
A Suggested Modification to FIGO Stage IV Epithelial Ovarian Cancer

 , ,
, ,  , , , ,
, , , ,  , , add
Show full author list
, , add
Show full author list
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
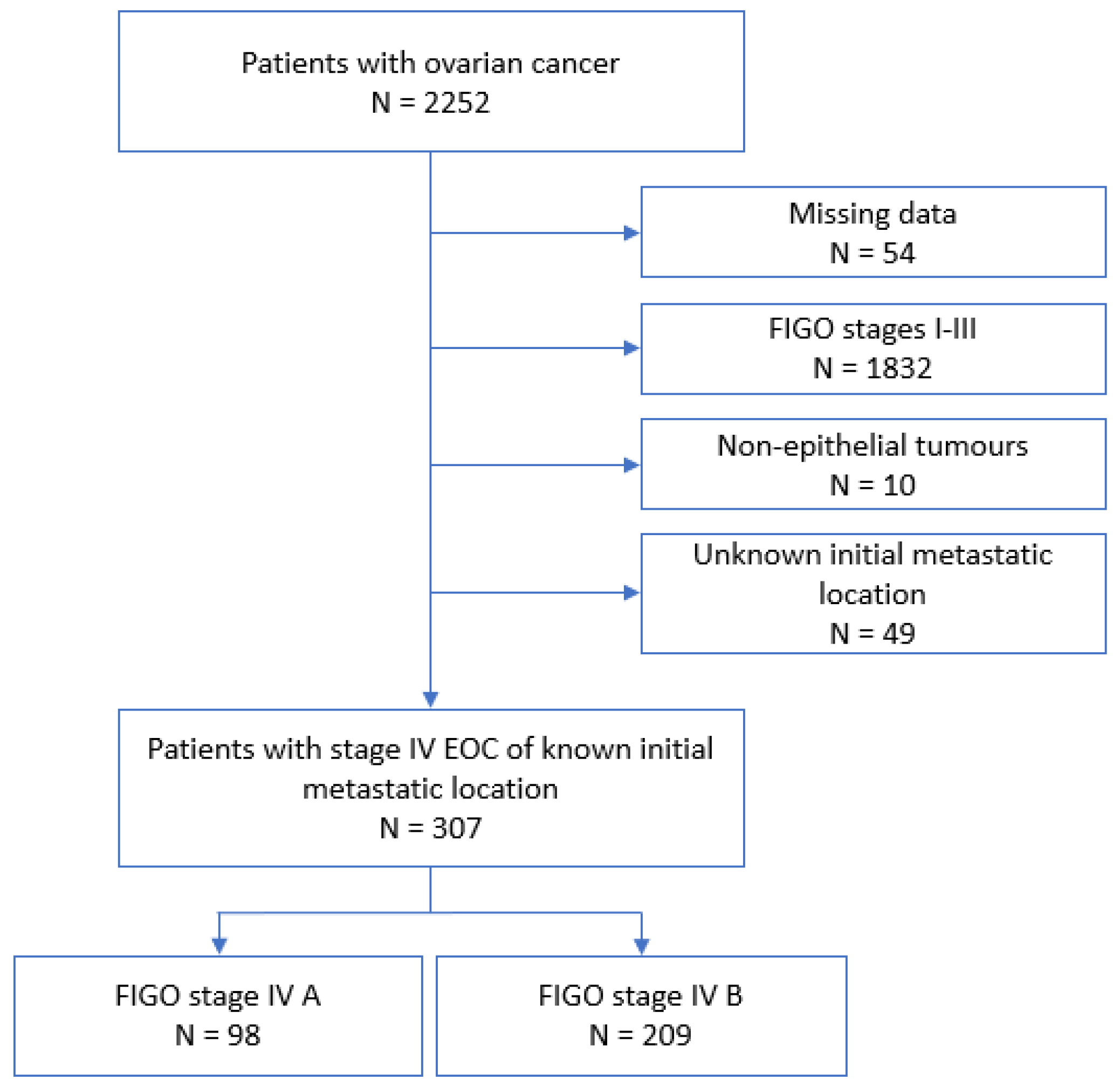
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Care Management
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Descriptive Analysis of the Population
3.2. Descriptive Analysis of the Treatment Regimen
3.3. Descriptive Analysis of Surgery for Operated Patients
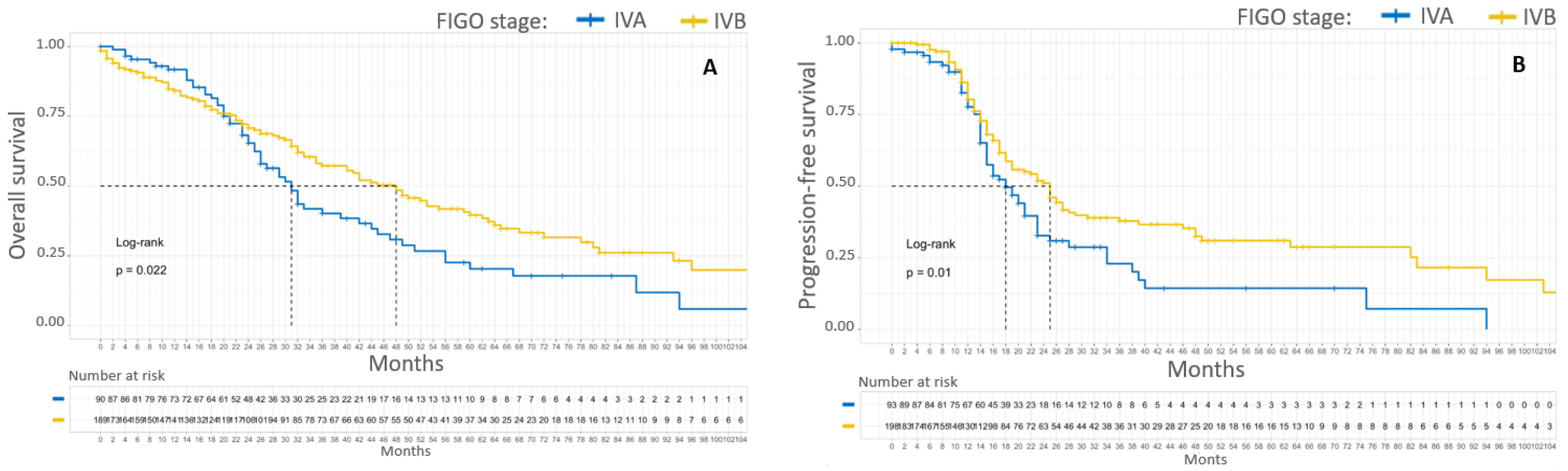
3.4. Survival Analysis by FIGO Stage
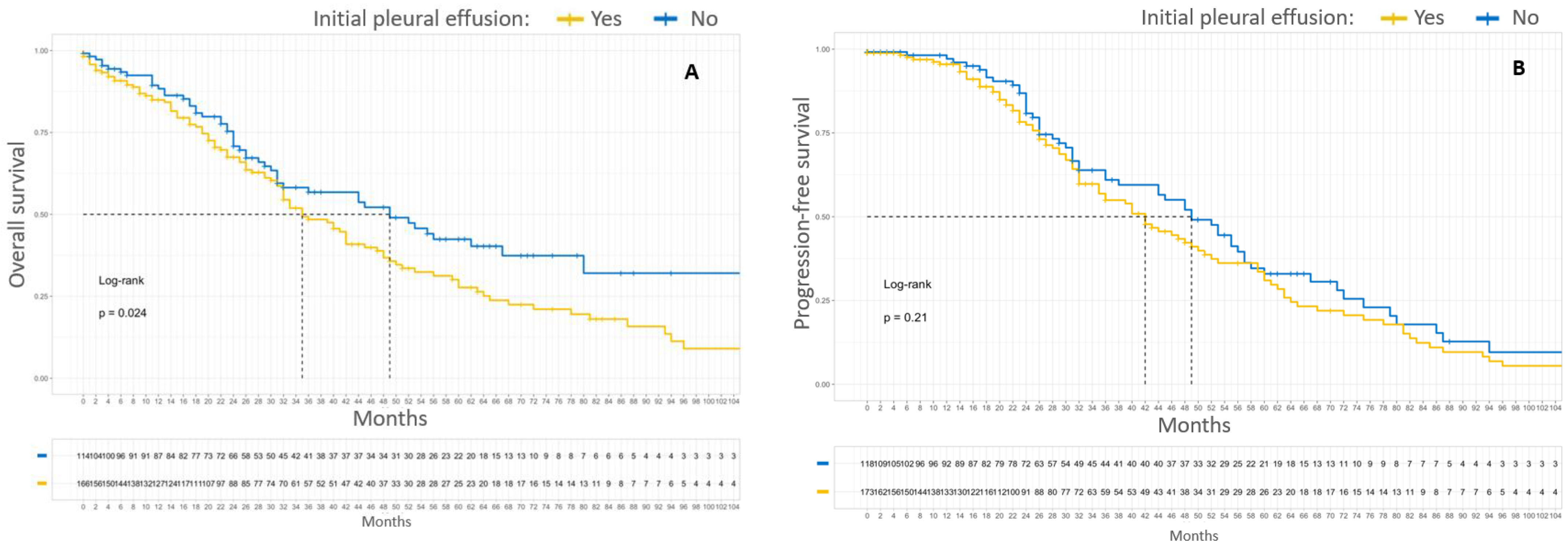
3.5. Survival Analysis by Initial Metastatic Location
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mutch, D.G.; Prat, J. 2014 FIGO Staging for Ovarian, Fallopian Tube and Peritoneal Cancer. Gynecol. Oncol. 2014, 133, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Berek, J.S.; Kehoe, S.T.; Kumar, L.; Friedlander, M. Cancer of the Ovary, Fallopian Tube, and Peritoneum. Int. J. Gynecol. Obstet. 2018, 143, 59–78. [Google Scholar] [CrossRef] [PubMed]
- Deng, K.; Yang, C.; Tan, Q.; Song, W.; Lu, M.; Zhao, W.; Lou, G.; Li, Z.; Li, K.; Hou, Y. Sites of Distant Metastases and Overall Survival in Ovarian Cancer: A Study of 1481 Patients. Gynecol. Oncol. 2018, 150, 460–465. [Google Scholar] [CrossRef]
- For the Groupe de Recherche FRANCOGYN; Dabi, Y.; Huchon, C.; Ouldamer, L.; Bendifallah, S.; Collinet, P.; Bricou, A.; Daraï, E.; Ballester, M.; Lavoue, V.; et al. Patients with Stage IV Epithelial Ovarian Cancer: Understanding the Determinants of Survival. J. Transl. Med. 2020, 18, 134. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, A.; Sykes, P.; Eva, L.; Bergzoll, C.; Simcock, B. Subtypes of Stage IV Ovarian Cancer; Response to Treatment and Patterns of Disease Recurrence. Gynecol. Oncol. 2017, 146, 273–278. [Google Scholar] [CrossRef]
