
Associations between Single Nucleotide Polymorphisms from the Genes of Chemokines and the CXCR2 Chemokine Receptor and an Increased Risk of Endometrial Cancer
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. DNA Extraction
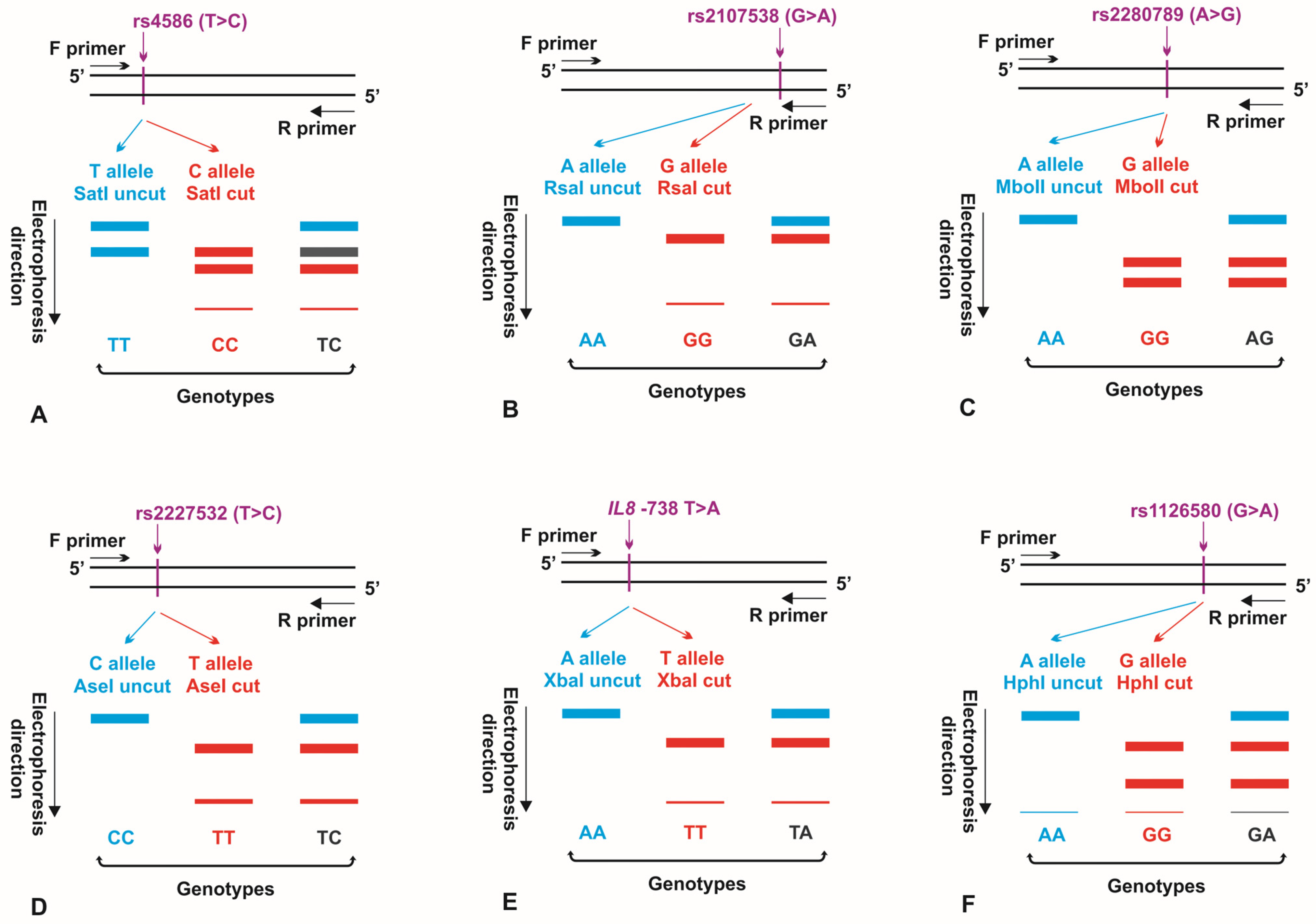
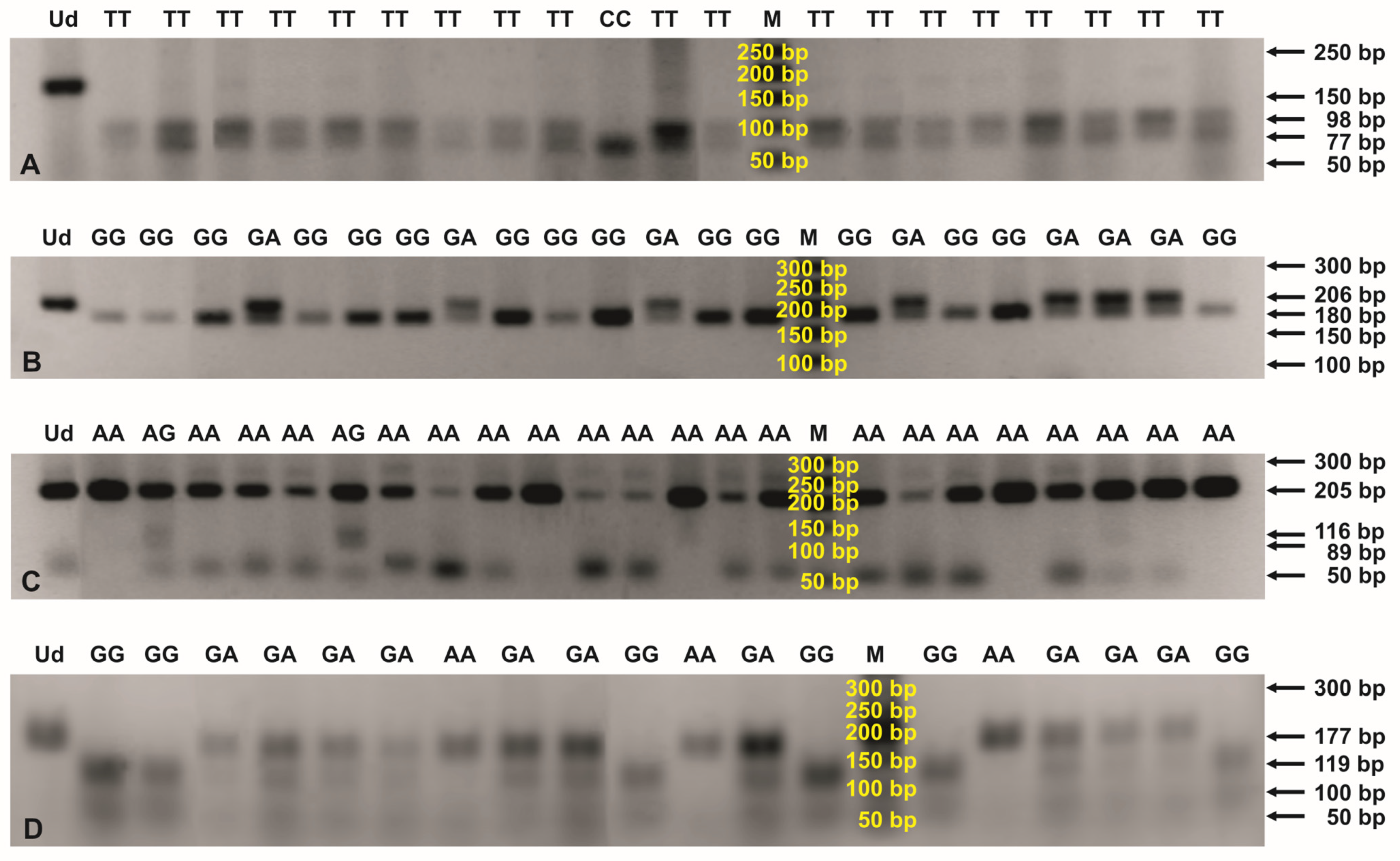
2.2. Genotypes within SNPs of Chemokine and Chemokine Receptor Genes
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Hardy-Weinberg Equilibrium and Linkage Disequilibrium
3.3. Genotypes in Chemokine and Chemokine Receptor Gene Polymorphisms
3.4. Allelic Variants within SNPs of the Chemokine and Chemokine Receptor Genes
3.5. Sample Size Calculation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, B.; Chen, P.; Xi, D.; Zhu, H.; Gao, Y. ATF4 regulates CCL2 expression to promote endometrial cancer growth by controlling macrophage infiltration. Exp. Cell Res. 2017, 360, 105–112. [Google Scholar] [CrossRef]
- Yu, X.; Zhou, B.; Zhang, Z.; Lan, Z.; Chen, P.; Duan, R.; Zhang, L.; Xi, M. Insertion/deletion polymorphism in IL1A 3′-UTR is associated with susceptibility to endometrial cancer in Chinese Han women. J. Obstet. Gynaecol. Res. 2016, 42, 983–989. [Google Scholar] [CrossRef]
- Ewington, L.; Taylor, A.; Sriraksa, R.; Horimoto, Y.; Lam, E.W.; El-Bahrawy, M.A. The expression of interleukin-8 and interleukin-8 receptors in endometrial carcinoma. Cytokine 2012, 59, 417–422. [Google Scholar] [CrossRef]
- Smith, H.O.; Stephens, N.D.; Qualls, C.R.; Fligelman, T.; Wang, T.; Lin, C.Y.; Burton, E.; Griffith, J.K.; Pollard, J.W. The clinical significance of inflammatory cytokines in primary cell culture in endometrial carcinoma. Mol. Oncol. 2013, 7, 41–54. [Google Scholar] [CrossRef]
- Tong, H.; Ke, J.Q.; Jiang, F.Z.; Wang, X.J.; Wang, F.Y.; Li, Y.R.; Lu, W.; Wan, X.P. Tumor-associated macrophage-derived CXCL8 could induce ERα suppression via HOXB13 in endometrial cancer. Cancer Lett. 2016, 376, 127–136. [Google Scholar] [CrossRef]
- Attar, R.; Agachan, B.; Kuran, S.B.; Cacina, C.; Sozen, S.; Yurdum, L.M.; Attar, E.; Isbir, T. Association of CCL2 and CCR2 gene variants with endometrial cancer in Turkish women. In Vivo 2010, 24, 243–248. [Google Scholar]
