

IGF1 and Insulin Receptor Single Nucleotide Variants Associated with Response in HER2-Negative Breast Cancer Patients Treated with Neoadjuvant Chemotherapy with or without a Fasting Mimicking Diet (BOOG 2013-04 DIRECT Trial)

 ,
,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. IGF1R and INSR SNV Distribution
3.2. IGF1 Receptor SNVs Are Associated with Worsened Pathological Response and INSR SNV Is Potentially Associated with Worse Radiological Response
3.3. IGF1R SNVs and FMD Interaction
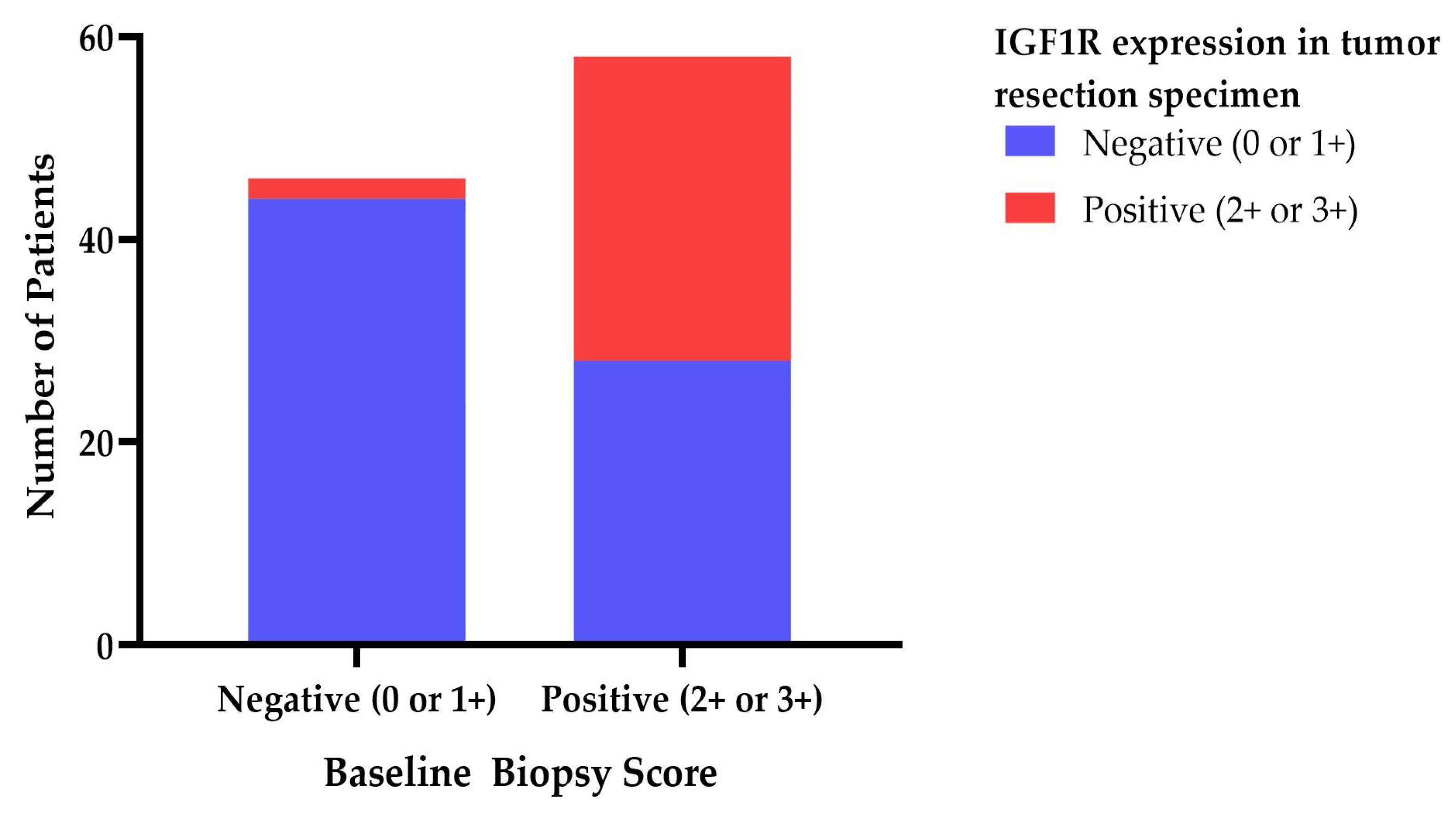
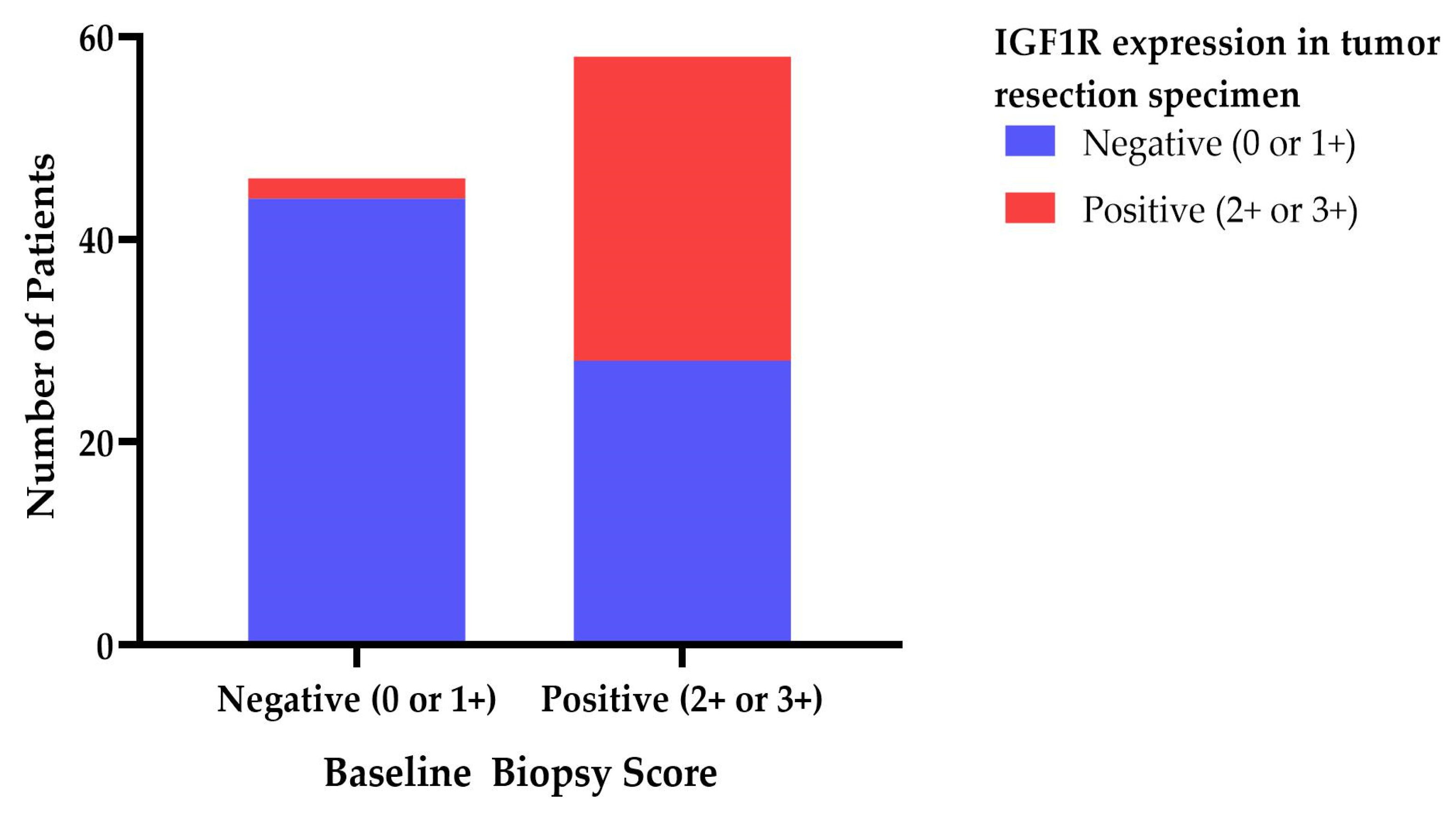
3.4. IGF1R Expression Score Is Not Associated with Clinical Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pollak, M. Insulin and insulin-like growth factor signalling in neoplasia. Nat. Rev. Cancer 2008, 8, 915–928. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The Next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Endogenous Hormones and Breast Cancer Collaborative Group; Key, T.J.; Appleby, P.N.; Reeves, G.K.; Roddam, A.W. Insulin-like growth factor 1 (IGF1), IGF binding protein 3 (IGFBP3), and breast cancer risk: Pooled individual data analysis of 17 prospective studies. Lancet Oncol. 2010, 11, 530–542. [Google Scholar] [PubMed]
- Key, T.J. Diet, insulin-like growth factor-1 and cancer risk. Proc. Nutr. Soc. 2011, 70, 385–388. [Google Scholar] [CrossRef] [PubMed]
- de Groot, S.; Charehbili, A.; van Laarhoven, H.W.; Mooyaart, A.L.; Dekker-Ensink, N.G.; van de Ven, S.; Janssen, L.G.M.; Swen, J.J.; Smit, V.T.H.B.M.; Heijns, J.B.; et al. Insulin-like growth factor 1 receptor expression and IGF1R 3129G > T polymorphism are associated with response to neoadjuvant chemotherapy in breast cancer patients: Results from the NEOZOTAC trial (BOOG 2010-01). Breast Cancer Res BCR. 2016, 18, 3. [Google Scholar] [CrossRef] [PubMed]
- Nencioni, A.; Caffa, I.; Cortellino, S.; Longo, V.D. Fasting and cancer: Molecular mechanisms and clinical application. Nat. Rev. Cancer 2018, 18, 707–719. [Google Scholar] [CrossRef] [PubMed]
