
Oncological Efficacy of Robotic Nephroureterectomy vs. Open and Laparoscopic Nephroureterectomy for Suspected Non-Metastatic UTUC—A Systematic Review and Meta-Analysis
 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Evidence Acquisition
2.1.1. Criteria for Considered Studies in This Review
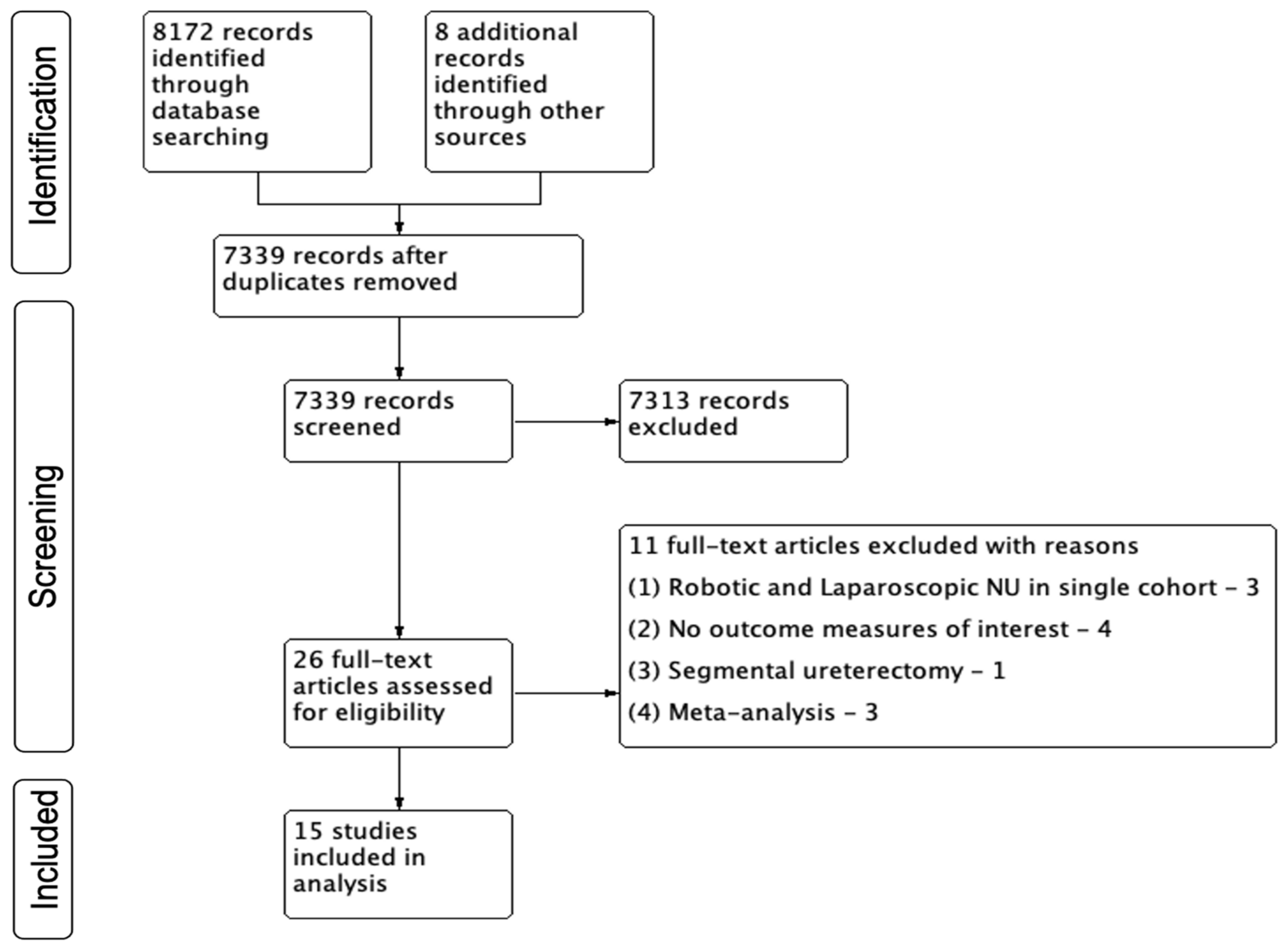
2.1.2. Search Strategy and Study Selection
2.2. Outcomes Measures
2.2.1. Primary—Time-to-Event Analysis
- Overall survival (OS);
- Cancer-specific survival (CSS);
- Disease-free survival (DFS);
- Intravesical recurrence-free survival (IV-RFS).
2.2.2. Secondary
- Lymph node dissection rates;
- Positive margin rates;
- Proportion of patients receiving bladder intra-vesical chemotherapy.
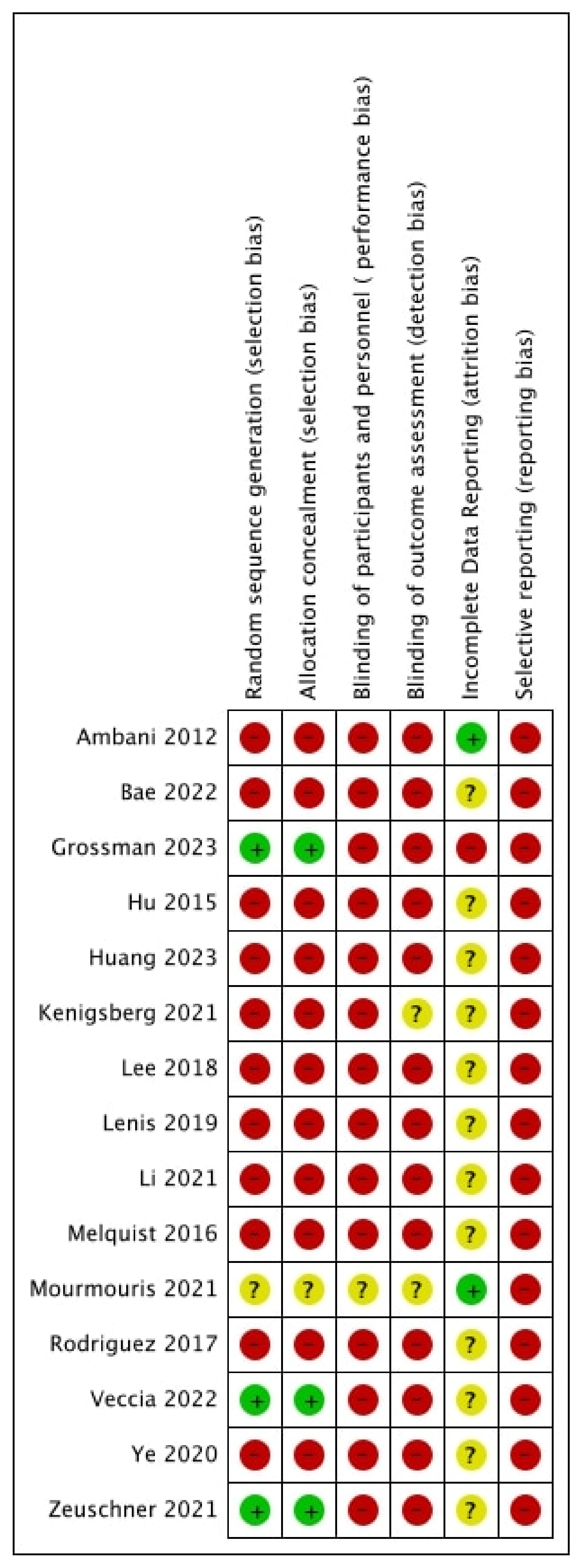
2.3. Quality Assessment of Evidence and Certainty of Outcomes
2.4. Data Extraction and Analysis
3. Results
3.1. Primary Outcome: Time-to-Event Analysis (Table 4)
3.1.1. Overall Survival (OS) (Figure 2)
- RNU vs. LNU

| Author | Follow-Up (Months) | Survival Outcomes |
|---|---|---|
| Rodriguez et al. 2017 [16] | ND | ONU vs. RNU—HR, CI, p-value OS RNU—0.88, (0.71–1.09), p = 0.227 |
| Lee et al., 2019 [17] (included in SR) | RNU vs. LNU vs. ONU 23.7 ± 2.1 vs. 38.1 ± 3.3 vs. 41.7 ± 3.3 (p < 0.001) (Mean, SD) | Multivariate analysis: ONU vs. RNU (HR (95% CI), p-value) Intravesical recurrence-free survival (IV-RFS)—0.665 (0.405–1.092), 0.107; Overall mortality—0.335 (0.097–1.158), 0.084; Cancer-specific mortality—0.336 (0.070–1.607), 0.172; Disease-free survival (DFS)—0.574 (0.276–1.325), 0.326. Multivariate Cox proportional hazard analyses were used to reveal the predictors of postoperative survival outcomes using the following covariates: age, sex, BMI, ECOG score, T stage, tumor size, tumor grade, Charlson’s comorbidity index, multifocality of the tumor, lymphadenectomy, and lymph node invasion. |
| Ye et al. 2020 [19] Balanced for - Primary grade and clinical stage; - Location of the tumor; - Previous ureteroscopy; - No data on other confounders. | RNU vs. LNU 40.5 vs. 40.4 (Median) | RNU vs. LNU 5-year OS 67.4% vs. 84.0%, (p = 0.524); 5-year CSS 71.2% vs. 84.7%, (p = 0.728); 5-year IV-RFS 88.0% vs. 85.5%, (p = 0.611); 5-year retroperitoneal recurrence-free survival (77.3% vs. 87.7%, p = 0.737); 5-year metastasis-free survival (93.1% vs. 96.7%, p = 0.323). |
| Kenigsberg et al. 2021 [20] (included in SR) | RNU vs. LNU 33.3 vs. 35.1 (p = 0.063) (Mean) | RNU vs. LNU Kaplan–Meier survival analysis Median OS—71.1 months vs. 62.6 months, p = 0.033 Multivariate analysis All-cause mortality LNU worse than RNU → HR- 1.182, 95% CI 1.016–1.375, p = 0.030 Multivariate Cox proportional hazard analyses were used to reveal the predictors of postoperative survival outcomes using the following covariates: age, sex, year of diagnosis, Charlson’s comorbidity index, cellular grade, ECOG score, T stage, N stage, positive surgical margin, lymphadenectomy, neoadjuvant chemotherapy. |
| Li et al. 2021 [21] | ND | Hand-assisted LNU vs. LNU vs. RNU 5-year OS 71% 74% vs. 82% (p = 0.010); 5-year CSS 80% vs. 86% vs. 87% (p = 0.037). Hand-assisted LNU vs. RNU—multivariate analysis, HR (95%CI), p-value OS—0.534 (0.318, 0.896), p = 0.018; CSS 0.730 (0.413, 1.290), p = 0.279; IV-RFS 1.082 (0.751, 1.558), p = 0.673. Multivariate Cox proportional hazard analyses were used to reveal the predictors of postoperative survival outcomes using the following covariates: age, sex, stage of chronic kidney disease, cytology, history of bladder cancer, hydronephrosis, tumor location, tumor grade, tumor size, multifocality, ECOG score, T stage, N stage, histological variant, tumor necrosis. |
