
Characterization of Age-Associated, Neutrophil-to-Lymphocyte Ratio (NLR) and Systemic Immune-Inflammatory Index (SII) as Biomarkers of Inflammation in Geriatric Patients with Cancer Treated with Immune Checkpoint Inhibitors: Impact on Efficacy and Survival

 , ,
, ,  ,
,  , , ,
, , ,  , ,
, ,  , ,
, ,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design and Data Sources
2.2. Outcomes and Statistical Analysis
3. Results
3.1. Patient Characteristics
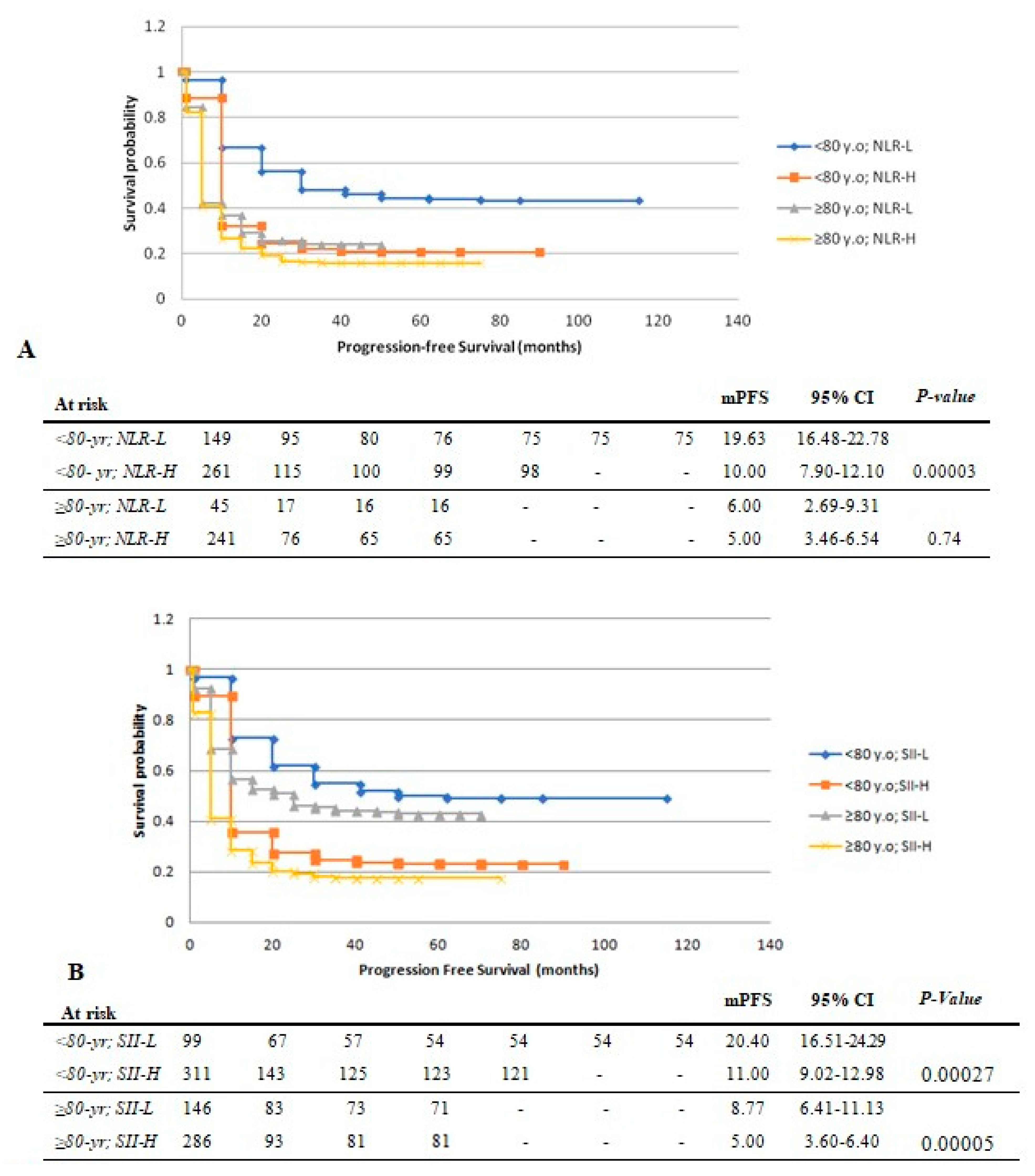
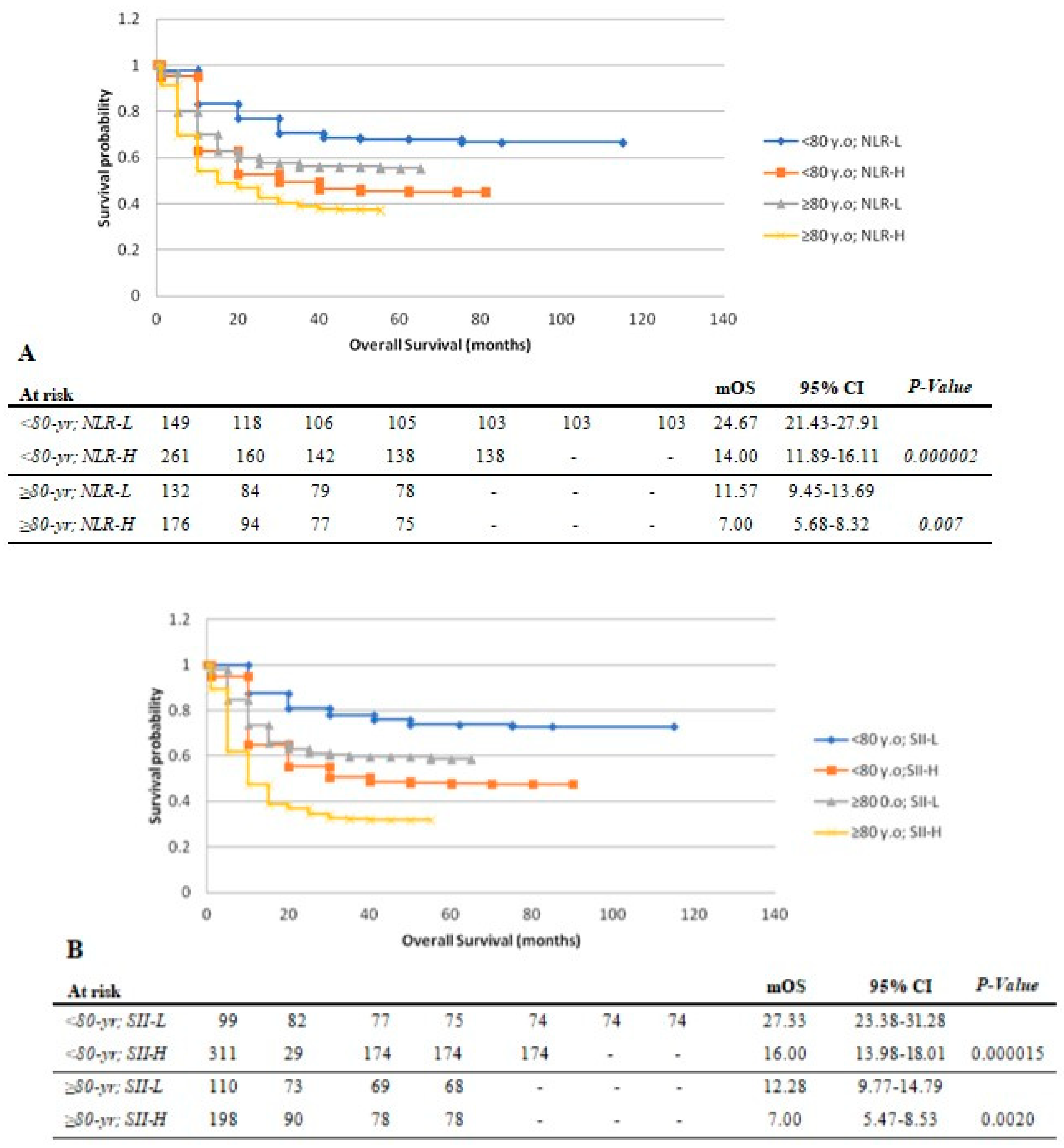
3.2. Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Robert, C. A Decade of Immune-Checkpoint Inhibitors in Cancer Therapy. Nat. Commun. 2020, 11, 3801. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Kanapuru, B.; Smith, C.; Fashoyin-Aje, L.A.; Myers, A.; Kim, G.; Pazdur, R. FDA Analysis of Enrollment of Older Adults in Clinical Trials for Cancer Drug Registration: A 10-Year Experience by the U.S. Food and Drug Administration. JCO 2017, 35, 10009. [Google Scholar] [CrossRef]
- Nebhan, C.A.; Cortellini, A.; Ma, W.; Ganta, T.; Song, H.; Ye, F.; Irlmeier, R.; Debnath, N.; Saeed, A.; Radford, M.; et al. Clinical Outcomes and Toxic Effects of Single-Agent Immune Checkpoint Inhibitors Among Patients Aged 80 Years or Older with Cancer: A Multicenter International Cohort Study. JAMA Oncol. 2021, 7, 1856–1861. [Google Scholar] [CrossRef] [PubMed]
- Martins, F.; Sofiya, L.; Sykiotis, G.P.; Lamine, F.; Maillard, M.; Fraga, M.; Shabafrouz, K.; Ribi, C.; Cairoli, A.; Guex-Crosier, Y.; et al. Adverse Effects of Immune-Checkpoint Inhibitors: Epidemiology, Management and Surveillance. Nat. Rev. Clin. Oncol. 2019, 16, 563–580. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.Y.; Salem, J.-E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; Zhao, S.; Das, S.; Beckermann, K.E.; Ha, L.; et al. Fatal Toxic Effects Associated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. JAMA Oncol. 2018, 4, 1721. [Google Scholar] [CrossRef] [PubMed]