- Brooks, N.; Stojanovska, L.; Grant, P.; Apostolopoulos, V.; McDonald, C.F.; Pouniotis, D.S. Characterization of blood monocyte phenotype in patients with endometrial cancer. Int. J. Gynecol. Cancer 2012, 22, 1500–1508. [Google Scholar] [CrossRef]
- Doster, A.; Schwarzig, U.; Zygmunt, M.; Rom, J.; Schutz, F.; Fluhr, H. Unfractionated Heparin Selectively Modulates the Expression of CXCL8, CCL2 and CCL5 in Endometrial Carcinoma Cells. Anticancer. Res. 2016, 36, 1535–1544. [Google Scholar]
- Pena, C.G.; Nakada, Y.; Saatcioglu, H.D.; Aloisio, G.M.; Cuevas, I.; Zhang, S.; Miller, D.S.; Lea, J.S.; Wong, K.K.; DeBerardinis, R.J.; et al. LKB1 loss promotes endometrial cancer progression via CCL2-dependent macrophage recruitment. J. Clin. Investig. 2015, 125, 4063–4076. [Google Scholar] [CrossRef]
- Zhang, W.; Hou, F.; Zhang, Y.; Tian, Y.; Jiao, J.; Ma, D.; Kong, B.; Cui, B. Changes of Th17/Tc17 and Th17/Treg cells in endometrial carcinoma. Gynecol. Oncol. 2014, 132, 599–605. [Google Scholar] [CrossRef]
- Berry, K.K.; Varney, M.L.; Dave, B.J.; Bucana, C.D.; Fidler, I.J.; Singh, R.K. Expression of interleukin-8 in human metastatic endometrial carcinoma cells and its regulation by inflammatory cytokines. Int. J. Gynecol. Cancer 2001, 11, 54–60. [Google Scholar] [CrossRef]
- Di Donato, V.; Giannini, A.; Bogani, G. Recent Advances in Endometrial Cancer Management. J. Clin. Med. 2023, 12, 2241. [Google Scholar] [CrossRef]
- Golia D’Augè, T.; Cuccu, I.; Santangelo, G.; Muzii, L.; Giannini, A.; Bogani, G.; Di Donato, V. Novel Insights into Molecular Mechanisms of Endometrial Diseases. Biomolecules 2023, 13, 499. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network; Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar]
- Dinkic, C.; Kruse, A.; Zygmunt, M.; Schuetz, F.; Brucker, J.; Rom, J.; Sohn, C.; Fluhr, H. Influence of Paclitaxel and Heparin on Vitality, Proliferation and Cytokine Production of Endometrial Cancer Cells. Geburtshilfe Frauenheilkd. 2017, 77, 1104–1110. [Google Scholar] [CrossRef]
- He, S.; Zhang, X. The rs1024611 in the CCL2 gene and risk of gynecological cancer in Asians: A meta-analysis. World J. Surg. Oncol. 2018, 16, 34. [Google Scholar] [CrossRef]