- Raffaghello, L.; Lee, C.; Safdie, F.M.; Wei, M.; Madia, F.; Bianchi, G.; Longo, V.D. Starvation-dependent differential stress resistance protects normal but not cancer cells against high-dose chemotherapy. Proc. Natl. Acad. Sci. USA 2008, 105, 8215–8220. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Safdie, F.M.; Raffaghello, L.; Wei, M.; Madia, F.; Parrella, E.; Hwang, D.; Cohen, P.; Bianchi, G.; Longo, V.D. Reduced levels of IGF-I mediate differential protection of normal and cancer cells in response to fasting and improve chemotherapeutic index. Cancer Res. 2010, 70, 1564–1572. [Google Scholar] [CrossRef]
- Longo, V.D.; Mattson, M.P. Fasting: Molecular mechanisms and clinical applications. Cell Metab. 2014, 19, 181–192. [Google Scholar] [CrossRef]
- Brandhorst, S.; Choi, I.Y.; Wei, M.; Cheng, C.W.; Sedrakyan, S.; Navarrete, G.; Dubeau, L.; Yap, L.P.; Park, R.; Vinciguerra, M.; et al. A Periodic Diet that Mimics Fasting Promotes Multi-System Regeneration, Enhanced Cognitive Performance, and Healthspan. Cell Metab. 2015, 22, 86–99. [Google Scholar] [CrossRef]
- Merimee, T.J.; Zapf, J.; Froesch, E.R. Insulin-like growth factors in the fed and fasted states. J. Clin. Endocrinol. Metab. 1982, 55, 999–1002. [Google Scholar] [CrossRef] [PubMed]
- Vernieri, C.; Fuca, G.; Ligorio, F.; Huber, V.; Vingiani, A.; Iannelli, F.; Raimondi, A.; Rinchai, D.; Frigè, G.; Belfiore, A.; et al. Fasting-mimicking diet is safe and reshapes metabolism and antitumor immunity in cancer patients. Cancer Discov. 2021, 12, 90–107. [Google Scholar] [CrossRef] [PubMed]
- de Groot, S.; Lugtenberg, R.T.; Cohen, D.; Welters, M.J.P.; Ehsan, I.; Vreeswijk, M.P.G.; Smit, V.T.; de Graaf, H.; Heijns, J.B.; Portielje, J.E.; et al. Fasting mimicking diet as an adjunct to neoadjuvant chemotherapy for breast cancer in the multicentre randomized phase 2 DIRECT trial. Nat. Commun. 2020, 11, 3083. [Google Scholar] [CrossRef] [PubMed]
