
Extradural Primary Malignant Spinal Tumors in a Population Younger than 25 Years: An Ambispective International Multicenter Study on Onco-Surgical Outcomes



 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
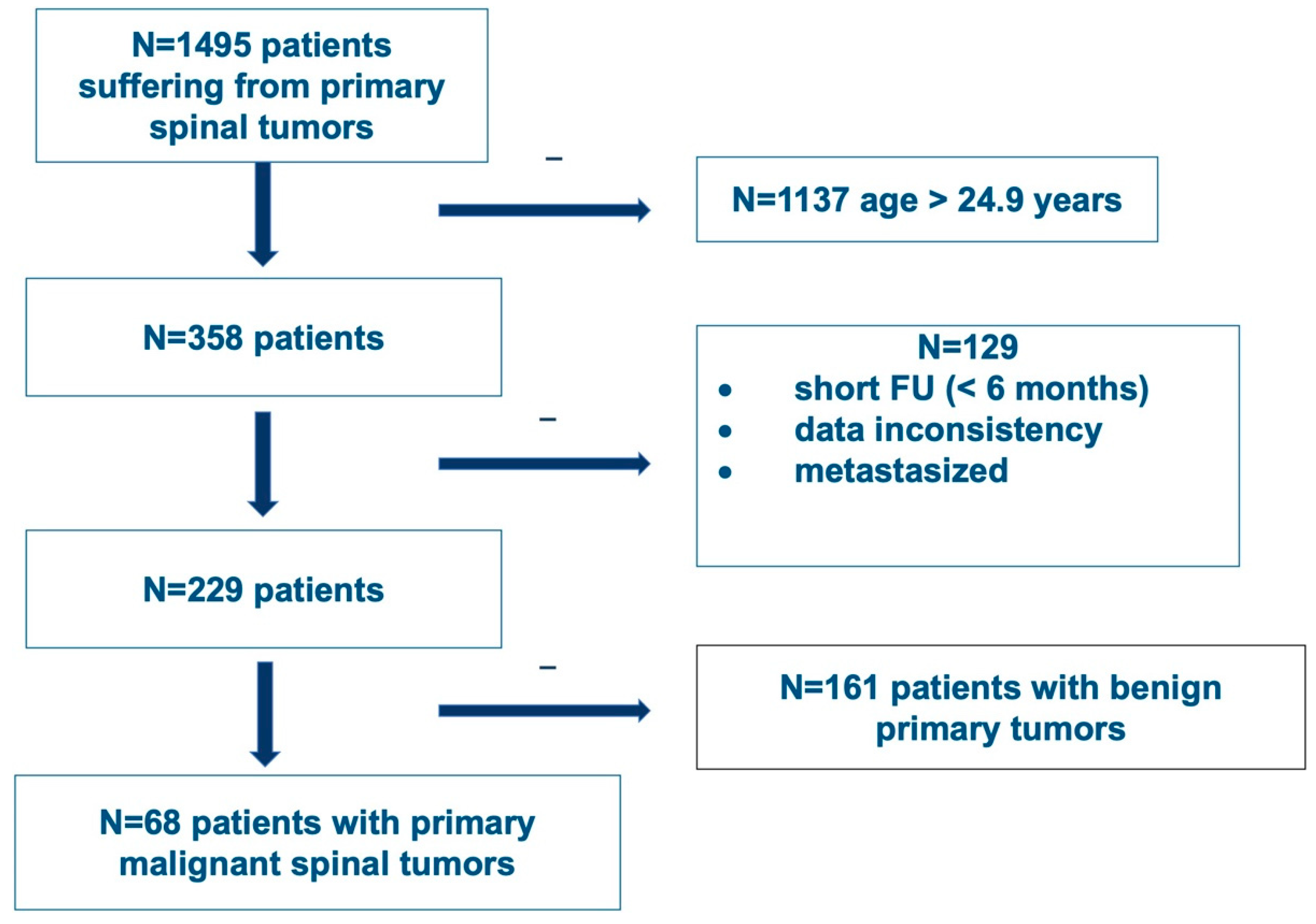
2.1. Design and Patients
2.2. Neurological Status
2.3. Treatment
2.4. Statistics
3. Results
3.1. Patients
3.2. Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arora, R.S.; Alston, R.D.; Eden, T.O.; Geraci, M.; Birch, J.M. The contrasting age-incidence patterns of bone tumours in teenagers and young adults: Implications for aetiology. Int. J. Cancer 2012, 131, 1678–1685. [Google Scholar] [CrossRef] [PubMed]
- Whelan, J.; McTiernan, A.; Cooper, N.; Wong, Y.K.; Francis, M.; Vernon, S.; Strauss, S.J. Incidence and survival of malignant bone sarcomas in England 1979–2007. Int. J. Cancer 2012, 131, E508–E517. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Ro, J.Y. The 2020 WHO Classification of Tumors of Bone: An Updated Review. Adv. Anat. Pathol. 2021, 28, 119–138. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.D.M. The evolving classification of soft tissue tumours—An update based on the new 2013 WHO classification. Histopathology 2014, 64, 2–11. [Google Scholar] [CrossRef]
- van den Berg, H.; Kroon, H.M.; Slaar, A.; Hogendoorn, P. Incidence of biopsy-proven bone tumors in children: A report based on the Dutch pathology registration “PALGA”. J. Pediatr. Orthop. 2008, 28, 29–35. [Google Scholar] [CrossRef]
- Boriani, S.; Weinstein, J.N.; Biagini, R. Primary bone tumors of the spine. Terminology and surgical staging. Spine 1997, 22, 1036–1044. [Google Scholar] [CrossRef]
- Enneking, W.F.; Spanier, S.S.; Goodman, M.A. A system for the surgical staging of musculoskeletal sarcoma. Clin. Orthop. Relat. Res. 1980, 153, 106–120. [Google Scholar] [CrossRef]
- Dea, N.; Gokaslan, Z.; Choi, D.; Fisher, C. Spine Oncology—Primary Spine Tumors. Neurosurgery 2017, 80, S124–S130. [Google Scholar] [CrossRef]
- Chan, P.; Boriani, S.; Fourney, D.R.; Biagini, R.; Dekutoski, M.B.; Fehlings, M.G.; Ryken, T.C.; Gokaslan, Z.L.; Vrionis, F.D.; Harrop, J.S.; et al. An Assessment of the Reliability of the Enneking and Weinstein-Boriani-Biagini Classifications for Staging of Primary Spinal Tumors by the Spine Oncology Study Group. Spine 2009, 34, 384–391. [Google Scholar] [CrossRef]