| Zeuschner et al. 2021 [23] Propensity matched analysis—balanced for - pT stage; - Tumor location; - Prior cystectomies. | Overall cohort 30.9 (1.4–129.5) (Median, range) | RNU vs. ONU 5-year OS 59.1% (39.0–74.5) vs. 46.9% (27.9–64.5) p = 0.087; 5-year progression-free survival (PFS) 47.9% (27.8–65.4) vs. 38.0% (20.5–55.4) p = 0.132. No difference in OS and PFS between RNU and ONU in multivariate analysis. Multivariate Cox proportional hazard analyses were used to reveal the predictors of postoperative survival outcomes using the following covariates: age, sex, BMI, previous cystectomy, simultaneous cystectomy, bladder cuff excision, lymphadenectomy, locally advanced tumor, pR1, pN+. |
| Bae et al. 2022 [25] (included in SR) | RNU vs. LNU vs. ONU 22 ± 12.4 vs. 29.92 ± 15.3 vs. 32.4 ± 16.4 (p < 0.001) (Mean, SD) | RNU vs. LNU vs. ONU 3-year OS—92.1% vs. 90.4% vs. 91.8%, p = 0.819; 3-year DFS- 80.9% vs. 74.2% vs. 77.1%, p = 0.842. Multivariate Cox proportional hazards of robotic—reference vs. lap, open—HR (95% CI), p value PFS—1.45 (0.68–3.11), 1.29 (0.71–2.33), p = 0.580; CSS—0.98 (0.22–4.40), 1.12 (0.35–3.54), p = 0.970; OS—0.77 (0.18–3.30), 1.28 (0.45–3.61), p = 0.699. Multivariate Cox proportional hazard analyses were used to reveal the predictors of postoperative survival outcomes using the following covariates: age, pT staging ≥T3, pN+, positive surgical margin, presence of LVI, tumor grade III, adjuvant chemotherapy. |
| Grossmann et al. 2023 [26] (included in SR) | Overall cohort 32 (15–61) (Median, IQR) | RNU vs. LNU vs. ONU—(95% CI), p value 3-year OS—80.9%(73.8–88.6) vs. 75.1(69.3–81.2) vs. 76.9(71.4–82.7), p = 0.7; 3-year CSS—85.5%(79.1–92.5) vs. 84.1%(79.2–89.4) vs. 86.5 (81.9–91.3), p = 0.7; 3-year DFS—72.9%(66–80.6) vs. 77.6% (72.2–83.4) vs. 73.5% (67.9–79.7), p = 0.7; 3-year IV-RFS—58.9%(51.9–66.7) vs. 58.8(52.5–65.8) vs. 73.5(67.7–79.8)—Improved IV-RFS for open in pairwise log rank p < 0.001. Multivariate Cox regression, ONU vs. RNU—HR (95% CI), p value RFS → 1.03 (0.71–1.49), p = 0.9; IV-RFS → 1.73 (1.22–2.47), p = 0.002; CSS → 0.65 (0.39–1.10), p = 0.1; OS → 0.81 (0.55–1.19), p = 0.3. Multivariate Cox proportional hazard analyses were used to reveal the predictors of postoperative survival outcomes using the following covariates: age, ASA, BMI, sex, previous bladder cancer, hydronephrosis, tumor location, diagnostic ureteroscopy performed, neoadjuvant chemotherapy, year of surgery, perioperative intravesical chemotherapy, lymphadenectomy, T stage, tumor grade, variant histology, multifocality, number of lymph nodes removed, lymph node involvement, positive surgical margins, lymphovascular invasion, concomitant CIS, adjuvant chemotherapy, adjuvant radiotherapy. |
| Huang et al. 2023 [27] Balanced for - TNM stage; - Neo-adjuvant chemotherapy; - Prior bladder cancer; - Tumor location; - Body mass index; - ASA. | RNU vs. LNU 20 (8–37) vs. 29 (15–42.5), p = 0.006 (Median, IQR) | RNU vs. LNU 5-year OS 84.7% vs. 75%, p = 0.534; 5-year CSS 90.3% vs. 87.7%, p = 0.923; 5-year IV-RFS 62.9% vs. 65.2%, p = 0.363. |
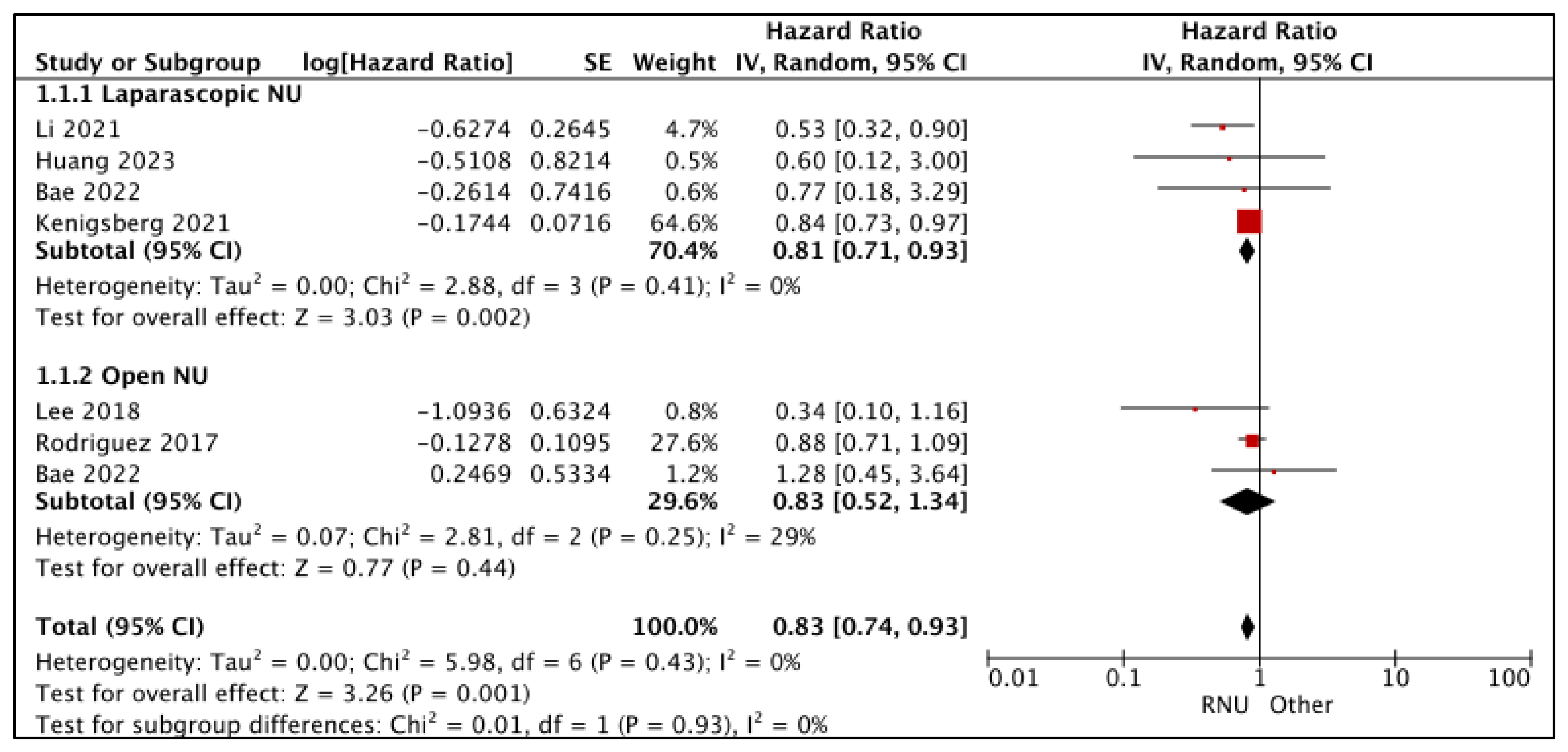
- RNU vs. ONU
3.1.2. Cancer-Specific Survival (CSS) (Figure 3)
- RNU vs. LNU
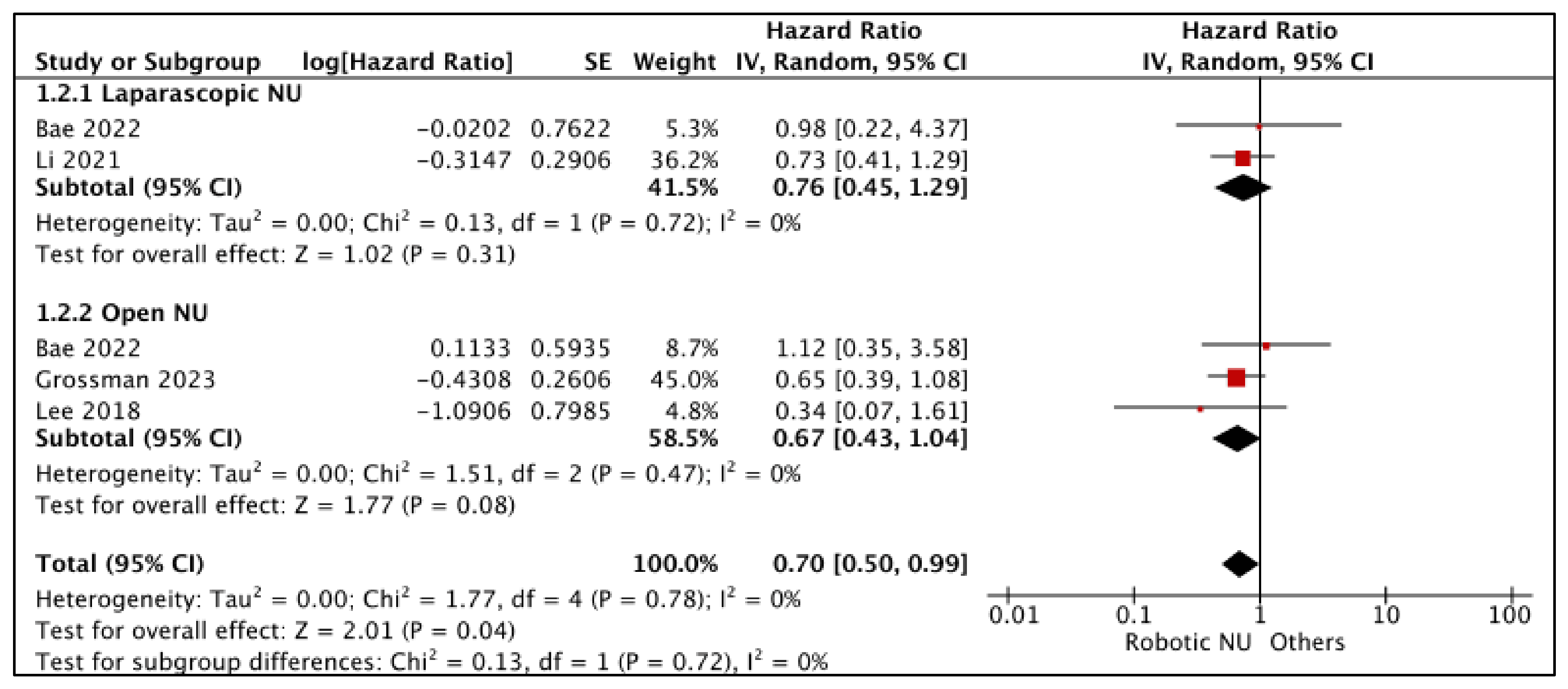
- RNU vs. ONU
3.1.3. Disease-Free Survival (DFS) (Figure 4)
- RNU vs. LNU
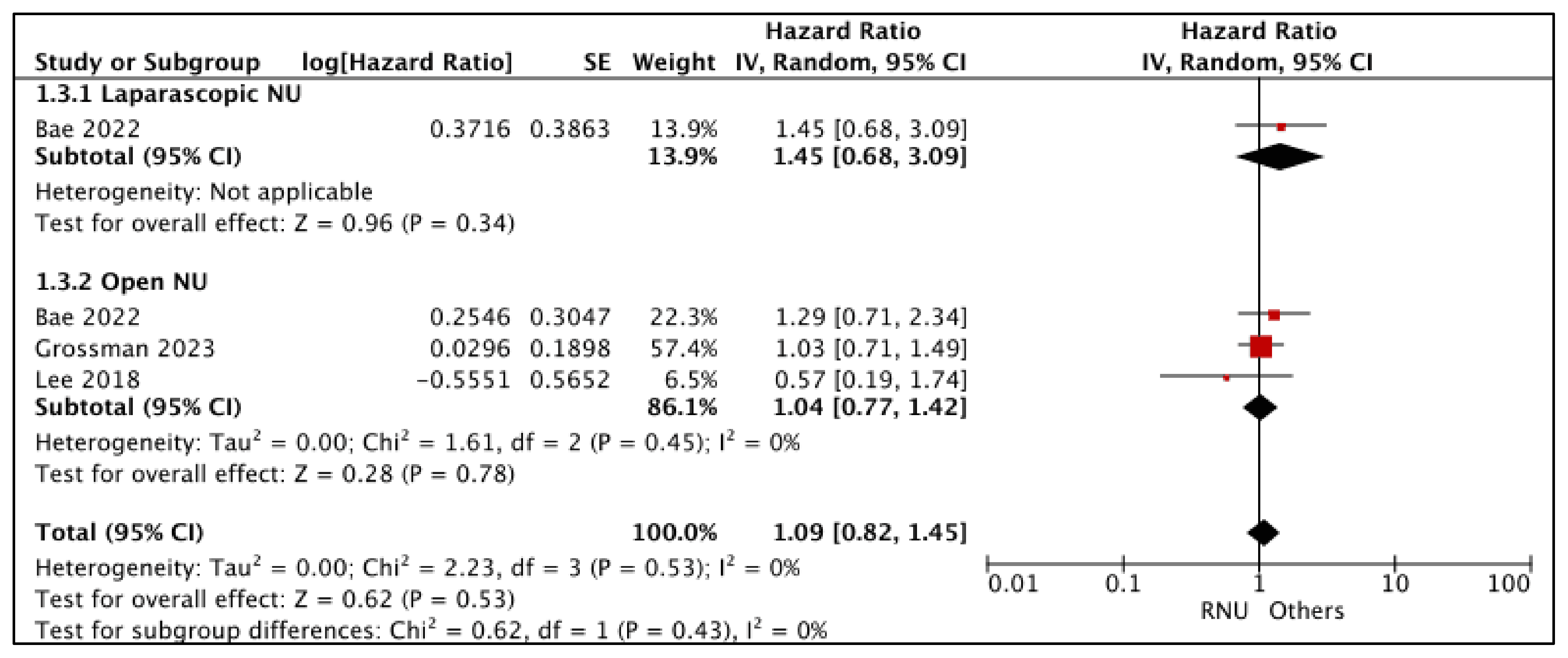
- RNU vs. ONU
3.1.4. Intravesical Recurrence-Free Survival (IV-RFS) (Figure 5)
- RNU vs. LNU
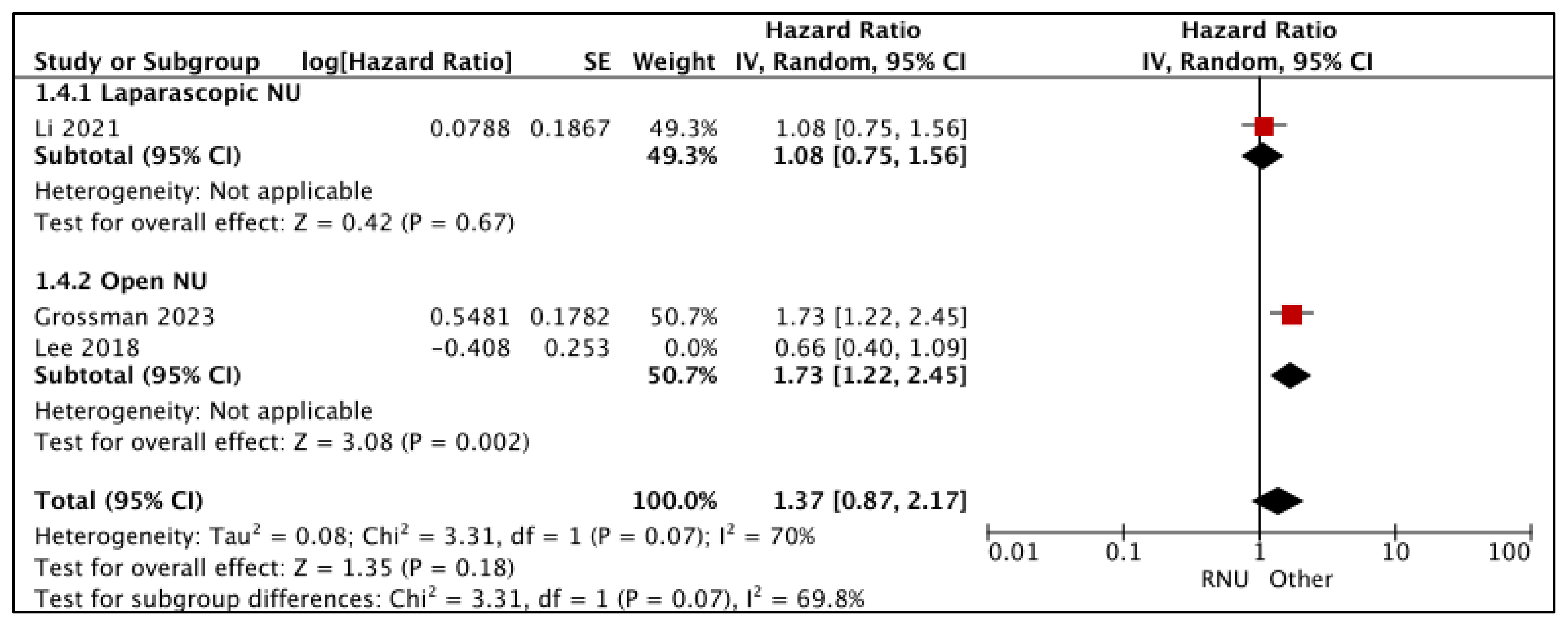
- RNU vs. ONU
3.2. Secondary Outcomes
3.2.1. Lymph Node Dissection Rates (LND) (Figure 6)
