
Is Reflex Germline BRCA1/2 Testing Necessary in Women Diagnosed with Non-Mucinous High-Grade Epithelial Ovarian Cancer Aged 80 Years or Older?
 , , , , ,
, , , , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mateo, J.; Lord, C.J.; Serra, V.; Tutt, A.; Balmana, J.; Castroviejo-Bermejo, M.; Cruz, C.; Oaknin, A.; Kaye, S.B.; de Bono, J.S. A decade of clinical development of PARP inhibitors in perspective. Ann. Oncol. 2019, 30, 1437–1447. [Google Scholar] [CrossRef] [PubMed]
- Parmigiani, G.; Berry, D.; Aguilar, O. Determining carrier probabilities for breast cancer-susceptibility genes BRCA1 and BRCA2. Am. J. Hum. Genet. 1998, 62, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, A.C.; Pharoah, P.P.; Smith, P.; Easton, D.F. The BOADICEA model of genetic susceptibility to breast and ovarian cancer. Br. J. Cancer 2004, 91, 1580–1590. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.; Eccles, D.M.; Rahman, N.; Young, K.; Bulman, M.; Amir, E.; Shenton, A.; Howell, A.; Lalloo, F. A new scoring system for the chances of identifying a BRCA1/2 mutation outperforms existing models including BRCAPRO. J. Med. Genet. 2004, 41, 474–480. [Google Scholar] [CrossRef] [PubMed]
- George, A.; Riddell, D.; Seal, S.; Talukdar, S.; Mahamdallie, S.; Ruark, E.; Cloke, V.; Slade, I.; Kemp, Z.; Gore, M.; et al. Implementing rapid, robust, cost-effective, patient-centred, routine genetic testing in ovarian cancer patients. Sci. Rep. 2016, 6, 29506. [Google Scholar] [CrossRef]
- Plaskocinska, I.; Shipman, H.; Drummond, J.; Thompson, E.; Buchanan, V.; Newcombe, B.; Hodgkin, C.; Barter, E.; Ridley, P.; Ng, R.; et al. New paradigms for BRCA1/BRCA2 testing in women with ovarian cancer: Results of the Genetic Testing in Epithelial Ovarian Cancer (GTEOC) study. J. Med. Genet. 2016, 53, 655–661. [Google Scholar] [CrossRef]
- Rust, K.; Spiliopoulou, P.; Tang, C.Y.; Bell, C.; Stirling, D.; Phang, T.; Davidson, R.; Mackean, M.; Nussey, F.; Glasspool, R.; et al. Routine germline BRCA1 and BRCA2 testing in patients with ovarian carcinoma: Analysis of the Scottish real-life experience. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 1451–1458. [Google Scholar] [CrossRef]
- Rahman, B.; Lanceley, A.; Kristeleit, R.S.; Ledermann, J.A.; Lockley, M.; McCormack, M.; Mould, T.; Side, L. Mainstreamed genetic testing for women with ovarian cancer: First-year experience. J. Med. Genet. 2019, 56, 195–198. [Google Scholar] [CrossRef]
- Rumford, M.; Lythgoe, M.; McNeish, I.; Gabra, H.; Tookman, L.; Rahman, N.; George, A.; Krell, J. Oncologist-led BRCA ‘mainstreaming’ in the ovarian cancer clinic: A study of 255 patients and its impact on their management. Sci. Rep. 2020, 10, 3390. [Google Scholar] [CrossRef]