- Ogston, K.N.; Miller, I.D.; Payne, S.; Hutcheon, A.W.; Sarkar, T.K.; Smith, I.; Schofield, A.; Heys, S.D. A new histological grading system to assess response of breast cancers to primary chemotherapy: Prognostic significance and survival. Breast 2003, 12, 320–327. [Google Scholar] [CrossRef]
- Schwartz, L.H.; Litière, S.; de Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1—Update and Clarification: From the RECIST Committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Kent, W.J.; Sugnet, C.W.; Furey, T.S.; Roskin, K.M.; Pringle, T.H.; Zahler, A.M.; Haussler, D. The human genome browser at UCSC. Genome Res. 2002, 12, 996–1006. [Google Scholar] [CrossRef] [PubMed]
- Nassar, L.R.; Barber, G.P.; Benet-Pagès, A.; Casper, J.; Clawson, H.; Diekhans, M.; Fischer, C.; Gonzalez, J.N.; Hinrichs, A.S.; Lee, B.T.; et al. The UCSC Genome Browser database: 2023 update. Nucleic Acids Res. 2023, 51, D1188–D1195. [Google Scholar] [CrossRef]
- Ward, L.D.; Kellis, M. HaploReg: A resource for exploring chromatin states, conservation, and regulatory motif alterations within sets of genetically linked variants. Nucleic Acids Res. 2012, 40, D930–D934. [Google Scholar] [CrossRef]
- Machiela, M.J.; Chanock, S.J. LDlink: A web-based application for exploring population-specific haplotype structure and linking correlated alleles of possible functional variants. Bioinformatics 2015, 31, 3555–3557. [Google Scholar] [CrossRef]
- Biong, M.; Gram, I.T.; Brill, I.; Johansen, F.; Solvang, H.K.; Alnaes, G.I.; Fagerheim, T.; Bremnes, Y.; Chanock, S.J.; Burdett, L.; et al. Genotypes and haplotypes in the insulin-like growth factors, their receptors and binding proteins in relation to plasma metabolic levels and mammographic density. BMC Med. Genom. 2010, 3, 9. [Google Scholar] [CrossRef]
- Tice, J.A.; Cummings, S.R.; Smith-Bindman, R.; Ichikawa, L.; Barlow, W.E.; Kerlikowske, K. Using clinical factors and mammographic breast density to estimate breast cancer risk: Development and validation of a new predictive model. Ann. Intern. Med. 2008, 148, 337–347. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | Label | n Cases (Median) | % | Missing Cases | Total Cases |