- Fisher, C.G.; Goldschlager, T.; Boriani, S.; Varga, P.P.; Rhines, L.D.; Fehlings, M.G.; Luzzati, A.; Dekutoski, M.B.; Reynolds, J.J.; Chou, D.; et al. An evidence-based medicine model for rare and often neglected neoplastic conditions. J. Neurosurg. Spine 2014, 21, 704–710. [Google Scholar] [CrossRef]
- Charest-Morin, R.; Dirks, M.S.; Patel, S.; Boriani, S.; Luzzati, A.; Fehlings, M.G.; Fisher, C.G.; Dekutoski, M.B.; Williams, R.; Quraishi, N.A.; et al. Ewing Sarcoma of the Spine: Prognostic Variables for Survival and Local Control in Surgically Treated Patients. Spine 2018, 43, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Dea, N.; Charest-Morin, R.; Sciubba, D.M.; Bird, J.E.; Disch, A.C.; Mesfin, A.; Lazáry, Á.; Fisher, C.G.; Ames, C. Optimizing the Adverse Event and HRQOL Profiles in the Management of Primary Spine Tumors. Spine 2016, 41 (Suppl. S20), S212–S217. [Google Scholar] [CrossRef] [PubMed]
- Dekutoski, M.B.; Clarke, M.J.; Rose, P.; Luzzati, A.; Rhines, L.D.; Varga, P.P.; Fisher, C.G.; Chou, D.; Fehlings, M.G.; Reynolds, J.J.; et al. Osteosarcoma of the spine: Prognostic variables for local recurrence and overall survival, a multicenter ambispective study. J. Neurosurg. Spine 2016, 25, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C.G.; Versteeg, A.L.; Dea, N.; Boriani, S.; Varga, P.P.; Dekutoski, M.B.; Luzzati, A.; Gokaslan, Z.L.; Williams, R.P.; Reynolds, J.J.; et al. Surgical Management of Spinal Chondrosarcomas. Spine 2016, 41, 678–685. [Google Scholar] [CrossRef]
- Charest-Morin, R.; Dea, N.; Fisher, C.G. Health-Related Quality of Life After Spine Surgery for Primary Bone Tumour. Curr. Treat. Options Oncol. 2016, 17, 9. [Google Scholar] [CrossRef]
- Gokaslan, Z.L.; Zadnik, P.L.; Sciubba, D.M.; Germscheid, N.; Goodwin, C.R.; Wolinsky, J.-P.; Bettegowda, C.; Groves, M.L.; Luzzati, A.; Rhines, L.D.; et al. Mobile spine chordoma: Results of 166 patients from the AOSpine Knowledge Forum Tumor database. J. Neurosurg. Spine 2016, 24, 644–651. [Google Scholar] [CrossRef]
- Casali, P.G.; Bielack, S.; Abecassis, N.; Aro, H.T.; Bauer, S.; Biagini, R.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brennan, B.; et al. Bone sarcomas: ESMO-PaedCan-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. S4), iv79–iv95. [Google Scholar] [CrossRef]