- Rosendahl, M.; Høgdall, C.K.; Mosgaard, B.J. Restaging and Survival Analysis of 4036 Ovarian Cancer Patients According to the 2013 FIGO Classification for Ovarian, Fallopian Tube, and Primary Peritoneal Cancer. Int. J. Gynecol. Cancer 2016, 26, 680–687. [Google Scholar] [CrossRef]
- Ataseven, B.; Harter, P.; Grimm, C.; Heitz, F.; Heikaus, S.; Traut, A.; Kahl, A.; Kurzeder, C.; Prader, S.; du Bois, A. The Revised 2014 FIGO Staging System for Epithelial Ovarian Cancer: Is a Subclassification into FIGO Stage IVA and IVB Justified? Gynecol. Oncol. 2016, 142, 243–247. [Google Scholar] [CrossRef]
- Feng, Z.; Wen, H.; Ju, X.; Bi, R.; Chen, X.; Yang, W.; Wu, X. Metastatic Patterns Do Not Provide Additional Prognostic Information for Patients with FIGO Stage IV High-grade Serous Ovarian Cancer. J. Surg. Oncol. 2020, 122, 315–319. [Google Scholar] [CrossRef]
- Tajik, P.; van de Vrie, R.; Zafarmand, M.H.; Coens, C.; Buist, M.R.; Vergote, I.; Bossuyt, P.M.M.; Kenter, G.G. The FIGO Stage IVA Versus IVB of Ovarian Cancer: Prognostic Value and Predictive Value for Neoadjuvant Chemotherapy. Int. J. Gynecol. Cancer 2018, 28, 453–458. [Google Scholar] [CrossRef]
- Hjerpe, E.; Staf, C.; Dahm-Kähler, P.; Stålberg, K.; Bjurberg, M.; Holmberg, E.; Borgfeldt, C.; Tholander, B.; Hellman, K.; Kjølhede, P.; et al. Lymph Node Metastases as Only Qualifier for Stage IV Serous Ovarian Cancer Confers Longer Survival than Other Sites of Distant Disease – a Swedish Gynecologic Cancer Group (SweGCG) Study. Acta Oncol. 2018, 57, 331–337. [Google Scholar] [CrossRef]
- Dabi, Y.; Thubert, T.; Fuchs, F.; Barjat, T.; Belaisch–Allart, J.; Ceccaldi, P.F. How Is Functionning the Ethical Review Board «Comité d’Ethique Pour La Recherche En Obstétrique Et Gynécologie» (CEROG)? J. Gynecol. Obstet. Hum. Reprod. 2022, 51, 102352. [Google Scholar] [CrossRef]
