
Liver Resection and Transplantation Following Yttrium-90 Radioembolization for Primary Malignant Liver Tumors: A 15-Year Single-Center Experience

 , ,
, ,  , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Evaluation and Eligibility
2.1.1. Inclusion Criteria
2.1.2. Criteria for Considering Patients Unsuitable for LR or LT
2.1.3. Indications for Yttrium-90 Radioembolization
2.2. Yttrium-90 Radioembolization
2.2.1. Eligibility
- (a)
- A lung shunt fraction >20% or an estimated dose of radiation to the lungs > 30 Gy;
- (b)
- Previous stereotactic body radiation therapy to the liver;
- (c)
- Presence of collateral vessels feeding extrahepatic organs that cannot be corrected by angiographic techniques.
2.2.2. Radioembolization Protocol
2.3. Response to Radioembolization, Re-Evaluation, and Eligibility for Liver Resection or Transplantation
2.4. Surgical Outcomes
2.5. Data Collection
2.6. Statistical Analysis
3. Results
3.1. Radioembolization Characteristics and Outcomes
3.2. Surgical Outcomes
3.2.1. Liver Resection
3.2.2. Laparoscopic Liver Resection
3.2.3. Liver Transplantation
3.3. Postoperative Outcomes
3.3.1. Liver Resection
3.3.2. Liver Transplantation
3.4. Survival Analysis
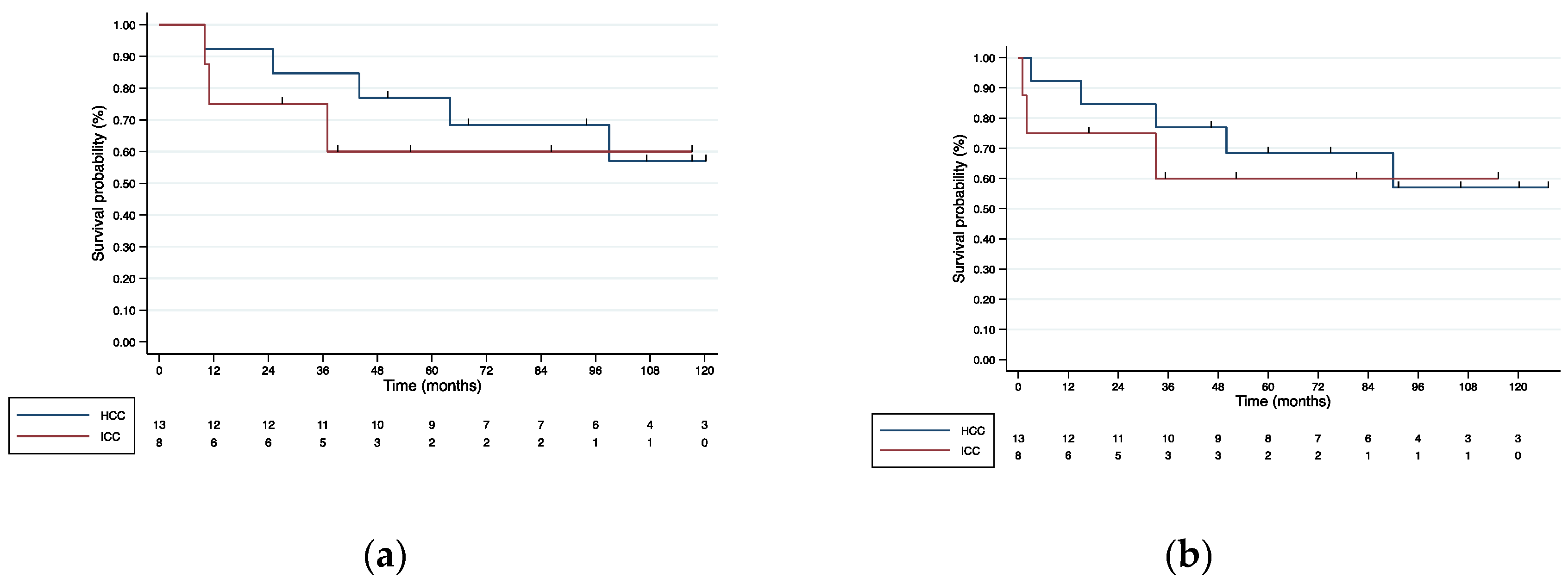
3.4.1. Liver Resection
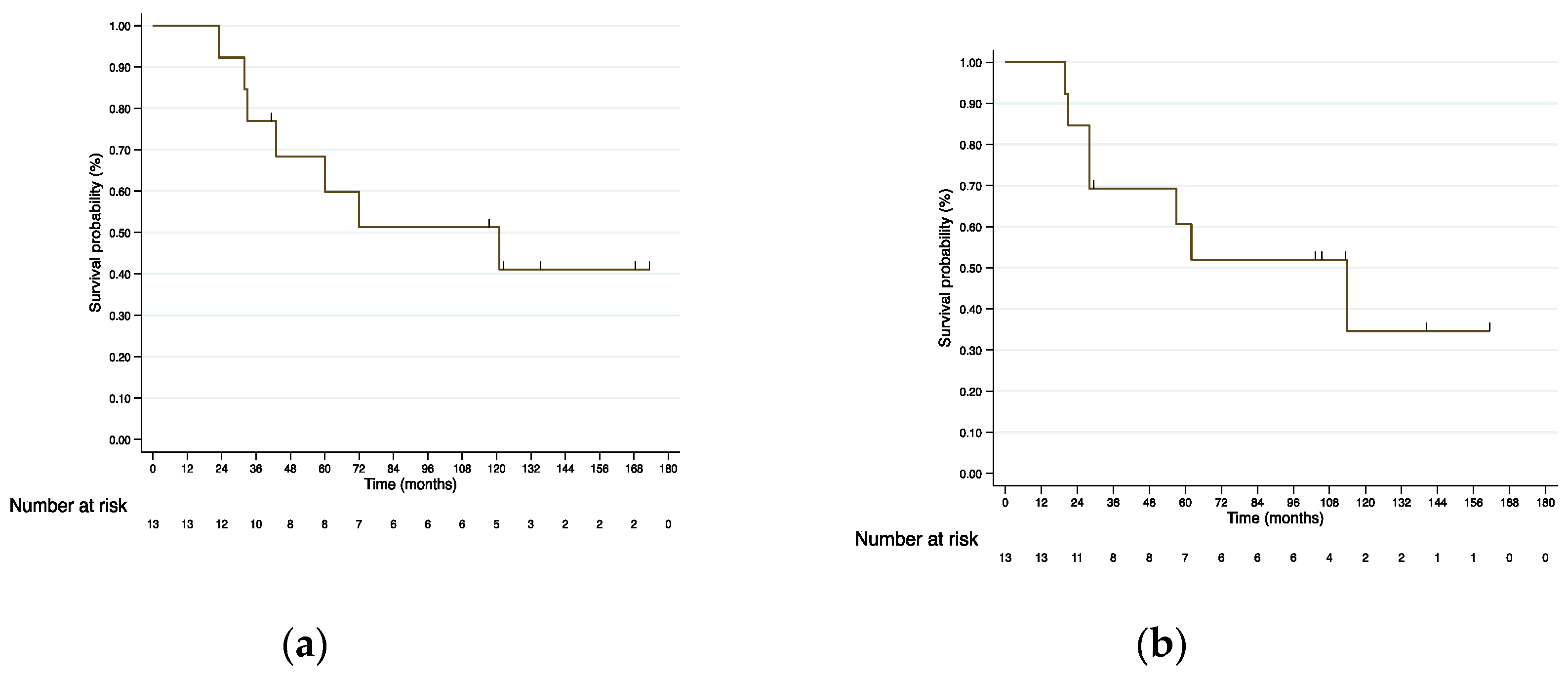
3.4.2. Liver Transplantation
4. Discussion
4.1. Liver Resection
4.1.1. Postoperative Outcomes
4.1.2. HCC Survival Outcomes
4.1.3. ICC Survival Outcomes
4.2. Liver Transplantation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Rumgay, H.; Ferlay, J.; de Martel, C.; Georges, D.; Ibrahim, A.S.; Zheng, R.; Wei, W.; Lemmens, V.E.P.P.; Soerjomataram, I. Global, Regional and National Burden of Primary Liver Cancer by Subtype. Eur. J. Cancer. 2022, 161, 108–118. [Google Scholar] [CrossRef]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, Regional, and National Life Expectancy, All-Cause Mortality, and Cause-Specific Mortality for 249 Causes of Death, 1980–2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.-L.; Schirmacher, P.; Vilgrain, V.; European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Weber, S.M.; Ribero, D.; O’Reilly, E.M.; Kokudo, N.; Miyazaki, M.; Pawlik, T.M. Intrahepatic Cholangiocarcinoma: Expert Consensus Statement. Hpb 2015, 17, 669–680. [Google Scholar] [CrossRef]
- Llovet, J.M.; Baere, T.D.; Kulik, L.; Haber, P.K.; Greten, T.F.; Meyer, T.; Lencioni, R. Locoregional Therapies in the Era of Molecular and Immune Treatments for Hepatocellular Carcinoma. Nat. Rev. Gastroentero. 2021, 18, 293–313. [Google Scholar] [CrossRef]
- Sangro, B.; Salem, R.; Kennedy, A.; Coldwell, D.; Wasan, H. Radioembolization for Hepatocellular Carcinoma. Am. J. Clin. Oncol. 2011, 34, 422–431. [Google Scholar] [CrossRef]