- Sciubba, D.M.; Hsieh, P.; McLoughlin, G.S.; Jallo, G.I. Pediatric Tumors Involving the Spinal Column. Neurosurg. Clin. N. Am. 2008, 19, 81–92. [Google Scholar] [CrossRef]
- Ravindra, V.M.; Eli, I.M.; Schmidt, M.H.; Brockmeyer, D.L. Primary osseous tumors of the pediatric spinal column: Review of pathology and surgical decision making. Neurosurg. Focus 2016, 41, E3. [Google Scholar] [CrossRef]
- Charest-Morin, R.; Flexman, A.M.; Srinivas, S.; Fisher, C.G.; Street, J.T.; Boyd, M.C.; Ailon, T.; Dvorak, M.F.; Kwon, B.K.; Paquette, S.J.; et al. Perioperative adverse events following surgery for primary bone tumors of the spine and en bloc resection for metastases. J. Neurosurg. Spine 2019, 32, 98–105. [Google Scholar] [CrossRef]
- Bosma, S.E.; van der Heijden, L.; Sierrasesúmaga, L.; Merks, H.J.H.M.; Haveman, L.M.; van de Sande, M.A.J.; San-Julián, M. What Do We Know about Survival in Skeletally Premature Children Aged 0 to 10 Years with Ewing Sarcoma? A Multicenter 10-Year Follow-Up Study in 60 Patients. Cancers 2022, 14, 1456. [Google Scholar] [CrossRef] [PubMed]
- Helenius, I.J.; Krieg, A.H. Primary malignant bone tumours of spine and pelvis in children. J. Child. Orthop. 2021, 15, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Sciubba, D.M.; Ramos, R.D.L.G.; Goodwin, C.R.; Abu-Bonsrah, N.; Bydon, A.; Witham, T.F.; Bettegowda, C.; Gokaslan, Z.L.; Wolinsky, J.-P. Clinical, surgical, and molecular prognostic factors for survival after spinal sarcoma resection. Neurosurg. Focus 2016, 41, E9. [Google Scholar] [CrossRef] [PubMed]
- Worch, J.; Ranft, A.; Dubois, S.G.; Paulussen, M.; Juergens, H.; Dirksen, U. Age dependency of primary tumor sites and metastases in patients with Ewing sarcoma. Pediatr. Blood Cancer 2018, 65, e27251. [Google Scholar] [CrossRef] [PubMed]
- Luzzati, A.; Scotto, G.; Cannavò, L.; di Uccio, A.S.; Orlando, G.; Petriello, L.; Zoccali, C. En bloc resection in patients younger than 16 years affected by primary spine tumors: Indications, results and complications in a series of 22 patients. Eur. Spine J. 2020, 29, 3135–3147. [Google Scholar] [CrossRef] [PubMed]
- Schaser, K.-D.; Melcher, I.; Luzzati, A.; Disch, A.C. Bone sarcoma of the spine. Recent Results Cancer Res. 2009, 179, 141–167. [Google Scholar]
