,109) | p-Value |
|---|---|---|---|
| Age at screening (years) | 57.1 ± 9.7 | 57.1 ± 9.8 | <0.001 |
| Age group at screening | |||
| 40–49 years | 66,376 (22.5) | 367,285 (23.0) | <0.001 |
| 50–59 years | 109,451 (37.1) | 579,176 (36.3) | |
| 60–69 years | 82,100 (27.9) | 440,026 (27.6) | |
| ≥70 years | 36,779 (12.5) | 207,622 (13.0) | |
| Sex | |||
| Female | 123,644 (42.0) | 613,556 (38.5) | <0.001 |
| Male | 171,062 (58.0) | 980,553 (61.5) | |
| Obesity (BMI ≥ 25 kg/m2) | |||
| No | 190,779 (64.7) | 1,021,777 (64.1) | <0.001 |
| Yes | 103,902 (35.3) | 572,168 (35.9) | |
| Unknown | 25 (0.0) | 164 (0.0) | |
| Smoking habit | |||
| Never | 195,926 (66.5) | 1,115,474 (70.0) | <0.001 |
| Former | 51,370 (17.4) | 232,825 (14.6) | |
| Current | 47,309 (16.1) | 245,282 (15.4) | |
| Unknown | 101 (0.0) | 528 (0.0) | |
| Alcohol consumption | |||
| 0 or 1 time per week | 227,576 (77.2) | 1,252,957 (78.6) | <0.001 |
| ≥2 times per week | 66,897 (22.7) | 340,069 (21.3) | |
| Unknown | 233 (0.1) | 1083 (0.1) | |
| Physical activity | |||
| No | 66,836 (22.7) | 394,668 (24.8) | <0.001 |
| Yes (≥1 time per week) | 227,552 (77.2) | 1,197,894 (75.2) | |
| Unknown | 318 (0.1) | 1547 (0.1) | |
| Comorbidities | |||
| Hypertension | 80,762 (27.4) | 462,299 (29.0) | <0.001 |
| Diabetes mellitus | 30,353 (10.3) | 170,240 (10.7) | |
| Dyslipidemia | 23,646 (8.0) | 120,842 (7.6) | |
| Ischemic heart disease | 11,569 (3.9) | 61,131 (3.8) | |
| Stroke | 3656 (1.2) | 19,605 (1.2) | |
| Comorbidity status (yes) | 108,743 (36.9) | 606,308 (38.0) | <0.001 |
| Indication for H. pylori eradication | |||
| Gastric ulcer | 61,147 (20.7) | 320,248 (20.1) | <0.001 |
| Duodenal ulcer | 15,229 (5.2) | 79,547 (5.0) | |
| Gastric and duodenal ulcer a | 13,469 (4.6) | 74,606 (4.7) | |
| Gastric MALT lymphoma | 4 (0.0) | 3 (0.0) | |
| H. pylori-associated gastritis | 204,857 (69.5) | 1,119,705 (70.2) |
| Variables | N | Person–Years | Incidence (95% CI) a | Crude HR (95% CI) | Adjusted HR (95% CI) |
|---|---|---|---|---|---|
| Age at H. pylori eradication | |||||
| ≥75 years | 214 | 45,998 | 4.65 (4.03–5.28) | 1 (Reference) | 1 (Reference) |
| 70–74 years | 287 | 69,429 | 4.13 (3.66–4.61) | 0.89 (0.75–1.06) | 0.98 (0.79–1.21) |
| 65–69 years | 553 | 172,833 | 3.20 (2.93–3.47) | 0.69 (0.59–0.81) | 0.88 (0.74–1.05) |
| 60–64 years | 396 | 162,193 | 2.44 (2.20–2.68) | 0.52 (0.44–0.62) | 0.76 (0.59–0.99) |
| 55–59 years | 544 | 314,374 | 1.73 (1.59–1.88) | 0.37 (0.32–0.44) | 0.62 (0.44–0.88) |
| 50–54 years | 311 | 225,437 | 1.38 (1.23–1.53) | 0.30 (0.25–0.35) | 0.57 (0.36–0.90) |
| 45–49 years | 157 | 187,873 | 0.84 (0.70–0.97) | 0.18 (0.15–0.22) | 0.38 (0.22–0.66) |