- Bagchi, S.; Yuan, R.; Engleman, E.G. Immune Checkpoint Inhibitors for the Treatment of Cancer: Clinical Impact and Mechanisms of Response and Resistance. Annu. Rev. Pathol. Mech. Dis. 2021, 16, 223–249. [Google Scholar] [CrossRef] [PubMed]
- Nikolich-Žugich, J. The Twilight of Immunity: Emerging Concepts in Aging of the Immune System. Nat. Immunol. 2018, 19, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Nishijima, T.F.; Muss, H.B.; Shachar, S.S.; Moschos, S.J. Comparison of Efficacy of Immune Checkpoint Inhibitors (ICIs) between Younger and Older Patients: A Systematic Review and Meta-Analysis. Cancer Treat. Rev. 2016, 45, 30–37. [Google Scholar] [CrossRef]
- Fulop, T.; Le Page, A.; Fortin, C.; Witkowski, J.M.; Dupuis, G.; Larbi, A. Cellular Signaling in the Aging Immune System. Curr. Opin. Immunol. 2014, 29, 105–111. [Google Scholar] [CrossRef]
- Franceschi, C.; Bonafè, M.; Valensin, S. Human Immunosenescence: The Prevailing of Innate Immunity, the Failing of Clonotypic Immunity, and the Filling of Immunological Space. Vaccine 2000, 18, 1717–1720. [Google Scholar] [CrossRef]
- Wyczalkowska-Tomasik, A.; Czarkowska-Paczek, B.; Zielenkiewicz, M.; Paczek, L. Inflammatory Markers Change with Age, but Do Not Fall Beyond Reported Normal Ranges. Arch. Immunol. Ther. Exp. 2016, 64, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Bonafè, M.; Valensin, S.; Olivieri, F.; De Luca, M.; Ottaviani, E.; De Benedictis, G. Inflamm-Aging: An Evolutionary Perspective on Immunosenescence. Ann. N. Y. Acad. Sci. 2006, 908, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Campisi, J. Chronic Inflammation (Inflammaging) and Its Potential Contribution to Age-Associated Diseases. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69, S4–S9. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Garagnani, P.; Parini, P.; Giuliani, C.; Santoro, A. Inflammaging: A new immune–metabolic viewpoint for age-related diseases. Nat. Rev. Endocrinol. 2018, 14, 576–590. [Google Scholar] [CrossRef]