- Garg, S.; Mehta, S.; Dormans, J.P. Modern surgical treatment of primary aneurysmal bone cyst of the spine in children and adolescents. J. Pediatr. Orthop. 2005, 25, 387–392. [Google Scholar] [CrossRef]
- Gupta, A.A.; Pappo, A.; Saunders, N.; Hopyan, S.; Ferguson, P.; Wunder, J.; O’Sullivan, B.; Catton, C.; Greenberg, M.; Blackstein, M. Clinical outcome of children and adults with localized Ewing sarcoma: Impact of chemotherapy dose and timing of local therapy. Cancer 2010, 116, 3189–3194. [Google Scholar] [CrossRef]
- Seto, T.; Merchant, M.; Morse, L.J.; Fang, A.; Song, M.-N.; Russell, E.A.; Pan, M. Pain as Initial Presenting Symptom Is Associated with Delay to Seeking Medical Attention, Higher Risk of Relapse, and Shorter Survival in Patients with Early-Stage Extremity or Trunk Synovial Sarcoma. Perm. J. 2022, 26, 94–102. [Google Scholar] [CrossRef]
- Wurtz, L.D.; Peabody, T.D.; Simon, M.A. Delay in the Diagnosis and Treatment of Primary Bone Sarcoma of the Pelvis. J. Bone Jt. Surg. 1999, 81, 317–325. [Google Scholar] [CrossRef]
- Datzmann, T.; Kisel, W.; Kramer, J.; Dreimann, M.; Müller-Broich, J.D.; Netzer, C.; Schaser, K.D.; Schmitt, J.; Disch, A.C.; Sauer, D.; et al. eCross-cultural adaptation of the spine oncology-specific SOSGOQ2.0 questionnaire to German language and the assessment of its validity and reliability in the clinical setting. BMC Cancer 2021, 21, 1044. [Google Scholar] [CrossRef] [PubMed]
- Barrientos-Ruiz, I.; Ortiz-Cruz, E.J.; Serrano-Montilla, J.; Bernabeu-Taboada, D.; Pozo-Kreilinger, J.J. Are Biopsy Tracts a Concern for Seeding and Local Recurrence in Sarcomas? Clin. Orthop. Relat. Res. 2017, 475, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Berger-Richardson, D.; Swallow, C.J. Needle tract seeding after percutaneous biopsy of sarcoma: Risk/benefit considerations. Cancer 2017, 123, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.Y.; Oh, E.; Kwon, J.W.; Kim, H.S. Percutaneous Image-Guided Spinal Lesion Biopsies: Factors Affecting Higher Diagnostic Yield. Am. J. Roentgenol. 2018, 211, 1068–1074. [Google Scholar] [CrossRef] [PubMed]
- Dandurand, C.; Fisher, C.G.; Rhines, L.D.; Boriani, S.; Charest-Morin, R.; Gasbarrini, A.; Luzzati, A.; Reynolds, J.J.; Wei, F.; Gokaslan, Z.L.; et al. Feasibility of achieving planned surgical margins in primary spine tumor: A PTRON study. Neurosurg. Focus 2021, 50, E16. [Google Scholar] [CrossRef]