- Dvoretsky, P.M.; Richards, K.A.; Angel, C.; Rabinowitz, L.; Stoler, M.H.; Beecham, J.B.; Bonfiglio, T.A. Distribution of Disease at Autopsy in 100 Women with Ovarian Cancer. Hum. Pathol. 1988, 19, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Raban, O.; Peled, Y.; Krissi, H.; Goldberg, N.; Aviram, A.; Sabah, G.; Levavi, H.; Eitan, R. The Significance of Paracardiac Lymph-Node Enlargement in Patients with Newly Diagnosed Stage IIIC Ovarian Cancer. Gynecol. Oncol. 2015, 138, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Chen, V.W.; Ruiz, B.; Killeen, J.L.; Coté, T.R.; Wu, X.C.; Correa, C.N.; Howe, H.L. Pathology and Classification of Ovarian Tumors. Cancer 2003, 97, 2631–2642. [Google Scholar] [CrossRef] [PubMed]
- Fagotti, A.; Ferrandina, G.; Fanfani, F.; Garganese, G.; Vizzielli, G.; Carone, V.; Salerno, M.G.; Scambia, G. Prospective Validation of a Laparoscopic Predictive Model for Optimal Cytoreduction in Advanced Ovarian Carcinoma. Am. J. Obstet. Gynecol. 2008, 199, 642.e1–642.e6. [Google Scholar] [CrossRef] [PubMed]
- Fagotti, A.; Ferrandina, G.; Fanfani, F.; Ercoli, A.; Lorusso, D.; Rossi, M.; Scambia, G. A Laparoscopy-Based Score To Predict Surgical Outcome in Patients With Advanced Ovarian Carcinoma: A Pilot Study. Ann. Surg. Oncol. 2006, 13, 1156–1161. [Google Scholar] [CrossRef]
- Colombo, N.; Sessa, C.; du Bois, A.; Ledermann, J.; McCluggage, W.G.; McNeish, I.; Morice, P.; Pignata, S.; Ray-Coquard, I.; Vergote, I.; et al. ESMO–ESGO Consensus Conference Recommendations on Ovarian Cancer: Pathology and Molecular Biology, Early and Advanced Stages, Borderline Tumours and Recurrent Disease. Ann. Oncol. 2019, 30, 672–705. [Google Scholar] [CrossRef]
- du Bois, A.; Quinn, M.; Thigpen, T.; Vermorken, J.; Avall-Lundqvist, E.; Bookman, M.; Bowtell, D.; Brady, M.; Casado, A.; Cervantes, A.; et al. 2004 Consensus Statements on the Management of Ovarian Cancer: Final Document of the 3rd International Gynecologic Cancer Intergroup Ovarian Cancer Consensus Conference (GCIG OCCC 2004). Ann. Oncol. 2005, 16, viii7–viii12. [Google Scholar] [CrossRef]