- Pardoll, D.M. The Blockade of Immune Checkpoints in Cancer Immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Llosa, N.J.; Cruise, M.; Tam, A.; Wicks, E.C.; Hechenbleikner, E.M.; Taube, J.M.; Blosser, R.L.; Fan, H.; Wang, H.; Luber, B.S.; et al. The Vigorous Immune Microenvironment of Microsatellite Instable Colon Cancer Is Balanced by Multiple Counter-Inhibitory Checkpoints. Cancer Discov. 2015, 5, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Kugel, C.H.; Douglass, S.M.; Webster, M.R.; Kaur, A.; Liu, Q.; Yin, X.; Weiss, S.A.; Darvishian, F.; Al-Rohil, R.N.; Ndoye, A.; et al. Age Correlates with Response to Anti-PD1, Reflecting Age-Related Differences in Intratumoral Effector and Regulatory T-Cell Populations. Clin. Cancer Res. 2018, 24, 5347–5356. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, A.G.; Wages, N.A.; Hu, Y.; Smolkin, M.E.; Slingluff, C.L. Defining the Effects of Age and Gender on Immune Response and Outcomes to Melanoma Vaccination: A Retrospective Analysis of a Single-Institution Clinical Trials’ Experience. Cancer Immunol. Immunother. 2015, 64, 1531–1539. [Google Scholar] [CrossRef]
- Grotz, T.E.; Vaince, F.; Hieken, T.J. Tumor-Infiltrating Lymphocyte Response in Cutaneous Melanoma in the Elderly Predicts Clinical Outcomes. Melanoma Res. 2013, 23, 132–137. [Google Scholar] [CrossRef]
- Lalani, A.-K.A.; Xie, W.; Martini, D.J.; Steinharter, J.A.; Norton, C.K.; Krajewski, K.M.; Duquette, A.; Bossé, D.; Bellmunt, J.; Van Allen, E.M.; et al. Change in Neutrophil-to-Lymphocyte Ratio (NLR) in Response to Immune Checkpoint Blockade for Metastatic Renal Cell Carcinoma. J. Immunother. Cancer 2018, 6, 5. [Google Scholar] [CrossRef]
- Guo, Y.; Xiang, D.; Wan, J.; Yang, L.; Zheng, C. Focus on the Dynamics of Neutrophil-to-Lymphocyte Ratio in Cancer Patients Treated with Immune Checkpoint Inhibitors: A Meta-Analysis and Systematic Review. Cancers 2022, 14, 5297. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Li, Y.; Chen, P.; Xu, W.; Wu, Y.; Che, G. Prognostic Value of the Pretreatment Systemic Immune-Inflammation Index (SII) in Patients with Non-Small Cell Lung Cancer: A Meta-Analysis. Ann. Transl. Med. 2019, 7, 433. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-G.; Chang, H.; Keam, B.; Chun, S.H.; Park, J.; Park, K.U.; Shin, S.H.; An, H.J.; Lee, K.E.; Lee, K.