- Jakóbisiak, M.; Lasek, W. Immunologia nowotworów. In Immunologia; Gołąb, J., Jakóbisiak, M., Lasek, W., Stokłosa, T., Eds.; Wydawnictwo Naukowe PWN SA: Warszawa, Poland, 2012; pp. 450–467. [Google Scholar]
- Wallace, A.E.; Sales, K.J.; Catalano, R.D.; Anderson, R.A.; Williams, A.R.; Wilson, M.R.; Schwarze, J.; Wang, H.; Rossi, A.G.; Jabbour, H.N. Prostaglandin F2alpha-F-prostanoid receptor signaling promotes neutrophil chemotaxis via chemokine (C-X-C motif) ligand 1 in endometrial adenocarcinoma. Cancer Res. 2009, 69, 5726–5733. [Google Scholar] [CrossRef]
- Wang, J.; Taylor, A.; Showeil, R.; Trivedi, P.; Horimoto, Y.; Bagwan, I.; Ewington, L.; Lam, E.W.; El-Bahrawy, M.A. Expression profiling and significance of VEGF-A, VEGFR2, VEGFR3 and related proteins in endometrial carcinoma. Cytokine 2014, 68, 94–100. [Google Scholar] [CrossRef]
- FIGO Staging of Endometrial Cancer: 2023. Available online: https://www.figo.org/news/figo-staging-endometrial-cancer-2023 (accessed on 26 September 2023).
- Dan, H.; Liu, W.; Zhou, Y.; Wang, J.; Chen, Q.; Zeng, X. Association of interleukin-8 gene polymorphisms and haplotypes with oral lichen planus in a Chinese population. Inflammation 2010, 33, 76–81. [Google Scholar] [CrossRef]
- Mhmoud, N.; Fahal, A.; Wendy van de Sande, W.J. Association of IL-10 and CCL5 single nucleotide polymorphisms with tuberculosis in the Sudanese population. Trop. Med. Int. Health 2013, 18, 1119–1127. [Google Scholar] [CrossRef]
- Singh, B.; Chitra, J.; Selvaraj, P. CCL2, CCL3 and CCL4 gene polymorphisms in pulmonary tuberculosis patients of South India. Int. J. Immunogenet. 2014, 41, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Viana, A.C.; Kim, Y.J.; Cirelli, J.A.; Orrico, S.R.; Curtis, K.C.; Cano, V.S.; Valentini, S.R.; Scarel-Caminaga, R.M. A novel PCR-RFLP assay for the detection of the single nucleotide polymorphism at position +1440 in the human CXCR2 gene. Biochem. Genet. 2007, 45, 737–741. [Google Scholar] [CrossRef]
- SNPStats Software. 2023. Available online: https://www.snpstats.net/start.htm (accessed on 26 September 2023).