- Sangro, B.; Bilbao, J.I.; Boan, J.; Martinez-Cuesta, A.; Benito, A.; Rodriguez, J.; Panizo, A.; Gil, B.; Inarrairaegui, M.; Herrero, I.; et al. Radioembolization Using 90Y-Resin Microspheres for Patients with Advanced Hepatocellular Carcinoma. Int J. Radiat. Oncol. Biology Phys. 2006, 66, 792–800. [Google Scholar] [CrossRef]
- Salem, R.; Johnson, G.E.; Kim, E.; Riaz, A.; Bishay, V.; Boucher, E.; Fowers, K.; Lewandowski, R.; Padia, S.A. Yttrium-90 Radioembolization for the Treatment of Solitary, Unresectable Hepatocellular Carcinoma: The LEGACY Study. Hepatology 2021. [Google Scholar] [CrossRef]
- Kulik, L.M.; Carr, B.I.; Mulcahy, M.F.; Lewandowski, R.J.; Atassi, B.; Ryu, R.K.; Sato, K.T.; Benson, A.; Nemcek, A.A.; Gates, V.L.; et al. Safety and Efficacy of 90Y Radiotherapy for Hepatocellular Carcinoma with and without Portal Vein Thrombosis. Hepatology 2008, 47, 71–81. [Google Scholar] [CrossRef]
- Iñarrairaegui, M.; Pardo, F.; Bilbao, J.I.; Rotellar, F.; Benito, A.; D’Avola, D.; Herrero, J.I.; Rodriguez, M.; Martí, P.; Zozaya, G.; et al. Response to Radioembolization with Yttrium-90 Resin Microspheres May Allow Surgical Treatment with Curative Intent and Prolonged Survival in Previously Unresectable Hepatocellular Carcinoma. Eur. J. Surg. Oncol. EJSO 2012, 38, 594–601. [Google Scholar] [CrossRef]
- Riby, D.; Mazzotta, A.D.; Bergeat, D.; Verdure, L.; Sulpice, L.; Bourien, H.; Lièvre, A.; Rolland, Y.; Garin, E.; Boudjema, K.; et al. Downstaging with Radioembolization or Chemotherapy for Initially Unresectable Intrahepatic Cholangiocarcinoma. Ann. Surg. Oncol. 2020, 27, 3729–3737. [Google Scholar] [CrossRef]
- Tohme, S.; Sukato, D.; Chen, H.; Amesur, N.; Zajko, A.B.; Humar, A.; Geller, D.A.; Marsh, J.W.; Tsung, A. Yttrium-90 Radioembolization as a Bridge to Liver Transplantation: A Single-Institution Experience. J. Vasc. Interv. Radiol. 2013, 24, 1632–1638. [Google Scholar] [CrossRef]
- Salem, R.; Gordon, A.C.; Mouli, S.; Hickey, R.; Kallini, J.; Gabr, A.; Mulcahy, M.F.; Baker, T.; Abecassis, M.; Miller, F.H.; et al. Y90 Radioembolization Significantly Prolongs Time to Progression Compared with Chemoembolization in Patients with Hepatocellular Carcinoma. Gastroenterology 2016, 151, 1155–1163.e2. [Google Scholar] [CrossRef]
- Gaba, R.C.; Lewandowski, R.J.; Kulik, L.M.; Riaz, A.; Ibrahim, S.M.; Mulcahy, M.F.; Ryu, R.K.; Sato, K.T.; Gates, V.; Abecassis, M.M.; et al. Radiation Lobectomy: Preliminary Findings of Hepatic Volumetric Response to Lobar Yttrium-90 Radioembolization. Ann. Surg. Oncol. 2009, 16, 1587–1596. [Google Scholar] [CrossRef]
- Noda, C.; Williams, G.A.; Foltz, G.; Kim, H.; Sanford, D.E.; Hammill, C.W.; Fields, R.C. The Safety of Hepatectomy after Transarterial Radioembolization: Single Institution Experience and Review of the Literature. J. Surg. Oncol. 2020. [Google Scholar] [CrossRef]