-W.; et al. Outcomes and Biomarkers of Immune Checkpoint Inhibitor Therapy in Patients with Refractory Head and Neck Squamous Cell Carcinoma: KCSG HN18-12. Cancer Res. Treat. 2021, 53, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, A.; Ricciuti, B.; Borghaei, H.; Naqash, A.R.; D’Alessio, A.; Fulgenzi, C.A.M.; Addeo, A.; Banna, G.L.; Pinato, D.J. Differential Prognostic Effect of Systemic Inflammation in Patients with Non–Small Cell Lung Cancer Treated with Immunotherapy or Chemotherapy: A Post Hoc Analysis of the Phase 3 OAK Trial. Cancer 2022, 128, 3067–3079. [Google Scholar] [CrossRef] [PubMed]
- Muhammed, A.; Fulgenzi, C.A.M.; Dharmapuri, S.; Pinter, M.; Balcar, L.; Scheiner, B.; Marron, T.U.; Jun, T.; Saeed, A.; Hildebrand, H.; et al. The Systemic Inflammatory Response Identifies Patients with Adverse Clinical Outcome from Immunotherapy in Hepatocellular Carcinoma. Cancers 2021, 14, 186. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Li, S.; Zhang, S.; Liu, Y.; Ma, L.; Zhu, J.; Xin, Y.; Wang, Y.; Yang, C.; Cheng, Y. Systemic Immune-inflammation Index, Neutrophil-to-lymphocyte Ratio, Platelet-to-lymphocyte Ratio Can Predict Clinical Outcomes in Patients with Metastatic Non-small-cell Lung Cancer Treated with Nivolumab. J. Clin. Lab. Anal. 2019, 33, e22964. [Google Scholar] [CrossRef] [PubMed]
- De Giorgi, U.; Procopio, G.; Giannarelli, D.; Sabbatini, R.; Bearz, A.; Buti, S.; Basso, U.; Mitterer, M.; Ortega, C.; Bidoli, P.; et al. Association of Systemic Inflammation Index and Body Mass Index with Survival in Patients with Renal Cell Cancer Treated with Nivolumab. Clin. Cancer Res. 2019, 25, 3839–3846. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-H.; Zhai, E.-T.; Yuan, Y.-J.; Wu, K.-M.; Xu, J.-B.; Peng, J.-J.; Chen, C.-Q.; He, Y.-L.; Cai, S.-R. Systemic Immune-Inflammation Index for Predicting Prognosis of Colorectal Cancer. WJG 2017, 23, 6261. [Google Scholar] [CrossRef]
- Chen, L.; Kong, X.; Wang, Z.; Wang, X.; Fang, Y.; Wang, J. Pre-treatment Systemic Immune-inflammation Index Is a Useful Prognostic Indicator in Patients with Breast Cancer Undergoing Neoadjuvant Chemotherapy. J. Cell Mol. Med. 2020, 24, 2993–3021. [Google Scholar] [CrossRef]