- Braun, M.M.; Overbeek-Wager, E.A.; Grumbo, R.J. Diagnosis and Management of Endometrial Cancer. Am. Fam. Physician 2016, 93, 468–474. [Google Scholar] [PubMed]
- Gentry-Maharaj, A.; Karpinskyj, C. Current and future approaches to screening for endometrial cancer. Best. Pract. Res. Clin. Obstet. Gynaecol. 2020, 65, 79–97. [Google Scholar] [CrossRef] [PubMed]
- Yao, L.; Li, C.; Cheng, J. The relationship between endometrial thickening and endometrial lesions in postmenopausal women. Arch. Gynecol. Obstet. 2022, 306, 2047–2054. [Google Scholar] [CrossRef]
- Zhang, L.; Guo, Y.; Qian, G.; Su, T.; Xu, H. Value of endometrial thickness for the detection of endometrial cancer and atypical hyperplasia in asymptomatic postmenopausal women. BMC Womens Health 2022, 22, 517. [Google Scholar] [CrossRef]
- Shan, J.; Chouchane, A.; Mokrab, Y.; Saad, M.; Boujassoum, S.; Sayaman, R.W.; Ziv, E.; Bouaouina, N.; Remadi, Y.; Gabbouj, S.; et al. Genetic Variation in CCL5 Signaling Genes and Triple Negative Breast Cancer: Susceptibility and Prognosis Implications. Front. Oncol. 2019, 9, 1328. [Google Scholar] [CrossRef] [PubMed]
- Eskandari-Nasab, E.; Hashemi, M.; Ebrahimi, M.; Amininia, S.; Bahari, G.; Mashhadi, M.A.; Taheri, M. Evaluation of CCL5 -403 G>A and CCR5 Δ32 gene polymorphisms in patients with breast cancer. Cancer Biomark. 2014, 14, 343–351. [Google Scholar] [CrossRef]
- Charni, F.; Sutton, A.; Rufat, P.; Laguillier, C.; Mansouri, A.; Moreau, R.; Ganne-Carrié, N.; Trinchet, J.C.; Beaugrand, M.; Charnaux, N.; et al. Chemokine RANTES promoter dimorphisms and hepatocellular carcinoma occurrence in patients with alcoholic or hepatitis C virus-related cirrhosis. Cancer Epidemiol. Biomark. Prev. 2011, 20, 1439–1446. [Google Scholar] [CrossRef]
- Kidd, L.R.; Jones, D.Z.; Rogers, E.N.; Kidd, N.C.; Beache, S.; Rudd, J.E.; Ragin, C.; Jackson, M.; McFarlane-Anderson, N.; Tulloch-Reid, M.; et al. Chemokine Ligand 5 (CCL5) and chemokine receptor (CCR5) genetic variants and prostate cancer risk among men of African Descent: A case-control study. Hered. Cancer Clin. Pract. 2012, 10, 16. [Google Scholar] [CrossRef]
- Kwon, K.H.; Lee, Y.C.; Chung, J.H.; Eun, Y.G. Association study of chemokine (C-C motif) ligand 5 gene polymorphism and papillary thyroid cancer. J. Investig. Surg. 2013, 26, 319–324. [Google Scholar] [CrossRef]
- Weng, C.J.; Chien, M.H.; Lin, C.W.; Chung, T.T.; Zavras, A.I.; Tsai, C.M.; Chen, M.K.; Yang, S.F. Effect of CC chemokine ligand 5 and CC chemokine receptor 5 genes polymorphisms on the risk and clinicopathological development of oral cancer. Oral. Oncol. 2010, 46, 767–772. [Google Scholar] [CrossRef]
- Pang, Y.; Li, H.; Gong, Y.; Jing, S.; Peng, C.; Liu, W.; Zhao, Y.; Wang, H.; Kaushik, D.; Rodriguez, R.; et al. Association of CCL2, CCR2 and CCL5 genetic polymorphisms with the development and progression of benign prostatic hyperplasia. Oncol. Rep. 2019, 41, 2491–2501. [Google Scholar] [CrossRef] [PubMed]
- GTEx Portal. 2018. Available online: http://www.gtexportal.org/home/ (accessed on 26 September 2023).
- Subramaniam, K.S.; Tham, S.T.; Mohamed, Z.; Woo, Y.L.; Mat Adenan, N.A.; Chung, I. Cancer-associated fibroblasts promote proliferation of endometrial cancer cells. PLoS ONE 2013, 8, e68923. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.E.; Fallin, D.; Ruczinski, I.; Hutchinson, A.; Staats, B.; Vitale, F.; Lauria, C.; Serraino, D.; Rezza, G.; Mbisa, G.; et al. Associations of classic Kaposi sarcoma with common variants in genes that modulate host immunity. Cancer Epidemiol. Biomark. Prev. 2006, 15, 926–934. [Google Scholar] [CrossRef]
- Hsing, A.W.; Sakoda, L.C.; Rashid, A.; Andreotti, G.; Chen, J.; Wang, B.S.; Shen, M.C.; Chen, B.E.; Rosenberg, P.S.; Zhang, M.; et al. Variants in inflammation genes and the risk of biliary tract cancers and stones: A population-based study in China. Cancer Res. 2008, 68, 6442–6452. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Dai, Y.; Zheng, T.; Ma, S. Risk Factors of Non-Hodgkin Lymphoma. Expert Opin. Med. Diagn. 2011, 5, 539–550. [Google Scholar] [CrossRef]