- Flaum, N.; Morgan, R.D.; Burghel, G.J.; Bulman, M.; Clamp, A.R.; Hasan, J.; Mitchell, C.L.; Badea, D.; Moon, S.; Hogg, M.; et al. Mainstreaming germline BRCA1/2 testing in non-mucinous epithelial ovarian cancer in the North West of England. Eur. J. Hum. Genet. 2020, 28, 1541–1547. [Google Scholar] [CrossRef]
- Frugtniet, B.; Morgan, S.; Murray, A.; Palmer-Smith, S.; White, R.; Jones, R.; Hanna, L.; Fuller, C.; Hudson, E.; Mullard, A.; et al. The detection of germline and somatic BRCA1/2 genetic variants through parallel testing of patients with high-grade serous ovarian cancer: A national retrospective audit. BJOG Int. J. Obstet. Gynaecol. 2022, 129, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.; Brady, A.F.; Frayling, I.M.; Hanson, H.; Tischkowitz, M.; Turnbull, C.; Side, L.; UK Cancer Genetics Group (UK-CGG). Consensus for genes to be included on cancer panel tests offered by UK genetics services: Guidelines of the UK Cancer Genetics Group. J. Med. Genet. 2018, 55, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Mandelker, D.; Donoghue, M.; Talukdar, S.; Bandlamudi, C.; Srinivasan, P.; Vivek, M.; Jezdic, S.; Hanson, H.; Snape, K.; Kulkarni, A.; et al. Germline-focussed analysis of tumour-only sequencing: Recommendations from the ESMO Precision Medicine Working Group. Ann. Oncol. 2019, 30, 1221–1231. [Google Scholar] [CrossRef]
- WHO. Female Genital Tumours. WHO Classification of Tumours, 5th ed.International Agency for Research on Cancer: Lyon, France, 2020; Volume 4. [Google Scholar]
- Prat, J.; FIGO Committee on Gynecologic Oncology. Staging classification for cancer of the ovary, fallopian tube, and peritoneum. Int. J. Gynaecol. Obstet. 2014, 124, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.D.; Burghel, G.J.; Flaum, N.; Bulman, M.; Clamp, A.R.; Hasan, J.; Mitchell, C.L.; Schlecht, H.; Woodward, E.R.; Lalloo, F.I.; et al. Prevalence of germline pathogenic BRCA1/2 variants in sequential epithelial ovarian cancer cases. J. Med. Genet. 2019, 56, 301–307. [Google Scholar] [CrossRef]
- Garrett, A.; Durkie, M.; Callaway, A.; Burghel, G.J.; Robinson, R.; Drummond, J.; Torr, B.; Cubuk, C.; Berry, I.R.; Wallace, A.J.; et al. Combining evidence for and against pathogenicity for variants in cancer susceptibility genes: CanVIG-UK consensus recommendations. J. Med. Genet. 2021, 58, 297–304. [Google Scholar] [CrossRef]
- Ellison, G.; Huang, S.; Carr, H.; Wallace, A.; Ahdesmaki, M.; Bhaskar, S.; Mills, J. A reliable method for the detection of BRCA1 and BRCA2 mutations in fixed tumour tissue utilizing multiplex PCR-based targeted next generation sequencing. BMC Clin. Pathol. 2015, 15, 5. [Google Scholar] [CrossRef]
- Telli, M.L.; Timms, K.M.; Reid, J.; Hennessy, B.; Mills, G.B.; Jensen, K.C.; Szallasi, Z.; Barry, W.T.; Winer, E.P.; Tung, N.M.; et al. Homologous Recombination Deficiency (HRD) Score Predicts Response to Platinum-Containing Neoadjuvant Chemotherapy in Patients with Triple-Negative Breast Cancer. Clin. Cancer Res. 2016, 22, 3764–3773. [Google Scholar] [CrossRef]