- Wang, K.; Diao, F.; Ye, Z.; Zhang, X.; Zhai, E.; Ren, H.; Li, T.; Wu, H.; He, Y.; Cai, S.; et al. Prognostic Value of Systemic Immune-Inflammation Index in Patients with Gastric Cancer. Chin. J. Cancer 2017, 36, 75. [Google Scholar] [CrossRef]
- Yang, R.; Chang, Q.; Meng, X.; Gao, N.; Wang, W. Prognostic Value of Systemic Immune-Inflammation Index in Cancer: A Meta-Analysis. J. Cancer 2018, 9, 3295–3302. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| <80 Years | ≥80 Years | Overall | p-Value | |
|---|---|---|---|---|
| Number of Patients (N) | 417 | 468 | 885 | - |
| Age (years) at ICI start, median (range) | 65.0 (16.0–79.9) | 82.8 (80.0–94.6) | 80.0 (16.0–94.6) | <0.001 |
| Sex (n = 697; %) | 0.012 | |||
| M | 141/244 (57.8) | 305/453 (67.3) | 446/697 (64.0) | |
| F | 103/244 (42.2) | 148/453 (32.7) | 251/697 (36.0) | |
| ECOG (n = 743; %) | <0.001 | |||
| 0–1 | 275/296 (92.9) | 363/447 (81.2) | 638/743 (85.87) | |
| 2 | 20/296 (6.76) | 70/447 (15.67) | 90/743 (12.11) | |
| >2 | 1/296 (0.34) | 14/447 (3.16) | 15/743 (2.02) | |
| Tumor types, N (%) | <0.001 | |||
| Melanoma | 118 (28.3) | 205 (43.80) | 323 (36.5) | |
| NSCLC | 282 (67.62) | 220 (47) | 502 (56.72) | |
| SCLC | 15 (3.60) | 2 (0.43) | 17 (1.92) | |
| RCC | 1 (0.24) | 9 (1.92) | 10 (1.13) | |
| Bladder/GU | 1 (0.24) | 21 (4.49) | 22 (2.49) | |
| Tongue/Larynx/glottis | - | 3 (0.64) | 3 (0.34) | |
| Gastric/esophageal | - | 3 (0.64) | 3 (0.34) | |
| HCC | - | 3 (0.64) | 3 (0.34) | |
| Sarcoma | - | 2 (0.44) | 2 (0.22) | |
| Stage (n = 882; %) | 0.123 | |||
| I | 7/414 (1.69) | 10/468 (2.14) | 17 (1.93) | |
| II | 11/414 (2.90) | 21/468 (4.49) | 33 (3.74) | |
| IIIA | 47/414 (11.35) | 34/468 (7.26) | 81 (9.18) | |
| IIIB/C | 46/414 (11.11) | 44/468 (9.4) | 90 (10.2) | |
| IV | 302/414 (72.95) | 359/468 (76.71) | 661 (74.95) | |
| Prior lines of therapy (n = 749; %) | 0.028 | |||
| 0 | 176/296 (59.46) | 249/453 (54.97) | 425/749 (56.74) | |
| 1 | 106/296 (35.81) | 155/453 (34.22) | 261/749 (34.85) | |
| 2 | 9/296 (3.04) | 30/453 (6.62) | 39/749 (5.21) | |
