
Long-COVID in Patients with Cancer Previously Treated with Early Anti-SARS-CoV-2 Therapies in an Out-of-Hospital Setting: A Single-Center Experience

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
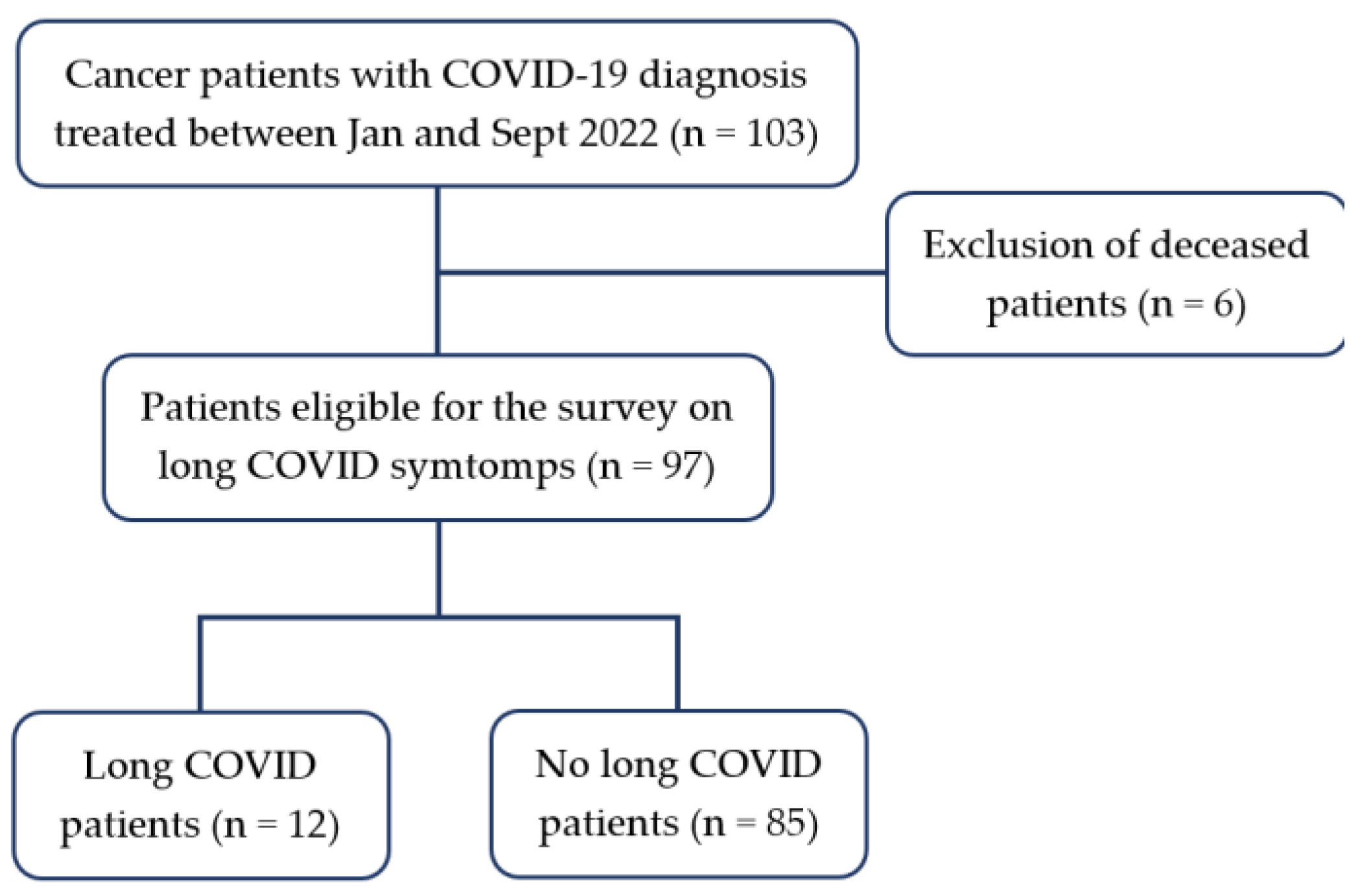
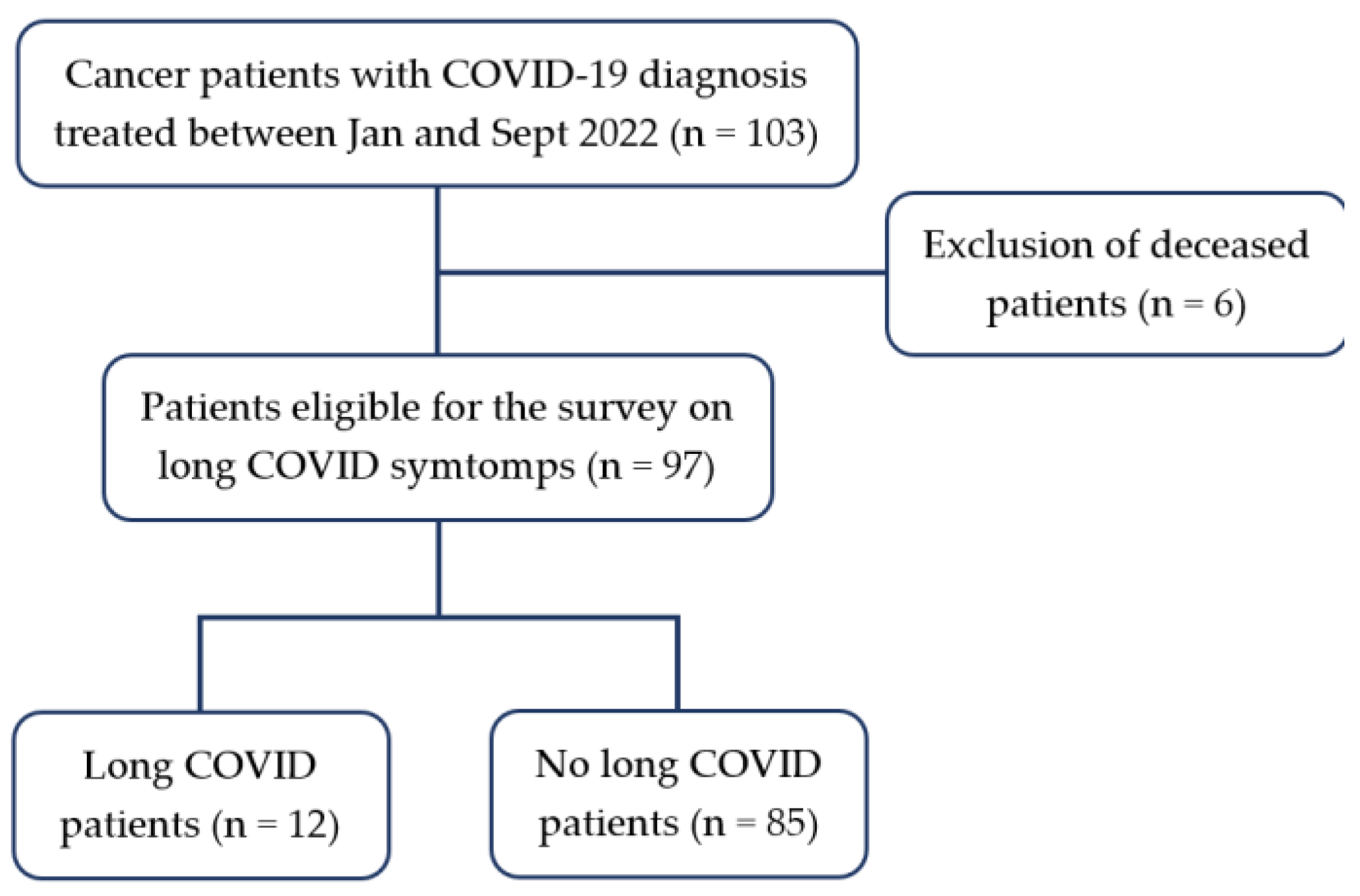
2.1. Participants
2.2. Outcomes
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
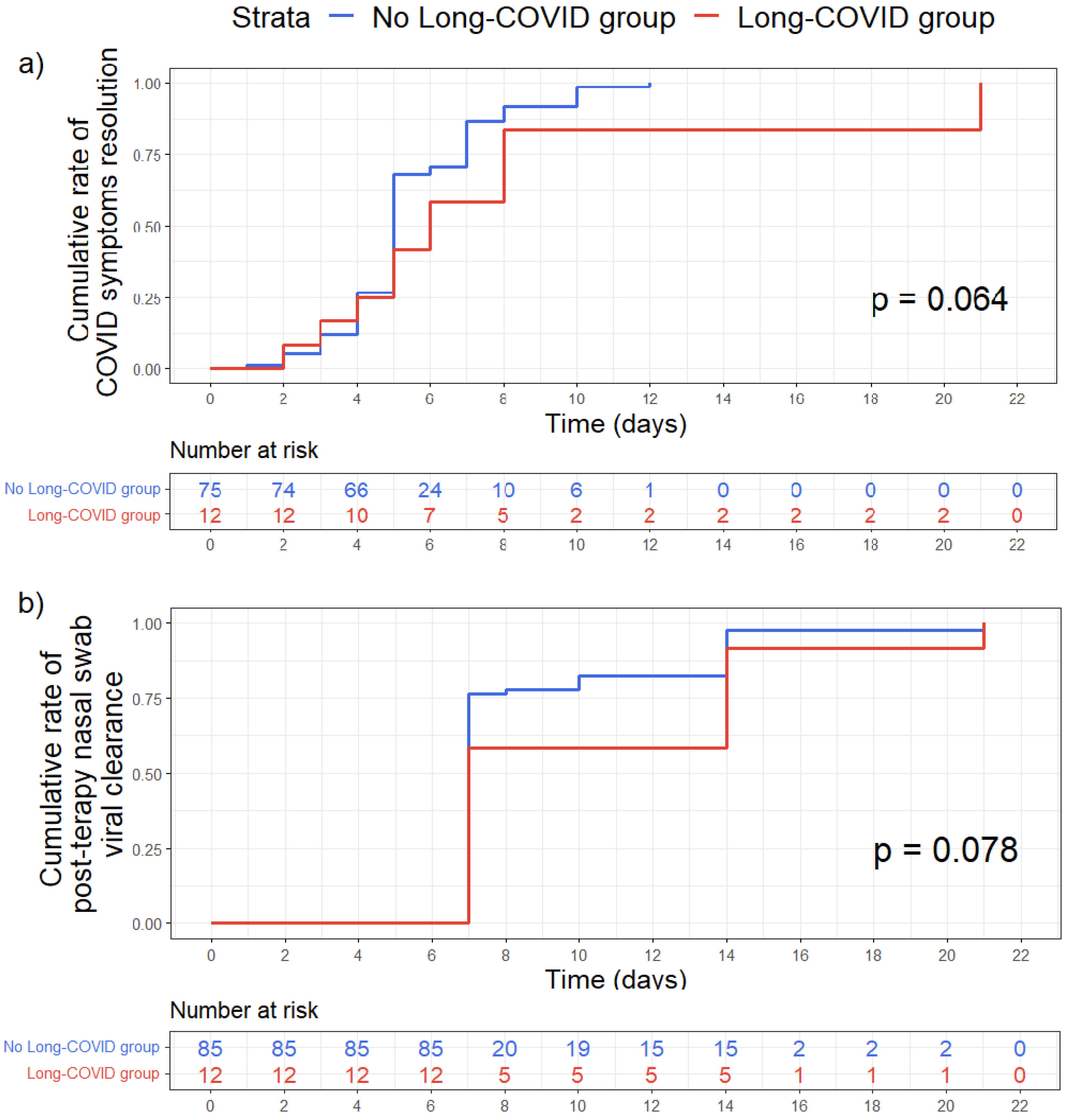
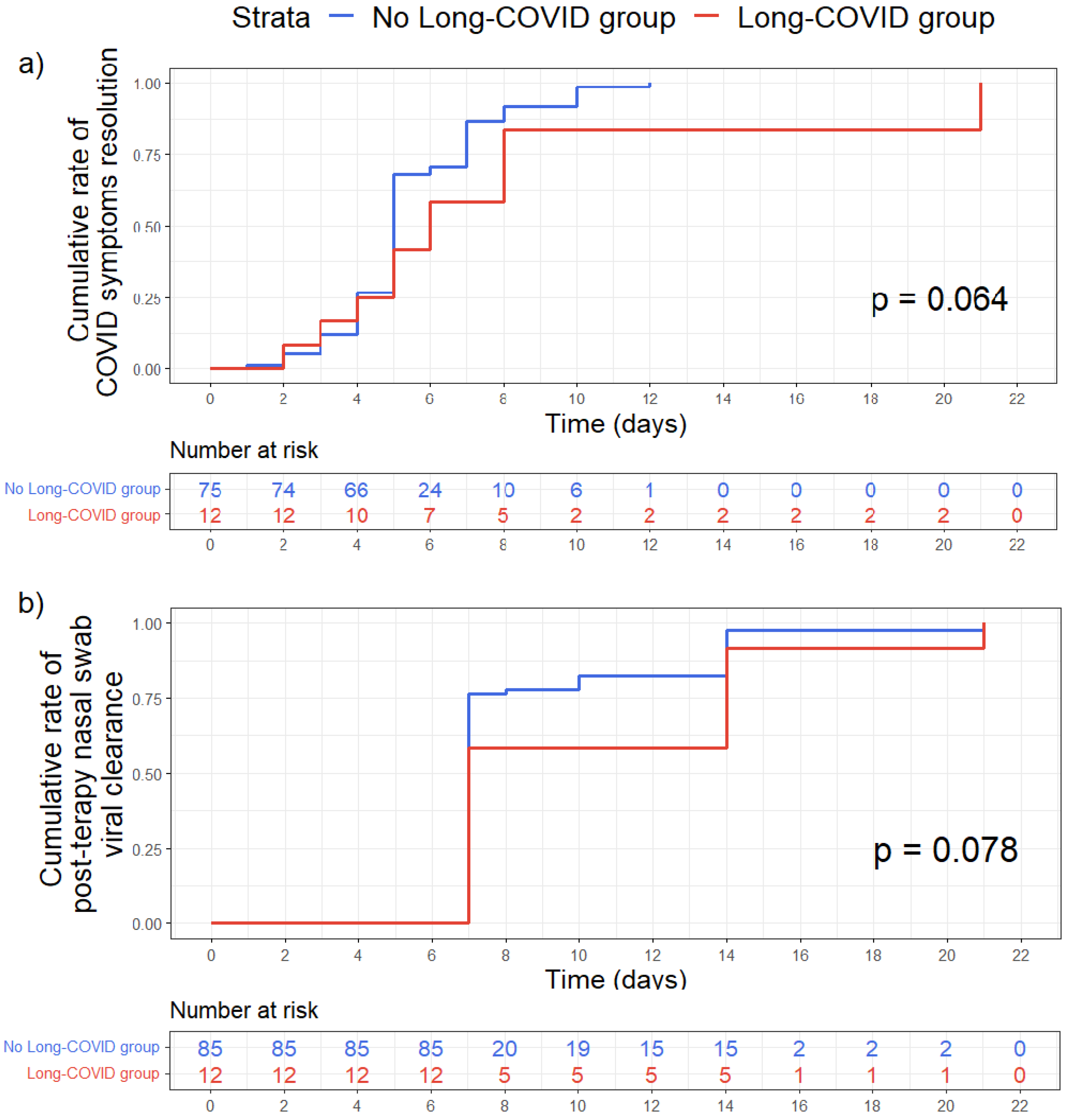
3.2. Statistical Analyses Comparing Long COVID vs. No Long COVID