- Imamura, H.; Sano, K.; Sugawara, Y.; Kokudo, N.; Makuuchi, M. Assessment of Hepatic Reserve for Indication of Hepatic Resection: Decision Tree Incorporating Indocyanine Green Test. J. Hepato-Biliary-Pancreat. Surg. 2005, 12, 16–22. [Google Scholar] [CrossRef]
- Herrero, J.I.; Sangro, B.; Quiroga, J.; Pardo, F.; Herraiz, M.; Cienfuegos, J.A.; Prieto, J. Influence of Tumor Characteristics on the Outcome of Liver Transplantation among Patients with Liver Cirrhosis and Hepatocellular Carcinoma. Liver Transpl. 2001, 7, 631–636. [Google Scholar] [CrossRef]
- Herrero, J.I.; Sangro, B.; Pardo, F.; Quiroga, J.; Iñarrairaegui, M.; Rotellar, F.; Montiel, C.; Alegre, F.; Prieto, J. Liver Transplantation in Patients with Hepatocellular Carcinoma across Milan Criteria. Liver Transpl. 2008, 14, 272–278. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Llovet, J.M.; Miceli, R.; Bhoori, S.; Schiavo, M.; Mariani, L.; Camerini, T.; Roayaie, S.; Schwartz, M.E.; Grazi, G.L.; et al. Predicting Survival after Liver Transplantation in Patients with Hepatocellular Carcinoma beyond the Milan Criteria: A Retrospective, Exploratory Analysis. Lancet Oncol. 2009, 10, 35–43. [Google Scholar] [CrossRef]
- Fernández-Ros, N.; Silva, N.; Bilbao, J.I.; Iñarrairaegui, M.; Benito, A.; D’Avola, D.; Rodriguez, M.; Rotellar, F.; Pardo, F.; Sangro, B. Partial Liver Volume Radioembolization Induces Hypertrophy in the Spared Hemiliver and No Major Signs of Portal Hypertension. Hpb 2014, 16, 243–249. [Google Scholar] [CrossRef]
- Edeline, J.; Lenoir, L.; Boudjema, K.; Rolland, Y.; Boulic, A.; Du, F.L.; Pracht, M.; Raoul, J.-L.; Clément, B.; Garin, E.; et al. Volumetric Changes after 90Y Radioembolization for Hepatocellular Carcinoma in Cirrhosis: An Option to Portal Vein Embolization in a Preoperative Setting? Ann. Surg. Oncol. 2013, 20, 2518–2525. [Google Scholar] [CrossRef] [PubMed]
- Gil-Alzugaray, B.; Chopitea, A.; Iñarrairaegui, M.; Bilbao, J.I.; Rodriguez-Fraile, M.; Rodriguez, J.; Benito, A.; Dominguez, I.; D’Avola, D.; Herrero, J.I.; et al. Prognostic Factors and Prevention of Radioembolization-induced Liver Disease. Hepatology 2013, 57, 1078–1087. [Google Scholar] [CrossRef]
- Sirtex Medical. SIR-Spheres® Y-90 Resin Microspheres Activity Chart; Sirtex Medical: Woburn, MA, USA, 2020. [Google Scholar]
- U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0; National Institutes of Health: Bethesda, MA, USA, 2018. [Google Scholar]
- Sangro, B.; Gil-Alzugaray, B.; Rodriguez, J.; Sola, I.; Martinez-Cuesta, A.; Viudez, A.; Chopitea, A.; Iñarrairaegui, M.; Arbizu, J.; Bilbao, J.I. Liver Disease Induced by Radioembolization of Liver Tumors. Cancer 2008, 112, 1538–1546. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Garden, O.J.; Padbury, R.; Brooke-Smith, M.; Crawford, M.; Adam, R.; Koch, M.; Makuuchi, M.; Dematteo, R.P.; Christophi, C.; et al. Posthepatectomy Liver Failure: A Definition and Grading by the International Study Group of Liver Surgery (ISGLS). Surgery 2011, 149, 713–724. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Garden, O.J.; Padbury, R.; Maddern, G.; Koch, M.; Hugh, T.J.; Fan, S.T.; Nimura, Y.; Figueras, J.; Vauthey, J.; et al. Post-hepatectomy Haemorrhage: A Definition and Grading by the International Study Group of Liver Surgery (ISGLS). Hpb 2011, 13, 528–535. [Google Scholar] [CrossRef]
- Koch, M.; Garden, O.J.; Padbury, R.; Rahbari, N.N.; Adam, R.; Capussotti, L.; Fan, S.T.; Yokoyama, Y.; Crawford, M.; Makuuchi, M.; et al. Bile Leakage after Hepatobiliary and Pancreatic Surgery: A Definition and Grading of Severity by the International Study Group of Liver Surgery. Surgery 2011, 149, 680–688. [Google Scholar] [CrossRef]
- Wakabayashi, G. What Has Changed after the Morioka Consensus Conference 2014 on Laparoscopic Liver Resection? Hepatobiliary Surg. Nutr. 2016, 5, 281–289. [Google Scholar] [CrossRef]
- Halls, M.C.; Berardi, G.; Cipriani, F.; Barkhatov, L.; Lainas, P.; Harris, S.; D’Hondt, M.; Rotellar, F.; Dagher, I.; Aldrighetti, L.; et al. Development and Validation of a Difficulty Score to Predict Intraoperative Complications during Laparoscopic Liver Resection. Brit. J. Surg 2018, 105, 1182–1191. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications. Ann. Surg 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Aliseda, D.; Martí-Cruchaga, P.; Zozaya, G.; Benito, A.; Lopez-Olaondo, L.; Rodríguez-Fraile, M.; Bilbao, J.I.; Hidalgo, F.; Iñarrairaegui, M.; Ciria, R.; et al. Pure Laparoscopic Major Liver Resection after Yttrium90 Radioembolization: A Case-Matched Series Analysis of Feasibility and Outcomes. Langenbeck’s Archives Surg. 2022, 407, 1099–1111. [Google Scholar] [CrossRef]
- Jakobs, T.F.; Saleem, S.; Atassi, B.; Reda, E.; Lewandowski, R.J.; Yaghmai, V.; Miller, F.; Ryu, R.K.; Ibrahim, S.; Sato, K.T.; et al. Fibrosis, Portal Hypertension, and Hepatic Volume Changes Induced by Intra-Arterial Radiotherapy with 90Yttrium Microspheres. Digest Dis. Sci. 2008, 53, 2556–2563. [Google Scholar] [CrossRef]
- Chua, T.C.; Bester, L.; Akther, J.; Morris, D.L. Successful Right Hepatectomy after Four Treatments of Yttrium-90 Microspheres (SIR-Spheres) and Concomitant FOLFOX as Bridging Therapy to Resection of Colorectal Liver Metastases. Anticancer Res. 2010, 30, 3005–3007. [Google Scholar]
- Pardo, F.; Sangro, B.; Lee, R.-C.; Manas, D.; Jeyarajah, R.; Donckier, V.; Maleux, G.; Pinna, A.D.; Bester, L.; Morris, D.L.; et al. The Post-SIR-Spheres Surgery Study (P4S): Retrospective Analysis of Safety Following Hepatic Resection or Transplantation in Patients Previously Treated with Selective Internal Radiation Therapy with Yttrium-90 Resin Microspheres. Ann. Surg. Oncol. 2017, 24, 2465–2473. [Google Scholar] [CrossRef]