| 40–44 years | 148 | 229,125 | 0.65 (0.54–0.75) | 0.14 (0.11–0.17) | 0.34 (0.17–0.67) |
| p for trend | <0.001 | <0.001 | |||
| Age at screening, per year | 1.06 (1.06–1.06) | 1.03 (1.01–1.05) | |||
| Sex | |||||
| Female | 970 | 822,475 | 1.18 (1.11–1.25) | 1 (Reference) | 1 (Reference) |
| Male | 1640 | 584,787 | 2.80 (2.67–2.94) | 2.37 (2.19–2.57) | 2.09 (1.88–2.34) |
| Obesity (BMI ≥ 25 kg/m2) | |||||
| No | 1681 | 910,886 | 1.85 (1.76–1.93) | 1 (Reference) | 1 (Reference) |
| Yes | 928 | 496,257 | 1.87 (1.75–1.99) | 1.01 (0.94–1.10) | 0.95 (0.87–1.03) |
| Smoking habit | |||||
| Never | 1348 | 940,476 | 1.43 (1.36–1.51) | 1 (Reference) | 1 (Reference) |
| Former | 700 | 243,307 | 2.88 (2.66–3.09) | 2.00 (1.83–2.19) | 1.17 (1.04–1.31) |
| Current | 561 | 222,999 | 2.52 (2.31– 2.72) | 1.75 (1.59–1.93) | 1.38 (1.22–1.56) |
| Alcohol consumption | |||||
| 0 or 1 time/week | 1869 | 1,089,055 | 1.72 (1.64–1.79) | 1 (Reference) | 1 (Reference) |
| ≥2 times/week | 740 | 317,127 | 2.33 (2.17–2.50) | 1.36 (1.25–1.48) | 1.08 (0.98–1.19) |
| Physical activity | |||||
| No | 603 | 320,047 | 1.88 (1.73–2.03) | 1 (Reference) | 1 (Reference) |
| Yes (≥1 time/week) | 2000 | 1,085,671 | 1.84 (1.76–1.92) | 0.98 (0.89–1.07) | 0.97 (0.88–1.06) |
| Comorbidity status b | |||||
| No | 1353 | 887,775 | 1.52 (1.44–1.61) | 1 (Reference) | 1 (Reference) |
| Yes | 1257 | 519,487 | 2.42 (2.29–2.55) | 1.59 (1.47–1.72) | 1.03 (0.95–1.12) |
| Variables | N | Person–Years | Incidence (95% CI) a | Crude HR (95% CI) | Adjusted HR (95% CI) |
|---|---|---|---|---|---|
| Age at H. pylori eradication | |||||
| ≥75 years | 827 | 262,139 | 3.15 (2.94–3.37) | 1 (Reference) | 1 (Reference) |
| 70–74 years | 1027 | 390,647 | 2.63 (2.47–2.79) | 0.84 (0.76–0.92) | 1.01 (0.91–1.13) |
| 65–69 years | 2039 | 953,595 | 2.14 (2.05–2.23) | 0.68 (0.63–0.74) | 0.95 (0.86–1.04) |
| 60–64 years | 1462 | 861,892 | 1.70 (1.61–1.78) | 0.54 (0.49–0.59) | 0.86 (0.75–0.98) |
| 55–59 years | 1884 | 1,669,636 | 1.13 (1.08–1.18) | 0.36 (0.33–0.39) | 0.67 (0.56–0.81) |
| 50–54 years | 953 | 1,181,730 | 0.81 (0.76–0.86) | 0.26 (0.23–0.28) | 0.56 (0.44–0.71) |
| 45–49 years | 663 | 988,615 | 0.67 (0.62–0.72) | 0.21 (0.19–0.24) | 0.51 (0.38–0.68) |
| 40–44 years | 477 | 1,285,235 | 0.37 (0.34–0.40) | 0.12 (0.11–0.13) | 0.33 (0.23–0.47) |
| p for trend | <0.001 | <0.001 | |||
| Age at screening, per year | 1.06 (1.06–1.06) | 1.03 (1.02–1.04) | |||
| Sex | |||||
| Female | 3539 | 4,700,031 | 0.75 (0.73–0.78) | 1 (Reference) | 1 (Reference) |
| Male | 5793 | 2,893,458 | 2.00 (1.95–2.05) | 2.65 (2.54–2.76) | 2.35 (2.23–2.49) |