- RNU vs. LNU
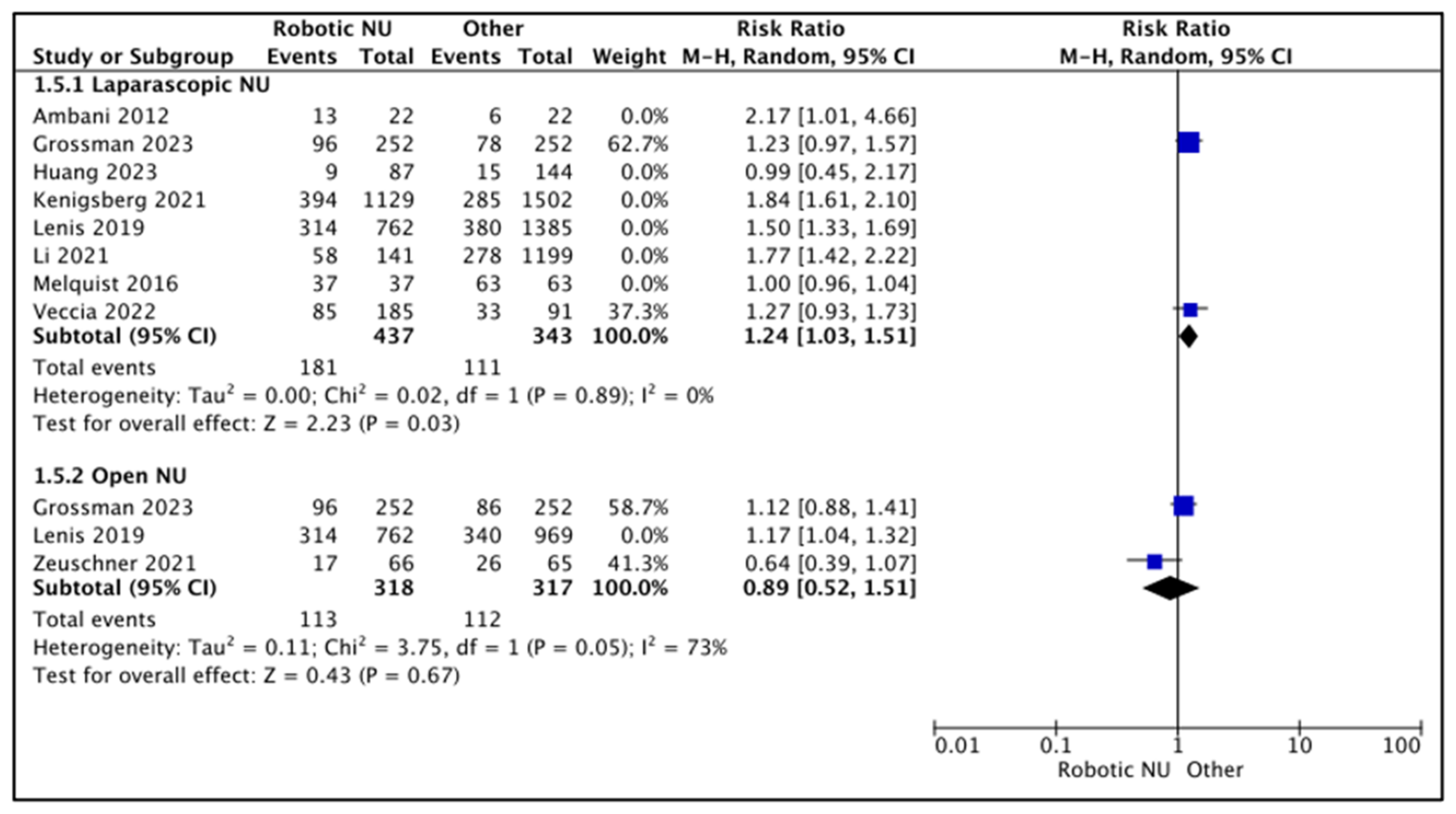
- RNU vs. ONU
3.2.2. Mean Lymph Node (LN) Count: (Figure 7)
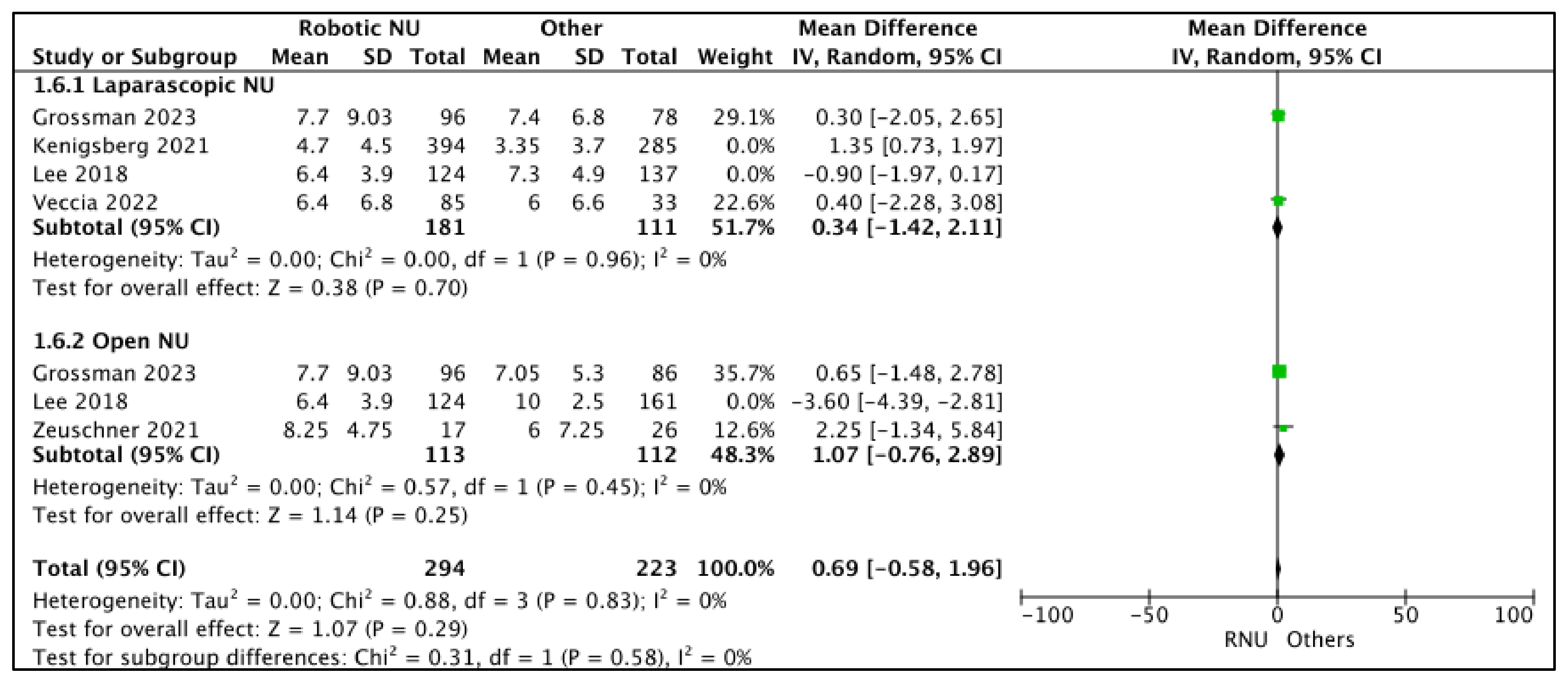
- RNU vs. LNU
- RNU vs. ONU
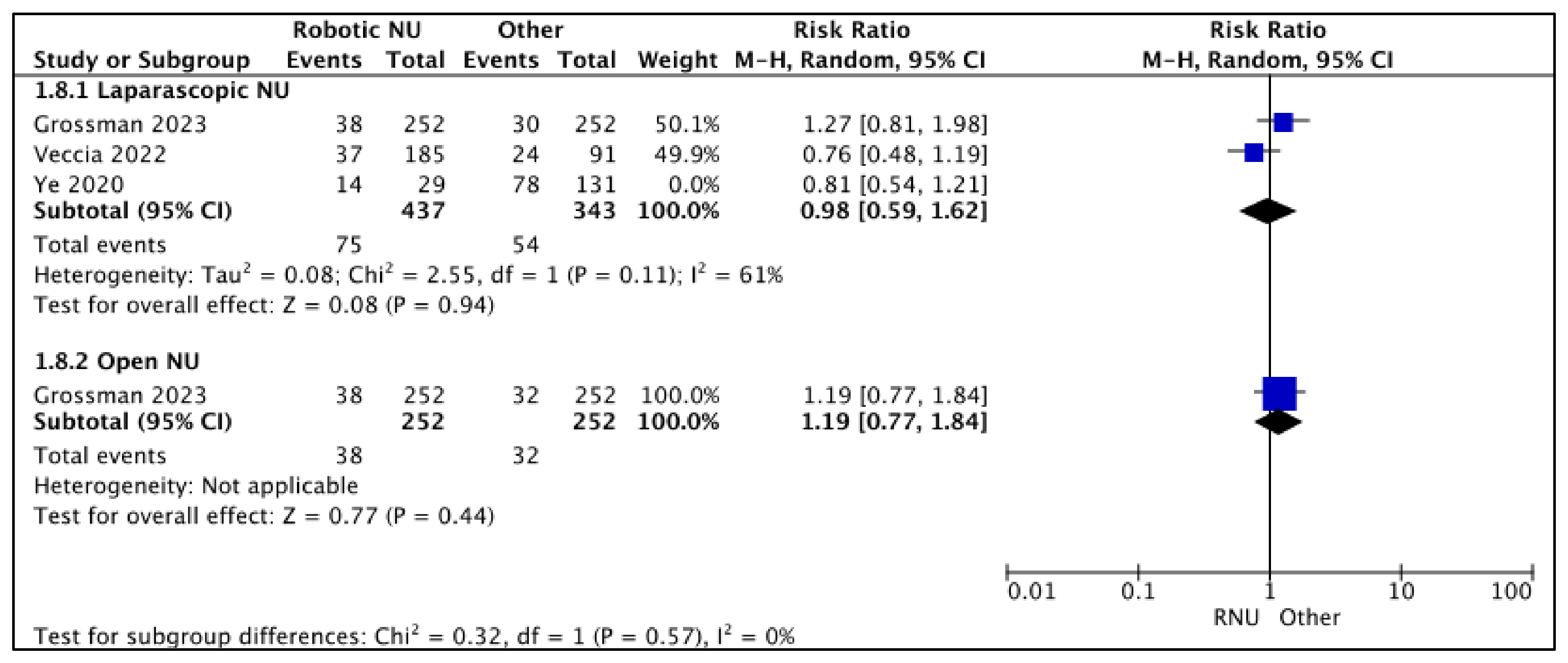
3.2.3. Positive Margin (PSM) Rates (Figure 8)
- RNU vs. LNU

- RNU vs. ONU
3.2.4. Post-NU Intravesical Chemotherapy Rates (Figure 9)
- RNU vs. LNU
- RNU vs. ONU
3.3. Quality of Evidence and Certainty of Outcomes (Figure 10, Table 5)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary and Secondary Outcomes Comparing RNU to ONU/LNU for Suspected UTUC | |||||
|---|---|---|---|---|---|
| Patient or Population: Patients with Suspected Non-Metastatic UTUC Setting: Hospital Intervention: RNU Comparison: LNU/ONU | |||||
| Outcomes | № of Participants (Studies) Follow-Up | Certainty of the Evidence (GRADE) | Relative Effect (95% CI) | Anticipated Absolute Effects | |
| Risk with Placebo | Risk Difference with Primary Outcomes | ||||
| Time-to-Event Analysis: Overall Survival—Laparoscopic NU | (4 observational studies) | ⨁◯◯◯ Very low a,b | HR 0.81 (0.71 to 0.93) | 0 per 1000 | -- per 1000 (-- to --) |
| Time-to-Event Analysis: Overall Survival—Open NU | (3 observational studies) | ⨁◯◯◯ Very low a,b | HR 0.83 (0.52 to 1.34) | 0 per 1000 | -- per 1000 (-- to --) |
| Time-to-Event Analysis: Cancer-Specific Survival—Laparoscopic NU | (2 observational studies) | ⨁◯◯◯ Very low a,b | HR 0.76 (0.45 to 1.29) | 0 per 1000 | -- per 1000 (-- to --) |
| Time-to-Event Analysis: Cancer-Specific Survival—Open NU | 285 (3 observational studies) | ⨁◯◯◯ Very low a,b | HR 0.67 (0.43 to 1.04) | 0 per 1000 | -- per 1000 (-- to --) |
| Time-to-Event Analysis: Disease-Free Survival—Laparoscopic NU | (1 observational study) | ⨁◯◯◯ Very low a,b,c | HR 1.45 (0.68 to 3.09) | 0 per 1000 | -- per 1000 (-- to --) |
| Time-to-Event Analysis: Disease-Free Analysis—Open NU | (3 observational studies) | ⨁◯◯◯ Very low a,b | HR 1.04 (0.77 to 1.42) | 0 per 1000 | -- per 1000 (-- to --) |
| Time-to-Event Analysis: Intravesical Recurrence-Free Survival—Laparoscopic NU | (1 observational study) | ⨁◯◯◯ Very low a,b | HR 1.08 (0.75 to 1.56) | 0 per 1000 | -- per 1000 (-- to --) |
| Time-to-Event Analysis: Intravesical Recurrence-Free Survival—Open NU | (1 observational study) | ⨁◯◯◯ Very low a,b | HR 1.73 (1.22 to 2.45) | 0 per 1000 | -- per 1000 (-- to --) |
| Lymphadenectomy Rates—Laparoscopic NU | 780 (2 observational studies) | ⨁⨁◯◯ Low a,b | RR 1.24 (1.03 to 1.51) | 324 per 1000 | 78 more per 1000 (10 more to 165 more) |
| Lymphadenectomy Rates—Open NU | 635 (2 observational studies) | ⨁◯◯◯ Very low a,b,d | RR 0.89 (0.52 to 1.51) | 353 per 1000 | 39 fewer per 1000 (170 fewer to 180 more) |
| Median Lymph Node Count—Laparoscopic NU | 292 (2 observational studies) | ⨁⨁◯◯ Low a,b | - | The mean median lymph node count—laparoscopic NU was 0 | MD 0.34 higher (1.42 lower to 2.11 higher) |
| Median Lymph Node Count—Open NU | 225 (2 observational studies) | ⨁⨁◯◯ Low a,b | - | The mean median lymph node count—open NU was 0 | MD 1.07 higher (0.76 lower to 2.89 higher) |
| Positive Margin Rates—Laparoscopic NU | 780 (2 observational studies) | ⨁⨁◯◯ Low a,b | RR 0.89 (0.38 to 2.09) | 32 per 1000 | 4 fewer per 1000 (20 fewer to 35 more) |
| Positive Margin Rates—Open NU | 635 (2 observational studies) | ⨁⨁◯◯ Low a,b | RR 0.26 (0.08 to 0.86) | 82 per 1000 | 61 fewer per 1000 (75 fewer to 11 fewer) |
| Proportion of Patients Receiving Intra-vesical Chemotherapy—Laparoscopic NU | 780 (2 observational studies) | ⨁◯◯◯ Very low a,b,c | RR 0.98 (0.59 to 1.62) | 157 per 1000 | 3 fewer per 1000 (65 fewer to 98 more) |