- Gulec, S.A.; Pennington, K.; Hall, M.; Fong, Y. Preoperative Y-90 Microsphere Selective Internal Radiation Treatment for Tumor Downsizing and Future Liver Remnant Recruitment: A Novel Approach to Improving the Safety of Major Hepatic Resections. World J. Surg. Oncol. 2009, 7, 6. [Google Scholar] [CrossRef]
- Gabr, A.; Abouchaleh, N.; Ali, R.; Baker, T.; Caicedo, J.; Katariya, N.; Abecassis, M.; Riaz, A.; Lewandowski, R.J.; Salem, R. Outcomes of Surgical Resection after Radioembolization for Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2018, 29, 1502–1510.e1. [Google Scholar] [CrossRef]
- Henry, L.R.; Hostetter, R.B.; Ressler, B.; Bowser, I.; Yan, M.; Vaghefi, H.; Abad, J.; Gulec, S.; Schwarz, R.E. Liver Resection for Metastatic Disease After Y90 Radioembolization: A Case Series with Long-Term Follow-Up. Ann. Surg. Oncol. 2015, 22, 467–474. [Google Scholar] [CrossRef]
- Chan, J.; Perini, M.; Fink, M.; Nikfarjam, M. The Outcomes of Central Hepatectomy versus Extended Hepatectomy: A Systematic Review and Meta-Analysis. Hpb 2018, 20, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Ratti, F.; Cipriani, F.; Ariotti, R.; Giannone, F.; Paganelli, M.; Aldrighetti, L. Laparoscopic Major Hepatectomies: Current Trends and Indications. A Comparison with the Open Technique. Updat. Surg. 2015, 67, 157–167. [Google Scholar] [CrossRef]
- Ciria, R.; Gomez-Luque, I.; Ocaña, S.; Cipriani, F.; Halls, M.; Briceño, J.; Okuda, Y.; Troisi, R.; Rotellar, F.; Soubrane, O.; et al. A Systematic Review and Meta-Analysis Comparing the Short- and Long-Term Outcomes for Laparoscopic and Open Liver Resections for Hepatocellular Carcinoma: Updated Results from the European Guidelines Meeting on Laparoscopic Liver Surgery, Southampton, UK, 2017. Ann. Surg. Oncol. 2019, 26, 252–263. [Google Scholar] [CrossRef]
- Kabir, T.; Tan, Z.Z.; Syn, N.L.; Wu, E.; Lin, J.D.; Zhao, J.J.; Tan, A.Y.H.; Hui, Y.; Kam, J.H.; Goh, B.K.P. Laparoscopic versus Open Resection of Hepatocellular Carcinoma in Patients with Cirrhosis: Meta-Analysis. Brit. J. Surg. 2021, 109, 21–29. [Google Scholar] [CrossRef]
- Rotellar, F.; Zozaya, G.; Martí-Cruchaga, P.; Pardo, F. Laparoscopic Right Hepatectomy after Radioembolization Using Yttrium-90 Resin Microspheres. Surg. Oncol. 2017, 26, 71–72. [Google Scholar] [CrossRef] [PubMed]
- Rotellar, F.; Pardo, F.; Martnez-Ortega, P. The Safety of Resection Post-Selective Internal Radiation Therapy. Future Oncol. 2014, 10, 53–55. [Google Scholar] [CrossRef]
- Lim, K.-C.; Chow, P.K.-H.; Allen, J.C.; Siddiqui, F.J.; Chan, E.S.-Y.; Tan, S.-B. Systematic Review of Outcomes of Liver Resection for Early Hepatocellular Carcinoma within the Milan Criteria. Brit. J. Surg. 2012, 99, 1622–1629. [Google Scholar] [CrossRef]