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Han, H.; He, T.; Labbe, K.E.; Hernandez, A.V.; Chen, H.; Velcheti, V.; Stebbing, J.; Wong, K.K. Clinical Characteristics and Outcomes of COVID-19–Infected Cancer Patients: A Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2021, 113, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Ehmsen, S.; Asmussen, A.; Jeppesen, S.S.; Nilsson, A.C.; Østerlev, S.; Kragh, A.; Frederiksen, H.; Ditzel, H.J. Antibody responses following third mRNA COVID-19 vaccination in patients with cancer and potential timing of a fourth vaccination. Cancer Cell. 2022, 40, 338–339. [Google Scholar] [CrossRef] [PubMed]
- Lasagna, A.; Bergami, F.; Lilleri, D.; Percivalle, E.; Quaccini, M.; Serra, F.; Comolli, G.; Sarasini, A.; Sammartino, J.C.; Ferrari, A.; et al. Six-month humoral and cellular immune response to the third dose of BNT162b2 anti-SARS-CoV-2 vaccine in patients with solid tumors: A longitudinal cohort study with a focus on the variants of concern. ESMO Open 2022, 7, 100574. [Google Scholar] [CrossRef] [PubMed]
- Gopinath, S.; Ishak, A.; Dhawan, N.; Poudel, S.; Shrestha, P.S.; Singh, P.; Xie, E.; Tahir, P.; Marzaban, S.; Michel, J.; et al. Characteristics of COVID-19 breakthrough infections among vaccinated individuals and associated risk factors: A systematic review. Trop. Med. Infect. Dis. 2022, 7, 81. [Google Scholar] [CrossRef] [PubMed]
- AIFA: Registri Farmaci Sottoposti a Monitoraggio. Available online: https://www.aifa.gov.it/web/guest/emergenza-covid-19 (accessed on 15 January 2023).