| Proportion of Patients Receiving Intra-vesical Chemotherapy—Open NU | 504 (1 observational study) | ⨁⨁◯◯ Low a,b | RR 1.19 (0.77 to 1.84) | 127 per 1000 | 24 more per 1000 (29 fewer to 107 more) |
| The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; HR: hazard ratio; MD: mean difference; RR: risk ratio. | |||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | |||||
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Rouprêt, M.; Seisen, T.; Birtle, A.J.; Capoun, O.; Compérat, E.M.; Dominguez-Escrig, J.L.; Gürses Andersson, I.; Liedberg, F.; Mariappan, P.; Hugh Mostafid, A.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2023 Update. Eur. Urol. 2023, 84, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Rai, B.P.; Shelley, M.; Coles, B.; Somani, B.; Nabi, G. Surgical management for upper urinary tract transitional cell carcinoma (UUT-TCC): A systematic review. BJU Int. 2012, 110, 1426–1435. [Google Scholar] [CrossRef] [PubMed]
- Simone, G.; Papalia, R.; Guaglianone, S.; Ferriero, M.; Leonardo, C.; Forastiere, E.; Gallucci, M. Laparoscopic versus open nephroureterectomy: Perioperative and oncologic outcomes from a randomised prospective study. Eur. Urol. 2009, 56, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Seisen, T.; Granger, B.; Colin, P.; Léon, P.; Utard, G.; Renard-Penna, R.; Compérat, E.; Mozer, P.; Cussenot, O.; Shariat, S.F.; et al. A Systematic Review and Meta-analysis of Clinicopathologic Factors Linked to Intravesical Recurrence After Radical Nephroureterectomy to Treat Upper Tract Urothelial Carcinoma. Eur. Urol. 2015, 67, 1122–1133. [Google Scholar] [CrossRef] [PubMed]
- Veccia, A.; Antonelli, A.; Francavilla, S.; Simeone, C.; Guruli, G.; Zargar, H.; Perdoná, S.; Ferro, M.; Carrieri, G.; Hampton, L.J.; et al. Robotic versus other nephroureterectomy techniques: A systematic review and meta-analysis of over 87,000 cases. World J. Urol. 2020, 38, 845–852. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; 2012 reprint. ed.; Wiley-Blackwell: Oxford, UK, 2008. [Google Scholar]
- Higgins, J.P.T.; Cochrane. Cochrane Handbook for Systematic Reviews of Interventions; Version 6 ed.; Cochrane: London, UK, 2019. [Google Scholar]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; Group, G.W. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- Ambani, S.N.; Weizer, A.Z.; Wolf, J.S.; He, C.; Miller, D.C.; Montgomery, J.S. Matched Comparison of Robotic vs Laparoscopic Nephroureterectomy: An Initial Experience. Urology 2014, 83, 345–349. [Google Scholar] [CrossRef]
- Hu, C.Y.; Yang, C.K.; Huang, C.Y.; Ou, Y.C.; Hung, S.F.; Chung, S.D.; Pu, Y.S. Robot-Assisted Laparoscopic Nephroureterectomy versus Hand-Assisted Laparoscopic Nephroureterectomy for Upper Urinary Tract Urothelial Carcinoma: A Matched Comparison Study. Biomed. Res. Int. 2015, 2015, 918486. [Google Scholar] [CrossRef] [PubMed]
- Melquist, J.J.; Redrow, G.; Delacroix, S.; Park, A.; Faria, E.E.; Karam, J.A.; Matin, S.F. Comparison of Single-docking Robotic-assisted and Traditional Laparoscopy for Retroperitoneal Lymph Node Dissection During Nephroureterectomy With Bladder Cuff Excision for Upper-tract Urothelial Carcinoma. Urology 2016, 87, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.F.; Packiam, V.T.; Boysen, W.R.; Johnson, S.C.; Smith, Z.L.; Smith, N.D.; Shalhav, A.L.; Steinberg, G.D. Utilization and Outcomes of Nephroureterectomy for Upper Tract Urothelial Carcinoma by Surgical Approach. J. Endourol. 2017, 31, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Kim, H.J.; Lee, S.E.; Hong, S.K.; Byun, S.S. Comparison of oncological and perioperative outcomes of open, laparoscopic, and robotic nephroureterectomy approaches in patients with non-metastatic upper-tract urothelial carcinoma. PLoS ONE 2019, 14, e0210401. [Google Scholar] [CrossRef] [PubMed]