|---|---|---|---|---|---|
| Median Age | (range) years | 50 (27–71) | 0 | 129 | |
| Median BMI | (range) kg/m2 | 25.8 (19.7–41.2) | 0 | 129 | |
| Randomization | chemo + FMD | 65 | 50.4% | 0 | 129 |
| chemo | 64 | 49.6% | |||
| Per-protocol * | chemo + FMD compliant | 22 | 17.1% | 0 | 124 |
| chemo + FMD non-compliant | 43 | 34.7% | |||
| chemo | 59 | 47.6% | |||
| HR status | ER−/Progesterone− | 21 | 16.3% | 1 (0.8%) | 128 |
| ER+/Progesterone− | 18 | 14.0% | |||
| ER+/Progesterone+ | 89 | 69.8% | |||
| Tumor Type | Other | 5 | 3.5% | 0 | 129 |
| Lobular | 22 | 20.2% | |||
| Ductal/Carcinoma | 102 | 76.3% | |||
| Tumor status ** | cT1 | 11 | 8.4% | 0 | 129 |
| cT2 | 83 | 64.9% | |||
| cT3 | 32 | 24.4% | |||
| cT4 | 3 | 2.3% | |||
| Lymph node status ** | cN0 | 63 | 48.1% | 0 | 129 |
| cN1 | 55 | 42.0% | |||
| cN2 | 11 | 8.4% | |||
| cN3 | 2 | 1.5% | |||
| Miller&Payne score | grade 1 no reduction | 35 | 27.1% | 1 (0.8%) | 128 |
| grade 2 < 30% tumor reduction | 26 | 20.9% | |||
| grade 3 30–90% tumor reduction | 33 | 25.6% | |||
| grade 4 > 90% tumor reduction | 20 | 15.5% | |||
| grade 5 no tumor | 14 | 10.9% | |||
| Miller&Payne pooled | grade 1–3 non-responders | 94 | 73.3% | 2 (1.5%) | 128 |
| grade 4–5 responders | 34 | 26.4% | |||
| Radiological response | CR | 16 | 14.8% | 23 (17.6%) | 108 |
| PR | 69 | 63.9% | |||
| SD | 22 | 20.4% | |||
| PD | 1 | 0.9% | |||
| Radiological response pooled | CR or PR responders | 85 | 78.7% | 23 (17.6%) | 108 |
| SD or PD non-responders | 23 | 21.3% |
| SNV | Reference Genotype | Heterozygous Genotype | Homozygous Genotype | MAF Ref Allele | N | HWE | p-Value * |
|---|---|---|---|---|---|---|---|
| IGF1R rs2016347 | 32 | 56 | 25 | 53% | 113 | 0.003 | 0.957 |
| IGF1R rs2229765 | 35 | 60 | 17 | 58% | 112 | 1.116 | 0.291 |
| IGF1R rs1815009 | 5 | 49 | 59 | 26% | 113 | 1.735 | 0.188 |