- Harris, C.J.; Helenowski, I.; Murphy, A.J.; Mansfield, S.A.; LaQuaglia, M.P.; Heaton, T.E.; Cavalli, M.; Murphy, J.T.; Newman, E.; Overmen, R.E.; et al. Implications of Tumor Characteristics and Treatment Modality on Local Recurrence and Functional Outcomes in Children with Chest Wall Sarcoma: A Pediatric Surgical Oncology Research Collaborative Study. Ann. Surg. 2020, 276, e969–e975. [Google Scholar] [CrossRef]
- Shankar, G.M.; Clarke, M.J.; Ailon, T.; Rhines, L.D.; Patel, S.R.; Sahgal, A.; Laufer, I.; Chou, D.; Bilsky, M.H.; Sciubba, D.M.; et al. The role of revision surgery and adjuvant therapy following subtotal resection of osteosarcoma of the spine: A systematic review with meta-analysis. J. Neurosurg. Spine 2017, 27, 97–104. [Google Scholar] [CrossRef]
- Ailon, T.; Torabi, R.; Fisher, C.G.; Rhines, L.D.; Clarke, M.J.; Bettegowda, C.; Boriani, S.; Yamada, Y.J.; Kawahara, N.; Varga, P.P.; et al. Management of Locally Recurrent Chordoma of the Mobile Spine and Sacrum: A Systematic Review. Spine 2016, 41 (Suppl. S20), S193–S198. [Google Scholar] [CrossRef]
- Charest-Morin, R.; Fisher, C.G.; Sahgal, A.; Boriani, S.; Gokaslan, Z.L.; Lazary, A.; Reynolds, J.; Bettegowda, C.; Rhines, L.D.; Dea, N. Primary Bone Tumor of the Spine—An Evolving Field: What a General Spine Surgeon Should Know. Glob. Spine J. 2019, 9 (Suppl. S1), 108S–116S. [Google Scholar] [CrossRef]
- Mirzaei, L.; Kaal, S.E.; Schreuder, H.W.; Bartels, R.H. The Neurological Compromised Spine Due to Ewing Sarcoma. What First: Surgery or Chemotherapy? Therapy, Survival, and Neurological Outcome of 15 Cases with Primary Ewing Sarcoma of the Vertebral Column. Neurosurgery 2015, 77, 718–724. [Google Scholar] [CrossRef]
- Disch, A.; Kleber, C.; Redemann, D.; Druschel, C.; Liljenqvist, U.; Schaser, K. Current surgical strategies for treating spinal tumors: Results of a questionnaire survey among members of the German Spine Society (DWG). Eur. J. Surg. Oncol. 2020, 46, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Colman, M.W.; Karim, S.M.; Lozano-Calderon, S.A.; Pedlow, F.X.; Raskin, K.A.; Hornicek, F.J.; Schwab, J.H. Quality of life after en bloc resection of tumors in the mobile spine. Spine J. 2015, 15, 1728–1737. [Google Scholar] [CrossRef] [PubMed]