- Lasagna, A.; Cassaniti, I.; Lilleri, D.; Quaccini, M.; Ferrari, A.; Sacchi, P.; Bruno, R.; Baldanti, F.; Pedrazzoli, P. Effectiveness of the available early therapies in reducing severe COVID-19 in non-hospitalized patients with solid tumors on active treatment. Front. Med. 2022, 9, 1036473. [Google Scholar] [CrossRef]
- World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus; WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 18 December 2022).
- Brightling, C.E.; Evans, R.A. Long COVID: Which symptoms can be attributed to SARS-CoV-2 infection? Lancet 2022, 400, 411–413. [Google Scholar] [CrossRef]
- Chasco, E.E.; Dukes, K.; Jones, D.; Comellas, A.P.; Hoffman, R.M.; Garg, A. Brain Fog and Fatigue following COVID-19 Infection: An Exploratory Study of Patient Experiences of Long COVID. Int. J. Environ. Res. Public Health 2022, 19, 15499. [Google Scholar] [CrossRef]
- Taquet, M.; Dercon, Q.; Luciano, S.; Geddes, J.R.; Husain, M.; Harrison, P.J. Incidence, Co-Occurrence, and Evolution of Long-COVID Features: A 6-Month Retrospective Cohort Study of 273,618 Survivors of COVID-19. PLoS Med. 2021, 18, e1003773. [Google Scholar] [CrossRef]
- Cortellini, A.; Salazar, R.; Gennari, A.; Aguilar-Company, J.; Bower, M.; Bertuzzi, A.; Brunet, J.; Lambertini, M.; Maluquer, C.; Pedrazzoli, P.; et al. Persistence of long-term COVID-19 sequelae in patients with cancer: An analysis from the OnCovid registry. Eur. J. Cancer 2022, 170, 10–16. [Google Scholar] [CrossRef]
- Monroy-Iglesias, M.J.; Tremble, K.; Russell, B.; Moss, C.; Dolly, S.; Sita-Lumsden, A.; Cortellini, A.; Pinato, D.J.; Rigg, A.; Karagiannis, S.N.; et al. Long-term effects of COVID-19 on cancer patients: The experience from Guy’s Cancer Centre. Future Oncol. 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Rapti, V.; Tsaganos, T.; Vathiotis, I.A.; Syrigos, N.K.; Li, P.; Poulakou, G. New Insights into SARS-CoV-2 and Cancer Cross-Talk: Does a Novel Oncogenesis Driver Emerge? Vaccines 2022, 10, 1607. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, M.A.F.; Neves, P.; Lima, S.S.; Lopes, J.D.C.; Torres, M.; Vallinoto, I.; Bichara, C.D.A.; Dos Santos, E.F.; de Brito, M.T.F.M.; da Silva, A.L.S.; et al. Cytokine Profiles Associated With Acute COVID-19 and Long COVID-19 Syndrome. Front. Cell Infect. Microbiol. 2022, 12, 922422. [Google Scholar] [CrossRef] [PubMed]
- Pusztai, L.; Mendoza, T.R.; Reuben, J.M.; Martinez, M.M.; Willey, J.S.; Lara, J.; Syed, A.; Fritsche, H.A.; Bruera, E.; Booser, D.; et al. Changes in plasma levels of inflammatory cytokines in response to paclitaxel chemotherapy. Cytokine 2004, 25, 94–102. [Google Scholar] [CrossRef]
- Piotrowski, I.; Kulcenty, K.; Suchorska, W. Interplay between inflammation and cancer. Rep. Pract. Oncol. Radiother. 2020, 25, 422–427. [Google Scholar] [CrossRef]