- Abkevich, V.; Timms, K.M.; Hennessy, B.T.; Potter, J.; Carey, M.S.; Meyer, L.A.; Smith-McCune, K.; Broaddus, R.; Lu, K.H.; Chen, J.; et al. Patterns of genomic loss of heterozygosity predict homologous recombination repair defects in epithelial ovarian cancer. Br. J. Cancer 2012, 107, 1776–1782. [Google Scholar] [CrossRef]
- Birkbak, N.J.; Wang, Z.C.; Kim, J.Y.; Eklund, A.C.; Li, Q.; Tian, R.; Bowman-Colin, C.; Li, Y.; Greene-Colozzi, A.; Iglehart, J.D.; et al. Telomeric allelic imbalance indicates defective DNA repair and sensitivity to DNA-damaging agents. Cancer Discov. 2012, 2, 366–375. [Google Scholar] [CrossRef]
- Popova, T.; Manie, E.; Rieunier, G.; Caux-Moncoutier, V.; Tirapo, C.; Dubois, T.; Delattre, O.; Sigal-Zafrani, B.; Bollet, M.; Longy, M.; et al. Ploidy and large-scale genomic instability consistently identify basal-like breast carcinomas with BRCA1/2 inactivation. Cancer Res. 2012, 72, 5454–5462. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.S.; Rothermundt, C.; Thomas, K.; Bancroft, E.; Eeles, R.; Shanley, S.; Ardern-Jones, A.; Norman, A.; Kaye, S.B.; Gore, M.G. “BRCAness” syndrome in ovarian cancer: A case-control study describing the clinical features and outcome of patients with epithelial ovarian cancer associated with BRCA1 and BRCA2 mutations. J. Clin. Oncol. 2008, 26, 5530–5536. [Google Scholar] [CrossRef] [PubMed]
- Gelmon, K.A.; Tischkowitz, M.; Mackay, H.; Swenerton, K.; Robidoux, A.; Tonkin, K.; Hirte, A.; Huntsman, D.; Clemons, M.; Gilks, B.; et al. Olaparib in patients with recurrent high-grade serous or poorly differentiated ovarian carcinoma or triple-negative breast cancer: A phase 2, multicentre, open-label, non-randomised study. Lancet Oncol. 2011, 12, 852–861. [Google Scholar] [CrossRef] [PubMed]
- Alsop, K.; Fereday, S.; Meldrum, C.; deFazio, A.; Emmanuel, C.; George, J.; Dobrovic, A.; Birrer, M.J.; Webb, P.M.; Stewart, C.; et al. BRCA mutation frequency and patterns of treatment response in BRCA mutation-positive women with ovarian cancer: A report from the Australian Ovarian Cancer Study Group. J. Clin. Oncol. 2012, 30, 2654–2663. [Google Scholar] [CrossRef] [PubMed]
- Ledermann, J.; Harter, P.; Gourley, C.; Friedlander, M.; Vergote, I.; Rustin, G.; Scott, C.L.; Meier, W.; Shapira-Frommer, R.; Safra, T.; et al. Olaparib maintenance therapy in patients with platinum-sensitive relapsed serous ovarian cancer: A preplanned retrospective analysis of outcomes by BRCA status in a randomised phase 2 trial. Lancet Oncol. 2014, 15, 852–861. [Google Scholar] [CrossRef]
- Norquist, B.M.; Brady, M.F.; Harrell, M.I.; Walsh, T.; Lee, M.K.; Gulsuner, S.; Bernards, S.S.; Casadei, S.; Burger, R.A.; Tewari, K.S.; et al. Mutations in Homologous Recombination Genes and Outcomes in Ovarian Carcinoma Patients in GOG 218: An NRG Oncology/Gynecologic Oncology Group Study. Clin. Cancer Res. 2018, 24, 777–783. [Google Scholar] [CrossRef]