- Joly, F.; Ray-Coquard, I. Mise à jour 2021 des recommandations pour la pratique clinique de Nice/Saint-Paul-de-Vence dans le cancer de l’ovaire épithélial de haut grade. Bull. Cancer 2021, 108, S1–S4. [Google Scholar] [CrossRef]
- Timmermans, M.; van der Hel, O.; Sonke, G.S.; Van de Vijver, K.K.; van der Aa, M.A.; Kruitwagen, R.F. The Prognostic Value of Residual Disease after Neoadjuvant Chemotherapy in Advanced Ovarian Cancer; A Systematic Review. Gynecol. Oncol. 2019, 153, 445–451. [Google Scholar] [CrossRef]
- Bristow, R.E.; Montz, F.J.; Lagasse, L.D.; Leuchter, R.S.; Karlan, B.Y. Survival Impact of Surgical Cytoreduction in Stage IV Epithelial Ovarian Cancer. Gynecol. Oncol. 1999, 72, 278–287. [Google Scholar] [CrossRef] [PubMed]
- Wimberger, P.; Wehling, M.; Lehmann, N.; Kimmig, R.; Schmalfeldt, B.; Burges, A.; Harter, P.; Pfisterer, J.; du Bois, A. Influence of Residual Tumor on Outcome in Ovarian Cancer Patients With FIGO Stage IV Disease: An Exploratory Analysis of the AGO-OVAR (Arbeitsgemeinschaft Gynaekologische Onkologie Ovarian Cancer Study Group). Ann. Surg. Oncol. 2010, 17, 1642–1648. [Google Scholar] [CrossRef] [PubMed]
- Ataseven, B.; Grimm, C.; Harter, P.; Heitz, F.; Traut, A.; Prader, S.; du Bois, A. Prognostic Impact of Debulking Surgery and Residual Tumor in Patients with Epithelial Ovarian Cancer FIGO Stage IV. Gynecol. Oncol. 2016, 140, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Sanabria, J.R.; Strasberg, S.M. Proposed Classification of Complications of Surgery with Examples of Utility in Cholecystectomy. Surgery 1992, 111, 518–526. [Google Scholar] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A New Proposal With Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Paik, E.S.; Lee, Y.-Y.; Lee, E.-J.; Choi, C.H.; Kim, T.-J.; Lee, J.-W.; Bae, D.-S.; Kim, B.-G. Survival Analysis of Revised 2013 FIGO Staging Classification of Epithelial Ovarian Cancer and Comparison with Previous FIGO Staging Classification. Obstet. Gynecol. Sci. 2015, 58, 124. [Google Scholar] [CrossRef]