| ≥3 | 5/296 (1.69) | 19/453 (4.19) | 24/749 (3.20) | |
| ICI (n = 696; %) | <0.001 | |||
| Pembrolizumab | 100/244 (40.98) | 227/452 (50.22) | 327/696 (46.99) | |
| Ipilimumab | 4/244 (1.64) | 17/452 (3.76) | 21/696 (3.02) | |
| Nivolumab | 79/244 (32.38) | 160/452 (35.40) | 239/696 (34.34) | |
| Atezolizumab | 15/244 (6.15) | 19/452 (4.20) | 34/696 (4.88) | |
| Avelumab | 1/244 (0.41) | 0 | 1/696 (0.14) | |
| Durvalumab | 36/244 (14.75) | 7/452 (1.55) | 43/696 (6.18) | |
| Cemiplimab | 0 | 3/452 (0.67) | 3/696 (0.43) | |
| ICI combination | 9/244 (3.69) | 19/452 (4.20) | 28/696 (4.02) | |
| Time (months) on ICI, median (range) | <0.001 | |||
| (n = 697) | 11.0 (1.0–82) | 4.55 (1.0–61.4) | 7.50 (1.0–82.0) | |
| Overall (n = 885) | <80 Years (n = 417) | ≥80 Years (n = 468) | ||
|---|---|---|---|---|
| mOS (months; [95% CI]) | 12.88 [11.74–14.02] | 14.30 [12.62–15.98] | 12.80 [11.23–14.37] | |
| mPFS (months; [95% CI]) | 8.60 [7.52–9.68] | 9.33 [7.73–10.93] | 8.33 [6.84–9.82] | |
| p-value | ||||
| ORR, (n = 638), (%) | 229/638 (35.89) | 114/237 (48.1) | 115/401 (28.68) | <0.001 |
| CR | 53 (8.31) | 14 (5.91) | 39 (9.73) | |
| PR | 176 (27.59) | 100 (42.19) | 76 (18.95) |
| Hazard Ratio (HR) for OS | Hazard Ratio (HR) for PFS | |||
|---|---|---|---|---|
| Characteristic | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Age at ICI initiation < 80 (vs. ≥80) | 0.26 (0.19–0.33) | <0.001 | 0.4 (0.31–0.51) | <0.001 |
| Sex: male (vs. female) | 1.27 (1.01–1.61) | 0.044 | 1.12 (0.9–1.4) | 0.298 |
| ECOG < 2 (vs. ≥2) | 0.58 (0.44–0.77) | <0.001 | 0.65 (0.5–0.86) | 0.002 |
| Tumor type NSCLC (vs. MEL + others) | 1.1 (0.2–8.0) | 0.91 | 1.3 (0.3–5.0) | 0.75 |
| MEL (vs. NSCLC + others) | 0.5 (0.1–3.8) | 0.52 | 1.2 (0.30–4.9) | 0.78 |
| Others (vs. NSCLC + MEL) | 1.8 (0.2–13.1) | 0.56 | 1.9 (0.5–8.0) | 0.37 |
| Stage < IIIB (vs. IIIB-IV) | 0.64 (0.46–0.89) | 0.008 | 0.51 (0.37–0.71) | <0.001 |
| ICI: anti-PD1/PDL1 (vs. non-PD1/L-1) | 0.85 (0.57–1.26) | 0.414 | 0.92 (0.62–1.38) | 0.69 |
| NLR ≤ 3 (vs. >3) | 0.89 (0.63–1.24) | 0.479 | 0.82 (0.6–1.14) | 0.244 |