- Zhong, Q.; Peng, H.L.; Zhao, X.; Zhang, L.; Hwang, W.T. Effects of BRCA1- and BRCA2-related mutations on ovarian and breast cancer survival: A meta-analysis. Clin. Cancer Res. 2015, 21, 211–220. [Google Scholar] [CrossRef]
- Daly, M.B.; Pal, T.; Berry, M.P.; Buys, S.S.; Dickson, P.; Domchek, S.M.; Elkhanany, A.; Friedman, S.; Goggins, M.; Hutton, M.L.; et al. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 77–102. [Google Scholar] [CrossRef]
- Sessa, C.; Balmana, J.; Bober, S.L.; Cardoso, M.J.; Colombo, N.; Curigliano, G.; Domchek, S.; Evans, D.G.; Fischerova, D.; Harbeck, N.; et al. Risk reduction and screening of cancer in hereditary breast-ovarian cancer syndromes: ESMO Clinical Practice Guideline. Ann. Oncol. 2022; Online ahead of print. [Google Scholar] [CrossRef]
- Witjes, V.M.; van Bommel, M.H.D.; Ligtenberg, M.J.L.; Vos, J.R.; Mourits, M.J.E.; Ausems, M.; de Hullu, J.A.; Bosse, T.; Hoogerbrugge, N. Probability of detecting germline BRCA1/2 pathogenic variants in histological subtypes of ovarian carcinoma. A meta-analysis. Gynecol. Oncol. 2022, 164, 221–230. [Google Scholar] [CrossRef]
- Sun, L.; Sobocan, M.; Rodriguez, I.V.; Wei, X.; Kalra, A.; Oxley, S.; Sideris, M.; Morgan, R.D.; Chandrasekaran, D.; Rust, K.; et al. Cost-effectiveness of unselected multigene germline and somatic genetic testing for epithelial ovarian cancer. Int. J. Gynecol. Cancer 2022, 32, A321–A322. [Google Scholar]
- Cancer Research, UK. Available online: www.cancerresearch.org.uk (accessed on 3 December 2022).
- Kwon, J.S.; Tinker, A.V.; Santos, J.; Compton, K.; Sun, S.; Schrader, K.A.; Karsan, A. Germline testing and somatic tumour testing for BRCA1/2 pathogenic variants in ovarian cancer: What is the optimal sequence testing. JCO Precis Oncol. 2022, 6. [Google Scholar]
- Jang, J.; Kim, Y.; Kim, J.-H.; Cho, S.-M.; Lee, K.A. Cost-effectiveness analysis of germline and somatic BRCA testing in patients with advanced ovarian cancer. Ann. Lab. Med. 2023, 43, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Hauke, J.; Hahnen, E.; Schneider, S.; Reuss, A.; Richters, L.; Kommoss, S.; Heimbach, A.; Marme, F.; Schmidt, S.; Prieske, K.; et al. Deleterious somatic variants in 473 consecutive individuals with ovarian cancer: Results of the observational AGO-TR1 study (NCT02222883). J. Med. Genet. 2019, 56, 574–580. [Google Scholar] [CrossRef]
- Morgan, R.D.; Burghel, G.J.; Flaum, N.; Bulman, M.; Smith, P.; Clamp, A.R.; Hasan, J.; Mitchell, C.L.; Salih, Z.; Woodward, E.R.; et al. BRCA1/2 in non-mucinous epithelial ovarian cancer: Tumour with or without germline testing? Br. J. Cancer 2022, 127, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Kwong, A.; Chen, J.; Shin, V.Y.; Ho, J.C.; Law, F.B.; Au, C.H.; Chan, T.-L.; Ma, E.S.K.; Ford, J.M. The importance of analysis of long-range rearrangement of BRCA1 and BRCA2 in genetic diagnosis of familial breast cancer. Cancer Genet. 2015, 208, 448–454. [Google Scholar] [CrossRef]