- Toptas, T.; Pestereli, E.; Erol, O.; Bozkurt, S.; Erdogan, G.; Simsek, T. Validation of Revised FIGO Staging Classification for Cancer of the Ovary, Fallopian Tube, and Peritoneum Based on a Single Histological Type. Int. J. Gynecol. Cancer 2016, 26, 1012–1019. [Google Scholar] [CrossRef]
- Mert, I.; Kumar, A.; Torres, D.; Huang, Y.; McGree, M.E.; Weaver, A.L.; Cliby, W.A. Should Mucosal Bowel Invasion in Ovarian Cancer Be Assigned to FIGO Stage IV Disease? Gynecol. Oncol. 2019, 153, 238–241. [Google Scholar] [CrossRef]
- Ataseven, B.; du Bois, A.; Harter, P.; Prader, S.; Grimm, C.; Kurzeder, C.; Schneider, S.; Heikaus, S.; Kahl, A.; Traut, A.; et al. Impact of Abdominal Wall Metastases on Prognosis in Epithelial Ovarian Cancer. Int. J. Gynecol. Cancer 2016, 26, 1594–1600. [Google Scholar] [CrossRef]
- Nasioudis, D.; Chapman-Davis, E.; Frey, M.K.; Caputo, T.A.; Witkin, S.S.; Holcomb, K. Should Epithelial Ovarian Carcinoma Metastatic to the Inguinal Lymph Nodes Be Assigned Stage IVB? Gynecol. Oncol. 2017, 147, 81–84. [Google Scholar] [CrossRef]
- Perri, T.; Ben-Baruch, G.; Kalfon, S.; Beiner, M.E.; Helpman, L.; Hogen, L.B.-D.; Shapira-Frommer, R.; Korach, J. Abdominopelvic Cytoreduction Rates and Recurrence Sites in Stage IV Ovarian Cancer: Is There a Case for Thoracic Cytoreduction? Gynecol. Oncol. 2013, 131, 27–31. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FIGO Stage IVA N = 98 | FIGO Stage IVB N = 209 | p-Value | |
|---|---|---|---|
| Age at diagnosis (years) Mean ± SD Median (rank) | 0.03 | ||
| 65.2 ± 9.9 | 62.3 ± 11.9 | ||
| 66.0 (41.0–86.0) | 62.0 (34.0–89.0) | ||
| Menopause N (%) HRT N (%) | 93/95 (97.9) | 171/202 (84.7) | <0.005 |
| 14/71 (19.7) | 25/135 (18.5) | 0.98 | |
| ASA score N (%) 1 | 0.76 | ||
| 24 (24.5) | 62 (29.7) | ||
| 2 3 | 25 (25.5) | 53 (25.4) | |
| 18 (18.4) | 31 (14.8) | ||
| 4 | 1 (1.0) | 2 (1.0) | |
| NA | 30 (30.6) | 61 (29.1) | |
| Mutation N (%) | 1 | ||
| BRCA1 | 7 (7.1) | 12 (5.7) | |
| BRCA2 | 3 (3.1) | 13 (6.2) | |
| Not sought | 54 (55.1) | 95 (45.5) | |