- Boriani, S.; Amendola, L.; Bandiera, S.; Simoes, C.E.; Alberghini, M.; Di Fiore, M.; Gasbarrini, A. Staging and treatment of osteoblastoma in the mobile spine: A review of 51 cases. Eur. Spine J. 2012, 21, 2003–2010. [Google Scholar] [CrossRef] [PubMed]
- Boriani, S.; Bandiera, S.; Casadei, R.; Boriani, L.; Donthineni, R.; Gasbarrini, A.; Pignotti, E.; Biagini, R.; Schwab, J.H. Giant cell tumor of the mobile spine: A review of 49 cases. Spine 2012, 37, E37–E45. [Google Scholar] [CrossRef] [PubMed]
- Engel, H.; Herget, G.W.; Füllgraf, H.; Sutter, R.; Benndorf, M.; Bamberg, F.; Jungmann, P.M. Chondrogenic Bone Tumors: The Importance of Imaging Characteristics. Rofo 2021, 193, 262–275. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N (%) or Mean ± Standard Deviation |
|---|---|
| Gender (n = 68) | |
| Female | 32 (47.1) |
| Male | 36 (52.9) |
| Age at time of diagnosis (years) (n = 68) | 18.6 ± 4.7 |
| Age at time of surgery (years) (n = 68) | 19.3 ± 4.8 |
| Pain at Diagnosis (n = 64) | |
| No | 3 (4.7) |
| Yes | 61 (95.3) |
| Pathologic Fracture at Diagnosis (n = 62) | |
| No | 54 (87.1) |
| Yes | 8 (12.9) |
| Previous Spine Tumor Operation (n = 68) | |
| No | 49 (72.1) |
| Yes | 19 (27.9) |
| Intralesional | 16 (84.2) |
| Unknown | 3 (15.8) |
| Preoperative Frankel and ASIA Score * (n = 65) | |
| A | 1 (1.5) |
| B | 2 (3.1) |
| C | 6 (9.2) |
| D | 13 (20.0) |
| E | 43 (66.2) |
| Variable | N (%) or Median (p25, p75) |
|---|---|
| Diagnosis (n = 68) | |
| Chordoma | 5 (7.4) |
| Chondrosarcoma | 12 (17.6) |
| Osteosarcoma | 18 (26.5) |
| Ewing’s sarcoma | 29 (42.6) |
| MPNST | 4 (5.9) |
| Tumor Volume Ellipsoid Body (cm3) * (n = 57) | 62.8 (20.9, 169.6) |
| <5 | 3 (5.3) |
| ≥5 | 54 (94.7) |
| Spinal level (n = 68) | |
| Mobile | 47 (69.1) |
| Fixed | 21 (30.9) |
| Level by Cervical, Thoracic, Lumbar, Sacral (n = 52) | |
| Cervical | 7 (13.5) |
| Thoracic | 13 (25.0) |
| Lumbar | 20 (38.5) |
| Sacral | 12 (23.1) |
| No. of Vertebral Levels Spanned by the Tumor (n = 68) | |
| 1 | 23 (33.8) |
| ≥2 | 45 (66.2) |
| Tumor Grade [Enneking Classification] (n = 68) | |
| Ib | 5 (7.4) |
| IIa | 7 (10.3) |
| IIb | 56 (82.4) |
| Preoperative Embolization (n = 32) | |
|---|---|
| No | 55 (84.6) |
| Yes | 10 (15.4) |
| Fixation Used (n = 68) | |
| Anterior | 1 (1.5) |
| Posterior | 41 (60.3) |
| Both | 8 (11.8) |
| None | 18 (26.5) |