- Lenis, A.T.; Donin, N.M.; Faiena, I.; Salmasi, A.; Johnson, D.C.; Drakaki, A.; Gollapudi, K.; Blumberg, J.; Belldegrun, A.; Pantuck, A.; et al. Role of surgical approach on lymph node dissection yield and survival in patients with upper tract urothelial carcinoma. Urol. Oncol. 2018, 36, 9.e1–9.e9. [Google Scholar] [CrossRef] [PubMed]
- Ye, H.; Feng, X.; Wang, Y.; Chen, R.; Zhang, C.; Zhang, W.; Guo, F.; Wang, Z.; Fang, Y.; Wu, Z.; et al. Single-docking robotic-assisted nephroureterectomy and extravesical bladder cuff excision without intraoperative repositioning: The technique and oncological outcomes. Asian J. Surg./Asian Surg. Assoc. 2020, 43, 978–985. [Google Scholar] [CrossRef] [PubMed]
- Kenigsberg, A.P.; Smith, W.; Meng, X.; Ghandour, R.; Rapoport, L.; Bagrodia, A.; Lotan, Y.; Woldu, S.L.; Margulis, V. Robotic Nephroureterectomy vs Laparoscopic Nephroureterectomy: Increased Utilization, Rates of Lymphadenectomy, Decreased Morbidity Robotically. J. Endourol. 2021, 35, 312–318. [Google Scholar] [CrossRef]
- Li, C.C.; Chang, C.H.; Huang, C.P.; Hong, J.H.; Huang, C.Y.; Chen, I.H.A.; Lin, J.T.; Lo, C.W.; Yu, C.C.; Tseng, J.S.; et al. Comparing Oncological Outcomes and Surgical Complications of Hand-Assisted, Laparoscopic and Robotic Nephroureterectomy for Upper Tract Urothelial Carcinoma. Front. Oncol. 2021, 11, 731460. [Google Scholar] [CrossRef]
- Mourmouris, P.; Argun, O.B.; Tzelves, L.; Tuna, M.B.; Gourtzelidou, M.; Tziotis, A.; Riza Kural, A.; Skolarikos, A. Is robotic radical nephroureterectomy a safe alternative to open approach: The first prospective analysis. Archivio Italiano di Urologia e Andrologia 2021, 93, 408–411. [Google Scholar] [CrossRef]
- Zeuschner, P.; Vollmer, S.G.; Linxweiler, J.; Wagenpfeil, G.; Wagenpfeil, S.; Saar, M.; Siemer, S.; Stöckle, M.; Heinzelbecker, J. Robot-assisted versus open radical nephroureterectomy for urothelial carcinoma of the upper urinary tract: A retrospective cohort study across ten years. Surg. Oncol. 2021, 38, 101607. [Google Scholar] [CrossRef] [PubMed]
- Veccia, A.; Carbonara, U.; Djaladat, H.; Mehazin, R.; Eun, D.D.; Reese, A.C.; Meng, X.; Uzzo, R.; Srivastava, A.; Porter, J.; et al. Robotic vs Laparoscopic Nephroureterectomy for Upper Tract Urothelial Carcinoma: A Multicenter Propensity-Score Matched Pair “Tetrafecta” Analysis (ROBUUST Collaborative Group). J. Endourol. 2022, 36, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Bae, H.; Chung, J.H.; Song, W.; Kang, M.; Jeon, H.G.; Jeong, B.C.; Seo, S.I.; Jeon, S.S.; Lee, H.M.; Sung, H.H. Robotic Radical Nephroureterectomy with Bladder Cuff Excision for Upper Tract Urothelial Carcinoma: A Trend Analysis of Utilization and a Comparative Study. Cancers 2022, 14, 2497. [Google Scholar] [CrossRef] [PubMed]
- Grossmann, N.C.; Soria, F.; Juvet, T.; Potretzke, A.M.; Djaladat, H.; Ghoreifi, A.; Kikuchi, E.; Mari, A.; Khene, Z.E.; Fujita, K.; et al. Comparing Oncological and Perioperative Outcomes of Open versus Laparoscopic versus Robotic Radical Nephroureterectomy for the Treatment of Upper Tract Urothelial Carcinoma: A Multicenter, Multinational, Propensity Score-Matched Analysis. Cancers 2023, 15, 1409. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.P.; Huang, E.Y.; Chung, H.J.; Tai, M.C.; Huang, T.H.; Wei, T.C.; Fan, Y.H.; Lin, C.C.; Lin, T.P.; Kuo, J.Y.; et al. Is Robotic Superior to Laparoscopic Approach for Radical Nephroureterectomy with Bladder Cuff Excision in Treating Upper Urinary Tract Urothelial Carcinoma? J. Endourol. 2023, 37, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Birtle, A.; Johnson, M.; Chester, J.; Jones, R.; Dolling, D.; Bryan, R.T.; Harris, C.; Winterbottom, A.; Blacker, A.; Catto, J.W.F.; et al. Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): A phase 3, open-label, randomised controlled trial. Lancet 2020, 395, 1268–1277. [Google Scholar] [CrossRef] [PubMed]