- Chan, A.; Zhang, W.Y.; Chok, K.; Dai, J.; Ji, R.; Kwan, C.; Man, N.; Poon, R.; Lo, C.M. ALPPS Versus Portal Vein Embolization for Hepatitis-Related Hepatocellular Carcinoma: A Changing Paradigm in Modulation of Future Liver Remnant Before Major Hepatectomy. Ann. Surg. 2019, 273, 957–965. [Google Scholar] [CrossRef]
- Lemaire, M.; Lucidi, V.; Bouazza, F.; Katsanos, G.; Vanderlinden, B.; Levillain, H.; Delatte, P.; Garcia, C.A.; Vouche, M.; Galdon, M.G.; et al. Selective Internal Radiation Therapy (SIRT) before Partial Hepatectomy or Radiofrequency Destruction for Treatment of Hepatocellular Carcinoma in Cirrhotic Patients: A Feasibility and Safety Pilot Study. Hpb 2018, 20, 641–648. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Gorgen, A.; Roayaie, S.; dit Busset, M.D.; Sapisochin, G. Liver Resection and Transplantation for Intrahepatic Cholangiocarcinoma. J. Hepatol. 2020, 72, 364–377. [Google Scholar] [CrossRef]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next Horizon in Mechanisms and Management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef]
- Edeline, J.; Touchefeu, Y.; Guiu, B.; Farge, O.; Tougeron, D.; Baumgaertner, I.; Ayav, A.; Campillo-Gimenez, B.; Beuzit, L.; Pracht, M.; et al. Radioembolization Plus Chemotherapy for First-Line Treatment of Locally Advanced Intrahepatic Cholangiocarcinoma. JAMA Oncol. 2020, 6, 51–59. [Google Scholar] [CrossRef]
- Rayar, M.; Sulpice, L.; Edeline, J.; Garin, E.; Sandri, G.B.L.; Meunier, B.; Boucher, E.; Boudjema, K. Intra-Arterial Yttrium-90 Radioembolization Combined with Systemic Chemotherapy Is a Promising Method for Downstaging Unresectable Huge Intrahepatic Cholangiocarcinoma to Surgical Treatment. Ann. Surg. Oncol. 2015, 22, 3102–3108. [Google Scholar] [CrossRef]
- Oligane, H.C.; Xing, M.; Kim, H.S. Effect of Bridging Local-Regional Therapy on Recurrence of Hepatocellular Carcinoma and Survival after Orthotopic Liver Transplantation. Radiology 2016, 282, 869–879. [Google Scholar] [CrossRef]
- Salem, R.; Gabr, A.; Riaz, A.; Mora, R.; Ali, R.; Abecassis, M.; Hickey, R.; Kulik, L.; Ganger, D.; Flamm, S.; et al. Institutional Decision to Adopt Y90 as Primary Treatment for Hepatocellular Carcinoma Informed by a 1,000-patient 15-year Experience. Hepatology 2018, 68, 1429–1440. [Google Scholar] [CrossRef] [PubMed]
- Oligane, H.C.; Close, O.N.; Xing, M.; Kim, H.S. Bridging Locoregional Therapy: Longitudinal Trends and Outcomes in Patients with Hepatocellular Carcinoma. Transplant. Rev. 2017, 31, 136–143. [Google Scholar] [CrossRef]
- Gabr, A.; Kulik, L.; Mouli, S.; Riaz, A.; Ali, R.; Desai, K.; Mora, R.A.; Ganger, D.; Maddur, H.; Flamm, S.; et al. Liver Transplantation following Yttrium-90 Radioembolization: 15-Year Experience in 207-Patient Cohort. Hepatology 2020. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N. Engl. J. Med. 1996, 334, 693–700. [Google Scholar] [CrossRef]