| Neurology Sacrificed: Cord (n = 66) | |
| No | 65 (98.5) |
| Yes | 1 (1.5) |
| Neurology Sacrificed: Cauda Equina (n = 66) | |
| No | 64 (97.0) |
| Yes | 2 (3.0) |
| Neurology Sacrificed: Nerve Roots (n = 65) | |
| No | 28 (43.1) |
| Yes | 37 (56.9) |
| Pathology result from the surgical specimen (n = 67) | |
| Wide or marginal | 40 (59.7) |
| Intralesional | 27 (40.3) |
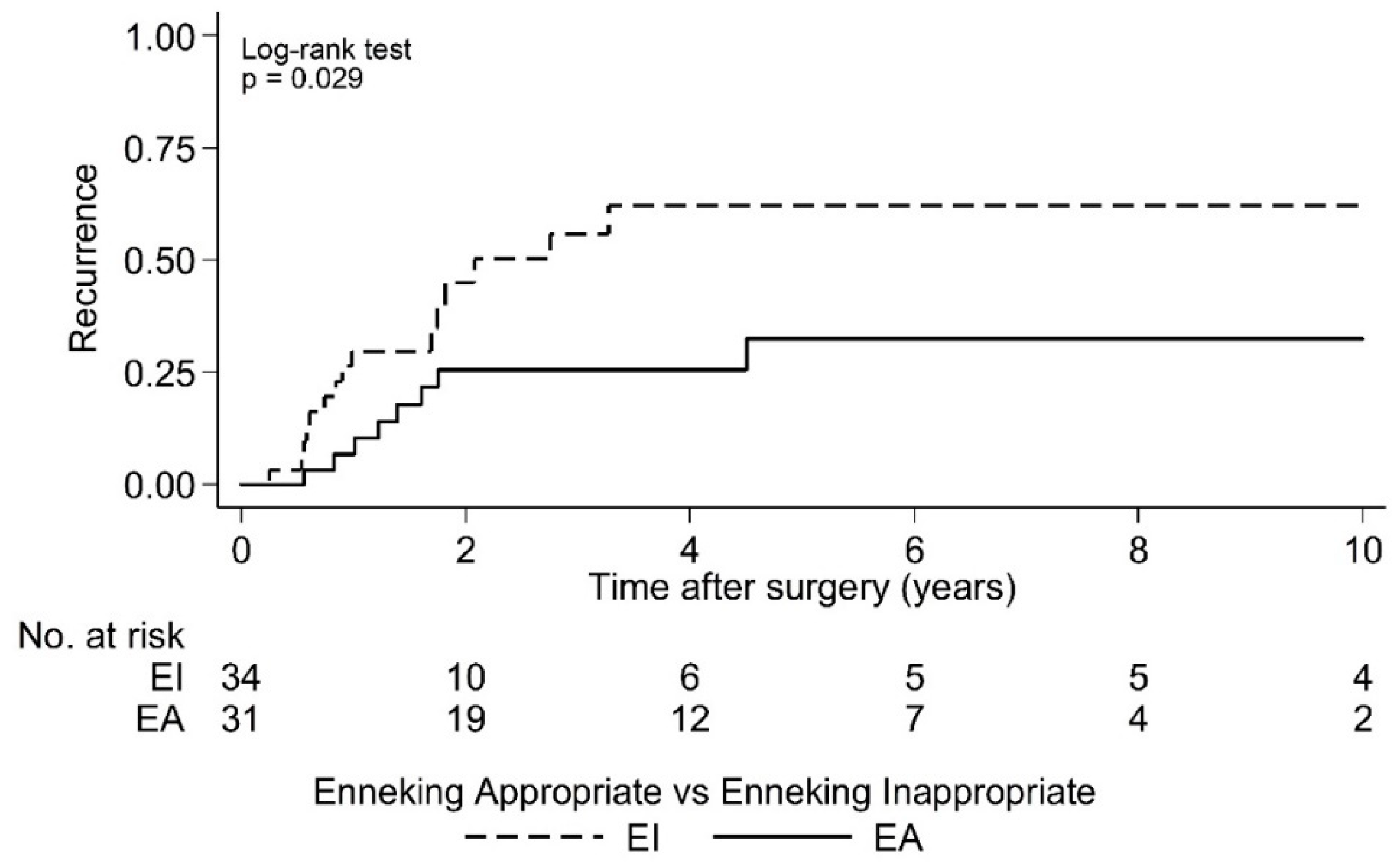
| Enneking appropriateness (n = 67) | |
| EA | 32 (47.8) |
| EI | 35 (52.2) |
| Adjuvant therapy (n = 68) | |
| No | 15 (22.1) |
| Yes | 53 (77.9) |
| Timing of chemotherapy (n = 68) | |
| Preop | 16 (23.5) |
| Postop | 8 (11.8) |
| Both | 24 (35.3) |
| Neither (no chemo) | 20 (29.4) |
| Timing of radiation therapy (n = 68) | |
| Preop | 17 (25.0) |
| Postop | 16 (23.5) |
| Both | 1 (1.5) |
| Neither (no radiation) | 34 (50.0) |
| Type of Radiation Therapy given (n = 34) | |
| Conventional | 29 (85.3) |
| IMRT | 2 (5.9) |
| Radiosurgery | 2 (5.9) |
| Proton Beam | 1 (2.9) |
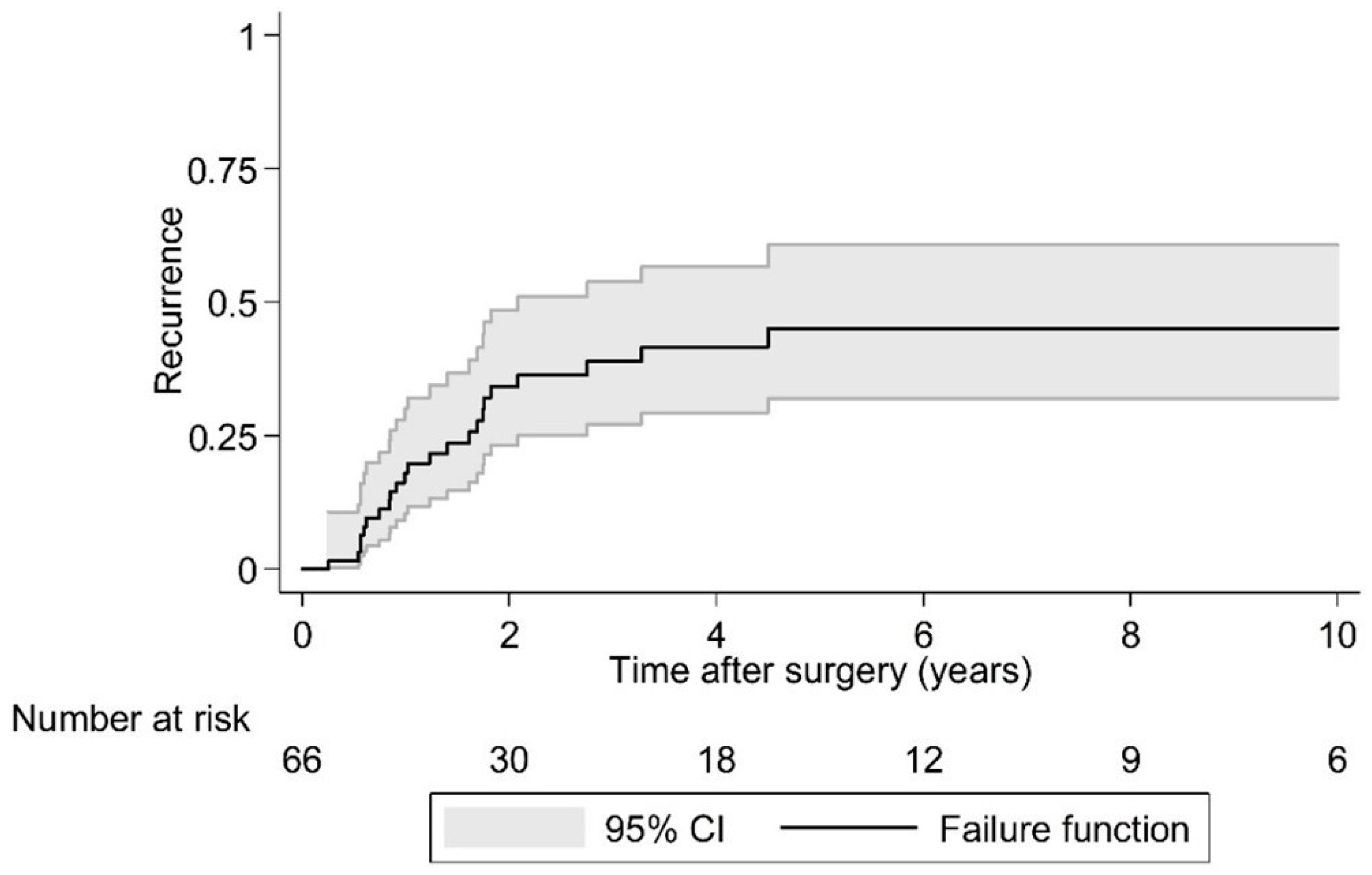
| Local recurrence over 10 years postoperative (n = 66) | |
| No | 42 (63.6) |
| Yes | 24 (36.4) |
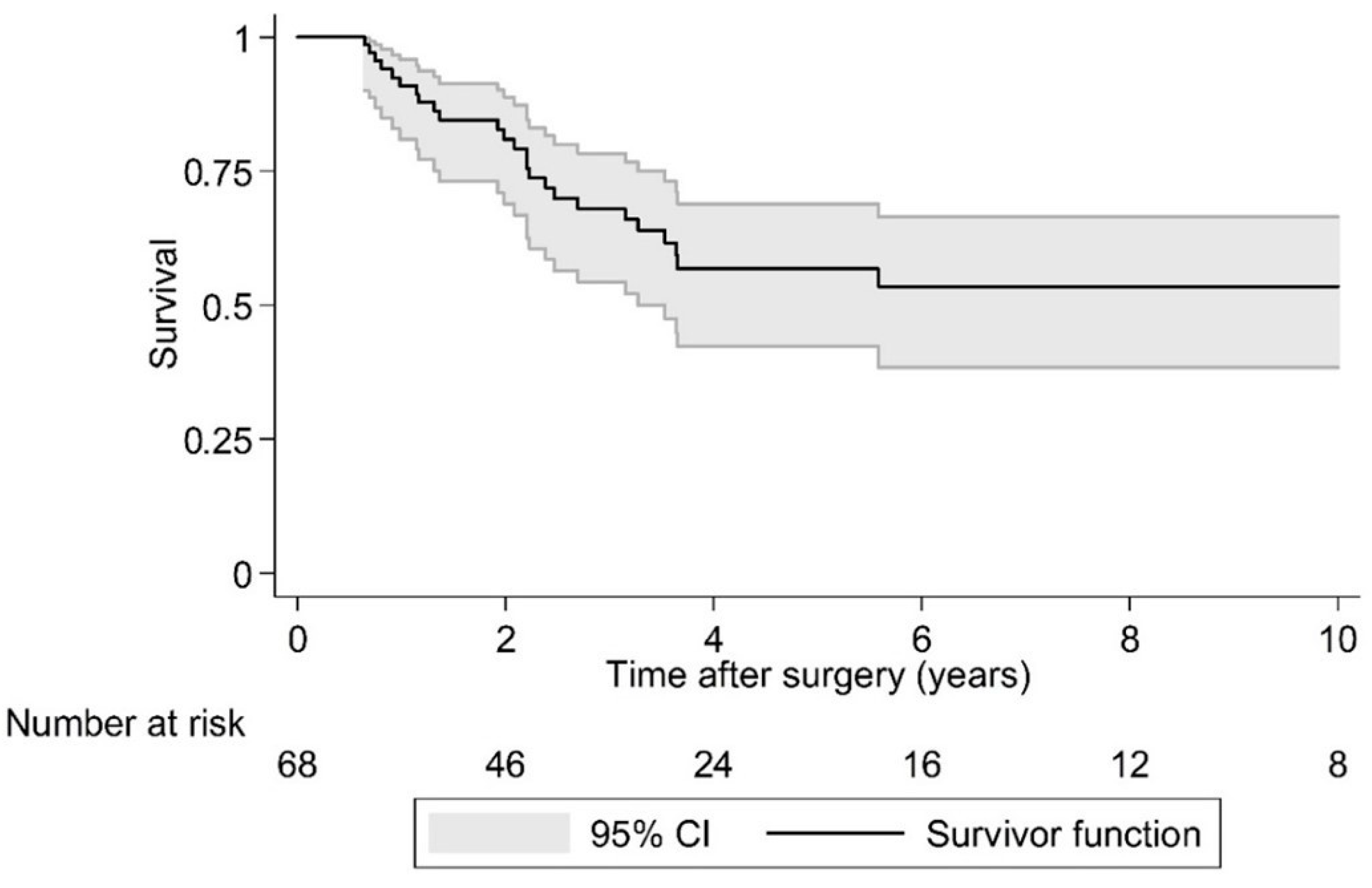
| Survival over 10 years postoperative (n = 66) | |
| Alive | 42 (63.6) |
| Dead | 24 (36.4) |
| Timing of Chemotherapy | Local Recurrence | |
| No N (%) | Yes N (%) | |
| Preop | 10 (62.5) | 6 (37.5) |
| Postop | 3 (37.5) | 5 (62.5) |
| Fisher’s exact test = 0.390 | ||
| Timing of Chemotherapy | Death | |
| No N (%) | Yes N (%) | |
| Preop | 9 (56.3) | 7 (43.8) |
| Postop | 4 (50.0) | 4 (50.0) |
| Fisher’s exact test = 1.000 | ||
| Timing of Radiation Therapy | Local Recurrence | |
| No N (%) | Yes N (%) | |
| Preop | 12 (70.6) | 5 (29.4) |
| Postop | 10 (66.7) | 5 (33.3) |
| Fisher’s exact test = 1.000 | ||
| Timing of Radiation Therapy | Death | |
| No N (%) | Yes N (%) | |
| Preop | 9 (56.3) | 7 (43.8) |
| Postop | 4 (50.0) | 11 (45.8) |
| Fisher’s exact test = 1.000 | ||
| Diagnosis | N (%) | Tumor Grade [Enneking Classification] (n = 68) N (%) | Enneking Appropriateness (n = 67) N (%) | Local Recurrence Over 10 Years Postoperative (n = 66) N (%) | Survival Over 10 Years Postoperative (n = 66) N (%) |
|---|---|---|---|---|---|
| Chordoma | 5 (7.4) | Ib = 2 (40) | EA = 4 (80) | No = 2 (40) | Alive = 3 (60) |