- Rusin, A.; Seymour, C.; Cocchetto, A.; Mothersill, C. Commonalities in the Features of Cancer and Chronic Fatigue Syndrome (CFS): Evidence for Stress-Induced Phenotype Instability? Int. J. Mol. Sci. 2022, 23, 691. [Google Scholar] [CrossRef]
- Boglione, L.; Meli, G.; Poletti, F.; Rostagno, R.; Moglia, R.; Cantone, M.; Esposito, M.; Scianguetta, C.; Domenicale, B.; Di Pasquale, F.; et al. Risk factors and incidence of long-COVID syndrome in hospitalized patients: Does remdesivir have a protective effect? QJM 2022, 114, 865–871. [Google Scholar] [CrossRef]
- Zhong, W.; Jiang, X.; Yang, X.; Feng, T.; Duan, Z.; Wang, W.; Sun, Z.; Chen, L.; Nie, X.; Zhu, C.; et al. The efficacy of paxlovid in elderly patients infected with SARS-CoV-2 omicron variants: Results of a non-randomized clinical trial. Front. Med. 2022, 9, 980002. [Google Scholar] [CrossRef]
- Ayoubkhani, D.; Bosworth, M.L.; King, S.; Pouwels, K.B.; Glickman, M.; Nafilyan, V.; Zaccardi, F.; Khunti, K.; Alwan, N.A.; Walker, A.S. Risk of Long COVID in People Infected with Severe Acute Respiratory Syndrome Coronavirus 2 After 2 Doses of a Coronavirus Disease 2019 Vaccine: Community-Based, Matched Cohort Study. Open Forum Infect. Dis. 2022, 9, ofac464. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Ortega-Santiago, R.; Fuensalida-Novo, S.; Martín-Guerrero, J.D.; Pellicer-Valero, O.J.; Torres-Macho, J. Differences in Long-COVID Symptoms between Vaccinated and Non-Vaccinated (BNT162b2 Vaccine) Hospitalized COVID-19 Survivors Infected with the Delta Variant. Vaccines 2022, 10, 1481. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Martín-Guerrero, J.D.; Pellicer-Valero, Ó.J.; Navarro-Pardo, E.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalón, J.A.; Cigarán-Méndez, M.; Hernández-Barrera, V.; Arendt-Nielsen, L. Female Sex Is a Risk Factor Associated with Long-Term Post-COVID Related-Symptoms but Not with COVID-19 Symptoms: The LONG-COVID-EXP-CM Multicenter Study. J. Clin. Med. 2022, 11, 413. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef] [PubMed]
- Scully, E.P.; Schumock, G.; Fu, M.; Massaccesi, G.; Muschelli, J.; Betz, J.; Klein, E.Y.; West, N.E.; Robinson, M.; Garibaldi, B.T.; et al. Sex and Gender Differences in Testing, Hospital Admission, Clinical Presentation, and Drivers of Severe Outcomes From COVID-19. Open Forum Infect Dis. 2021, 8, ofab448. [Google Scholar] [CrossRef]
- Fortunato, F.; Martinelli, D.; Lo Caputo, S.; Santantonio, T.; Dattoli, V.; Lopalco, P.L.; Prato, R. Sex and gender differences in COVID-19: An Italian local register-based study. BMJ Open 2021, 11, e051506. [Google Scholar] [CrossRef] [PubMed]
- Kloc, M.; Ghobrial, R.M.; Kubiak, J.Z. The Role of Genetic Sex and Mitochondria in Response to COVID-19 Infection. Int. Arch. Allergy Immunol. 2020, 181, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, D.; Nair, S.S.; Hammouda, N.; Ratnani, P.; Gharib, Y.; Wagaskar, V.; Mohamed, N.; Lundon, D.; Dovey, Z.; Kyprianou, N.; et al. Sex differences in SARS-CoV-2 infection rates and the potential link to prostate cancer. Commun. Biol. 2020, 3, 374. [Google Scholar] [CrossRef]