| Obesity (BMI ≥ 25 kg/m2) | |||||
| No | 5800 | 4,865,695 | 1.19 (1.16–1.22) | 1 (Reference) | 1 (Reference) |
| Yes | 3531 | 2,727,062 | 1.29 (1.25–1.34) | 1.09 (1.04–1.13) | 1.02 (0.98–1.07) |
| Smoking habit | |||||
| Never | 5094 | 5,336,735 | 0.95 (0.93–0.98) | 1 (Reference) | 1 (Reference) |
| Former | 2140 | 1,099,546 | 1.95 (1.86–2.03) | 2.03 (1.93–2.14) | 1.12 (1.05–1.19) |
| Current | 2094 | 1,154,625 | 1.81 (1.74–1.89) | 1.90 (1.80–1.99) | 1.39 (1.31–1.48) |
| Alcohol consumption | |||||
| 0 or 1 time/week | 6741 | 5,979,969 | 1.13 (1.10–1.15) | 1 (Reference) | 1 (Reference) |
| ≥2 times/week | 2589 | 1,608,489 | 1.61 (1.55–1.67) | 1.43 (1.36–1.49) | 1.06 (1.01–1.12) |
| Physical activity | |||||
| No | 2496 | 1,884,265 | 1.32 (1.27–1.38) | 1 (Reference) | 1 (Reference) |
| Yes (≥1 time/week) | 6827 | 5,701,664 | 1.20 (1.17–1.23) | 0.90 (0.86–0.94) | 0.92 (0.88–0.97) |
| Comorbidity status b | |||||
| No | 4699 | 4,704,372 | 1.00 (0.97–1.03) | 1 (Reference) | 1 (Reference) |
| Yes | 4633 | 2,889,117 | 1.60 (1.56–1.65) | 1.61 (1.54–1.67) | 1.02 (0.98–1.06) |
| Factors | H. pylori Eradication Regimen | |||||
|---|---|---|---|---|---|---|
| Standard Triple Therapy a | Sequential or Concomitant Therapy b | p-Value | ||||
| n | % | n | % | |||
| n = 1,757,599 | n = 127,566 | |||||
| Characteristics | ||||||
| Family history status | ||||||
| No | 1,483,863 | 84.4 | 107,309 | 84.1 | 0.004 | |
| Yes | 273,736 | 15.6 | 20,257 | 15.9 | ||
| Age group | ||||||
| ≥75 years | 63,261 | 3.6 | 2437 | 1.9 | <0.001 | |
| 70–74 years | 92,193 | 5.2 | 3841 | 3.0 | ||
| 65–69 years | 223,100 | 12.7 | 10,609 | 8.3 | ||
| 60–64 years | 202,709 | 11.5 | 11,110 | 8.7 | ||
| 55–59 years | 387,240 | 22.0 | 25,883 | 20.3 | ||
| 50–54 years | 271,491 | 15.4 | 22,461 | 17.6 | ||
| 45–49 years | 227,723 | 13.0 | 21,077 | 16.5 | ||
| 40–44 years | 289,882 | 16.5 | 30,148 | 23.6 | ||
| Cancer development | ||||||
| No | 1,746,513 | 99.4 | 126,745 | 99.4 | 0.312 | |
| Yes | 11,086 | 0.6 | 821 | 0.6 | ||
| Risk of gastric cancer development | ||||||
| Crude HR | Reference | 1.22 (1.13–1.31) | ||||
| Adjusted HR c | Reference | 1.62 (1.16–2.25) | ||||
| Variables | N | Crude HR (95% CI) | Adjusted HR a (95% CI) |
|---|---|---|---|
| Total | |||
| Age at H. pylori eradication | n = 6899 | ||
| ≥60 years | 3756 | 1 (Reference) | 1 (Reference) |
| 55–59 years | 1292 | 0.64 (0.60–0.68) | 0.72 (0.66–0.78) |
| 50–54 years | 1130 | 0.47 (0.44–0.51) | 0.56 (0.50–0.63) |
| 45–49 years | 439 | 0.29 (0.26–0.32) | 0.35 (0.30–0.41) |
| 40–44 years | 282 | 0.14 (0.13–0.16) | 0.18 (0.15–0.22) |
| p for trend | <0.001 | <0.001 | |