| INSR rs1051651 | 78 | 28 | 6 | 82% | 112 | 2.447 | 0.118 |
| INSR rs3745551 | 12 | 50 | 50 | 33% | 112 | 0.009 | 0.924 |
| IGF1R rs3743259 | 58 | 41 | 12 | 71% | 111 | 1.297 | 0.255 |
| IGF1R rs2684787 | 60 | 42 | 10 | 72% | 112 | 0.449 | 0.503 |
| IGF1R rs2654981 | 25 | 55 | 33 | 46% | 113 | 0.053 | 0.818 |
| IGF1R rs2654980 | 61 | 42 | 10 | 73% | 113 | 0.499 | 0.480 |
| IGF1R rs2684788 | 27 | 55 | 31 | 48% | 113 | 0.072 | 0.788 |
| IGF1R rs3743249 | 59 | 47 | 7 | 73% | 113 | 0.346 | 0.556 |
| IGF1R rs45484096 | 51 | 46 | 16 | 65% | 113 | 1.118 | 0.290 |
| INSR rs3833238 | 77 | 30 | 6 | 81% | 113 | 1.700 | 0.192 |
| INSR rs1051690 | 2 | 29 | 82 | 15% | 113 | 0.095 | 0.757 |
| INSR rs1799817 | 85 | 24 | 4 | 86% | 113 | 1.802 | 0.179 |
| INSR rs2252673 | 3 | 23 | 82 | 13% | 108 | 0.760 | 0.383 |
| IGF1R rs3743258 | 57 | 35 | 12 | 72% | 104 | 3.072 | 0.080 |
| Miller & Payne | Radiological Response | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SNVs | N | OR | 95%CI Lower-Upper | p-Value | N | OR | 95%CI Lower-Upper | p-Value | ||||
| IGF1R rs2016347 | 112 | 1.52 | 0.94 | - | 2.46 | 0.09 | 92 | 0.89 | 0.48 | - | 1.67 | 0.72 |
| IGF1R rs2229765 | 111 | 1.03 | 0.61 | - | 1.73 | 0.91 | 91 | 1.14 | 0.58 | - | 2.25 | 0.70 |
| IGF1R rs1815009 | 112 | 0.83 | 0.46 | - | 1.50 | 0.53 | 92 | 0.92 | 0.43 | - | 1.98 | 0.84 |
| INSR rs1051651 | 111 | 1.46 | 0.82 | - | 2.62 | 0.20 | 91 | 1.69 | 0.80 | - | 3.59 | 0.17 |
| INSR rs3745551 | 111 | 0.99 | 0.60 | - | 1.66 | 0.98 | 91 | 1.88 | 0.93 | - | 3.77 | 0.08 |
| IGF1R rs3743259 | 110 | 0.42 | 0.24 | - | 0.73 | 0.002 | 91 | 1.10 | 0.56 | - | 2.16 | 0.79 |
| IGF1R rs2684787 | 111 | 1.23 | 0.73 | - | 2.07 | 0.44 | 91 | 0.92 | 0.47 | - | 1.80 | 0.80 |
| IGF1R rs2654981 | 112 | 1.23 | 0.77 | - | 1.98 | 0.39 | 92 | 0.98 | 0.54 | - | 1.78 | 0.96 |
| IGF1R rs2654980 | 112 | 1.25 | 0.75 | - | 2.11 | 0.39 | 92 | 0.88 | 0.45 | - | 1.72 | 0.71 |
| IGF1R rs2684788 | 112 | 1.54 | 0.96 | - | 2.49 | 0.08 | 92 | 1.00 | 0.54 | - | 1.83 | 0.99 |