- Viana, A.C.; Kim, Y.J.; Curtis, K.M.; Renzi, R.; Orrico, S.R.; Cirelli, J.A.; Scarel-Caminaga, R.M. Association of haplotypes in the CXCR2 gene with periodontitis in a Brazilian population. DNA Cell Biol. 2010, 29, 191–200. [Google Scholar] [CrossRef]
- Lupiañez, C.B.; Canet, L.M.; Carvalho, A.; Alcazar-Fuoli, L.; Springer, J.; Lackner, M.; Segura-Catena, J.; Comino, A.; Olmedo, C.; Ríos, R.; et al. Polymorphisms in Host Immunity-Modulating Genes and Risk of Invasive Aspergillosis: Results from the AspBIOmics Consortium. Infect. Immun. 2015, 84, 643–657. [Google Scholar] [CrossRef]
- Kulinczak, M.; Sromek, M.; Panek, G.; Zakrzewska, K.; Lotocka, R.; Szafron, L.M.; Chechlinska, M.; Siwicki, J.K. Endometrial Cancer-Adjacent Tissues Express Higher Levels of Cancer-Promoting Genes than the Matched Tumors. Genes 2022, 13, 1611. [Google Scholar] [CrossRef]
- Shin, D.Y.; Kim, I.; Kim, J.H.; Lee, Y.G.; Kang, E.J.; Cho, H.J.; Lee, K.H.; Kim, H.J.; Park, E.H.; Lee, J.E.; et al. RANTES polymorphisms and the risk of graft-versus-host disease in human leukocyte antigen-matched sibling allogeneic hematopoietic stem cell transplantation. Acta Haematol. 2013, 129, 137–145. [Google Scholar] [CrossRef]
- An, P.; Nelson, G.W.; Wang, L.; Donfield, S.; Goedert, J.J.; Phair, J.; Vlahov, D.; Buchbinder, S.; Farrar, W.L.; Modi, W.; et al. Modulating influence on HIV/AIDS by interacting RANTES gene variants. Proc. Natl. Acad. Sci. USA 2002, 99, 10002–10007. [Google Scholar] [CrossRef] [PubMed]
- Suenaga, M.; Stintzing, S.; Cao, S.; Zhang, W.; Yang, D.; Ning, Y.; Okazaki, S.; Berger, M.D.; Miyamoto, Y.; Schirripa, M.; et al. Role of CCL5 and CCR5 gene polymorphisms in epidermal growth factor receptor signalling blockade in metastatic colorectal cancer: Analysis of the FIRE-3 trial. Eur. J. Cancer 2019, 107, 100–114. [Google Scholar] [CrossRef]
- Suenaga, M.; Cao, S.; Zhang, W.; Yang, D.; Ning, Y.; Okazaki, S.; Berger, M.D.; Miyamoto, Y.; Schirripa, M.; Soni, S.; et al. Genetic variants in CCL5 and CCR5 genes and serum VEGF-A levels predict efficacy of bevacizumab in metastatic colorectal cancer patients. Int. J. Cancer 2019, 144, 2567–2577. [Google Scholar] [CrossRef]
- Suenaga, M.; Schirripa, M.; Cao, S.; Zhang, W.; Yang, D.; Ning, Y.; Cremolini, C.; Antoniotti, C.; Borelli, B.; Mashima, T.; et al. Gene Polymorphisms in the CCL5/CCR5 Pathway as a Genetic Biomarker for Outcome and Hand-Foot Skin Reaction in Metastatic Colorectal Cancer Patients Treated With Regorafenib. Clin. Color. Cancer 2018, 17, e395–e414. [Google Scholar] [CrossRef] [PubMed]
- Gong, Z.; Quan, L.; Yao, S.; Zirpoli, G.; Bandera, E.V.; Roberts, M.; Coignet, J.G.; Cabasag, C.; Sucheston, L.; Hwang, H.; et al. Innate immunity pathways and breast cancer Risk in African American and European-American women in the Women’s Circle of Health Study (WCHS). PLoS ONE 2013, 8, e72619. [Google Scholar] [CrossRef]
- Naseem, M.; Cao, S.; Yang, D.; Millstein, J.; Puccini, A.; Loupakis, F.; Stintzing, S.; Cremolini, C.; Tokunaga, R.; Battaglin, F.; et al. Random survival forests identify pathways with polymorphisms predictive of survival in KRAS mutant and KRAS wild-type metastatic colorectal cancer patients. Sci. Rep. 2021, 11, 12191. [Google Scholar] [CrossRef] [PubMed]
- Sunakawa, Y.; Stremitzer, S.; Cao, S.; Zhang, W.; Yang, D.; Wakatsuki, T.; Ning, Y.; Yamauchi, S.; Stintzing, S.; Sebio, A.; et al. Association of variants in genes encoding for macrophage-related functions with clinical outcome in patients with locoregional gastric cancer. Ann. Oncol. 2015, 26, 332–339. [Google Scholar] [CrossRef]
- Yoon, S.; Kang, B.W.; Park, S.Y.; Kim, H.J.; Park, J.S.; Choi, G.S.; Kim, J.G. Prognostic relevance of genetic variants involved in immune checkpoints in patients with colorectal cancer. J. Cancer Res. Clin. Oncol. 2016, 142, 1775–1780. [Google Scholar] [CrossRef]