| Non-mutated | 34 (34.7) | 89 (42.6) | |
| Personal history N (%) | |||
| Pelvic cancer | 3/64 (4.7) | 3/189 (1.6) | 0.35 |
| Breast cancer | 2/67 (3.0) | 10/196 (5.1) | 0.71 |
| Hysterectomy | 3/67 (4.5) | 12/194 (6.2) | 0.83 |
| Ovarian surgery | 3/64 (4.7) | 7/188 (3.7) | 1 |
| Family history N (%) | |||
| Gynaecological cancer | 21/79 (26.6) | 64/182 (35.2) | 0.22 |
| Other cancers | 10/60 (16.7) | 47/175 (26.9) | 0.16 |
| Discovery mode N (%) | |||
| Imagery | 3/72 (4.2) | 12/136 (8.8) | 0.34 |
| Abdominal symptomatology a | 43/72 (59.7) | 78/136 (57.4) | 0.86 |
| Extra-abdominal symptomatology b | 41/72 (56.9) | 69/136 (50.7) | 0.48 |
| Histology N (%) | 0.57 | ||
| Serous | 79 (80.6) | 169 (80.9) | |
| High grade | 59/65 (90.8) | 133/141 (94.3) | |
| Low grade | 6/65 (9.2) | 8/141 (5.7) | |
| Mucinous | 3 (3.1) | 1 (0.5) | |
| Endometrioid | 3 (3.1) | 10 (4.8) | |
| Clear cells | 2 (2.0) | 6 (2.9) | |
| Other c | 5 (5.1) | 16 (7.6) | |
| NA | 6 (6.1) | 7 (3.3) | |
| Initial metastatic site N (%) | <0.001 | ||
| Pleural | 98 (100) | 124 (59.3) | 0.04 |
| Parenchymal | 0 (0) | 102/202 (50.5) | <0.001 |
| Intra-hepatic | 0 (0) | 73/202 (36.1) | <0.001 |
| Other d | 0 (0) | 43/202 (21.3) | <0.001 |
| Lymph node | 0 (0) | 138/202 (68.3) | <0.001 |
| Supra-diaphragmatic | 0 (0) | 131/202 (64.9) | <0.001 |
| Inguinal | 0 (0) | 10/202 (5.0) | 0.06 |
| CA 125 at diagnosis (U/mL) | 0.14 | ||
| ≤500 N (%) | 19/96 (19.8) | 58/203 (28.6) | |
| >500 N (%) | 77/96 (80.2) | 145/203 (71.4) |
| FIGO IVA N = 98 | FIGO IVB N = 209 | p-Value | |
|---|---|---|---|
| Treatment regimen N (%) CTA PCS | 0.07 | ||
| 20 (20.4) | 56 (26.8) | ||
| 11 (11.2) | 37/205 (17.7) | ||
| NACT-IS | 67 (68.4) | 112/205 (53.9) | |
| Chemotherapy N (%) | |||
| Neoadjuvant Number of NACT: Mean ± SD | 87 (88.8) | 112 (53.6) | 0.10 |
| 5.1 ± 1.9 | 4.9 ± 1.7 | 0.37 | |
| Adjuvant Number of ACT: Mean ± SD | 1 | ||
| 2.8 ± 2.2 | 3.4 ± 2.8 | 0.55 | |
| Platinum sensitivity | 0.21 | ||