| IGF1R rs3743249 | 112 | 1.39 | 0.79 | - | 2.45 | 0.25 | 92 | 0.95 | 0.47 | - | 1.94 | 0.89 |
| IGF1R rs45484096 | 112 | 1.03 | 0.64 | - | 1.65 | 0.91 | 92 | 1.04 | 0.56 | - | 1.94 | 0.89 |
| INSR rs3833238 | 112 | 1.32 | 0.75 | - | 2.35 | 0.34 | 92 | 1.75 | 0.83 | - | 3.67 | 0.14 |
| INSR rs1051690 | 112 | 0.53 | 0.27 | - | 1.06 | 0.07 | 92 | 2.92 | 1.16 | - | 7.36 | 0.02 |
| INSR rs1799817 | 112 | 0.78 | 0.40 | - | 1.49 | 0.45 | 92 | 1.89 | 0.74 | - | 4.81 | 0.18 |
| INSR rs2252673 | 107 | 0.87 | 0.42 | - | 1.78 | 0.70 | 88 | 2.37 | 0.89 | - | 6.34 | 0.09 |
| IGF1R rs3743258 | 103 | 0.40 | 0.23 | - | 0.70 | 0.002 | 86 | 1.12 | 0.57 | - | 2.20 | 0.75 |
| SNVs | Miller & Payne | Radiological Response | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | OR | 95%CI | p-Value | N | OR | 95%CI | p-Value | |||||
| IGF1R rs2016347 | 72 | 1.40 | 0.74 | - | 2.63 | 0.30 | 61 | 0.76 | 0.34 | - | 1.74 | 0.52 |
| IGF1R rs2229765 | 72 | 1.21 | 0.63 | - | 2.33 | 0.57 | 61 | 0.93 | 0.41 | - | 2.13 | 0.87 |
| IGF1R rs1815009 | 72 | 1.07 | 0.52 | - | 2.19 | 0.86 | 61 | 0.56 | 0.22 | - | 1.41 | 0.22 |
| INSR rs1051651 | 72 | 1.11 | 0.56 | - | 2.21 | 0.77 | 61 | 1.67 | 0.71 | - | 3.94 | 0.24 |
| INSR rs3745551 | 72 | 1.49 | 0.79 | - | 2.80 | 0.22 | 61 | 1.72 | 0.77 | - | 3.87 | 0.19 |
| IGF1R rs3743259 | 72 | 0.49 | 0.25 | - | 0.94 | 0.03 | 61 | 1.24 | 0.56 | - | 2.72 | 0.59 |
| IGF1R rs2684787 | 71 | 1.29 | 0.66 | - | 2.52 | 0.46 | 60 | 0.45 | 0.18 | - | 1.12 | 0.09 |
| IGF1R rs2654981 | 72 | 0.98 | 0.51 | - | 1.88 | 0.94 | 61 | 0.91 | 0.42 | - | 2.00 | 0.82 |
| IGF1R rs2654980 | 72 | 1.36 | 0.70 | - | 2.64 | 0.37 | 61 | 0.43 | 0.17 | - | 1.05 | 0.06 |
| IGF1R rs2684788 | 72 | 1.33 | 0.71 | - | 2.50 | 0.37 | 61 | 0.85 | 0.38 | - | 1.87 | 0.68 |
| IGF1R rs3743249 | 72 | 1.10 | 0.54 | - | 2.21 | 0.80 | 61 | 1.37 | 0.57 | - | 3.30 | 0.49 |
| IGF1R rs45484096 | 72 | 1.07 | 0.59 | - | 1.94 | 0.83 | 61 | 0.68 | 0.31 | - | 1.49 | 0.33 |
| INSR rs3833238 | 72 | 1.01 | 0.51 | - | 2.02 | 0.97 | 61 | 1.58 | 0.67 | - | 3.73 | 0.29 |