| With family history | |||
| Age at H. pylori eradication | n = 1450 | ||
| ≥60 years | 775 | 1 (Reference) | 1 (Reference) |
| 55–59 years | 264 | 0.62 (0.54–0.71) | 0.68 (0.56–0.82) |
| 50–54 years | 251 | 0.49 (0.43–0.57) | 0.57 (0.45–0.73) |
| 45–49 years | 96 | 0.29 (0.24–0.36) | 0.35 (0.25–0.49) |
| 40–44 years | 64 | 0.16 (0.12–0.21) | 0.20 (0.13–0.31) |
| p for trend | <0.001 | <0.001 | |
| Without family history | |||
| Age at H. pylori eradication | n = 5449 | ||
| ≥60 years | 2981 | 1 (Reference) | 1 (Reference) |
| 55–59 years | 1028 | 0.65 (0.60–0.69) | 0.73 (0.66–0.80) |
| 50–54 years | 879 | 0.47 (0.43–0.50) | 0.56 (0.49–0.63) |
| 45–49 years | 343 | 0.28 (0.25–0.32) | 0.35 (0.30–0.42) |
| 40–44 years | 218 | 0.14 (0.12–0.16) | 0.18 (0.15–0.22) |
| p for trend | <0.001 | <0.001 | |
| Age at H. pylori Eradication a | Total Population | With Family History | Without Family History | ||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) b | p c | HR (95% CI) b | p c | HR (95% CI) b | p c | ||
| 40–44 | Age 44→45 | Ref. | <0.001 | Ref. | 0.353 | Ref. | <0.001 |
| Age 43→45 | 0.98 (0.75–1.29) | 1.24 (0.71–2.16) | 0.91 (0.67–1.25) | ||||
| Age 42→45 | 0.86 (0.67–1.11) | 0.83 (0.48–1.43) | 0.87 (0.66–1.15) | ||||
| Age 41→45 | 0.78 (0.58–1.06) | 1.16 (0.64–2.09) | 0.68 (0.47–0.97) | ||||
| Age 40→45 | 0.70 (0.56–0.86) | 0.85 (0.54–1.34) | 0.66 (0.52–0.83) | ||||
| 45–49 | Age 49→50 | Ref. | 0.308 | Ref. | 0.693 | Ref. | 0.345 |
| Age 48→50 | 1.09 (0.89–1.33) | 1.10 (0.68–1.75) | 1.09 (0.87–1.36) | ||||
| Age 47→50 | 1.15 (0.92–1.44) | 1.14 (0.68–1.92) | 1.15 (0.89–1.48) | ||||
| Age 46→50 | 0.88 (0.71–1.10) | 0.96 (0.59–1.57) | 0.86 (0.68–1.10) | ||||
| Age 45→50 | 0.96 (0.76–1.23) | 0.91 (0.52–1.62) | 0.98 (0.75–1.28) | ||||
| 50–54 | Age 54→55 | Ref. | <0.001 | Ref. | 0.120 | Ref. | <0.001 |
| Age 53→55 | 0.84 (0.72–0.98) | 0.88 (0.65–1.20) | 0.83 (0.70–0.98) | ||||
| Age 52→55 | 0.80 (0.70–0.91) | 0.83 (0.64–1.09) | 0.79 (0.68–0.92) | ||||
| Age 51→55 | 0.79 (0.68–0.92) | 0.77 (0.56–1.06) | 0.80 (0.67–0.95) | ||||
| Age 50→55 | 0.75 (0.65–0.86) | 0.83 (0.63–1.09) | 0.73 (0.63–0.86) | ||||
| 55–59 | Age 59→60 | Ref. | <0.001 | Ref. | 0.022 | Ref. | <0.001 |
| Age 58→60 | 0.88 (0.76–1.01) | 0.88 (0.66–1.17) | 0.88 (0.75–1.02) | ||||
| Age 57→60 | 0.85 (0.73–0.98) | 0.76 (0.55–1.06) | 0.87 (0.73–1.03) | ||||
| Age 56→60 | 0.78 (0.68–0.90) | 0.79 (0.60–1.06) | 0.78 (0.67–0.91) | ||||
| Age 55→60 | 0.71 (0.60–0.83) | 0.67 (0.48–0.94) | 0.72 (0.60–0.86) | ||||
| 60–64 | Age 64→65 | Ref. | <0.001 | Ref. | 0.001 | Ref. | 0.005 |
| Age 63→65 | 0.85 (0.75–0.97) | 0.86 (0.66–1.12) | 0.85 (0.74–0.99) | ||||