- Ray-Coquard, I.; Pautier, P.; Pignata, S.; Perol, D.; Gonzalez-Martin, A.; Berger, R.; Fujiwara, K.; Vergote, I.; Colombo, N.; Maenpaa, J.; et al. Olaparib plus Bevacizumab as First-Line Maintenance in Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2416–2428. [Google Scholar] [CrossRef]
- Mirza, M.R.; Monk, B.J.; Herrstedt, J.; Oza, A.M.; Mahner, S.; Redondo, A.; Fabbro, M.; Ledermann, J.A.; Lorusso, D.; Vergote, I.; et al. Niraparib Maintenance Therapy in Platinum-Sensitive, Recurrent Ovarian Cancer. N. Engl. J. Med. 2016, 375, 2154–2164. [Google Scholar] [CrossRef]
- Coleman, R.L.; Oza, A.M.; Lorusso, D.; Aghajanian, C.; Oaknin, A.; Dean, A.; Colombo, N.; Weberpals, J.I.; Clamp, A.; Scambia, G.; et al. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 1949–1961. [Google Scholar] [CrossRef]
- Gonzalez-Martin, A.; Pothuri, B.; Vergote, I.; DePont Christensen, R.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef]
- Coleman, R.L.; Fleming, G.F.; Brady, M.F.; Swisher, E.M.; Steffensen, K.D.; Friedlander, M.; Okamoto, A.; Moore, K.N.; Ben-Baruch, N.E.; Werner, T.L.; et al. Veliparib with First-Line Chemotherapy and as Maintenance Therapy in Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2403–2415. [Google Scholar] [CrossRef]
- Monk, B.J.; Parkinson, C.; Lim, M.C.; O’Malley, D.M.; Oaknin, A.; Wilson, M.K.; Coleman, R.L.; Lorusso, D.; Bessette, P.; Ghamande, S.; et al. A Randomized, Phase III Trial to Evaluate Rucaparib Monotherapy as Maintenance Treatment in Patients With Newly Diagnosed Ovarian Cancer (ATHENA-MONO/GOG-3020/ENGOT-ov45). J. Clin. Oncol. 2022, 40, 3952–3964. [Google Scholar] [CrossRef] [PubMed]
- Ramus, S.J.; Song, H.; Dicks, E.; Tyrer, J.P.; Rosenthal, A.N.; Intermaggio, M.P.; Fraser, L.; Gentry-Maharaj, A.; Hayward, J.; Philpott, S.; et al. Germline Mutations in the BRIP1, BARD1, PALB2, and NBN Genes in Women With Ovarian Cancer. J. Natl. Cancer Inst. 2015, 107, djv214. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Dicks, E.; Ramus, S.J.; Tyrer, J.P.; Intermaggio, M.P.; Hayward, J.; Edlund, C.K.; Conti, D.; Harrington, P.; Fraser, L.; et al. Contribution of Germline Mutations in the RAD51B, RAD51C, and RAD51D Genes to Ovarian Cancer in the Population. J. Clin. Oncol. 2015, 33, 2901–2907. [Google Scholar] [CrossRef] [PubMed]
- Kurian, A.W.; Ward, K.C.; Howlader, N.; Deapen, D.; Hamilton, A.S.; Mariotto, A.; Miller, D.; Penberthy, L.S.; Katz, S.J. Genetic Testing and Results in a Population-Based Cohort of Breast Cancer Patients and Ovarian Cancer Patients. J. Clin. Oncol. 2019, 37, 1305–1315. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Integrated genomic analyses of ovarian carcinoma. Nature 2011, 474, 609–615. [Google Scholar] [CrossRef]