| INSR rs1051690 | 72 | 0.41 | 0.16 | - | 1.04 | 0.061 | 61 | 3.41 | 1.09 | - | 10.63 | 0.035 |
| INSR rs1799817 | 72 | 0.51 | 0.21 | - | 1.28 | 0.15 | 61 | 1.55 | 0.46 | - | 5.31 | 0.48 |
| INSR rs2252673 | 69 | 1.30 | 0.56 | - | 3.04 | 0.54 | 59 | 1.68 | 0.56 | - | 5.02 | 0.35 |
| IGF1R rs3743258 | 68 | 0.46 | 0.24 | - | 0.91 | 0.03 | 59 | 1.23 | 0.56 | - | 2.70 | 0.61 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Gruil, N.; Böhringer, S.; de Groot, S.; Pijl, H.; Kroep, J.R.; Swen, J.J. IGF1 and Insulin Receptor Single Nucleotide Variants Associated with Response in HER2-Negative Breast Cancer Patients Treated with Neoadjuvant Chemotherapy with or without a Fasting Mimicking Diet (BOOG 2013-04 DIRECT Trial). Cancers 2023, 15, 5872. https://doi.org/10.3390/cancers15245872
de Gruil N, Böhringer S, de Groot S, Pijl H, Kroep JR, Swen JJ. IGF1 and Insulin Receptor Single Nucleotide Variants Associated with Response in HER2-Negative Breast Cancer Patients Treated with Neoadjuvant Chemotherapy with or without a Fasting Mimicking Diet (BOOG 2013-04 DIRECT Trial). Cancers. 2023; 15(24):5872. https://doi.org/10.3390/cancers15245872
Chicago/Turabian Stylede Gruil, Nadia, Stefan Böhringer, Stefanie de Groot, Hanno Pijl, Judith R. Kroep, and Jesse J. Swen. 2023. "IGF1 and Insulin Receptor Single Nucleotide Variants Associated with Response in HER2-Negative Breast Cancer Patients Treated with Neoadjuvant Chemotherapy with or without a Fasting Mimicking Diet (BOOG 2013-04 DIRECT Trial)" Cancers 15, no. 24: 5872. https://doi.org/10.3390/cancers15245872
APA Stylede Gruil, N., Böhringer, S., de Groot, S., Pijl, H., Kroep, J. R., & Swen, J. J. (2023). IGF1 and Insulin Receptor Single Nucleotide Variants Associated with Response in HER2-Negative Breast Cancer Patients Treated with Neoadjuvant Chemotherapy with or without a Fasting Mimicking Diet (BOOG 2013-04 DIRECT Trial). Cancers, 15(24), 5872. https://doi.org/10.3390/cancers15245872