- Lasagna, A.; Zuccaro, V.; Ferraris, E.; Corbella, M.; Bruno, R.; Pedrazzoli, P. COVID-19 and breast cancer: May the microbiome be the issue? Future Oncol. 2021, 17, 123–126. [Google Scholar] [CrossRef]
- Liu, Q.; Mak, J.W.Y.; Su, Q.; Yeoh, Y.K.; Lui, G.C.; Ng, S.S.S.; Zhang, F.; Li, A.Y.L.; Lu, W.; Hui, D.S.; et al. Gut microbiota dynamics in a prospective cohort of patients with post-acute COVID-19 syndrome. Gut 2022, 71, 544–552. [Google Scholar] [CrossRef]
- Raveendran, A.V.; Misra, A. Post COVID-19 syndrome (“Long COVID”) and diabetes: Challenges in diagnosis and management. Diabetes Metab. Syndr. 2021, 15, 102235. [Google Scholar] [CrossRef]
- Heubner, L.; Petrick, P.L.; Güldner, A.; Bartels, L.; Ragaller, M.; Mirus, M.; Rand, A.; Tiebel, O.; Beyer-Westendorf, J.; Rößler, M.; et al. Extreme obesity is a strong predictor for in-hospital mortality and the prevalence of long-COVID in severe COVID-19 patients with acute respiratory distress syndrome. Sci. Rep. 2022, 12, 18418. [Google Scholar] [CrossRef]
- Notarte, K.I.; de Oliveira, M.H.S.; Peligro, P.J.; Velasco, J.V.; Macaranas, I.; Ver, A.T.; Pangilinan, F.C.; Pastrana, A.; Goldrich, N.; Kavteladze, D.; et al. Age, Sex and Previous Comorbidities as Risk Factors Not Associated with SARS-CoV-2 Infection for Long COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 7314. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Swank, Z.; Senussi, Y.; Manickas-Hill, Z.; Yu, X.G.; Li, J.Z.; Alter, G.; Walt, D.R. Persistent circulating SARS-CoV-2 spike is associated with post-acute COVID-19 sequelae. Clin. Infect. Dis. 2022, 2022, ciac722. [Google Scholar]

{kind=link}
{kind=link}
| Symptoms | Yes | No |
|---|---|---|
| Respiratory symptoms (breathlessness/cough) | ||
| Myalgia | ||
| Palpitations | ||
| Chest pain | ||
| Fatigue | ||
| Brain fog | ||
| Headache | ||
| Gastrointestinal symptoms (diarrhea/anorexia) | ||
| Skin rashes | ||
| Anosmia | ||
| Ageusia | ||
| Hair loss |
| Variable | Whole Sample (n = 97) | Long COVID Group (n = 12, 12.4%) | No Long COVID Group (n = 85, 87.6%) | p Value |
|---|---|---|---|---|
| Age [years], median (IQR) | 63 (16) | 58 (16) | 63 (16) | 0.290 |
| Sex, n (%) | 0.024 | |||
| Females | 58 (60%) | 11 (91.7%) | 47 (55.3%) | |
| Males | 39 (40%) | 1 (8.3%) | 38 (44.7%) | |
| Type of tumor, n (%) | 0.076 | |||
| Lung | 25 (25.8%) | 2 (16.7%) | 23 (27.1%) | |
| Melanoma | 8 (8.2%) | 1 (8.3%) | 7 (8.2%) | |
| Breast | 29 (29.9%) | 8 (66.7%) | 21 (24.7%) | |
| Kidney | 4 (4.2%) | 0 | 4 (4.7%) | |
| Gastrointestinal | 23 (23.7%) | 0 | 23 (27.1%) | |
| Other | 8 (8.2%) | 1 (8.3%) | 7 (8.2%) | |
| Stage of tumor, n (%) | 0.274 | |||
| II/III | 24 (24.8%) | 5 (41.7%) | 19 (22.3%) | |
| IV | 73 (75.2%) | 7 (58.3%) | 66 (77.7%) | |
| Type of oncological treatment, n (%) | 0.475 | |||