| Low | 27/68 (39.7) | 71/138 (51.4) | |
| Intermediate | 19/68 (27.9) | 36/138 (26.1) | |
| High | 22/68 (32.4) | 31/138 (22.5) | |
| Bevacizumab N (%) | 33/76 (43.4) | 80/159 (50.3) | 0.40 |
| Recurrence N (%) | 62/95 (65.3) | 99/209 (47.4) | 0.004 |
| CA-125 at relapse (U/mL) | 0.65 | ||
| Mean ± SD | 278.1 ± 692.5 | 217.6 ± 424.2 | |
| Median (rank) | 103 (5–4000) | 87 (5–2864) | |
| Chemotherapy at relapse | 45/95 (47.4) | 86/87 (98.9) | 0.60 |
| Surgery at relapse | 4/35 (11.4) | 13/65 (19.1) | 0.47 |
| Number of relapse | 0.96 | ||
| Mean ± SD | 0.86 ± 1.47 | 0.87 ± 1.4 | |
| Median (rank) | 0 (0–8) | 0 (0–6) | |
| Overall survival (months) | |||
| Mean ± SD | 29.2 ± 22.0 | 33.9 ± 28.0 | 0.15 |
| Median (rank) | 31.0 (1–106) | 48.0 (0–125) | 0.02 |
| Progression-free survival (months) | |||
| Mean ± SD | 18.5± 14.8 | 22.5 ± 22.3 | 0.66 |
| Median (rank) | 18 (0–94) | 25.0 (0–115) | 0.01 |
| FIGO IVA N = 78 | FIGO IVB N = 149 | p-Value | |
|---|---|---|---|
| PCI Initial PCI Mean ± SD | |||
| 0.03 | |||
| 20.4 ± 10.7 | 15.4 ± 9.5 | ||
| Median (rank) | 25.0 (0–31) | 14.0 (0–32) | |
| Operating time (minutes) | |||
| Mean ± SD Median (rank) | 350 ± 177.2 | 401.1 ± 199.4 | 0.69 |
| 330 (120–645) | 345 (120–690) | ||
| Digestive resection N (%) | 7/74 (9.5) | 48/143 (33.6) | <0.001 |
| Supra-mesocolic surgery a N (%) | |||
| Splenectomy | 6/63 (9.5) | 14/125 (11.2) | 0.92 |
| Cholecystectomy | 2/58 (3.4) | 5/119 (4.2) | 1 |
| Liver resection | 1/53 (1.9) | 9/119 (7.6) | 0.35 |
| Diaphragmatic dome resection | 25/74 (33.8) | 65/144 (45.1) | 0.13 |
| Lymphadenectomy N (%) | 32/74 (43.2) | 91/146 (62.3) | 0.01 |
| Urinary surgical procedure b N (%) | 1/70 (1.4) | 1/143 (0.7) | 1 |
| Intra-operative complication N (%) | 14/71 (19.7) | 53/138 (38.4) | 0.01 |
| Urinary or digestive | 1/71 (1.4) | 14/138 (10.1) | 0.24 |
| Vascular injury or hemorrhagic complication c | 14/71 (19.7) | 38/138 (27.5) | 1 |
| Pleural injury | 1/71 (1.4) | 10/138 (7.2) | 0.52 |