- Grisanti, F.; Prieto, E.; Bastidas, J.F.; Sancho, L.; Rodrigo, P.; Beorlegui, C.; Iñarrairaegui, M.; Bilbao, J.I.; Sangro, B.; Rodríguez-Fraile, M. 3D Voxel-Based Dosimetry to Predict Contralateral Hypertrophy and an Adequate Future Liver Remnant after Lobar Radioembolization. Eur. J. Nucl. Med. Mol. I 2021, 48, 3048–3057. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fábrega, J.; Burrel, M.; Garcia-Criado, A.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC Strategy for Prognosis Prediction and Treatment Recommendation Barcelona Clinic Liver Cancer (BCLC) Staging System. The 2022 Update. J. Hepatol. 2021, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Whole Cohort (n = 34) | Resection (n = 21) | Transplantation (n = 13) | |
|---|---|---|---|
| Age (years) a | 64.7 (1.2) | 66.3 (1.1) | 62 (1.3) |
| Sex (M:F) | 32:2 | 19:2 | 13:0 |
| Tumor type | |||
| HCC | 26 (76.4) | 13 (61.9) | 13 (100) |
| ICC | 8 (23.6) | 8 (38.1) | 0 (0.0) |
| BMI (kg/m2) a | 28.1 (0.7) | 27.4 (0.7) | 29.1 (1.2) |
| ASA score b | 3 (2–4) | 3 (2–4) | 3 (3–4) |
| Comorbidities | |||
| Hypertension | 14 (41.2) | 12 (57.1) | 2 (15.4) |
| Cardiopathy | 15 (44.1) | 8 (38.1) | 7 (53.8) |
| Diabetes | 10 (29.4) | 5 (23.8) | 5 (38.5) |
| COPD | 2 (5.9) | 2 (9.5) | 0 (0.0) |
| Chronic renal injury | 4 (11.8) | 3 (14.3) | 1 (7.7) |
| Prior abdominal surgery | 13 (38.2) | 10 (29.4) | 3 (23.1) |
| Pre-operative tumor size (cm) a | 6.3 (0.7) | 8.2 (0.8) | 3.4 (1.4) |
| Total bilirubin (mg/dl) b | 0.9 (0.4–6.8) | 0.7 (0.4–1.7) | 1.7 (0.5–6.8) |
| Prior liver procedure | 8 (23.6) | 4 (19.0) | 4 (30.7) |
| Resection | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Ablation | 4 (11.8) | 2 (9.5) | 2 (15.4) |
| Portal vein embolization | 2 (5.9) | 2 (9.5) | 0 (0.0) |
| TACE | 2 (5.9) | 0 (0.0) | 2 (15.4) |
| RE treatment | |||
| Whole liver radiation | 3 (8.9) | 3 (14.3) | 0 (0.0) |
| Lobar extended | 5 (14.7) | 4 (19.0) | 1 (7.7) |
| Lobar | 13 (38.2) | 6 (28.6) | 7 (53.8) |
| Segmental | 13 (38.2) | 8 (38.1) | 5 (38.5) |
| Pre-RE systemic treatment + | 10 (29.4) | 10 (47.6) | 0 (0.0) |
| Post-RE systemic treatment | 8 (23.5) | 8 (38.1) | 0 (0.0) |
| HCC Cohort (n = 26) | Resection (n = 13) | Transplantation (n = 13) | |
|---|---|---|---|
| Cirrhosis (Child–Pugh) | 23 (88.5) | 10 (76.9) | 13 (100) |
| Grade A | 20 (87.0) | 9 (90.0) | 11 (84.6) |
| Grade B | 3 (13.0) | 1 (10.0) | 2 (15.4) |
| Grade C | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Staging BCLC | |||
| BCLC A | 9 (34.6) | 2 (15.4) | 7 (53.8) |
| BCLC B | 14 (53.8) | 8 (61.5) | 6 (46.2) |
| BCLC C | 3 (11.5) | 3 (23.1) | 0 (0.0) |
| Etiology of HCC | |||
| Alcoholic cirrhosis | 9 (34.6) | 1 (7.7) | 8 (61.5) |
| HCV | 8 (30.8) | 6 (46.2) | 2 (15.4) |
| HBV | 2 (7.7) | 0 (0.0) | 2 (15.4) |
| NASH | 1 (3.8) | 1 (7.7) | 0 (0.0) |
| Hemochromatosis | 2 (7.7) | 2 (15.4) | 0 (0.0) |