- Lilyquist, J.; LaDuca, H.; Polley, E.; Davis, B.T.; Shimelis, H.; Hu, C.; Hart, S.N.; Dolinsky, J.S.; Couch, F.J.; Goldgar, D.E. Frequency of mutations in a large series of clinically ascertained ovarian cancer cases tested on multi-gene panels compared to reference controls. Gynecol. Oncol. 2017, 147, 375–380. [Google Scholar] [CrossRef]
- Bernards, S.S.; Pennington, K.P.; Harrell, M.I.; Agnew, K.J.; Garcia, R.L.; Norquist, B.M.; Swisher, E.M. Clinical characteristics and outcomes of patients with BRCA1 or RAD51C methylated versus mutated ovarian carcinoma. Gynecol. Oncol. 2018, 148, 281–285. [Google Scholar] [CrossRef]
- Subramanian, D.N.; Zethoven, M.; McInerny, S.; Morgan, J.A.; Rowley, S.M.; Lee, J.E.A.; Li, N.; Gorringe, K.L.; James, P.A.; Campbell, I.G. Exome sequencing of familial high-grade serous ovarian carcinoma reveals heterogeneity for rare candidate susceptibility genes. Nat. Commun. 2020, 11, 1640. [Google Scholar] [CrossRef]
- Rafnar, T.; Gudbjartsson, D.F.; Sulem, P.; Jonasdottir, A.; Sigurdsson, A.; Jonasdottir, A.; Besenbacher, S.; Lundin, P.; Stacey, S.N.; Gudmundsson, J.; et al. Mutations in BRIP1 confer high risk of ovarian cancer. Nat. Genet. 2011, 43, 1104–1107. [Google Scholar] [CrossRef]
- Hodgson, D.R.; Dougherty, B.A.; Lai, Z.; Fielding, A.; Grinsted, L.; Spencer, S.; O’Connor, M.J.; Ho, T.W.; Robertson, J.D.; Launchbury, J.S.; et al. Candidate biomarkers of PARP inhibitor sensitivity in ovarian cancer beyond the BRCA genes. Br. J. Cancer 2018, 119, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- Mirza, M.R.; Lindahl, G.; Mahner, S.; Redondo, A.; Fabbro, M.; Rimel, B.J.; Herrstedt, J.; Oza, A.M.; Canzier, U.; Berek, J.S.; et al. Ad-hoc analysis of the phase III ENGOT-OV16/NOVA study: Niraparib efficacy in germline BRCA wild-type recurrent ovarian cancer with homologous recombination repair defects. Cancer Res. Commun. 2022, 2, 1462–1470. [Google Scholar] [CrossRef]
- O’Malley, D.M.; Oza, A.M.; Lorusso, D.; Aghajanian, C.; Oaknin, A.; Dean, A.; Colombo, N.; Weberpals, J.I.; Clamp, A.R.; Scambia, G.; et al. Clinical and molecular characteristics of ARIEL3 patients who derived exceptional benefit from rucaparib maintenance treatment for high-grade ovarian carcinoma. Gynecol. Oncol. 2022; Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Swisher, E.M.; Kwan, T.T.; Oza, A.M.; Tinker, A.V.; Ray-Coquard, I.; Oaknin, A.; Coleman, R.L.; Aghajanian, C.; Konecny, G.E.; O’Malley, D.M.; et al. Molecular and clinical determinants of response and resistance to rucaparib for recurrent ovarian cancer treatment in ARIEL2 (Parts 1 and 2). Nat. Commun. 2021, 12, 2487. [Google Scholar] [CrossRef] [PubMed]