| Other d | 2/71 (2.8) | 4/138 (2.9) | 0.80 |
| Postoperative residual disease N (%) | 0.03 | ||
| Complete resection | 36/72 (50) | 108/142 (76.1) | |
| Residual disease < 10 mm | 10/72 (13.9) | 12/142 (8.5) | |
| Residual disease ≥ 10 mm | 26/72 (36.1) | 22/142 (15.4) | |
| Postoperative complication according to the Clavien–Dindo classification N (%) | 0.05 | ||
| 0 | 58/73 (79.5) | 91/138 (65.9) | |
| 1 | 0/73 (0) | 9/138 (6.5) | |
| 2 | 9/73 (12.3) | 14/138 (10.2) | |
| 3A | 4/73 (5.5) | 8/138 (5.8) | |
| 3B | 1/73 (1.4) | 9/138 (6.6) | |
| 4A | 0/73 (0) | 4/138 (2.9) | |
| 4B | 0/73 (0) | 2/138 (1.4) | |
| 5 | 1/73 (1.4) | 1/138 (0.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Métairie, M.; Benoit, L.; Koual, M.; Bentivegna, E.; Wohrer, H.; Bolze, P.-A.; Kerbage, Y.; Raimond, E.; Akladios, C.; Carcopino, X.; et al. A Suggested Modification to FIGO Stage IV Epithelial Ovarian Cancer. Cancers 2023, 15, 706. https://doi.org/10.3390/cancers15030706
Métairie M, Benoit L, Koual M, Bentivegna E, Wohrer H, Bolze P-A, Kerbage Y, Raimond E, Akladios C, Carcopino X, et al. A Suggested Modification to FIGO Stage IV Epithelial Ovarian Cancer. Cancers. 2023; 15(3):706. https://doi.org/10.3390/cancers15030706
Chicago/Turabian StyleMétairie, Marie, Louise Benoit, Meriem Koual, Enrica Bentivegna, Henri Wohrer, Pierre-Adrien Bolze, Yohan Kerbage, Emilie Raimond, Cherif Akladios, Xavier Carcopino, and et al. 2023. "A Suggested Modification to FIGO Stage IV Epithelial Ovarian Cancer" Cancers 15, no. 3: 706. https://doi.org/10.3390/cancers15030706
APA StyleMétairie, M., Benoit, L., Koual, M., Bentivegna, E., Wohrer, H., Bolze, P.-A., Kerbage, Y., Raimond, E., Akladios, C., Carcopino, X., Canlorbe, G., Uzan, J., Lavoué, V., Mimoun, C., Huchon, C., Koskas, M., Costaz, H., Margueritte, F., Dabi, Y., ... Azaïs, H. (2023). A Suggested Modification to FIGO Stage IV Epithelial Ovarian Cancer. Cancers, 15(3), 706. https://doi.org/10.3390/cancers15030706