| SII ≤ 600 (vs. >600) | 0.62 (0.44–0.88) | 0.008 | 0.61 (0.43–0.86) | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choucair, K.; Nebhan, C.; Cortellini, A.; Hentzen, S.; Wang, Y.; Liu, C.; Giusti, R.; Filetti, M.; Ascierto, P.A.; Vanella, V.; et al. Characterization of Age-Associated, Neutrophil-to-Lymphocyte Ratio (NLR) and Systemic Immune-Inflammatory Index (SII) as Biomarkers of Inflammation in Geriatric Patients with Cancer Treated with Immune Checkpoint Inhibitors: Impact on Efficacy and Survival. Cancers 2023, 15, 5052. https://doi.org/10.3390/cancers15205052
Choucair K, Nebhan C, Cortellini A, Hentzen S, Wang Y, Liu C, Giusti R, Filetti M, Ascierto PA, Vanella V, et al. Characterization of Age-Associated, Neutrophil-to-Lymphocyte Ratio (NLR) and Systemic Immune-Inflammatory Index (SII) as Biomarkers of Inflammation in Geriatric Patients with Cancer Treated with Immune Checkpoint Inhibitors: Impact on Efficacy and Survival. Cancers. 2023; 15(20):5052. https://doi.org/10.3390/cancers15205052
Chicago/Turabian StyleChoucair, Khalil, Caroline Nebhan, Alessio Cortellini, Stijn Hentzen, Yinghong Wang, Cynthia Liu, Raffaele Giusti, Marco Filetti, Paolo Antonio Ascierto, Vito Vanella, and et al. 2023. "Characterization of Age-Associated, Neutrophil-to-Lymphocyte Ratio (NLR) and Systemic Immune-Inflammatory Index (SII) as Biomarkers of Inflammation in Geriatric Patients with Cancer Treated with Immune Checkpoint Inhibitors: Impact on Efficacy and Survival" Cancers 15, no. 20: 5052. https://doi.org/10.3390/cancers15205052
APA StyleChoucair, K., Nebhan, C., Cortellini, A., Hentzen, S., Wang, Y., Liu, C., Giusti, R., Filetti, M., Ascierto, P. A., Vanella, V., Galetta, D., Catino, A., Al-Bzour, N., Saeed, A., Cavalcante, L., Pizzutilo, P., Genova, C., Bersanelli, M., Buti, S., ... Saeed, A. (2023). Characterization of Age-Associated, Neutrophil-to-Lymphocyte Ratio (NLR) and Systemic Immune-Inflammatory Index (SII) as Biomarkers of Inflammation in Geriatric Patients with Cancer Treated with Immune Checkpoint Inhibitors: Impact on Efficacy and Survival. Cancers, 15(20), 5052. https://doi.org/10.3390/cancers15205052