- Leow, J.J.; Chong, Y.L.; Chang, S.L.; Valderrama, B.P.; Powles, T.; Bellmunt, J. Neoadjuvant and Adjuvant Chemotherapy for Upper Tract Urothelial Carcinoma: A 2020 Systematic Review and Meta-analysis, and Future Perspectives on Systemic Therapy. Eur. Urol. 2021, 79, 635–654. [Google Scholar] [CrossRef]
- Dominguez-Escrig, J.L.; Peyronnet, B.; Seisen, T.; Bruins, H.M.; Yuan, C.Y.; Babjuk, M.; Bohle, A.; Burger, M.; Comperat, E.M.; Gontero, P.; et al. Potential Benefit of Lymph Node Dissection During Radical Nephroureterectomy for Upper Tract Urothelial Carcinoma: A Systematic Review by the European Association of Urology Guidelines Panel on Non-muscle-invasive Bladder Cancer. Eur. Urol. Focus 2019, 5, 224–241. [Google Scholar] [CrossRef]
- Yadav, K.; Lewis, R.J. Immortal Time Bias in Observational Studies. JAMA 2021, 325, 686–687. [Google Scholar] [CrossRef]
- Rai, B.P.; Bondad, J.; Vasdev, N.; Adshead, J.; Lane, T.; Ahmed, K.; Khan, M.S.; Dasgupta, P.; Guru, K.; Chlosta, P.L.; et al. Robotic versus open radical cystectomy for bladder cancer in adults. Cochrane Database Syst. Rev. 2019, 4, CD011903. [Google Scholar] [CrossRef]
| Author | Type of Study | Groups Compared | Centers | Study Characteristics | Site of Study |
|---|---|---|---|---|---|
| Ambani et al. 2012 [13] | Retrospective | Robotic vs. lap (including hand-assisted) | Single | Matched pair (tumor stage and age) | USA |
| Hu et al. 2015 [14] | Retrospective | Robotic vs. hand-assisted lap | Single | Matched pair (tumor location, sex, and age) | Taiwan |
| Melquist et al. 2016 [15] | Retrospective | Robotic vs. lap + open lower end | Single | Consecutive patients | USA |
| Rodriguez et al. 2017 [16] | Retrospective | Robotic vs. lap vs. open | Population database (NCDB) | - | USA |
| Lee et al. 2018 [17] | Retrospective | Robotic vs. lap vs. open | Population database (NCDB) | - | USA |
| Lenis et al. 2019 [18] | Retrospective | Robotic vs. lap vs. open | Single | - | Seoul, Republic of Korea |
| Ye et al. 2020 [19] | Retrospective | Robotic vs. lap | Single | - | China |
| Kenigsberg et al. 2021 [20] | Retrospective | Robotic vs. lap | Population database (NCDB) | - | USA |
| Li et al. 2021 [21] | Retrospective | Robotic vs. lap vs. hand-assisted lap | Multicenter (15 centers) | - | Taiwan |
| Mourmouris et al. 2021 [22] | Prospective | Robotic vs. open | Two centers | Consecutive patients | Greece, Turkey |
| Zeuschner et al. 2021 [23] | Retrospective | Robot-assisted vs. open | Single | Propensity-score matched pair (1:1) | Germany |
| Veccia et al. 2022 [24] | Retrospective | Robotic vs. lap | Multicenter (17 centers) | Propensity-score matched pair (2:1) | Worldwide |
| Bae et al. 2022 [25] | Retrospective | Robotic vs. lap vs. open | Single | - | Republic of Korea |
| Grossmann et al. 2023 [26] | Retrospective | Robotic vs. lap vs. open | Multicenter (21 centers) | 1:1:1 Propensity-score matching (PSM) analysis | Europe, Asia, USA |
| Huang et al. 2023 [27] | Retrospective | Robotic vs. lap | Single | - | Taiwan |