| ICIs | 27 (27.8%) | 2 (16.7%) | 25 (29.4%) | |
| Chemotherapy ** | 49 (50.5%) | 6 (50%) | 43 (50.6%) | |
| Target therapy/ormonotherapy | 21 (21.7%) | 4 (33.3%) | 17 (20%) | |
| CKD, n (%) | 1 (1%) | 0 | 1 (1.2%) | 1 |
| COPD, n (%) | 17 (17.5%) | 1 (8.3%) | 16 (18.8%) | 0.686 |
| Diabetes mellitus type 2, n (%) | 19 (19.6%) | 6 (50%) | 13 (15.3%) | 0.014 |
| Hypertension, n (%) | 22 (22.7%) | 3 (35%) | 19 (22.4%) | 1 |
| Ischemic heart disease, n (%) | 2 (2.1%) | 0 | 2 (2.4%) | 1 |
| Obesity, n (%) | 7 (7.2%) | 3 (25%) | 4 (4.7%) | 0.039 |
| Vaccination doses, n (%) | 0.847 | |||
| 0 | 3 (3.1%) | 0 | 3 (3.5%) | |
| 1 | 1 (1%) | 0 | 1 (1.2%) | |
| 2 | 3 (3.1%) | 0 | 3 (3.5%) | |
| 3 | 81 (83.5%) | 12 (100%) | 69 (81.2%) | |
| 4 | 9 (9.3%) | 0 | 9 (10.6%) | |
| Time between vaccination dose and positivity [months], median (IQR) | 7 (4) | 7 (3) | 7 (4) | 0.991 |
| Type of early therapies, n (%) | 0.443 | |||
| No treatment | 25 (25.8%) | 4 (33.3%) | 21 (24.7%) | |
| Sotrovimab | 2 (2%) | 0 | 2 (2.3%) | |
| Molnupinavir | 15 (15.5%) | 0 | 15 (17.7%) | |
| Remdesivir | 6 (6.2%) | 1 (8.3%) | 5 (5.9%) | |
| Nirmatrelvir/ritonavir | 49 (50.5%) | 7 (58.4%) | 42 (49.4%) | |
| Symptoms’ duration [days], median (IQR) | 5 (3) | 6 (3) | 5 (3) | 0.212 |
| First negative post-therapy swab [days], median (IQR) | 7 (1) | 7 (7) | 7 (0) | 0.124 |
| Outcome: Long COVID | |||
|---|---|---|---|
| Adjusted OR | 95% CI | p Value | |
| Diabetes Mellitus | 10.03 | 2.24–55.32 | 0.004 |
| Sex = Female | 6.27 | 0.74–137.5 | 0.132 |
| Breast cancer | 4.43 | 0.98–26.76 | 0.069 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lasagna, A.; Albi, G.; Figini, S.; Basile, S.; Sacchi, P.; Bruno, R.; Pedrazzoli, P. Long-COVID in Patients with Cancer Previously Treated with Early Anti-SARS-CoV-2 Therapies in an Out-of-Hospital Setting: A Single-Center Experience. Cancers 2023, 15, 1269. https://doi.org/10.3390/cancers15041269
Lasagna A, Albi G, Figini S, Basile S, Sacchi P, Bruno R, Pedrazzoli P. Long-COVID in Patients with Cancer Previously Treated with Early Anti-SARS-CoV-2 Therapies in an Out-of-Hospital Setting: A Single-Center Experience. Cancers. 2023; 15(4):1269. https://doi.org/10.3390/cancers15041269
Chicago/Turabian StyleLasagna, Angioletta, Giuseppe Albi, Simone Figini, Sara Basile, Paolo Sacchi, Raffaele Bruno, and Paolo Pedrazzoli. 2023. "Long-COVID in Patients with Cancer Previously Treated with Early Anti-SARS-CoV-2 Therapies in an Out-of-Hospital Setting: A Single-Center Experience" Cancers 15, no. 4: 1269. https://doi.org/10.3390/cancers15041269
APA StyleLasagna, A., Albi, G., Figini, S., Basile, S., Sacchi, P., Bruno, R., & Pedrazzoli, P. (2023). Long-COVID in Patients with Cancer Previously Treated with Early Anti-SARS-CoV-2 Therapies in an Out-of-Hospital Setting: A Single-Center Experience. Cancers, 15(4), 1269. https://doi.org/10.3390/cancers15041269