- Swisher, E.M.; Kristeleit, R.S.; Oza, A.M.; Tinker, A.V.; Ray-Coquard, I.; Oaknin, A.; Coleman, R.L.; Burris, H.A.; Aghajanian, C.; O’Malley, D.M.; et al. Characterization of patients with long-term responses to rucaparib treatment in recurrent ovarian cancer. Gynecol. Oncol. 2021, 163, 490–497. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Brown, J.; Barnicle, A.; Rowe, P.; Lao-Sirieix, P.; Criscione, S.; du Bois, A.; Lorusso, D.; Romero, I.; Petru, E.; et al. Homologous recombination repair mutation gene panels (excluding BRCA) are not predictive of maintenance olaparib plus bevacizumab efficacy in the first-line PAOLA-1/ENGOT-ov25 trial. Gynecol. Oncol. 2021, 162, S26–S27. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographic | Number of Patients Tested | BRCAm | BRCAwt | |
|---|---|---|---|---|
| Germline | Somatic | |||
| Age at diagnosis—years | 64 (20–92) | 58 (35–80) | 67 (40–92) | 65 (20–89) |
| Histology | ||||
| High-grade serous | 623 (89) | 61 | 49 | 513 |
| High-grade endometrioid | 34 (5) | 2 | 2 | 30 |
| Clear cell | 32 (5) | 4 | 3 | 25 |
| Adenocarcinoma, NOS | 11 (2) | 8 | 0 | 3 |
| Mixed | 2 (<1) | 0 | 0 | 2 |
| Total | 702 | 75 (11) | 54 (8) | 573 |
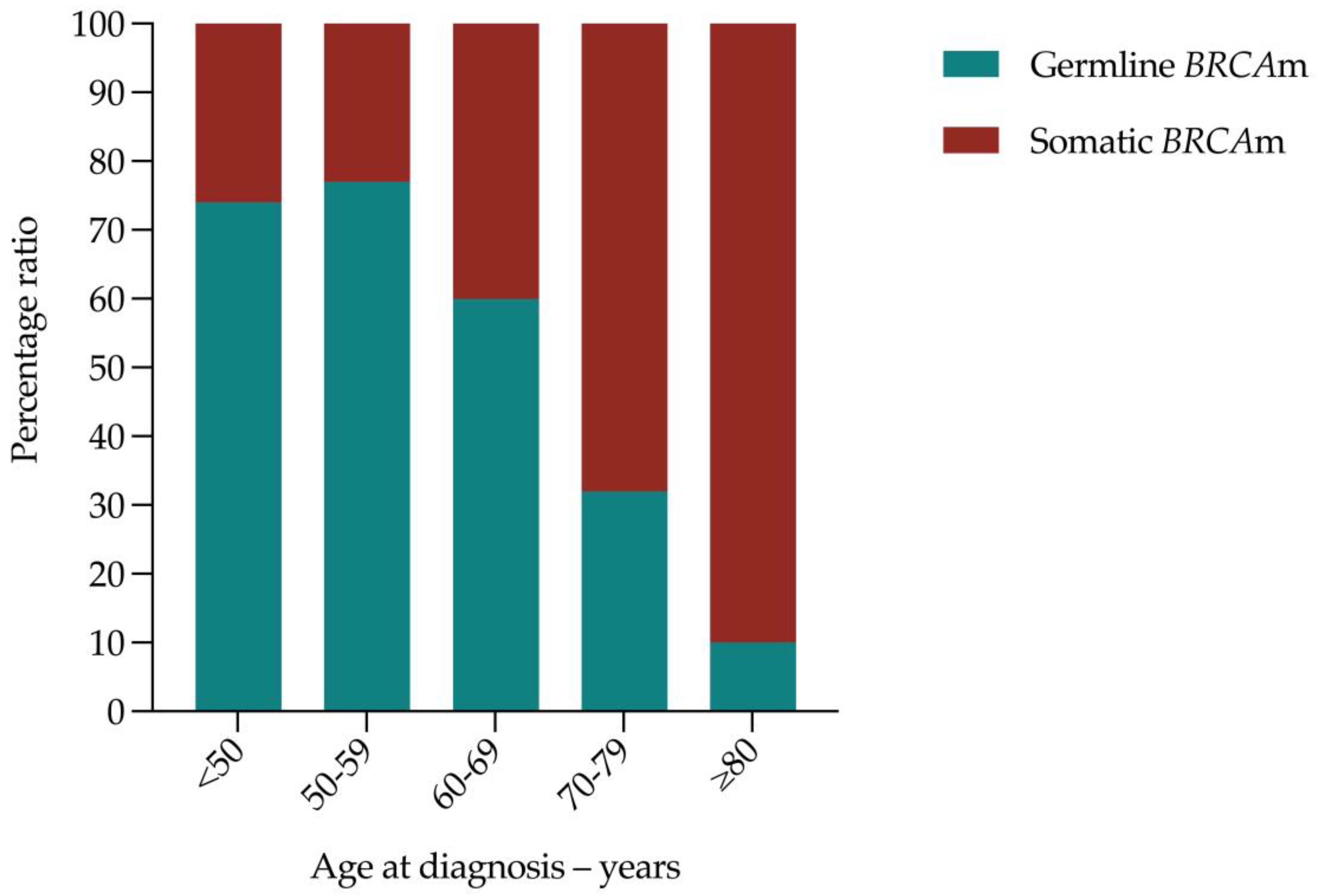
| Age at Diagnosis—Years | Number of Patients Tested | Germline Mutations | Somatic Mutations | % Total Germline to Somatic BRCAm Ratio | ||||
|---|---|---|---|---|---|---|---|---|
| BRCA1 | BRCA2 | Total | BRCA1 | BRCA2 | Total | |||
| <50 | 75 | 12 | 2 | 14 (19) | 4 | 1 | 5 (7) | 19:7 |
| 50–59 | 168 | 18 | 16 | 34 (20) | 7 | 3 | 10 (6) | 10:3 |
| 60–69 | 207 | 5 | 14 | 19 (9) | 9 | 6 | 15 (7) | 9:7 |
| 70–79 | 204 | 1 | 6 | 7 (3) | 7 | 8 | 15 (7) | 3:7 |
| ≥80 | 48 | 0 | 1 | 1 (2) | 3 | 6 | 9 (19) | 1:9 |
| Total | 702 | 36 | 39 | 75 (11) | 30 | 24 | 54 (8) | 11:8 |
| Demographic | Number of Patients Tested | HRD-Negative Tumours | HRD-Positive Tumours | |||
|---|---|---|---|---|---|---|
| BRCAm/GIS+ | BRCAm/GIS- | BRCAwt/GIS+ | Total | |||
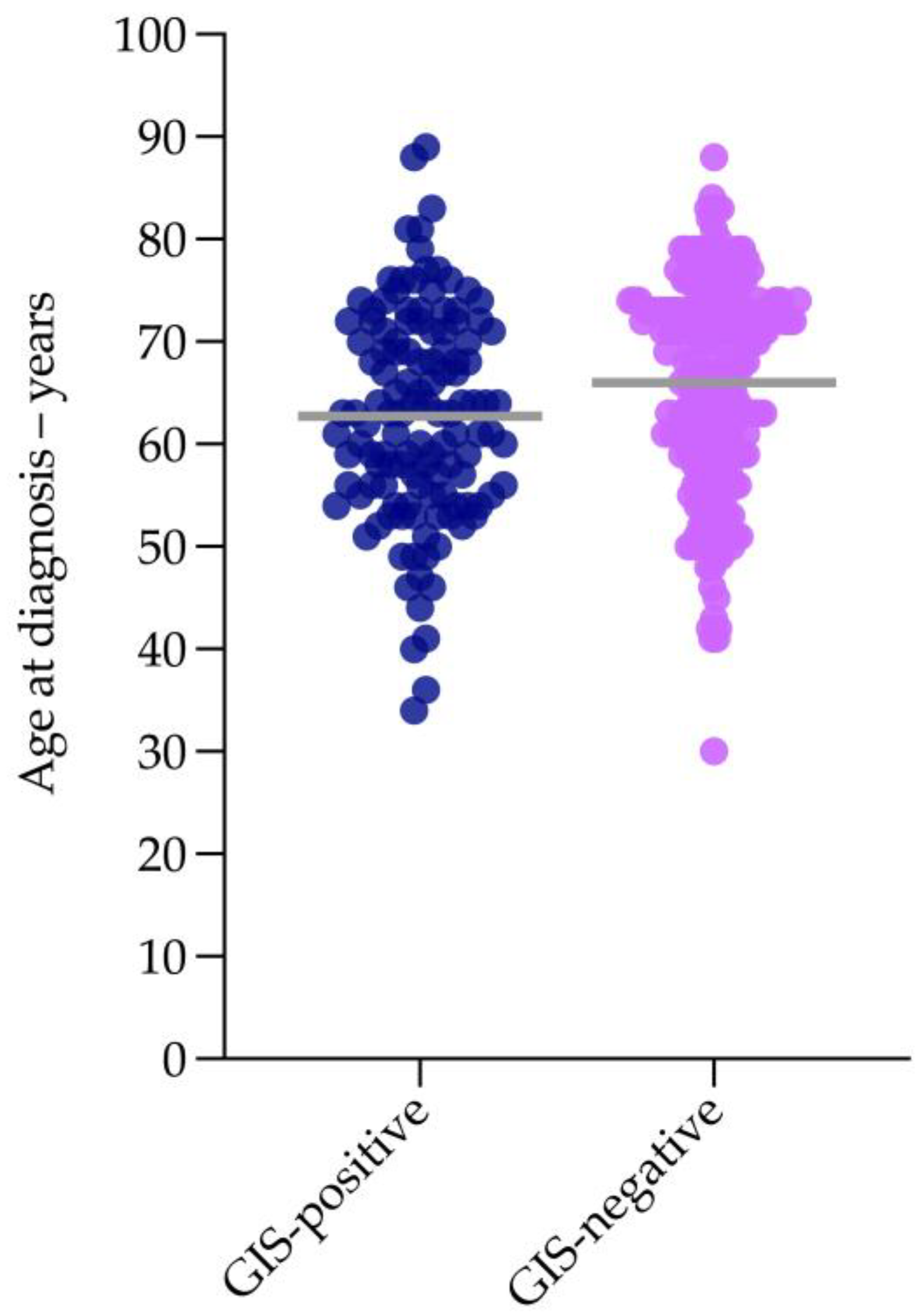
| Age at Diagnosis—Years | 65 (30–89) | 66 (30–88) | 63 (41–88) | 64 (53–75) | 63 (34–89) | 63 (34–89) |
| Histology | ||||||
| High-grade serous | 292 (84) | 183 | 42 | 2 | 65 | 109 |
| High-grade endometrioid | 28 (8) | 18 | 0 | 2 | 8 | 10 |
| Clear cell | 22 (6) | 13 | 5 | 0 | 4 | 9 |
| Adenocarcinoma, NOS | 2 (<1) | 0 | 1 | 0 | 1 | 2 |
| Mixed | 2 (<1) | 2 | 0 | 0 | 0 | 0 |
| Total | 346 | 216 | 48 | 4 | 78 | 130 |
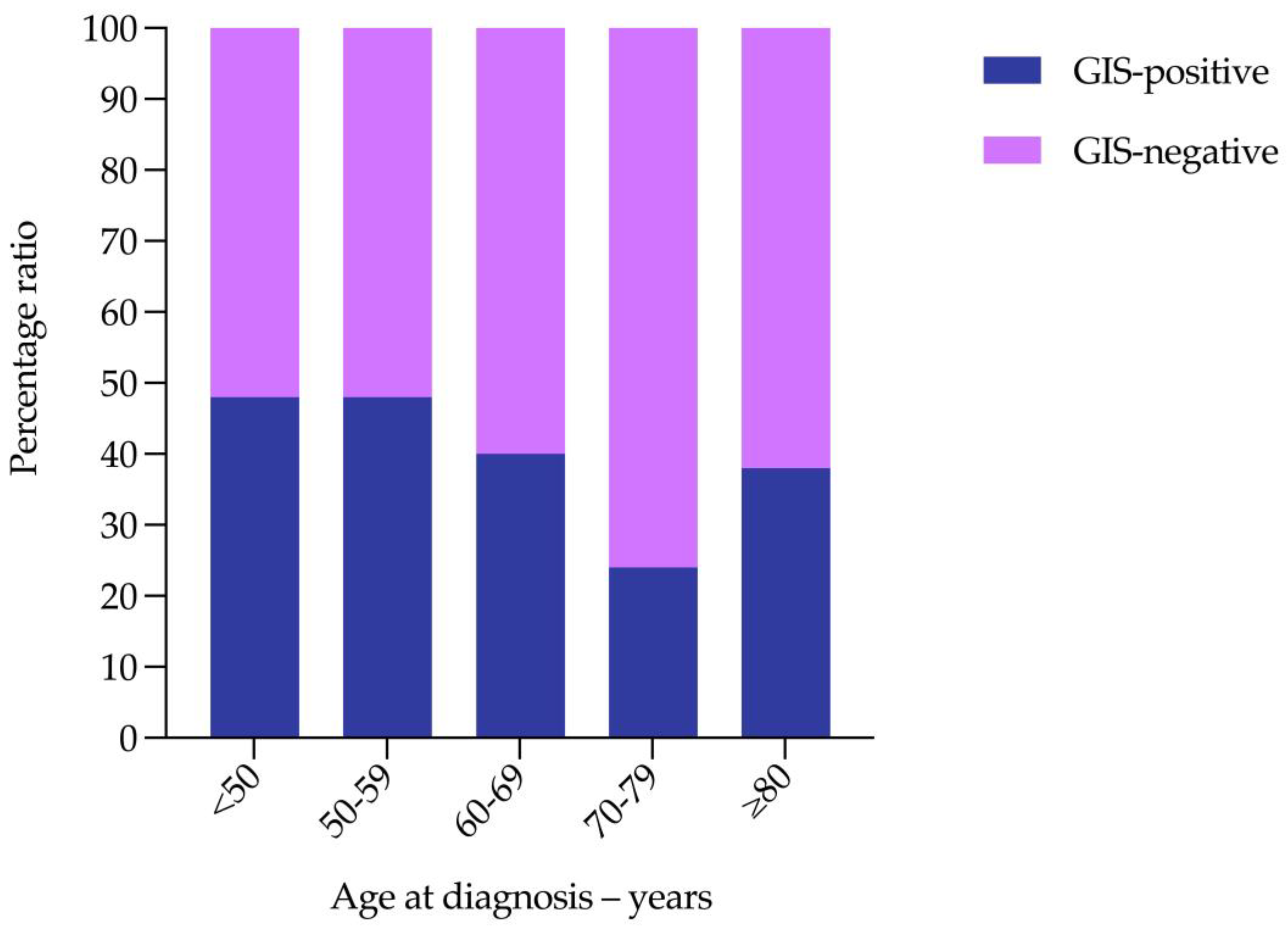
| Age at Diagnosis—Years | Number of Patients Tested | GIS-Positive | GIS-Negative | % Total GIS-Positive to GIS-Negative Ratio | ||||
|---|---|---|---|---|---|---|---|---|
| BRCAm | BRCAwt | Total | BRCAm | BRCAwt | Total | |||
| <50 | 23 | 2 | 9 | 11 (48) | 0 | 12 | 12 (52) | 12:13 |
| 50–59 | 84 | 20 | 20 | 40 (48) | 2 | 42 | 44 (52) | 12:13 |