- Sunakawa, Y.; Stintzing, S.; Cao, S.; Heinemann, V.; Cremolini, C.; Falcone, A.; Yang, D.; Zhang, W.; Ning, Y.; Stremitzer, S.; et al. Variations in genes regulating tumor-associated macrophages (TAMs) to predict outcomes of bevacizumab-based treatment in patients with metastatic colorectal cancer: Results from TRIBE and FIRE3 trials. Ann. Oncol. 2015, 26, 2450–2456. [Google Scholar] [CrossRef]
- GTEx Consortium. The Genotype-Tissue Expression (GTEx) project. Nat. Genet. 2013, 45, 580–585. [Google Scholar] [CrossRef]
- Lin, C.; Wang, Z.; Shen, L.; Yi, G.; Li, M.; Li, D. Genetic Variants, Circulating Level of MCP1 with Risk of Chronic Obstructive Pulmonary Disease: A Case-Control Study. Pharmgenom. Pers. Med. 2021, 14, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Li, J.; Yang, H.; Jiang, L.; Zhou, X.; Huang, Y.; Xu, N. Association of CCL2 Gene Variants with Osteoarthritis. Arch. Med. Res. 2019, 50, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Dobroch, J.; Bojczuk, K.; Kołakowski, A.; Baczewska, M.; Knapp, P. The Exploration of Chemokines Importance in the Pathogenesis and Development of Endometrial Cancer. Molecules 2022, 27, 2041. [Google Scholar] [CrossRef]
- Zhang, J.J.; Liu, W.; Xing, G.Z.; Xiang, L.; Zheng, W.M.; Ma, Z.L. Role of CC-chemokine ligand 2 in gynecological cancer. Cancer Cell Int. 2022, 22, 361. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic Features | Females with Endometrial Cancer | Non-Cancerous Controls | p-Value a |
|---|---|---|---|
| Examined women; n b (%) | 132 (46.8) | 150 (53.2) | |
| Age (years) | 61 (44–88) | 50 (36–75) | ≤0.001 |
| Diabetes mellitus (%) | 23/132 (17.4) | 2/140 (1.4) | ≤0.001 |
| Arterial hypertension (%) | 71/132 (53.8) | 22/140 (15.7) | ≤0.001 |
| FIGO c grade | |||
| G1 (%) | 61/117 (52.14) | ||
| G2 (%) | 41/117 (35.04) | ||
| G3 (%) | 15/117 (12.82) | ||
| FIGO stage | |||
| I (%) | 83/115 (72.2) | ||
| II (%) | 16/115 (13.9) | ||
| III (%) | 16/115 (13.9) | ||
| Endometrial thickness (mm) | 6.5 (1.2–116.0) | 11 (1.5–14.0) | ≤0.001 |
| >5 mm (%) | 97/116 (83.6) | 59/95 (62.1) | ≤0.001 |
| Gene | GenBank Accession No. a | SNP b Name | Oligonucleotides (5′-3′) | Annealing Temperature (°C) | Amplicon Length (bps) c | |
|---|---|---|---|---|---|---|
| CCL2 | NC_000017.11 | 903 T>C | External | For: TCCTCATGACTCTTTTCTGC | 52 | 263 |
| (rs4586) | Rev: GAGGCTTGTCCCTTGCTCCAC | |||||
| Internal | For: TTCCAGATGCAATCAATGCC | 55 | 173 | |||
| Rev: TCCACAAGGAAGAACTTCAG | ||||||
| CCL5 | NC_000017.11 | −403 G>A | For: CACAAGAGGACTCATTCCAACTCA | 55 | 206 | |
| (rs2107538) | Rev: GTTCCTGCTTATTCATTACAGATCGTA | |||||
| 351 A>G | External | For: CCTGGTCTTGACCACCACA | 52 | 343 | ||
| (rs2280789) | Rev: GCTGACAGGCATGAGTCAGA | |||||
| Internal | For: AGCATGAATACTGTCTGAACCC | 55 | 205 | |||
| Rev: GCTACTCATGACTACTAATCTCC | ||||||
| IL8 | NC_000004.12 | −845 T>C | External | For: AACCCAGCAGCTCCAGTG | 52 | 534 |
| (rs2227532) | Rev: AGATAAGCCAGCCAATCATT | |||||
| −738 T>A | Internal | For: CAACTGCCTTTGGAAGATTCTG | 55 | 185 | ||
| Rev: GGAGTAACTTTCTGAGTAATGTGG | ||||||
| CXCR2 | NC_000002.12 | 1440 G>A | External | For: CCCCATTGTGGTCACAGGACG | 52 | 343 |
| (rs1126580) | Rev: GCCTCCCAAGTAGCTGTGATTA | |||||
| Internal | For: GGCACTCTATGTTCTAAGAAGTG | 56.4 | 181 | |||
| Rev: GATTACAGGCACTCACCACC | ||||||
| Polymorphism | Endonuclease | Profile (bps) a |
|---|---|---|
| CCL2 | SatI | CC: 77, 66, 32 |
| 903 T>C | TC: 98, 77, 66, 32 | |
| TT: 98, 77 | ||
| CCL5 | RsaI | GG: 180, 26 |
| −403 G>A | GA: 206, 180, 26 | |
| AA: 206 | ||
| CCL5 | MboII | AA: 205 |
| 351 A>G | AG: 205, 116, 89 | |
| GG: 116, 89 | ||
| IL8 | AseI | TT: 142, 43 |
| −845 T>C | TC: 185, 142, 43 | |
| CC: 185 | ||
| IL8 | XbaI | TT: 152, 33 |
| −738 T>A | TA: 185, 152, 33 | |
| AA: 185 | ||
| CXCR2 | HphI | GG: 119, 58, 4 |
| 1440 G>A | GA: 177, 119, 58, 4 | |
| AA: 177, 4 |