| Cryptogenic | 4 (15.4) | 3 (23.1) | 1 (7.7) |
| Serum AFP (ng/mL) a | 5.99 (1.7–10659) | 2685 (1.8–10659) | 9.75 (1.7–805) |
| Whole Cohort (n = 34) | Resected (n = 21) | Transplanted (n = 13) | |||
|---|---|---|---|---|---|
| Postoperative Outcomes | Whole | Open (n = 12) | LLR (n = 9) | ||
| Hospital stay (day) a | 6 (3–17) | 5 (3–17) | 9.5 (4–17) | 3.5 (3–11) | 6 (5–16) |
| Overall complication | 13 (38.2) | 9 (42.9) | 6 (50.0) | 3 (33.3) | 4 (30.8) |
| Clavien–Dindo III-IV | 5 (14.7) | 4 (19.0) | 2 (16.7) | 2 (22.2) | 1 (7.7) |
| PHLF (ISGLS) | |||||
| PHLF C | 1 (2.9) | 1 (4.8) | 1 (4.8) | 0 (0.0) | 0 (0.0) |
| PHH (ISGLS) | |||||
| PHH C | 1 (2.9) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (7.7) |
| Bile leakage (≥grade B) (ISGLS) | 3 (8.8) | 3 (14.3) | 2 (16.7) | 1 (11.1) | 0 (0.0) |
| Re-operation | 2 (5.9) | 1 (4.8) | 0 (0.0) | 1 (11.1) | 1 (7.7) |
| 90 days readmission | 4 (11.8) | 2 (9.5) | 1 (4.8) | 1 (11.1) | 2 (15.4) |
| 90 days mortality | 2 (5.9) | 2 (9.5) | 2 (16.7) | 0 (0.0) | 0 (0.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aliseda, D.; Martí-Cruchaga, P.; Zozaya, G.; Rodríguez-Fraile, M.; Bilbao, J.I.; Benito-Boillos, A.; Martínez De La Cuesta, A.; Lopez-Olaondo, L.; Hidalgo, F.; Ponz-Sarvisé, M.; et al. Liver Resection and Transplantation Following Yttrium-90 Radioembolization for Primary Malignant Liver Tumors: A 15-Year Single-Center Experience. Cancers 2023, 15, 733. https://doi.org/10.3390/cancers15030733
Aliseda D, Martí-Cruchaga P, Zozaya G, Rodríguez-Fraile M, Bilbao JI, Benito-Boillos A, Martínez De La Cuesta A, Lopez-Olaondo L, Hidalgo F, Ponz-Sarvisé M, et al. Liver Resection and Transplantation Following Yttrium-90 Radioembolization for Primary Malignant Liver Tumors: A 15-Year Single-Center Experience. Cancers. 2023; 15(3):733. https://doi.org/10.3390/cancers15030733
Chicago/Turabian StyleAliseda, Daniel, Pablo Martí-Cruchaga, Gabriel Zozaya, Macarena Rodríguez-Fraile, José I. Bilbao, Alberto Benito-Boillos, Antonio Martínez De La Cuesta, Luis Lopez-Olaondo, Francisco Hidalgo, Mariano Ponz-Sarvisé, and et al. 2023. "Liver Resection and Transplantation Following Yttrium-90 Radioembolization for Primary Malignant Liver Tumors: A 15-Year Single-Center Experience" Cancers 15, no. 3: 733. https://doi.org/10.3390/cancers15030733
APA StyleAliseda, D., Martí-Cruchaga, P., Zozaya, G., Rodríguez-Fraile, M., Bilbao, J. I., Benito-Boillos, A., Martínez De La Cuesta, A., Lopez-Olaondo, L., Hidalgo, F., Ponz-Sarvisé, M., Chopitea, A., Rodríguez, J., Iñarrairaegui, M., Herrero, J. I., Pardo, F., Sangro, B., & Rotellar, F. (2023). Liver Resection and Transplantation Following Yttrium-90 Radioembolization for Primary Malignant Liver Tumors: A 15-Year Single-Center Experience. Cancers, 15(3), 733. https://doi.org/10.3390/cancers15030733