| 60–69 | 98 | 15 | 24 | 39 (40) | 0 | 59 | 59 (60) | 2:3 |
| 70–79 | 128 | 8 | 23 | 31 (24) | 2 | 95 | 97 (76) | 6:19 |
| ≥80 | 13 | 3 | 2 | 5 (38) | 0 | 8 | 8 (62) | 19:31 |
| Total | 346 | 48 | 78 | 126 (36) | 4 | 216 | 220 (64) | 9:16 |
| GIS Status | Number of Patients Tested | Germline | Somatic | BRCAwt | Germline Non-BRCA1/2 HRRm | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| BRCA1 | BRCA2 | BRCA1 | BRCA2 | BRIP1 | PALB2 | RAD51C | RAD51D | |||
| GIS-positive | 86 | 14 | 16 | 12 | 9 | 35 | 2 | 0 | 0 | 0 |
| GIS-negative | 88 | 0 | 1 a | 1 b | 2 c | 84 | 2 | 0 | 0 | 0 |
| Total | 174 | 14 | 17 | 13 | 11 | 119 | 4 (3) | 0 | 0 | 0 |
| BRIP1 Variant | Age at Diagnosis—Years | Histology | FIGO Stage | Family History | BRCAm | GIS | HRD status | ||
|---|---|---|---|---|---|---|---|---|---|
| Nucleotide Level | Protein Level | Germline | Tumour | ||||||
| c.1888dup | (p.Thr630fs) | 68 | HGSOC | IIIC | 1 × FDR Breast Cancer | WT | WT | 40 | Negative |
| c.2108delinsTCC | (p.Lys703fs) | 68 | HGSOC | IIIC | 1 × FDR Ovarian Cancer | WT | WT | 49 | Positive |
| c.2392C>T | (p.Arg798Ter) | 59 | HGSOC | IVB | 1 × SDR Breast Cancer | WT | WT | 57 | Positive |
| c.2492+2dup | p.(?) | 60 | HGSOC | IVA | 3 × FDR Breast Cancer | WT | WT | 41 | Negative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morgan, R.D.; Burghel, G.J.; Flaum, N.; Bulman, M.; Smith, P.; Clamp, A.R.; Hasan, J.; Mitchell, C.L.; Salih, Z.; Woodward, E.R.; et al. Is Reflex Germline BRCA1/2 Testing Necessary in Women Diagnosed with Non-Mucinous High-Grade Epithelial Ovarian Cancer Aged 80 Years or Older? Cancers 2023, 15, 730. https://doi.org/10.3390/cancers15030730
Morgan RD, Burghel GJ, Flaum N, Bulman M, Smith P, Clamp AR, Hasan J, Mitchell CL, Salih Z, Woodward ER, et al. Is Reflex Germline BRCA1/2 Testing Necessary in Women Diagnosed with Non-Mucinous High-Grade Epithelial Ovarian Cancer Aged 80 Years or Older? Cancers. 2023; 15(3):730. https://doi.org/10.3390/cancers15030730
Chicago/Turabian StyleMorgan, Robert D., George J. Burghel, Nicola Flaum, Michael Bulman, Philip Smith, Andrew R. Clamp, Jurjees Hasan, Claire L. Mitchell, Zena Salih, Emma R. Woodward, and et al. 2023. "Is Reflex Germline BRCA1/2 Testing Necessary in Women Diagnosed with Non-Mucinous High-Grade Epithelial Ovarian Cancer Aged 80 Years or Older?" Cancers 15, no. 3: 730. https://doi.org/10.3390/cancers15030730
APA StyleMorgan, R. D., Burghel, G. J., Flaum, N., Bulman, M., Smith, P., Clamp, A. R., Hasan, J., Mitchell, C. L., Salih, Z., Woodward, E. R., Lalloo, F., Crosbie, E. J., Edmondson, R. J., Schlecht, H., Jayson, G. C., & Evans, D. G. R. (2023). Is Reflex Germline BRCA1/2 Testing Necessary in Women Diagnosed with Non-Mucinous High-Grade Epithelial Ovarian Cancer Aged 80 Years or Older? Cancers, 15(3), 730. https://doi.org/10.3390/cancers15030730