| Gene Polymorphism | Genetic Model | Genotype | Genotype Prevalence Rates; n (%) a | OR b (95% CI) c | p-Value d | |
|---|---|---|---|---|---|---|
| Endometrial Cancer | Non-Cancerous Controls | |||||
| CCL2 | Codominant | T/T | 112 (86.2%) | 133 (89.3%) | 1.00 | |
| 903 T>C | T/C | 4 (3.1%) | 3 (2.0%) | 1.58 (0.35–7.22) | ||
| C/C | 14 (10.8%) | 13 (8.7%) | 1.28 (0.58–2.83) | 0.710 | ||
| Dominant | T/T | 112 (86.2%) | 133 (89.3%) | 1.00 | ||
| T/C-C/C | 18 (13.8%) | 16 (10.7%) | 1.34 (0.65–2.74) | 0.430 | ||
| Recessive | T/T-T/C | 116 (89.2%) | 136 (91.3%) | 1.00 | ||
| C/C | 14 (10.8%) | 13 (8.7%) | 1.26 (0.57–2.79) | 0.560 | ||
| Overdominant | T/T-C/C | 126 (96.9%) | 146 (98.0%) | 1.00 | ||
| T/C | 4 (3.1%) | 3 (2.0%) | 1.54 (0.34–7.03) | 0.570 | ||
| CCL5 | Codominant | G/G | 70 (56.9%) | 99 (66.4%) | 1.00 | |
| −403 G>A | G/A | 33 (26.8%) | 44 (29.5%) | 1.06 (0.61–1.83) | ||
| A/A | 20 (16.3%) | 6 (4.0%) | 4.71 (1.80–12.34) | 0.002 | ||
| Dominant | G/G | 70 (56.9%) | 99 (66.4%) | 1.00 | ||
| G/A-A/A | 53 (43.1%) | 50 (33.6%) | 1.50 (0.92–2.45) | 0.110 | ||
| Recessive | G/G-G/A | 103 (83.7%) | 143 (96.0%) | 1.00 | ||
| A/A | 20 (16.3%) | 6 (4.0%) | 4.63 (1.80–11.93) | ≤0.001 | ||
| Overdominant | G/G-A/A | 90 (73.2%) | 105 (70.5%) | 1.00 | ||
| G/A | 33 (26.8%) | 44 (29.5%) | 0.88 (0.51–1.49) | 0.620 | ||
| CCL5 | Codominant | A/A | 108 (85.0%) | 124 (83.2%) | 1.00 | |
| 351 A>G | A/G | 18 (14.2%) | 25 (16.8%) | 0.83 (0.43–1.60) | ||
| G/G | 1 (0.8%) | 0 (0.0%) | NA (0.00–NA) e | 0.390 | ||
| Dominant | A/A | 108 (85.0%) | 124 (83.2%) | 1.00 | ||
| A/G-G/G | 19 (15.0%) | 25 (16.8%) | 0.87 (0.46–1.67) | 0.680 | ||
| Recessive | A/A-A/G | 126 (99.2%) | 149 (100.0%) | 1.00 | ||
| G/G | 1 (0.8%) | 0 (0.0%) | NA (0.00–NA) | 0.210 | ||
| Overdominant | A/A-G/G | 109 (85.8%) | 124 (83.2%) | 1.00 | ||
| A/G | 18 (14.2%) | 25 (16.8%) | 0.82 (0.42–1.58) | 0.550 | ||
| IL8 | - | T/T | 129 (99.2%) | 149 (99.3%) | 1.00 | |
| −738 T>A | T/A | 1 (0.8%) | 1 (0.7%) | 1.16 (0.07–18.65) | 0.920 | |
| CXCR2 | Codominant | A/A | 56 (44.4%) | 83 (55.7%) | 1.00 | |
| 1440 G>A | G/A | 45 (35.7%) | 22 (14.8%) | 3.03 (1.64–5.59) | ||
| G/G | 25 (19.8%) | 44 (29.5%) | 0.84 (0.46–1.53) | ≤0.001 | ||
| Dominant | A/A | 56 (44.4%) | 83 (55.7%) | 1.00 | 0.062 | |
| G/A-G/G | 70 (55.6%) | 66 (44.3%) | 1.57 (0.98–2.53) | |||
| Recessive | A/A-G/A | 101 (80.2%) | 105 (70.5%) | 1.00 | 0.063 | |
| G/G | 25 (19.8%) | 44 (29.5%) | 0.59 (0.34–1.04) | |||
| Overdominant | A/A-G/G | 81 (64.3%) | 127 (85.2%) | 1.00 | ≤0.001 | |
| G/A | 45 (35.7%) | 22 (14.8%) | 3.21 (1.79–5.73) | |||
| Covariate | Genetic Model | Genotype | Genotype Prevalence, n a (%) | OR b (95% CI c) | p-Value d | |
|---|---|---|---|---|---|---|
| Endometrial Cancer | Non-Cancerous Controls | |||||
| Age | Codominant | A/A | 75 (59.5%) | 52 (50.0%) | 1.00 | 0.020 |
| G/A | 14 (11.1%) | 31 (29.8%) | 3.62 (1.42–9.20) | |||
| G/G | 37 (29.4%) | 21 (20.2%) | 1.15 (0.51–2.57) | |||
| Dominant | A/A | 75 (59.5%) | 52 (50.0%) | 1.00 | 0.082 | |
| G/A-G/G | 51 (40.5%) | 52 (50.0%) | 1.82 (0.92–3.60) | |||
| Recessive | A/A-G/A | 89 (70.6%) | 83 (79.8%) | 1.00 | 0.630 | |
| G/G | 37 (29.4%) | 21 (20.2%) | 0.83 (0.39–1.78) | |||
| Overdominant | A/A-G/G | 112 (88.9%) | 73 (70.2%) | 1.00 | 0.005 | |
| G/A | 14 (11.1%) | 31 (29.8%) | 3.46 (1.42–8.43) | |||
| Diabetes mellitus | Codominant | A/A | 69 (58.0%) | 52 (50.0%) | 1.00 | 0.002 |
| G/A | 14 (11.8%) | 31 (29.8%) | 3.00 (1.42–6.32) | |||
| G/G | 36 (30.2%) | 21 (20.2%) | 0.71 (0.36–1.41) | |||
| Dominant | A/A | 69 (58.0%) | 52 (50.0%) | 1.00 | 0.290 | |
| G/A-G/G | 50 (42.0%) | 52 (50.0%) | 1.35 (0.78–2.34) | |||
| Recessive | A/A-G/A | 83 (69.8%) | 83 (79.8%) | 1.00 | 0.056 | |
| G/G | 36 (30.2%) | 21 (20.2%) | 0.53 (0.28–1.03) | |||
| Overdominant | A/A-G/G | 105 (88.2%) | 73 (70.2%) | 1.00 | 0.001 | |
| G/A | 14 (11.8%) | 31 (29.8%) | 3.33 (1.62–6.82) | |||
| Arterial hypertension | Codominant | A/A | 69 (58.0%) | 52 (50.0%) | 1.00 | 0.015 |