| Age 62→65 | 0.89 (0.79–0.99) | 0.80 (0.64–1.01) | 0.91 (0.80–1.03) | ||||
| Age 61→65 | 0.78 (0.68–0.89) | 0.75 (0.57–0.99) | 0.79 (0.67–0.91) | ||||
| Age 60→65 | 0.82 (0.73–0.91) | 0.68 (0.54–0.86) | 0.86 (0.76–0.97) | ||||
| 65–69 | Age 69→70 | Ref. | 0.039 | Ref. | 0.150 | Ref. | 0.113 |
| Age 68→70 | 0.85 (0.75–0.97) | 0.84 (0.61–1.14) | 1.10 (0.94–1.30) | ||||
| Age 67→70 | 0.89 (0.79–0.99) | 0.78 (0.55–1.12) | 1.00 (0.83–1.20) | ||||
| Age 66→70 | 0.78 (0.68–0.89) | 0.81 (0.60–1.10) | 0.95 (0.80–1.12) | ||||
| Age 65→70 | 0.82 (0.73–0.91) | 0.73 (0.52–1.03) | 0.92 (0.77–1.10) | ||||
| 70–74 | Age 74→75 | Ref. | 0.079 | Ref. | 0.149 | Ref. | 0.234 |
| Age 73→75 | 1.04 (0.90–1.20) | 1.09 (0.75–1.60) | 0.93 (0.75–1.15) | ||||
| Age 72→75 | 0.95 (0.80–1.11) | 1.05 (0.76–1.45) | 0.97 (0.82–1.16) | ||||
| Age 71→75 | 0.92 (0.79–1.06) | 0.87 (0.59–1.26) | 0.85 (0.70–1.03) | ||||
| Age 70→75 | 0.88 (0.75–1.02) | 0.85 (0.62–1.16) | 0.89 (0.76–1.05) | ||||
| ≥75 | Age ≥79→age + 1 d | Ref. | 0.529 | Ref. | 0.437 | Ref. | 0.739 |
| Age 78→80 | 1.10 (0.88–1.38) | 1.38 (0.84–2.25) | 1.04 (0.81–1.34) | ||||
| Age 77→80 | 0.91 (0.71–1.17) | 1.01 (0.57–1.80) | 0.89 (0.67–1.17) | ||||
| Age 76→80 | 0.99 (0.81–1.20) | 1.33 (0.87–2.03) | 0.91 (0.73–1.14) | ||||
| Age 75→80 | 0.96 (0.77–1.18) | 0.65 (0.38–1.14) | 1.03 (0.81–1.29) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, Y.S.; Tran, M.T.X.; Song, H.; Park, B.; Moon, C.M. Association between Age at Helicobacter pylori Eradication and the Risk of Gastric Cancer Stratified by Family History of Gastric Cancer: A Nationwide Population-Based Study. Cancers 2023, 15, 1604. https://doi.org/10.3390/cancers15051604
Jung YS, Tran MTX, Song H, Park B, Moon CM. Association between Age at Helicobacter pylori Eradication and the Risk of Gastric Cancer Stratified by Family History of Gastric Cancer: A Nationwide Population-Based Study. Cancers. 2023; 15(5):1604. https://doi.org/10.3390/cancers15051604
Chicago/Turabian StyleJung, Yoon Suk, Mai Thi Xuan Tran, Huiyeon Song, Boyoung Park, and Chang Mo Moon. 2023. "Association between Age at Helicobacter pylori Eradication and the Risk of Gastric Cancer Stratified by Family History of Gastric Cancer: A Nationwide Population-Based Study" Cancers 15, no. 5: 1604. https://doi.org/10.3390/cancers15051604
APA StyleJung, Y. S., Tran, M. T. X., Song, H., Park, B., & Moon, C. M. (2023). Association between Age at Helicobacter pylori Eradication and the Risk of Gastric Cancer Stratified by Family History of Gastric Cancer: A Nationwide Population-Based Study. Cancers, 15(5), 1604. https://doi.org/10.3390/cancers15051604