| Author | Groups | Age | p-Value | Gender—Males (n, %) | p-Value | Hydronephrosis | p-Value | BMI | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Ambani et al. 2012 [13] | RNU vs. LNU | 70.1 ± 2.2 vs. 70.8 ± 2.2 (Mean, SD) | 0.53 | 14 (64%) vs. 16 (73%) | 0.71 | ND | ND | ||
| Hu et al. 2015 [14] | RNU vs. LNU | 70.4 ± 6.3 vs. 69.6 ± 5.7 (Mean, SD) | 0.646 | 5 (27.8%) vs. 5 (27.8%) | 1 | 12 (66.7%) vs. 11 (61.1%) | 1 | 23.8 ± 3.4 vs. 25.0 ± 4.9 (Mean, SD) | 0.411 |
| Melquist et al. 2016 [15] | RNU vs. LNU | 68 (63.6–73.6) vs. 72.6 (65.8–81.8) (Median, IQR) | 0.06 | 26 (70%) vs. 36 (57%) | 0.2 | ND | 28 (26.1–32.6) vs. 28 (25.1–31.3) (Median, IQR) | 0.34 | |
| Rodriguez et al. 2017 [16] | RNU vs. LNU vs. ONU | 70.3 vs. 71.1 vs. 71 (Mean) | 0.01 | 62.40% vs. 59.10% vs. 59.10% | 0.03 | ND | ND | ||
| Lee et al. 2018 [17] | RNU vs. LNU vs. ONU | 67.6 ± 11.3 vs. 68.6 ± 10.4 vs. 67.5 ± 10.2 (Mean, SD) | 0.642 | 85 (68.5%) vs. 97 (70.8%) vs. 117 (72.7%) | 0.75 | 83 (68.0%) vs. 90 (65.7%) vs. 115 (71.9%) | 0.577 | 24.6 ± 2.9 vs. 23.9 ± 3.6 vs. 23.7 ± 2.8 (Mean, SD) | 0.062 |
| Lenis et al. 2019 [18] | RNU vs. LNU vs. ONU | 70.0 ± 10.9 vs. 70.6 ± 10.4 vs. 70.6 ± 10.5 (Mean, SD) | 0.48 | 469 (61.6%) vs. 772 (55.7%) vs. 537 (55.4%) | 0.02 | ND | ND | ||
| Ye et al. 2020 [19] | RNU vs. LNU | 71 (48–84) vs. 66 (44–83) (Median, IQR) | 0.924 | 21 (72.4%) vs. 82 (62.6%) | 0.394 | ND | ND | ||
| Kenigsberg et al. 2021 [20] | RNU vs. LNU | 71.4 vs. 72.7 (Mean) | <0.001 | 741 (65.6%) vs. 909 (60.5%) | 0.007 | ND | ND | ||
| Li et al. 2021 [21] | RNU vs. LNU | PD | 0.140 | 61 (43.3%) vs. 194 (42.4%) | 0.916 | 61 (43.3%) vs. 250 (54.6%) | <0.001 | ND | |
| Mourmouris et al. 2021 [22] | RNU vs. ONU | 68.12 ± 9.0 vs. 67.12 ± 12.19 (Mean, SD) | 0.8 | 14 (87.5%) vs. 24 (82.8%) | 1 | ND | 25.2 ± 1.85 vs. 26.54 ± 1.95 (Mean, SD) | 0.12 | |
| Zeuschner et al. 2021 [23] | RNU vs. ONU | 70.5 (39–86) vs. 74 (51–92) (Median, range) | 0.147 | 35 (53%) vs. 43 (66.2%) | 0.126 | 3 (4.5%) vs. 10 (15.4%) | 0.062 | 26 (18–35) vs. 26 (17–40) (Median, range) | 0.987 |
| Veccia et al. 2022 [24] | RNU vs. LNU | 72 (65–78) vs. 71 (64–77) (Median, IQR) | 0.44 | 106 (57.8%) vs. 55 (60.4%) | 0.69 | 72 (38.9%) vs. 44 (48.3%) | 0.33 | 26.3 (24.2–28.7) vs. 26.6 (24.7–28.5) (Median, IQR) | 0.57 |
| Bae et al. 2022 [25] | RNU vs. LNU vs. ONU | 68.5 ± 9.1 vs. 67.6 ± 9.6 vs. 69.7 ± 9.4 (Mean, SD) | 0.295 | 85 (71.4%) vs. 131 (70.8%) vs. 41 (67.2%) | 0.830 | ND | 25.2 ± 3.8 vs. 24.6 ± 3.2 vs. 25.3 ± 3.2 (Mean, SD) | 0.171 | |
| Grossmann et al. 2023 [26] | RNU vs. LNU vs. ONU | 70 (62–77) vs. 72 (65–78) vs. 73 (66–78) (Median, IQR) | 0.05 | 168 (66.7%) vs. 170 (67.4%) vs. 167 (66.3%) | >0.9 | 114 (45%) vs. 111 (44%) vs. 91 (36%) | 26 (23.4–29) vs. 26 (23–29) vs. 25.6 (22.3–28.9) (Median, IQR) | 0.3 | |
| Huang et al. 2023 [27] | RNU vs. LNU | 72 (63–80) vs. 72 (63–81) (Median, IQR) | 0.987 | 47 (54%) vs. 76 (52.8%) | 0.892 | ND | 23.9 (21.6–25.9) vs. 24 (21.1–26.9) Median, IQR | 0.703 |
| Author | Groups | TNM Stage | Tumor Grade | Tumor Location | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| <T2 | ≥T2 | p-Value | Low | High | p-Value | Kidney | Ureter | Both | p-Value | ||
| Ambani et al. 2012 [13] | RNU vs. LNU | 55% vs. 55% | 45% vs. 45% | ND | ND | ND | ND | 64% vs. 64% | 27% vs. 27% | 9% vs. 9% | 0.32 |
| Hu et al. 2015 [14] | RNU vs. LNU | 44.5% vs. 50% | 55.5% vs. 50% | 0.165 | 5.56% vs. 16.7% | 94.4% vs. 83.3% | 0.603 | 55.6% vs. 55.6% | 27.8% vs. 27.8%) | 16.7% vs. 16.7% | 1 |
| Melquist et al. 2016 [15] | RNU vs. LNU | 75% vs. 56% | 25% vs. 45% | 0.43 | ND | ND | ND | 57% vs. 46% | 24% vs. 37% | 19% vs. 17% | 0.44 |