| G/A | 14 (11.8%) | 31 (29.8%) | 2.50 (1.13–5.52) | |||
| G/G | 36 (30.2%) | 21 (20.2%) | 0.69 (0.34–1.41) | |||
| Dominant | A/A | 69 (58.0%) | 52 (50.0%) | 1.00 | 0.540 | |
| G/A-G/G | 50 (42.0%) | 52 (50.0%) | 1.20 (0.67–2.16) | |||
| Recessive | A/A-G/A | 83 (69.8%) | 83 (79.8%) | 1.00 | 0.077 | |
| G/G | 36 (30.2%) | 21 (20.2%) | 0.54 (0.27–1.08) | |||
| Overdominant | A/A-G/G | 105 (88.2%) | 73 (70.2%) | 1.00 | 0.007 | |
| G/A | 14 (11.8%) | 31 (29.8%) | 2.81 (1.31–6.01) | |||
| Endometrial thickness >5 mm | Codominant | A/A | 42 (51.2%) | 43 (47.2%) | 1.00 | 0.075 |
| G/A | 12 (14.6%) | 28 (30.8%) | 1.96 (0.87–4.45) | |||
| G/G | 28 (34.1%) | 20 (22.0%) | 0.70 (0.34–1.46) | |||
| Dominant | A/A | 42 (51.2%) | 43 (47.2%) | 1.00 | 0.760 | |
| G/A-G/G | 40 (48.8%) | 48 (52.8%) | 1.10 (0.60–2.03) | |||
| Recessive | A/A-G/A | 54 (65.8%) | 71 (78.0%) | 1.00 | 0.120 | |
| G/G | 28 (34.1%) | 20 (22.0%) | 0.57 (0.29–1.15) | |||
| Overdominant | A/A-G/G | 70 (85.4%) | 63 (69.2%) | 1.00 | 0.038 | |
| G/A | 12 (14.6%) | 28 (30.8%) | 2.23 (1.03–4.83) | |||
| Alleles in CCL5 SNPs a | Haplotype Prevalence | OR b (95% CI c) | p-Value d | ||
|---|---|---|---|---|---|
| −403 G>A | 351 A>G | Endometrial Cancer | Non-Cancerous Controls | ||
| G | A | 0.696 | 0.801 | 1.00 | |
| A | A | 0.225 | 0.116 | 1.84 (1.21–2.81) | 0.005 |
| A | G | 0.068 | 0.072 | 1.09 (0.55–2.15) | 0.800 |
| G | G | 0.010 | 0.012 | 0.93 (0.15–5.77) | 0.940 |
| Alleles in CCL2 and CCL5 SNPs a | Haplotype Prevalence | OR b (95% CI c) | p-Value d | |||
|---|---|---|---|---|---|---|
| CCL2 903 T>C | CCL5 | Endometrial Cancer | Non-Cancerous Controls | |||
| −403 G>A | 351 A>G | |||||
| T | G | A | 0.613 | 0.720 | 1.00 | |
| T | A | A | 0.190 | 0.108 | 1.71 (1.10–2.65) | 0.017 |
| C | G | A | 0.084 | 0.081 | 1.06 (0.64–1.77) | 0.820 |
| T | A | G | 0.068 | 0.063 | 1.24 (0.62–2.51) | 0.540 |
| C | A | A | 0.036 | 0.008 | 4.10 (0.90–18.66) | 0.069 |
| Gene Polymorphism | Allele | No. a of Carriers with Specific Alleles (%) | p-Value b | |
|---|---|---|---|---|
| Endometrial Cancer | Non-Cancerous Controls | |||
| CCL2 | T | 228 (87.7%) | 269 (90.3%) | 0.331 |
| 903 T>C | C | 32 (12.3%) | 29 (9.7%) | |
| CCL5 | G | 173 (70.3%) | 242 (81.2%) | 0.003 |
| −403 G>A | A | 73 (29.7%) | 56 (18.8%) | |
| CCL5 | A | 234 (92.1%) | 273 (91.6%) | 0.825 |
| 351 A>G | G | 20 (7.9%) | 25 (8.4%) | |
| IL8 | T | 259 (99.6%) | 299 (99.7%) | 0.919 |
| −738 T>A | A | 1 (0.4%) | 1 (0.3%) | |
| CXCR2 | G | 95 (37.7%) | 110 (36.9%) | 0.849 |
| 1440 G>A | A | 157 (62.3%) | 188 (63.1%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wujcicka, W.I.; Zając, A.; Szyłło, K.; Romanowicz, H.; Smolarz, B.; Stachowiak, G. Associations between Single Nucleotide Polymorphisms from the Genes of Chemokines and the CXCR2 Chemokine Receptor and an Increased Risk of Endometrial Cancer. Cancers 2023, 15, 5416. https://doi.org/10.3390/cancers15225416
Wujcicka WI, Zając A, Szyłło K, Romanowicz H, Smolarz B, Stachowiak G. Associations between Single Nucleotide Polymorphisms from the Genes of Chemokines and the CXCR2 Chemokine Receptor and an Increased Risk of Endometrial Cancer. Cancers. 2023; 15(22):5416. https://doi.org/10.3390/cancers15225416
Chicago/Turabian StyleWujcicka, Wioletta Izabela, Agnieszka Zając, Krzysztof Szyłło, Hanna Romanowicz, Beata Smolarz, and Grzegorz Stachowiak. 2023. "Associations between Single Nucleotide Polymorphisms from the Genes of Chemokines and the CXCR2 Chemokine Receptor and an Increased Risk of Endometrial Cancer" Cancers 15, no. 22: 5416. https://doi.org/10.3390/cancers15225416
APA StyleWujcicka, W. I., Zając, A., Szyłło, K., Romanowicz, H., Smolarz, B., & Stachowiak, G. (2023). Associations between Single Nucleotide Polymorphisms from the Genes of Chemokines and the CXCR2 Chemokine Receptor and an Increased Risk of Endometrial Cancer. Cancers, 15(22), 5416. https://doi.org/10.3390/cancers15225416