| IIb = 3 (60) | EI = 1 (20) | Yes = 3 (60) | Dead = 2 (40) | ||
| Chondrosarcoma | 12 (17.6) | Ib = 3 (25) | EA = 8 (66.7) | No = 9 (75) | Alive = 10 (83.3) |
| IIb = 9 (75) | EI = 4 (33.3) | Yes = 3 (25) | Dead = 2 (16.7) | ||
| Osteosarcoma | 18 (26.5) | IIb = 18 (100) | EA = 8 (44.4) | No = 12 (66.7) | Alive = 10 (55.6) |
| EI = 10 (55.6) | Yes = 6 (33.3) | Dead = 8 (44.4) | |||
| Ewing’s sarcoma | 29 (42.6) | IIa = 5 (17.2) | EA = 11 (39.3) | No = 17 (63) | Alive = 15 (55.6) |
| IIb = 24 (82.8) | EI = 17 (60.7) | Yes = 10 (37) | Dead = 12 (44.4) | ||
| MPNST | 4 (5.9) | IIa = 2 (50) | EA = 1 (25) | No = 2 (50) | Alive = 4 (100) |
| IIb = 2 (50) | EI = 3 (75) | Yes = 2 (50) | Dead = 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Disch, A.C.; Boriani, S.; Luzzati, A.; Rhines, L.D.; Fisher, C.G.; Lazary, A.; Gokaslan, Z.L.; Chou, D.; Clarke, M.J.; Fehlings, M.G.; et al. Extradural Primary Malignant Spinal Tumors in a Population Younger than 25 Years: An Ambispective International Multicenter Study on Onco-Surgical Outcomes. Cancers 2023, 15, 845. https://doi.org/10.3390/cancers15030845
Disch AC, Boriani S, Luzzati A, Rhines LD, Fisher CG, Lazary A, Gokaslan ZL, Chou D, Clarke MJ, Fehlings MG, et al. Extradural Primary Malignant Spinal Tumors in a Population Younger than 25 Years: An Ambispective International Multicenter Study on Onco-Surgical Outcomes. Cancers. 2023; 15(3):845. https://doi.org/10.3390/cancers15030845
Chicago/Turabian StyleDisch, Alexander C., Stefano Boriani, Alessandro Luzzati, Laurence D. Rhines, Charles G. Fisher, Aron Lazary, Ziya L. Gokaslan, Dean Chou, Michelle J. Clarke, Michael G. Fehlings, and et al. 2023. "Extradural Primary Malignant Spinal Tumors in a Population Younger than 25 Years: An Ambispective International Multicenter Study on Onco-Surgical Outcomes" Cancers 15, no. 3: 845. https://doi.org/10.3390/cancers15030845
APA StyleDisch, A. C., Boriani, S., Luzzati, A., Rhines, L. D., Fisher, C. G., Lazary, A., Gokaslan, Z. L., Chou, D., Clarke, M. J., Fehlings, M. G., Schaser, K.-D., Germscheid, N. M., Reynolds, J. J., & The AO Spine Knowledge Forum Tumor. (2023). Extradural Primary Malignant Spinal Tumors in a Population Younger than 25 Years: An Ambispective International Multicenter Study on Onco-Surgical Outcomes. Cancers, 15(3), 845. https://doi.org/10.3390/cancers15030845