| Rodriguez et al. 2017 [16] | RNU vs. LNU vs. ONU | 55.4% vs. 54.3% vs. 52.7% | 44.5% vs. 45.7% vs. 47.3% | 0.02 | ND | 69% vs. 69.8% vs. 72.9% | 0.01 | ND | 32% vs. 30.6% vs. 34.4% | ND | <0.01 |
| Lee et al. 2018 [17] | RNU vs. LNU vs. ONU | 33.9% vs. 35.8% vs. 23% | 66.1% vs. 64.3% vs. 77% | 0.001 | PD | PD | 0.177 | 50.8% vs. 56.9% vs. 52.2% | 42.7% vs. 38.7% vs. 33.5% | 6.5% vs. 4.4% vs. 14.3% | 0.013 |
| Lenis et al. 2019 [18] | RNU vs. LNU vs. ONU | 51.4% vs. 47.9% vs. 43.5% | 46.7% vs. 50.1% vs. 54.1% | <0.01 | 29.7% vs. 25.6% vs. 23.4% | 70.3% vs. 74.4% vs. 76.6% | 0.01 | 71.9% vs. 70.7% vs. 65.9% | 28.1% vs. 29.3% vs. 34.1% | ND | 0.01 |
| Ye et al. 2020 [19] | RNU vs. LNU | 41.3% vs. 37.4% | 58.7% vs. 62.6% | 0.842 | 44.8% vs. 32.1% | 55.2% vs. 67.9% | 0.201 | 37.9% vs. 44.3% | 51.7% vs. 45.8% | 10.4% vs. 9.9% | 0.817 |
| Kenigsberg et al. 2021 [20] | RNU vs. LNU | 62% vs. 60.3% | 38.1% vs. 39.7% | 0.456 | PD | PD | 0.456 | ND | ND | ND | ND |
| Li et al. 2021 [21] | RNU vs. LNU | 45.3% vs. 44.5% | 54.6% vs. 55.5% | 0.906 | 12.8% vs. 13.8% | 87.2% vs. 86.2% | 0.015 | 59.3% vs. 48.7% | 23.6% vs. 38.4% | 17.1% vs. 12.9% | <0.001 |
| Mourmouris et al. 2021 [22] | RNU vs. ONU | 50% vs. 48.3% | 50% vs. 51.7% | 0.01 | 56.3% vs. 27.6% | 43.7% vs. 72.4% | 0.06 | 62.5% vs. 48.3% | 37.5% vs. 51.7% | ND | 0.06 |
| Zeuschner et al. 2021 [23] | RNU vs. ONU | 34.8% vs. 30.8% | 65.1% vs. 69.2% | NS | ND | ND | ND | DNC | DNC | DNC | DNC |
| Veccia et al. 2022 [24] | RNU vs. LNU | 45.4% vs. 42.8% | 54.3% vs. 57.2% | 0.11 | ND | 55.3% vs. 70.4% | 0.23 | 69% vs. 64.6% | ND | ND | |
| Bae et al. 2022 [25] | RNU vs. LNU vs. ONU | 42% vs. 49.3% vs. 47.5% | 57.9% vs. 50.8% vs. 52.5% | 0.742 | PD | PD | 0.222 | 44.5% vs. 42.2% vs. 41% | 45.4% vs. 49.7% vs. 52.5% | 10.1% vs. 8.1% vs. 6.6% | 0.863 |
| Grossmann et al. 2023 [26] | RNU vs. LNU vs. ONU | 53% vs. 57% vs. 53% | 47% vs. 43% vs. 46% | 0.8 | 26% vs. 25% vs. 23% | 74% vs. 75% vs. 77% | 0.6 | 65% vs. 65% vs. 63% | 33% vs. 32% vs. 32% | 2% vs. 3.2% vs. 4.8% | 0.5 |
| Huang et al. 2023 [27] | RNU vs. LNU | 47.1% vs. 53.5% | 52.8% vs. 45.8% | 0.593 | 5.7% vs. 8.3% | 94.3% vs. 91% | 0.606 | 52.9% vs. 52.1% | 31% vs. 38.2% | 16.1% vs. 9.7% | 0.262 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajan, K.; Khalifa, A.; Geraghty, R.; Parmar, K.; KandaSwamy, G.; Gómez Rivas, J.; Somani, B.; Rai, B.P. Oncological Efficacy of Robotic Nephroureterectomy vs. Open and Laparoscopic Nephroureterectomy for Suspected Non-Metastatic UTUC—A Systematic Review and Meta-Analysis. Cancers 2023, 15, 4926. https://doi.org/10.3390/cancers15204926
Rajan K, Khalifa A, Geraghty R, Parmar K, KandaSwamy G, Gómez Rivas J, Somani B, Rai BP. Oncological Efficacy of Robotic Nephroureterectomy vs. Open and Laparoscopic Nephroureterectomy for Suspected Non-Metastatic UTUC—A Systematic Review and Meta-Analysis. Cancers. 2023; 15(20):4926. https://doi.org/10.3390/cancers15204926
Chicago/Turabian StyleRajan, Karthik, Ahmad Khalifa, Robert Geraghty, Kalpesh Parmar, Gokul KandaSwamy, Juan Gómez Rivas, Bhaskar Somani, and Bhavan Prasad Rai. 2023. "Oncological Efficacy of Robotic Nephroureterectomy vs. Open and Laparoscopic Nephroureterectomy for Suspected Non-Metastatic UTUC—A Systematic Review and Meta-Analysis" Cancers 15, no. 20: 4926. https://doi.org/10.3390/cancers15204926
APA StyleRajan, K., Khalifa, A., Geraghty, R., Parmar, K., KandaSwamy, G., Gómez Rivas, J., Somani, B., & Rai, B. P. (2023). Oncological Efficacy of Robotic Nephroureterectomy vs. Open and Laparoscopic Nephroureterectomy for Suspected Non-Metastatic UTUC—A Systematic Review and Meta-Analysis. Cancers, 15(20), 4926. https://doi.org/10.3390/cancers15204926